
Abstract
Economic losses due to health-related implications of air pollution were huge and incurred significant burdens towards healthcare providers. The objective of this study is to systematically review published literature on the financial implications of air pollution on health in Asia. Four databases: PubMed, Scopus, NHS Economic Evaluation Database (NHS EED), and Web of Science (WoS) were used to identify all the relevant articles. It was limited to all articles that had been published in the respected databases from January 2007 until March 2017. Twenty-four articles were included in this review. Five of the 24 studies (20.8%) reported financial implications of air pollution-related disease through value of statistical life (VOSL) which ranged from USD180 million to USD2.2 billion, six (25%) studies used cost of illness (COI) to evaluate air pollution-related morbidity and found that the cost ranged from USD5.4 million to USD9.1 billion. Another six studies (25%) used a combination of VOSL and COI for both mortality and morbidity valuation and found that the financial implications ranging from USD253 million to USD2.9 billion. Thirteen (54.2%) studies reported healthcare cost associated with both hospital admission and outpatient visit, five (20.1%) on hospital admission only, and one (4.2%) on outpatient visit only. Economic impacts of air pollution can be huge with significant deterioration of health among the Asians.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rapid urbanization, together with the dramatic increase in population density especially in the urban area is commonly associated with the deterioration of air quality (Abdullah et al. 2012). Air pollution occurs as a result of increased particulate matter (PM) level, and greenhouse gases that are released into the atmosphere, exceeding their normal levels (Razak et al. 2013). Exposure to air pollution results in significant health effects which is associated with increased healthcare utilization rate. Numerous studies had been done to show the association between the pollution level, especially PM and healthcare utilization. Although there were variations in the results due to differences in the geographical locations, seasonal trends and chemical compositions of the pollutants, majority of the studies agreed that there was a significant increase in healthcare utilization rate with every increase in the unit of the pollutant level (Kochi et al. 2009; Anderson et al. 2012; Atkinson et al. 2014). Increase in healthcare utilization rate will subsequently lead to increase in healthcare cost and expenditure. Economic losses due to health-related implications of air pollution were huge and incur substantial burden to the healthcare providers (Kochi et al. 2010; Othman et al. 2014). Majority of Asian countries are still developing and the rapid urbanization and industrial activities together with sudden surge of population density in major cities (especially in China) were the main contributors towards the deterioration of air quality level. On top of that, without the evidence-based estimation that specifically focused on the economic burden of air pollution towards Asian countries, it is difficult to convince the policy makers to allocate enough resources for mitigation plan to improve air quality level to take place.
The objective of this study is to systematically review published literatures on the financial implications of air pollution on health in Asia. The financial implications of health effects from air pollution were related to 1) increase in healthcare utilization and 2) reduce productivity due to work absenteeism. Although many studies had been conducted to determine the financial implications of air pollution on health, only few studies did a systematic review on this particular topic. To our knowledge, no systematic review has been published on the financial burden of air pollution on health in the Asian region. Due to the variation in terms of climate, population background, and sociodemographic factors compared to other continents like Europe and America, this review is important to provide a clear view on the financial implications of air pollution on health among the Asian countries. In addition, this study will provide the evidence-based estimate of healthcare utilization and its financial implications due to air pollution so that steps can be taken to combat the situation as well as to allocate appropriate resources to meet the healthcare demand associated with air pollution.
Methods
Literature search
A thorough and systematic literature search strategy was done using the traditional search and citation forward and backward tracking (snowballing). Four databases: PubMed, Scopus, NHS Economic Evaluation Database (NHS EED), and Web of Science (WoS) were used to identify all the relevant articles. The literature search was done using specific keywords and identified MeSH terms (for PubMed) in April 2017. It was limited to all articles that had been published in the respected databases from January 2007 until March 2017. A full detail on the search strategy is available in Appendix. This study was also registered with PROSPERO (CRD42017076150) on 13 December 2017.
Inclusion and exclusion criteria
This review includes all the relevant articles that cover the economic evaluation of air pollution in the Asian region that were published in English language and within the specified time period. A ten-year period from 2007 to 2017 was chosen in view of the heterogeneities of the pattern of air pollution in Asia that were influent by the different climates, environmental factors, and sociodemographic backgrounds. Articles that reported on indoor air pollution or mixed pollution (e.g., noise and air), review papers, chapter in books, proceedings, or policy papers were excluded. We also excluded articles that were not health related or did not include economic evaluation.
