
Abstract
A previous genome-wide association study suggested that polymorphisms in the thyrotrophin-releasing hormone receptor (TRHR) gene contribute to fat-free mass (FFM) variation. The aim of the present study was to examine the association between polymorphisms in the TRHR gene with FFM and muscle strength in older women. Volunteers (n = 241; age = 66.65 ± 5.5 years) underwent quadriceps strength assessment using isokinetics and fat-free mass by dual-energy X-ray absorptiometry. TRHR polymorphisms and ancestry-informative markers were genotyped through standard procedures. No significant difference was observed for rs7832552. Regarding the rs16892496, ANCOVA revealed that appendicular fat-free mass (AFFM) and relative AFFM were significantly different between groups (p = 0.04 and p = 0.05, respectively). Individuals carrying A/A and A/C genotypes respectively showed, on average, an extra 1 kg and 900 g of AFFM when compared to C/C genotype carriers. Also, the C/C genotype group presented a significantly higher chance to have reduced muscle strength. The observations presented here provide further evidence that the rs16892496 polymorphism in the TRHR gene may play a role in FFM variation. Moreover, the results bring the novel insight that this genetic variant can present a modest contribution to muscle strength in older women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sarcopenia is described as the loss of skeletal muscle mass and strength related to aging (Forbes 1976; Gallagher et al. 1997; Hughes et al. 2001). This process is associated with negative consequences among the elderly, such as loss of functional capacity and autonomy (Fleg and Lakatta 1988; Baumgartner et al. 1998; Lima et al. 2009), increased risk of falls (Whipple et al. 1987), metabolic impairments (Bloesch et al. 1988), and reduced bone mineral density (Gentil et al. 2007a, b, 2009; Lima et al. 2009). Previous reports provide evidence that sarcopenia has significant health-care cost implications that warrant efforts to understand and counteract this age-related muscle mass and strength decline (Janssen et al. 2004).
The etiology of sarcopenia is not completely known but seems to be influenced by a variety and interrelated factors. It is well established that heritability significantly contributes to the interindividual variability of muscle mass and strength (Arden and Spector 1997; Tiainen et al. 2009) and to the decrease of strength due to aging (Carmelli and Reed 2000). Previous studies provide evidence that genetic factors are responsible for about 60–80 % of the interindividuals variation in fat-free mass (Seeman et al. 1996). However, although the heritability of muscle-related phenotypes is well documented in the literature, the identification of genes and polymorphisms associated with these phenotypes requires further studies. A reasonable number of allelic variants have been studied, but lack of consistency on replicating the findings makes the identification of genes with significant contribution still unclear. Detection of significant contributor's genetic variants may assist in improving the life quality of seniors, enabling to target preventive practices best suited to each individual, reducing the risk of developing dependence and related complications. The advent of biotechnology and reduced costs of genotyping have made genome-wide association studies (GWAS) an important tool in the search for candidate genes.
Regarding muscle-related phenotypes, few GWAS have been conducted, and few candidate genes have been identified. De Mars et al. (2008) sought to identify chromosomal regions linked to muscle area and bone cross-sectional, knee flexors, and extensors isometric torque in twins. The authors concluded that many genes still have little explanation for muscle strength determination (De Mars et al. 2008). Liu et al. (2009) studied the association of the thyrotrophin-releasing hormone receptor (TRHR) gene and fat-free mass (FFM) in 1,000 individuals. The authors reported that the polymorphisms rs16892496 (GG) and rs7832552 (TT) in the TRHR gene are associated with FFM and replicated these findings in three independent samples. According to the authors, subjects with these genotypes have, on average, 2.70 and 2.55 kg less FFM, respectively, when compared to those with other genotypes. However, it was not in the scope of the report to examine the association with muscle strength.
Studies conducted in different populations are needed to better understand the influence of the TRHR gene on muscle phenotypes. Accordingly, this study sought to examine candidate genes previously identified through GWAS against muscle phenotypes. Specifically, the objective was to replicate the results of previous studies, to verify whether there is an association between polymorphisms in the TRHR gene (rs16892496 and rs7832552) and muscle strength and FFM phenotypes in a sample of Brazilian elderly women. Aware of the high admixture in Brazilians and of its potential complications when performing association studies in such population (Lins et al. 2011), 19 ancestry-informative single-nucleotide polymorphisms were genotyped, and the estimated genetic ancestry values were included as covariates during the analysis.
