
Abstract
Identification of predictors of cognitive trajectories through the establishment of composite or single-parameter dimensional categories of cognition and mood may facilitate development of strategies to improve quality of life in the elderly. Participants (n = 487, aged 50+ years) were representative of the Portuguese population in terms of age, gender, and educational status. Cognitive and mood profiles were established using a battery of neurocognitive and psychological tests. Data were subjected to principal component analysis to identify core dimensions of cognition and mood, encompassing multiple test variables. Dimensions were correlated with age and with respect to gender, education, and occupational status. Cluster analysis was applied to isolate distinct patterns of cognitive performance and binary logistic regression models to explore interrelationships between aging, cognition, mood, and socio-demographic characteristics. Four main dimensions were identified: memory, executive function, global cognitive status, and mood. Based on these, strong and weak cognitive performers were distinguishable. Cluster analysis revealed further distinction within these two main categories into very good, good, poor, and very poor performers. Mood was the principal factor contributing to the separation between very good and good, as well as poor and very poor, performers. Clustering was also influenced by gender and education, albeit to a lesser extent; notably, however, female gender × lower educational background predicted significantly poorer cognitive performance with increasing age. Mood has a significant impact on the rate of cognitive decline in the elderly. Gender and educational level are early determinants of cognitive performance in later life.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Aging is typically associated with a gradual decline in cognition, the extent of which varies between individuals. The aging brain retains a degree of plasticity, allowing for functional reorganization and compensation. The factors and mechanisms that promote development of this potential are incompletely defined; although, educational (Ardila et al. 2000; Paulo et al. 2011) and social status as well as cognitive engagement (Paulo et al. 2011; Stine-Morrow et al. 2008), motivation, and mood (Forstmeier and Maercker 2008; Harvey et al. 2006) are likely important modulators of cognitive aging. Differential interactions between these factors may serve to maintain cognitive ability and may explain intra- and inter-individual differences in cognitive performance over the lifespan (Hilborn et al. 2009; Stern 2009). Resolving the common denominators of age-associated cognitive decline (Salthouse 2010a, b) becomes a complex task in light of the high (and unpredictable) number of interacting cognitive variables and the fact that each permutation may lead to overlapping or differential courses of cognitive decline.
The present report from the Switchbox Consortium (http://www.switchbox-online.eu/) is based on findings in older, community-dwelling individuals living in the Minho Region of Portugal; the cohort, representative of the country’s population, is enrolled in a longitudinal study design. The study population was initially stratified into cognitively “strong” and “weak” groups, and a cross-sectional analysis was then undertaken to examine the role of mood in determining individual cognitive profiles; in addition, the influence of other potential determinants of cognitive performance (gender, educational level, and occupational status) were analyzed. The results may have broader implications given that, on measures of literacy, (un)employment rates, positive experience/mental health, and other demographic characteristics, Portugal ranks close to the Organisation for Economic Co-operation and Development (OECD, www.oecd.org/) average (OECD 2012).
Material and methods
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki (59th Amendment) and was approved by national (Comissão Nacional de Protecção de Dados) and local (Hospital Escala Braga, Braga; Centro Hospitalar do Alto Ave, Guimarães; and Unidade Local de Saúde do Alto Minho, Viana-do-Castelo/Ponte-de-Lima) ethics review boards. As required by the national ethics committee, medical and/or research professionals involved in the study signed a Statement of Responsibility and Confidentiality. Potential participants were explained the study goals and the nature of the tests, and all volunteers provided informed consent.
Sample characteristics
Participants (n = 487) were randomly selected from the Guimarães and Vizela local area health authority registries in the Minho Region of Portugal; selection criteria are described elsewhere (Paulo et al. 2011), and further information is provided in the Supplementary Online Material. Briefly, the primary exclusion criteria included participant choice to withdraw from the study, incapacity and/or inability to attend the clinical and neuropsychological assessment session(s), diagnosed neuropsychiatric disorder, and/or inability to understand informed consent. A team of experienced clinicians performed a standardized clinical interview.