Methodology
Subjects
After applying the exclusion criteria, this study included 241 women aged between 60 to 82 years and participants in a voluntary project developed at the university. The following were excluded from the study participants: those who (a) did not have Brazilian nationality, (b) were not able to walk independently, (c) had unilateral or bilateral hip prosthetic, (d) had a prosthetic heart valve, (e) were smokers, (f) had endocrine or metabolic disorder known to affect the muscular system, and (g) had abnormal cardiac conduction or infusion that would contraindicate the practice of physical activities. To take part in the study, volunteers signed a written consent. The study was approved by the Research Ethics Committee of the university (CEP/UCB 014/2007).
The official Portuguese long version of the International Physical Activity Questionnaire (IPAQ) was used to determine the physical activity level of each volunteer. The questionnaire was performed in face-to-face interviews as recommended. The IPAQ was developed by investigators from various countries with the support of the World Health Organization. It has been reported as an instrument with acceptable measurement properties in various countries (Craig et al. 2003).
Assessment of body composition
Body composition measurements were conducted using dual-energy X-ray absorptiometry (DXA) (DPX-L, Lunar Radiation Corporation, Madison, WI). All measurements were carried out by the same trained technician according to the procedures previously described (Lima et al. 2007). Besides total FFM (TFFM) and fat mass, computer-generated lines with subsequent manual adjustment enabled specification of FFM for the arms, legs, and trunk. Appendicular FFM (AFFM) was calculated as the sum of both arms and legs FFM. In addition to the use of absolute TFFM and AFFM, these variables were considered relative to body height squared (in kilogram per square meter) (Baumgartner et al. 1998). Coefficients of variation observed for the DXA were 2.1 and 1.9 % for fat mass and FFM, respectively.
Isokinetic muscle peak torque
Quadriceps strength was measured using the Biodex System 3 isokinetic dynamometer (Biodex Medical Systems, New York, USA). Before each test, participants underwent 5 min of warm-up in a cycle ergometer with low load and comfortable speed. After a detailed explanation of the evaluation procedures, volunteers were carefully positioned on the seat of the equipment. The rotation axis from the dynamometer arm was aligned with the dominant femoral epicondyle. The force application point was positioned 2 cm above the medial malleolus. Fastened Velcro belts were used on the trunk, pelvis, and thigh to avoid compensatory movements. The protocol consisted of three sets of four concentric muscle contractions (60°/s) with 30-s rest intervals between sets (Bottaro et al. 2005). The recorded value for analysis was the highest peak torque (PT) of the three series, which was expressed in absolute values (in normal meter) and relative to body mass (in normal meter per kilogram). Participants were asked to perform the contractions with the greatest possible force, and verbal encouragement was offered during the measurement. The calibration of the equipment was performed according to manufacturer's specifications at the beginning of the evaluation sessions, and the same evaluator carried out the procedures.
Genotyping
Blood samples from all participants were collected in the antecubital vein, and genomic DNA of high molecular weight was extracted from peripheral leukocytes by the “salting out” method (Miller et al. 1988).
Genotyping of the rs16892496 (A/C) and rs7832552 (A/C) SNPs was performed using a multiplex PCR (Qiagen® Multiplex PCR kit), followed by purification with exonuclease I and shrimp alkaline phosphatase, and single-base extension method (ABI Prism® SNaPshot® Multiplex kit, Applied Biosystems, Foster City, CA, USA) followed by purification with shrimp alkaline phosphatase. An aliquot of this purified product, prepared with a molecular size standard (GS120 Liz, Applied Biosystems) and highly deionized formamide, was denatured at 95 °C to the subsequent capillary electrophoresis (ABI 3130xl, Applied Biosystems). The electropherograms were analyzed using the GeneMapper™ 4.0 software (Applied Biosystems, Foster City, CA, USA). Genotyping of 19 ancestry-informative markers was performed under the same conditions described above.
Genetic ancestry evaluation
To estimate genomic ancestry, 19 ancestry-informative markers were genotyped for all the samples, and individual ancestry in each parental population was estimated using the software ADMIXMAP (http://homepages.ed.ac.uk/pmckeigu/admixmap/), with 2,500 iterations for the burn-in period and 10,000 iterations to measure parameter data.
Statistical analysis
Normality of data distribution was examined using the Kolmogorov–Smirnov test. Data are presented using descriptive statistics, with mean and standard deviations procedures (unless otherwise noted). To verify if the allelic frequencies were in accordance with the Hardy–Weinberg equilibrium, the chi-square test was used. Analysis of variance (ANOVA) was applied to test for differences between genotypes in the following variables: age, weight, height, BMI, and fat percentage. To verify differences between genotypes for noncontinuous variables such as the prevalence of sarcopenia, calcium supplementation, use of hormone replacement therapy, and physical activity level, the chi-square test was conducted. To test the association between genotypes and muscle-related phenotypes, analysis of covariance models was performed with LSD post hoc covariates which included years of menopause, hormone replacement, calcium supplementation, and physical activity levels. The inclusion of individual African genomic ancestry was also used as covariate as an attempt to correct for population stratification. Mantel–Haenszel common odds ratio analysis was used to investigate the association between outcomes (phenotypes) and risks (genotype), adjusted for age and genomic ancestry. To reach this end, muscle phenotypes variables were divided into quartiles, where Q1 was the lower quartile, and Q4, the highest. The significance level was p ≤ 0.05, and data were analyzed using SPSS 13.0 for Windows.
Results
The descriptive data of the sample such as age, weight, height, BMI, years since menopause, peak torque, and body composition are shown in Table 1. According to the approach proposed by Baumgartner et al. (1998), 17.3 % of subjects were classified as sarcopenic. In relation to hormone replacement therapy and calcium supplements, 19 (7.9 %) and 56 (23.7 %) women were using both, respectively. Physical activity levels were as follows: 5 (2.1 %) were sedentary, 69 (28.6 %) were insufficiently active, 163 (67.6 %) were active, and 4 (1.7 %) were very active.
The genotype distribution of the TRHR gene (rs16892496 and rs7832552) was consistent with Hardy–Weinberg equilibrium (p > 0.05). No significant difference was observed for rs7832552, and thus, the results are all related to the rs16892496. The prevalence of sarcopenia was 27.6, 17.8, and 13.3 %, respectively, for genotypes C/C, A/C, and A/A; however, the chi-square test did not reveal significant differences. Furthermore, ANOVA revealed no significant difference for weight, height, or BMI; however, age was significantly higher for those with genotype C/C and, therefore, was used as covariate in subsequent analyses along with African genomic ancestry. The results of body composition and muscle-related phenotypes (i.e., FFM and strength) according to the rs16892496 genotypes are shown in Table 2. No significant differences were observed for BMI or body fat percentage. ANOVA revealed that AFFM and PT were significantly different between groups, with lower values of AFFM in subjects carrying C/C genotype. However, when age and genomic ancestry were entered as covariates, the results did not reach a statistical significance, but only a trend (p values ranging from 0.07 to 0.15; Table 2). When genotype C/C was compared to the group composed by A allele carriers (i.e., A/A+A/C), significant differences were observed for AFFM and relative AFFM with lower values for the C/C genotype (after adjustment for age and African genomic ancestry).
Appendicular FFM relative to height squared and PT relative to body weight were divided into quartiles, and the odds ratio in relation to genotype groups are presented in Table 3. It was observed that the C/C genotype group presented a significantly higher chance to be classified in the lower quartile of AFFM when compared to both A/A genotypes. Regarding PT relative to body weight, the C/C genotype presented a threefold increase in the chance to be classified in the lower quartile when compared to the A/A genotype.
Discussion
Based on previous GWAS showing an association between the rs16892496 and rs7832552 and FFM in different populations with a wide age range, the present study was designed to examine its association in older women not only with FFM but also with muscle strength. Muscle mass and strength decline with advancing age (Goodpaster et al. 2008), and this process is associated with negative clinical outcomes in the elderly (Baumgartner et al. 1998; Lima et al. 2009). Therefore, it is of particular interest to examine the association of gene polymorphisms and muscular phenotypes in the elderly. The main findings of the present study provide further evidence of an association between the THRH rs16892496 polymorphism and FFM. Moreover, the results bring the insight that this genetic variant can present a contribution to muscle strength in older women. Of note, these observations remained significantly after adjustment for genomic African ancestry.