The cohort was representative of the general Portuguese population with respect to gender (261 or 54 % were women), age (range, 50–91 years; M = 67, SD = 9.0; age categories, [50–60], 23.2 % (females, 53.1 %); [60–70], 32.9 % (females, 55.0 %); [70 + ], 43.9 % (females, 52.8 %)); and years of formal education (median years of schooling = 4; 10.9, 17.3, 56.4, 5.3, 8.2, and 1.9 % of the cohort attended school for 0, 1–2, 3–4, 5–8, 9–12, and 13+ years, respectively; literacy rate 83.3 %). All participants lived in noninstitutional communities, with equal distribution between urban and rural areas. The majority of participants were retired (n = 352, 72 %); of the non-retired, 27 (5 %) were unemployed. Using the Graffar measure of socioeconomic status, 62 % of participants belonged to the medium stratum (class III). Regarding general health, 2.1 % (females, 30.0 %) had history of renal failure; 13.3 % (females, 41.5 %), coronary/cardiac disease or insufficiency (including coronary bypass, peripheral vascular disease, cardiac insufficiency, myocardial infarction, coronary disease, and arrhythmia), 21.1 % (females, 44.7 %) diabetes (including diabetes mellitus type I and II), 58.1 % (females, 56.2 %) dyslipidemia, 56.7 % (females, 59.4 %) hypertension, and 9.4 % (females, 34.8 %) hyperuricemia. Physical activity status was reported as “none” for 61.7 % (females, 55.7 %), “less than three times per week” for 14.4 % (females, 55.7 %), “over three times per week” for 12.6 % (females, 44.3 %), and “daily” for 11.3 % (females, 50.9 %).
Cognitive and psychological evaluation
Tests were selected to provide general cognitive profiles (specifically, memory and executive functions), mood, and socioeconomic status. Short-term verbal memory was assessed with the digit span forward test (subtest of the Wechsler adult intelligence test WAIS III, 1997) (Wechsler 1997); verbal working memory with the digit span backward test (subtest of the Wechsler adult intelligence test WAIS III, 1997) (Wechsler 1997); response inhibition/cognitive flexibility with the Stroop color and word test (Strauss et al. 2006); verbal fluency with the controlled oral word association test (COWAT, FAS) (Lezak et al. 2004); multiple trial verbal learning and memory with the selective reminding test (SRT) (Buschke 1995); high-level information processing speed with the digit symbol substitution test (DSST, subtest of the Wechsler adult intelligence test WAIS III, 1997) (Strauss et al. 2006); global cognitive status with the mini-mental state examination (MMSE) (Folstein et al. 1975); mood with the geriatric depression scale (GDS, long version) (Yesavage et al. 1983); and socioeconomic status with the Graffar test (Graffar 1956). A team of trained psychologists conducted the neurocognitive and psychological assessments.