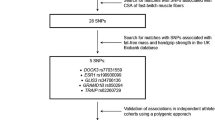
A variety of previous reports had shown association between a reasonable number of candidate gene polymorphisms and muscle-related phenotypes, but with little agreement on significant contributors (Rankinen et al. 2010; Lima et al. 2011; Tan et al. 2012). GWAS has become an important tool for better understanding the association between phenotypes and genotypes. Exercise scientists need to prioritize high-quality research designs, and replication studies with large sample sizes are urgently needed (Rankinen et al. 2010). Liu et al. (2009) published the first GWAS focusing on skeletal muscular traits, specifically FFM. Although muscle strength was not assessed in their investigation, the authors identified that rs16892496 and rs7832552 polymorphisms in the TRHR gene were associated with FFM (by dual-energy X-ray absorptiometry) in a study of 9,350,000 SNPs examined in nearly 1,000 unrelated US whites. Moreover, these authors replicated the significant associations in three independent samples. Taken together with the present results, these observations suggest that the TRHR gene might be an important candidate for interindividual differences in muscular phenotypes.
This replication study in a sample of Brazilian elderly suggests a modest association between rs16892496 and FFM. Individuals carrying the C/C genotype presented a higher chance for low values of AFFM when compared to homozygous A/A. Individuals A/A and A/C, on average, respectively showed an extra 1 kg and 900 g of AFFM compared to C/C genotype carriers. Furthermore, we observed a trend for the difference between genotypes for isokinetic peak torque. It was observed that the C allele carriers were more likely to be classified in the lower quartile of muscle strength. However, the differences observed in the present study were modest when considering the high heritability of muscle-related phenotypes (Liu et al. 2009; De Mars et al. 2008). Probably, many genes with small contributions, rather than few genes with strong influence, are expected to determine the interindividual differences of such traits (Thompson et al. 2004; De Mars et al. 2008; Pescatello et al. 2006). Thus, the present study provides evidence that the studied polymorphism (rs16892496) in the TRHR gene is one genetic variant that contributes to FFM and muscle strength in cross-sectional analyses, though its clinical relevance remains to be investigated.
In fact, heritability of a variety of complex phenotypes is well documented in the literature (Thompson et al. 2004; Tiainen et al. 2009; Tan et al. 2012); however, the contributory genes remain unclear. Understanding the relationship between genotypes and muscular phenotypes in the elderly might contribute to assist in an early intervention and allow preventive practices best suited to each individual, thus ultimately improving life quality in this population. Identification of significant genetic variants underlying sarcopenia will provide valuable insights into important potential targets for risk stratification, as well as pharmacogenetic interventions aimed at increasing muscle mass and strength. Few genes have been identified to date, but lack of replication does not enable unequivocal conclusions (Tan et al. 2012).
The TRHR gene encodes the thyrotrophin-releasing hormone receptor. Because of the functional importance of thyroid hormone in skeletal muscle development, the TRHR gene is thus recognized as an important candidate gene for future investigations, with potential consequences for the correlated traits of muscle strength and power (Rankinen et al. 2010). Thyrotrophin-releasing hormone is a small neuropeptide widely distributed throughout the central nervous system and peripheral tissues, as well as in the extraneurais tissues. This hormone exerts its effect by binding to TRHR (located in the region 8q.23.1) on the surface, thyrotrophic pituitary cells. The main consequence of this connection is the stimulation of secretion of thyroid-stimulating hormone. In response, the thyroid-stimulating hormone stimulates the release of thyroxine, which is important in developing skeletal muscle of vertebrates (Larsson et al. 1994; Gáspár et al. 2010). The study by Liu et al. (2009) is pointed by the catalog of the National Human Genome Research Institute (Hindorff et al. 2010) as the only work that found the association of TRHR gene and body mass (lean). Until then, studies with this gene were associated with other outcomes such as pituitary adenoma (Igarashi-Migitaka et al. 2003) and hypertension (García et al. 2001; Ruixing et al. 2008).
In summary, the observations presented here provide further evidence that the rs16892496 polymorphism in the TRHR gene may play a role in FFM variation. Moreover, the results bring the novel insight that this genetic variant can present a contribution to muscle strength in older women. These results remained unchanged with the inclusion of genomic ancestry as a measure to correct for population stratification. Determination of genetic variants associated with muscular phenotypes in the elderly may be useful in identifying individuals who are more susceptible to lose muscle mass and strength with advancing age. For instance, however, it seems that the adoption of preventive habits such as regular physical activity practice is the intervention of choice for all individuals, independent of their genetic background.