Statistical analysis
This study aimed to (a) identify dimensions of cognitive performance and mood and (b) characterize clusters based on these two variables, in a cross-sectional elderly population. After structuring the data as described in the Supplementary Online Material data, the following analyses were performed:
-
(1)
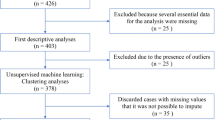
Principal component analysis (PCA), as detailed in the Supplementary Online Material data. Briefly, the sample for PCA analysis (n = 247, with no missing values; 129 or 52 % women; age range, 50–88 years, M = 66, SD = 8.97) was derived from the initial sample of 487 subjects. All subjects were literate, the median value of formal school education being 4 years (three-to-four school year category, 67.6 %). The sample chosen for PCA analysis was representative of the initial study population in terms of occupation (169 or 68 % were retired; 19 or 8 % of non-retirees unemployed) as well as socioeconomic status (70 % belonged to class III). Analysis of the neurocognitive and psychological test datasets identified four significant dimensions of cognitive performance and mood: memory (MEM, based on SRT variables; CLTR, LTS, and delayed recall) and executive function (EXEC, Stroop parameters; words, colors, and words/colors; FAS parameter, admissible; and forward/backward digit spans) global cognitive status (MMSE) and mood (GDS). The results were obtained by conducting PCA in two steps. Initially, a sample comprising 247 subjects (sampling adequacy, KMO = 0.825) was selected (Table 1). Bartlett’s sphericity test revealed significant correlation between the variables (test parameters) (χ 2 (55) = 992.4; p < 0.001). Parameters that had low Cronbach α values (e.g., intrusions in the SRT and non-admissible in the FAS) were excluded from the PCA dimensional composite. The variable GDS was excluded from the final composite PCA dimension due to a low communalities value (<0.300); similarly, the variable MMSE was excluded since its component loadings were <0.5 and saturation with similar weights in two separate components. Each variable was instead considered as a unique single dimension (respectively, GDS and MMSE) in all further analyses. The DSST data were not considered due to small sample size (n = 161). The validity of these dimensional groupings for all participants in the study was demonstrated in a subsequent PCA (MEM, based on n = 482 with ≤1 missing variables, and n = 436 [90 %] with no missing parameters; EXEC, n = 405 [67 %] with ≤1 missing variables) (Table 1). Missing values were calculated on the basis of the weight of each remaining parameter in the case of MEM (10 % missing data on delayed recall) and EXEC (33 % missing data on the admissible variable in FAS), resulting in valid sample sizes of 487 for each of these dimensions (Table 1).
Table 1 Principal component analysis with varimax rotation: identification of composite dimensions -
(2)
Cluster analysis, as detailed in the Supplementary Online Material data. Patterns (clusters) of cognitive performance and mood were identified by applying a K-means-constrained cluster solution to the composite or single z-scores of the identified core dimensions (clustering variables: MEM, EXEC, MMSE, GDS). Four separate clustering solutions, comprised of two to five clusters, were tested. In order to identify the most suitable solution, ANOVAs were performed on each cluster solution, using the four dimensions (cognition and mood) as dependent variables and cluster membership as a factor variable (independent variable). General effect size η 2 was derived by dividing the sum of all between-groups sum of squares by the sum of the total sum of groups; for the two-, three-, four-, and five-cluster solutions, η 2 was 0.33, 0.47, 0.56, and 0.61, respectively. The four-membership clustering solution was considered to provide the best cluster solution. Finally, Levene’s test for homogeneity of variances was used to test equality of variance between the different age categories ([50–60], [60–70], [70 + ]) in the clusters.
-
(3)
Two binary logistic regression models were used to examine socio-demographic characteristics (variables gender, age, occupational status, and years of schooling) that might discriminate cluster membership, as well to explore the possible hierarchical importance of these.
Results
Socio-demographic factors influence cognitive and mood dimensions
The distribution of the identified PCA-derived dimensions (MEM, EXEC, MMSE, and GDS) across all age groups in the complete population sample (n = 487) was analyzed with respect to gender (Fig. 1), education level (number of formal school years, 0, 1–2, 3–4, 5–8, 9–12, and 13+) (Fig. 2) and occupational status (employed, unemployed, retired) (Fig. 3).

Gender relationship with age for each identified composite and single dimension. a MEM (R 2 linear, female, 0.126; male, 0.176), b EXEC (R 2 linear, female, 0.114; male, 0.155), c MMSE (R 2 linear, female, 0.184; male, 0.148), d GDS (R 2 linear, female, 0.003; male, 0.003). Males and females are represented in blue and green circles, respectively

Relationship between educational level and age for each identified composite and single dimension. a MEM (R 2 linear, 0, 0.034; 1–2, 0.047; 3–4, 0.096; 5–8, 0.289; 9–12, 0.054; 13+ years, 0.519), b EXEC (R 2 linear, 0, 0.109; 1–2, 0.02; 3–4, 0.118; 5–8, 0.114; 9–12, <0.001; 13+ years, 0.002), c MMSE (R 2 linear, 0, 0.046; 1–2, 0.088; 3–4, 0.084; 5–8, 0.013; 9–12, 0.035; 13+ years, 0.039), d GDS (R 2 linear: 0, <0.001; 1–2, <0.001; 3–4, 0.004; 5–8, 0.031; 9–12, 0.079; 13+ years, 0.271). School years 0, 1–2, 3–4, 5–8, 9–12, and 13+ are shown as blue, green, red, purple, orange, and white circles, respectively

Relationship between occupational status and age for each identified composite and single dimension. a MEM (R 2 linear, retirement, 0.093; employment, 0.164; unemployment, 0.039), b EXEC (R 2 linear, retirement, 0.117; employment, 0.067; unemployment, 0.003), c MMSE (R 2 linear retirement, 0.116; employment, 0.214; unemployment, 0.007), d GDS (R 2 linear, retirement, 0.001; employment, 0.042; unemployment, <0.001). Occupational statuses are shown as blue (retirement), green (employed), and red (unemployed) circles
For both genders, performance in all cognitive dimensions decreased with age (Fig. 1a–c). Based on the proportion of variability in the dataset, accounted for by the statistical model (coefficient of determination values, R 2), the percentage of scores explained by age varied between 11.4 % (EXEC, females) and 18.4 % (MMSE, females). Women tended to score lower with age (sharper decline) in the MMSE dimension (Fig. 1c), but not in the EXEC dimension (Fig. 1b), although still presenting lower scores throughout aging. For MEM performance and decline with age appear similar between men and women (Fig. 1a). Furthermore, according to R 2, age does not predict GDS values.
In general, subjects with higher levels of education level performed better in all cognitive dimensions (Fig. 2a–c), although aging was associated with lower performance, irrespective of educational level. Age accounted for lower MEM scores in 51.9 % of subjects with 13+ years of education (r = −0.721, p = 0.029), lower EXEC scores in 11.8 % of subjects with 3–4 years of education (r = −0.343, p < 0.001), and lower MMSE scores in 8.8 % of subjects with 1–2 years of education (r = −0.297, p < 0.05). While higher education was associated with better mood levels (lower GDS values) (Fig. 2d), aging was linked with marked increases in GDS values in the following rank order: 13+ years of education group (R 2 = 27.1 %; r = 0.520; p = 0.151, nonsignificant, probably due to small sample size of nine individuals), 9–12 years (R 2 = 7.9 %, nonsignificant), 5–8 years (R 2 = 3.1 %, nonsignificant), and 3–4 years (R 2 < 1 %, nonsignificant). The percentage of scores explained by age in subjects with <3 years of formal education was negligible.
Occupational status did not have an impact on performance scores in the MEM and EXEC dimensions in any of the age groups (Fig. 3a, b). Retired and employed subjects did not differ in their age-corrected test MMSE scores, but age explained 11.6 % (r = −0.341, p < 0.001) and 21.4 % (r = −0.463, p < 0.001) of the scores in retirees and employees, respectively (Fig. 3c). Retired and employed subjects did not differ in terms of GDS scores; however, depression scores increased prominently with aging in employed subjects (R 2 = 4.2 %, p = 0.032) (Fig. 3d). No significant relationships were noted between age and any of the dimensional test scores in the small group of unemployed subjects within the study population.
Regarding clinical pathology, for the considered variables (gender, education level, and occupational status), renal failure, diabetes, and dyslipidemia were not significantly different between groups (no pathology “No” vs. pathology “Yes”); however, individuals with history of coronary/cardiac disease (insufficiency) or hypertension were significantly older (coronary/cardiac, No, M = 67, SD = 8.80; Yes, M = 72, SD = 8.96, p < 0.001; hypertension, No, M = 65, SD = 9.50; Yes, M = 69, SD = 8.23, p < 0.001) and had significantly less school years (coronary/cardiac, No, M = 4.17, SD = 3.10; Yes, M = 3.25, SD = 2.70, p = 0.023; hypertension, No, M = 4.61, SD = 3.34; Yes, M = 3.62, SD = 2.78, p < 0.001). Regarding physical activity, status (none, less than three times per week, over three times per week, and daily) was not significantly different across each considered variable. Individuals with an exercise activity level of less than three times per week had a significantly higher MEM and EXEC score compared with those with none (p = 0.012 and p = 0.02, respectively), as well as a higher MEM score compared with the daily group (p = 0.034); no other significant differences noted between groups.