References
Arden N, Spector T (1997) Genetic influences on muscle strength, lean body mass, and bone mineral density: a twin study. J Bone and Mineral Res 12(12):2076–2081
Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, Garry PJ, Lindeman RD (1998) Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 147(8):755–763
Bloesch D, Schutz Y, Breitenstein E, Jequier E, Felber J (1988) Thermogenic response to an oral glucose load in man: comparison between young and elderly subjects. J Am College of Nutr 7(6):471–483
Bottaro M, Russo A, Oliveira R (2005) The effects of rest interval on quadriceps torque during an isokinetic testing protocol in elderly. J Sports Sci and Med 4(3):285–290
Carmelli D, Reed T (2000) Stability and change in genetic and environmental influences on hand-grip strength in older male twins. J Appl Physiol 89(5):1879–1883
Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF (2003) International physical activity questionnaire: 12-country reliability and validity. Med Sci in Sports Exercise 35(8):1381
De Mars G, Windelinckx A, Huygens W, Peeters MW, Beunen GP, Aerssens J, Vlietinck R, Thomis MAI (2008) Genome-wide linkage scan for contraction velocity characteristics of knee musculature in the Leuven Genes for Muscular Strength Study. Physiol Genomics 35(1):36–44
Fleg JL, Lakatta EG (1988) Role of muscle loss in the age-associated reduction in VO2 max. J Appl Physiol 65(3):1147–1151
Forbes GB (1976) Adult decline in lean body mass. [/sup 40/K tracer technique]. Hum Biol; (United States) 48 (1)
Gallagher D, Visser M, De Meersman RE, Sepúlveda D, Baumgartner RN, Pierson RN, Harris T, Heymsfield SB (1997) Appendicular skeletal muscle mass: effects of age, gender, and ethnicity. J Appl Physiol 83(1):229–239
García SI, Porto PI, Dieuzeide G, Landa MS, Kirszner T, Plotquin Y, Gonzalez C, Pirola CJ (2001) Thyrotropin-releasing hormone receptor (TRHR) gene is associated with essential hypertension. Hypertension 38(3):683–687
Gáspár E, Hardenbicker C, Bodó E, Wenzel B, Ramot Y, Funk W, Kromminga A, Paus R (2010) Thyrotropin releasing hormone (TRH): a new player in human hair-growth control. FASEB J 24(2):393–403
Gentil P, de Lima LTC, Lima RM, De Abreu BS, Grattapaglia D, Bottaro M, De Oliveira RJ, Pereira RW (2009) Vitamin-D-receptor genotypes and bone-mineral density in postmenopausal women: interaction with physical activity. J Aging and Phys Act 17(1):31
Gentil P, Lima R, Lins T, Abreu B, Pereira R, Oliveira R (2007a) Physical activity, Cdx-2 genotype, and BMD. Int J Sports Med 28(12):1065
Gentil P, Lima RM, Jacó de Oliveira R, Pereira RW, Reis VM (2007b) Association between femoral neck bone mineral density and lower limb fat-free mass in postmenopausal women. J Clin Densitom 10(2):174–178
Goodpaster BH, Chomentowski P, Ward BK, Rossi A, Glynn NW, Delmonico MJ, Kritchevsky SB, Pahor M, Newman AB (2008) Effects of physical activity on strength and skeletal muscle fat infiltration in older adults: a randomized controlled trial. J Appl Physiol 105(5):1498–1503
Hindorff LA, Junkins HA, Mehta J, Manolio T (2010) A catalog of published genome-wide association studies. National Human Genome Research Institute (Available at http://www.genome.gov/page.cfm?pageid=26525384#searchForm)
Hughes VA, Frontera WR, Wood M, Evans WJ, Dallal GE, Roubenoff R, Singh MAF (2001) Longitudinal muscle strength changes in older adults. J Gerontology Series A: Biol Sci and Med Sci 56(5):B209–B217
Igarashi-Migitaka J, Yamada S, Hara M, Sano T, Ozawa Y, Ohtani-Kaneko R, Hirata K (2003) Gene expression study of thyrotropin releasing hormone (TRH) receptor using RT-PCR: relationship to clinical and immunohistochemical phenotypes in a series of human pituitary adenomas. Endocr J 50(4):459
Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R (2004) The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc 52(1):80–85