Clusters in cognitive performance: the mood dimension differentiates between subclusters
The K-means clustering method was used to identify groups sharing similar characteristics within each of the identified behavioral dimensions. This analysis revealed four distinct clusters (C1 to C4) for each dimension (Fig. 4 and Table 2). Individual clusters within each dimension differed significantly from each other (four ANOVAs, followed by Games–Howell post hoc tests). The different clusters showed the following consistent rank order of performance in all cognitive dimensions: C1 > C2 > C3 > C4, with all clusters differing significantly from one another. In terms of the mood dimension, the C1/C3 and the C2/C4 clusters lay at the two opposite extremes. GDS scores for C1 and C3 did not differ significantly, but differed significantly from both C2 and C4 clusters (Table 2). Subjects in the C2 and C4 clusters displayed higher GDS scores that differed significantly from one another. No significant differences were found between clusters regarding pathology and physical activity status.

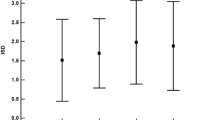
Cluster analysis. Mean performance z-scores by clusters in the MEM, EXEC, MMSE, and GDS dimensions
Clustering with respect to socio-demographic indicators
Whereas men made up the majority of C1 and C3 [males, C1, n = 58 (59 %); C3, n = 71 (60 %)], C2 and C4 were mainly comprised of women [females, C2, n = 66 (62 %); C4, n = 54 (66 %)]. The median ages of each of the four clusters were different (C1, M = 62, SD = 8.00, range 50–79 years; C2, M = 64, SD = 8.68, range 50–84 years; C3, M = 69, SD = 8.25, range 51–86 years; C4, M = 71, SD = 8.52, range 50–88 years). In all clusters the majority of subjects were retired [C1, n = 52 (53 %); C2, n = 69 (65 %); C3, n = 94 (80 %); C4, n = 66 (81 %)]. In respect to school years, clusters were characterized as follows: C1, M = 6.57, SD = 4.09; C2, M = 4.41, SD = 2.54; C3, M = 4.14, SD = 2.11; C4, M = 3.16, SD = 1.26. In all clusters, the majority of subjects belonged to class III (medium stratum) of the Graffar socioeconomic scale (C1, 69.2 %; C2, 59.7 %; C3, 73 %; C4, 59.6 %).
Next, the influence of aging on the various behavioral dimensions was analyzed. The patterns of cognitive performance displayed by each of the four clusters (all cognitive dimensions) were found to remain generally constant during aging (Fig. 5; best performance by C1 > C2 > C3 > C4); however, at 80+ years performance by C4 on the MEM dimension was better than that of C3. With respect to mood, our analysis showed that the GDS score patterns of all clusters did not change significantly with aging (C1 = C3 < C2 < C4). Importantly, growth curves (linear R 2 values) indicated that clustering does not predict MEM, EXEC, MMSE, or GDS values (R 2 close to zero in all cases) (Fig. 5a–d). Lastly, analysis of dispersion (between-individual variability) revealed homogenous variances between the different age categories ([50–60], [60–70], and [70 + ]) in every dimension (Supplementary Fig. 1).