Larsson L, Li X, Teresi A, Salviati G (1994) Effects of thyroid hormone on fast- and slow-twitch skeletal muscles in young and old rats. J Physiol 481(Pt 1):149–161
Lima R, Leite T, Pereira R, Rabelo H, Roth S, Oliveira R (2011) ACE and ACTN3 genotypes in older women: muscular phenotypes. Int J Sports Med 32(1):66
Lima RM, Bezerra L, Rabelo HT, Silva MAF, Silva AJR, Bottaro M, De Oliveira RJ (2009) Fat-free mass, strength, and sarcopenia are related to bone mineral density in older women. J Clin Densitom 12(1):35–41
Lima RM, De Abreu BS, Gentil P, de Lima Lins TC, Grattapaglia D, Pereira RW, De Oliveira RJ (2007) Lack of association between vitamin D receptor genotypes and haplotypes with fat-free mass in postmenopausal Brazilian women. J Gerontology Series A: Biol Sci and Med Sci 62(9):966–972
Lins TC, Vieira RG, Abreu BS, Gentil P, Moreno-Lima R, Oliveira RJ, Pereira RW (2011) Genetic heterogeneity of self-reported ancestry groups in an admixed Brazilian population. J Epidemiol 21(4):240–245
Liu XG, Tan LJ, Lei SF, Liu YJ, Shen H, Wang L, Yan H, Guo YF, Xiong DH, Chen XD, Pan F, Yang TL, Zhang YP, Guo Y, Tang NL, Zhu XZ, Deng HY, Levy S, Recker RR, Papasian CJ, Deng HW (2009) Genome-wide association and replication studies identified TRHR as an important gene for lean body mass. Am J Hum Genet 84(3):418–423. doi:10.1016/j.ajhg.2009.02.004
Miller S, Dykes D, Polesky H (1988) A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 16(3):1215
Pescatello LS, Kostek MA, Gordish-Dressman H, Thompson PD, Seip RL, Price TB, Angelopoulos TJ, Clarkson PM, Gordon PM, Moyna NM (2006) ACE ID genotype and the muscle strength and size response to unilateral resistance training. Med Sci in Sports Exercise 38(6):1074
Rankinen T, Roth SM, Bray MS, Loos R, Pérusse L, Wolfarth B, Hagberg JM, Bouchard C (2010) Advances in exercise, fitness, and performance genomics. Med Sci in Sports Exercise 42(5):835
Ruixing Y, Jinzhen W, Shangling P, Weixiong L, Dezhai Y, Yuming C (2008) Sex differences in environmental and genetic factors for hypertension. Am J Med 121(9):811–819
Seeman E, Hopper JL, Young NR, Formica C, Goss P, Tsalamandris C (1996) Do genetic factors explain associations between muscle strength, lean mass, and bone density? A twin study. Am J Physiol Endocrinol Metab 270(2):E320–E327
Tan LJ, Liu SL, Lei SF, Papasian CJ, Deng HW (2012) Molecular genetic studies of gene identification for sarcopenia. Hum Genet 131(1):1–31. doi:10.1007/s00439-011-1040-7
Thompson PD, Moyna N, Seip R, Price T, Clarkson P, Angelopoulos T, Gordon P, Pescatello L, Visich P, Zoeller R (2004) Functional polymorphisms associated with human muscle size and strength. Med Sci in Sports Exercise 36(7):1132
Tiainen K, Sipila S, Kauppinen M, Kaprio J, Rantanen T (2009) Genetic and environmental effects on isometric muscle strength and leg extensor power followed up for three years among older female twins. J Appl Physiol 106(5):1604–1610. doi:10.1152/japplphysiol.91056.2008
Whipple R, Wolfson L, Amerman P (1987) The relationship of knee and ankle weakness to falls in nursing home residents: an isokinetic study. J Am Geriatr Soc 35(1):13
Acknowledgments
We thank the participants of the study. Funding was provided by a grant 193.000.555/2009 from the Research Support Foundation of the Federal District (FAP-DF) and by a grant from the National Council for Scientific and Technological Development (CNPq).
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Lunardi, C.C., Lima, R.M., Pereira, R.W. et al. Association between polymorphisms in the TRHR gene, fat-free mass, and muscle strength in older women. AGE 35, 2477–2483 (2013). https://doi.org/10.1007/s11357-013-9526-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11357-013-9526-y