Cluster relationship, according to age, for each identified composite and single dimension. a MEM (R 2 linear, C1, <0.001; C2, 0.031; C3, 0.092; C4, 0.006), b EXEC (R 2 linear C1, <0.001; C2, 0.037; C3, 0.073; C4, 0.089), c MMSE (R 2 linear, C1, 0.006; C2, 0.032; C3, 0.018; C4, 0.049), d GDS (R 2 linear, C1, 0.005; C2, 0.009; C3, 0.051; C4, 0.031). Total fit line is represented in black dotted line (R 2 linear MEM, 0.123; EXEC, 0.122; MMSE, 0.114; GDS, <0.001). Individuals in clusters C1, C2, C3, and C4 are depicted as blue, green, red, and purple circles, respectively
Two binary logistic regression models were used to examine whether one or more socio-demographic characteristics account for delineation between clusters C1 vs. C2 and clusters C3 vs. C4, as well to explore the possible hierarchical importance of the variables (Table 3). Significant logistic regression models were obtained in both cases (C1 vs. C2, χ 2 (5) = 30.3, p < 0.001; C3 vs. C4, χ 2 (5) = 29.0, p < 0.001). In both models, socio-demographic variables were shown to determine cluster membership; Pseudo R 2 Nagelkerke values were ~0.18, indicating that about 20 % of membership of any cluster could be predicted by socio-demographic (independent) variables. Hit rates of 66.3 % for C1 vs. C2 and 63.5 % for C3 vs. C4, indicate that, on the basis of the four independent variables, the models applied provided correct classifications for approximately 67 % of subjects. Gender and number of years of formal education proved to be significant predictors of membership of clusters C1 and C2 and of clusters C3 and C4. Male gender doubled the odds of C1 vs. C2 membership [odds ratio, Exp(B)] and halved the odds of C4 membership. Each year of school attendance increased the odds of C1 membership by approximately 20 % and reduced the odds ratio of C4 membership by 25 %.
Discussion
The present cross-sectional analysis designed, without an a priori hypothesis, to isolate main cognitive and mood dimensions grouped multiple neurocognitive and psychological test variables. Four primary dimensions were identified: memory (MEM) and executive functions (EXEC), mini-mental state (MMSE), and mood (GDS); while the first two dimensions were composites of multiple test variables, the latter two were comprised of single-variable (non-composite) categories (Table 1). For each dimension, basic socio-demographic characteristics (gender, educational level, and occupational status) were explored with respect to the age of individual subjects in order to examine which of these factors might account for observed differences in neurocognitive performance (Figs. 1, 2, 3 and 4).
As expected, there was a significant decline in cognitive performance with increasing age; the decline was found for both genders (Fig. 1), resulting in an age-dependent shift for the entire population (distribution), rather than in large age-related differences in between-subject variability, as measured by dispersion (Fig. 5). The latter was particularly evident after cluster analysis of performance: mean declines were observed in the absence of significant parallel increases in between-subject variability (Fig. 5, Table 3, and Supplementary Fig. 1). As noted by Salthouse et al. (2010a, b), these findings suggest that the mechanisms underlying age-associated cognitive decline lie at the root of entire distribution shifts, with age being a more important covariate than between-subject differences. The present analysis disclosed the significant roles of gender and educational levels, and confirmed our previous observations that education can compensate for gender (Paulo et al. 2011). Here, it is important to note that while education itself might not directly slow general cognitive decline (Zahodne et al. 2011), it most likely acts by facilitating greater independence in aging individuals (Plassman et al. 1995). For example, higher-educated individuals present with lower levels of self-reported disability (Lutz and Kc 2011) and dementia (Ardila 2007). They also have more effective strategies for coping with (Steffener and Stern 2011) and compensating for (Salthouse 2010a, b) normal age-associated changes in memory and executive performance; together, these abilities reduce the social, health, and economic burden of aging (Beddington et al. 2008). Nonetheless, additional factors that are individual-specific may have a differential impact on the breadth of distribution of cognitive scores; for example, dispersion is associated with demographic and health factors (Hilborn et al. 2009). Ongoing collection of data from the present cohort is expected to provide further insights into intra-individual stability of cognition over time.
Analysis of cluster-specific cognitive performance with respect to aging revealed only small linear growth curves for each cluster; in contrast, a significant growth decline (cognitive shift) became evident when all participants were considered as a single group (Fig. 5). Interestingly, mood was found to divide the cognitively better performers into two separate clusters (C1 and C2); mood also distinguished between two types of cognitively weaker performers (C3 and C4) (Figs. 4 and 5). It is important to note that these distinctions were possible only because GDS score was considered as a continuous variable, rather than as a categorical value. Nevertheless, mood alone does not explain a shift in performance from a higher (here, C1 and C2 clusters) to a lower (here, C3 or C4) cognitive level. Our findings are concordant with those of other large longitudinal studies that individuals with persistent depressive episodes are at greater risk for developing cognitive deficits later in life (e.g., Whitehall II study) (Singh-Manoux et al. 2010). Notably, depression in the elderly is associated with poor memory and mental flexibility, as well as with poor scores in other general measures of “crystallized” and “fluid” abilities (Rabbitt et al. 1995). Further, depression is associated with cognitive decline and, in women especially (Yaffe et al. 1999), is a suspect risk factor for conversion to mild cognitive impairment and dementia (Singh-Manoux et al. 2010). Current follow-up investigations are seeking more robust correlations between mood status and rate of cognitive decline; they are also examining how severe persistent depressive symptoms need to be before they have a significant impact on cognitive decline (Paterniti et al. 2002).
The most striking finding in the present work was that lowered mood accelerates decline in cognitive performance and may thus serve to predict stability or deterioration of cognitive performance. Positive mood not only stimulates cognitive capacity and preserves motivation for a lifestyle that is cognitively engaging (Stine-Morrow et al. 2008; Forstmeier and Maercker 2008), but also acts, together with educational level, to prevent transition to negative cognitive status (Minicuci et al. 2005). Indeed, components of mental, social, and physical lifestyle and their interactions are suggested to have a beneficial effect on cognition in elderly participants and to prevent or at least retard dementia (Fratiglioni et al. 2004). The present findings support calls for increased focus on the cognitive and emotional aspects of aging (Depp et al. 2010). Lastly, cognition and mood should be evaluated in elderly participants complaining of cognitive difficulties since lowered mood—shown here to be a continuous variable rather than a systematic categorization—negatively impacts on cognitive performance and the individual’s capacity to better cope with normal, age-related cognitive decline.
References
Ardila A (2007) Normal aging increases cognitive heterogeneity: analysis of dispersion in WAIS-III scores across age. Arch Clin Neuropsychol 22:1003–1011
Ardila A, Ostrosky-Solis F, Rosselli M, Gómez C (2000) Age-related cognitive decline during normal aging: the complex effect of education. Arch Clin Neuropsychol 15:495–513
Beddington J, Cooper CL, Field J, Goswami U, Huppert FA, Jenkins R et al (2008) The mental wealth of nations. Nature 455:1057–1060
Buschke H, Sliwinski M, Kuslansky G, Lipton RB (1995) Aging, encoding specificity, and memory change in the double memory test. J Int Neuropsychol Soc 1:483–493
Depp C, Vahia IV, Jeste D (2010) Successful aging: focus on cognitive and emotional health. Annu Rev Clin Psychol 6:527–550
Folstein MF, Folstein SE, McHugh PR (1975) Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Forstmeier S, Maercker A (2008) Motivational reserve: lifetime motivational abilities contribute to cognitive and emotional health in old age. Psychol Aging 23:886–899
Fratiglioni L, Paillard-Borg S, Winblad B (2004) An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurol 3:343–353
Graffar M (1956) Une methode de classification sociale d'echantillon des populations. Courrier 6:455–459
Harvey PD, Reichenberg A, Bowie CR (2006) Cognition and aging in psychopathology: focus on schizophrenia and depression. Annu Rev Clin Psychol 2:389–409
Hilborn JV, Strauss E, Hultsch DF, Hunter MA (2009) Intraindividual variability across cognitive domains: investigation of dispersion levels and performance profiles in older adults. J Clin Exp Neuropsychol 31:412–424
Lezak M, Howieson D, Loring D (2004) Neuropsychological assessment. Oxford University Press, New York
Lutz W, Kc S (2011) Global human capital: integrating education and population. Science 333:587–592
Minicuci N, Marzari C, Maggi S, Noale M, Senesi A, Crepaldi G (2005) Predictors of transitions in vitality: the Italian longitudinal study on aging. J Gerontol A Biol Sci Med Sci 60A:566–573
OECD (2012) Country statisticial profile–Portugal. Available from: http://dx.doi.org/10.1787/csp-prt-Table-2011-1-en doi:10.1787/csp-prt-table-2011-1-en
Paterniti S, Verdier-Taillefer MH, Dufouil C, Alpérovitch A (2002) Depressive symptoms and cognitive decline in elderly people: longitudinal study. Br J Psychiatry 181:406–410
Paulo AC, Sampaio A, Santos NC, Costa PS, Cunha P, Zihl J et al (2011) Patterns of cognitive performance in healthy ageing in northern Portugal: a cross-sectional analysis. PLoS One 6:e24553
Plassman BL, Welsh KA, Helms M, Brandt J, Page WF, Breitner JC (1995) Intelligence and education as predictors of cognitive state in late life: a 50-year follow-up. Neurology 45:1446–1450
Rabbitt P, Donlan C, Watson P, McInnes L, Bent N (1995) Unique and interactive effects of depression, age, socioeconomic advantage, and gender on cognitive performance of normal healthy older people. Psychol Aging 10:307–313
Salthouse TA (2010a) Does the meaning of neurocognitive change change with age? Neuropsychology 24:273–278
Salthouse TA (2010b) Selective review of cognitive aging. J Int Neuropsychol Soc 16:754–760
Singh-Manoux A, Akbaraly TN, Marmot M, Melchior M, Ankri J, Sabia S et al (2010) Persistent depressive symptoms and cognitive function in late midlife: the Whitehall II study. J Clin Psychiatry 71:1379–1385
Steffener J, Stern Y (2011) Exploring the neural basis of cognitive reserve in aging. Biochim Biophys Acta 1822:467–473
Stern Y (2009) Cognitive reserve. Neuropsychologia 47:2015–2028
Stine-Morrow EAL, Parisi JM, Morrow DG, Park DC (2008) The effects of engaged lifestyles on cognitive vitality: a field experiment. Psychol Aging 23:778–786
Strauss E, Sherman EMS, Spreen O (2006) A compendium of neuropsychological tests: administration, norms and commentary. Oxford University Press, New York
Wechsler D (1997) Wechsler adult intelligence scale (WAIS-III). Harcourt Assessment, San Antonio
Yaffe K, Blackwell T, Gore R, Sands L, Reus V, Browner WS (1999) Depressive symptoms and cognitive decline in nondemented elderly women: a prospective study. Arch Gen Psychiatry 56:425–430
Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M et al (1983) Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res 17:37–49
Zahodne LB, Glymour MM, Sparks C, Bontempo D, Dixon RA, MacDonald SW et al (2011) Education does not slow cognitive decline with aging: 12-year evidence from the Victoria longitudinal study. J Int Neuropsychol Soc 17:1039–1046
Acknowledgments
This work was funded by the European Commission (FP7) “SwitchBox” (Contract HEALTH-F2-2010-259772). NCS is supported by a SwitchBox post-doctoral fellowship. We are thankful to all study participants. The authors would like to acknowledge all colleagues who assisted with participant recruitment and evaluation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Nadine Correia Santos and Patrício Soares Costa contributed equally in the authorship and should be listed as co-first authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 239 kb)
About this article
Cite this article
Santos, N.C., Costa, P.S., Cunha, P. et al. Mood is a key determinant of cognitive performance in community-dwelling older adults: a cross-sectional analysis. AGE 35, 1983–1993 (2013). https://doi.org/10.1007/s11357-012-9482-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11357-012-9482-y