Data extraction
Data extractions were done by three authors (HJ, NAR, AA). The titles and abstracts of articles were screened, and the relevant information was summarized in the evidence table. The table included the authors’ name and year of publication, pollution year, pollution index used, health outcomes, study settings, methods of costing analysis, and results. Any disagreement between the three authors over the eligibility of particular studies was resolved through discussions with a fourth and fifth authors (MI, MD). Further analysis and quality assessment of the selected articles were done by all authors (HJ, NAR, AA, MI, MD). All costs in the reviewed articles were converted into US dollar (USD), and were inflated to the year 2016 by using the purchasing power parities (USD PPP) to reduce heterogeneity and ensure that all data were comparable (OECD 2017; X-Rates 2017).
Quality assessment
The methodological quality of economic evaluation of all the articles included in this study was assessed using the Consensus on Health Economic Criteria (CHEC) list, a checklist developed by Evers et al. (2005). CHEC is commonly used to critically appraise published studies on economic evaluations. It consists of 19 criteria, including the standard elements in reporting an economic evaluation study (study population, competing alternatives, time horizon, study perspective, discount rate, incremental analysis, sensitivity analysis), cost and outcome identification and valuation, discussions on generalizability of the study result, conclusion, ethical issues as well as the potential of conflicts of interest. Each criterion present in the articles was marked as “Yes” and given one mark. The scores were then summed up to obtain the total score for each article. The number of criteria present in all the articles was also calculated to generate an overview of the overall economic evaluation quality.
Results and discussion
Search results
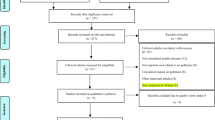
The initial systematic literature search from four databases had retrieved 2095 articles. There were 714 articles from PubMed, 201 from Scopus, 337 from WoS, and 843 from NHS. After all the articles from these databases were merged, 172 duplicates were removed. The title and abstract screening was done to the remaining 1923 articles, but only 163 articles were found to be relevant and had been considered. In addition, we found that 104 articles which were published beyond the specified time period and had to be excluded. A full text screening was done on the remaining 59 articles. There were 35 articles which did not fulfill the inclusion and exclusion criteria (not in Asian region, indoor air pollution, mixed pollution, not health related, not economic evaluation paper, review papers, proceeding papers, and policy papers) were also excluded. A total of 24 articles were finally considered and included in this review. The flow chart of the systematic literature search is summarized in Fig. 1.

Flow chart of study selection (PRISMA flowchart)
General characteristics
Overall, the most recent articles were published in 2017 (Etchie et al. 2017; Maji et al. 2017; Shen et al. 2017) and the oldest article was in 2007 (Chen et al. 2007). The reported years for air pollution ranged from 1991 (Maji et al. 2017) to 2015 (Li et al. 2016; Maji et al. 2017; Shen et al. 2017), with the projections based on regression modeling made for 2020 (Chen et al. 2007) and 2030 (Othman et al. 2014; Xie et al. 2016). Majority of the studies (n = 14, 58.3%) were conducted in China, followed by India (n = 4, 16.7%) and one each for Taiwan, Hong Kong, South Korea, Bangladesh, Malaysia, and Iran. All studies used PM (PM10, PM2.5, or both) as their main pollution index, with six studies also including CO, nitrogen dioxide (NO2), sulfur dioxide (SO2), and ozone (O3) as the other measured pollutants.
Out of the 24 studies, 18 studies (75%) included premature mortality attributed to air pollution as their health outcome. All studies in this review except for Wadud and Khan (2013) and Lee et al. (2010) used respiratory related illnesses as their morbidity outcome. Another 16 studies (66.7%) assessed the cardiovascular related illnesses, while four studies (16.7%) included cerebrovascular accident as their health outcome. There were 13 (54.2%) studies that reported costs associated with both hospital admission and outpatient visit, five studies (20.1%) on hospital admission only, and one study (4.2%) on outpatient visit only.
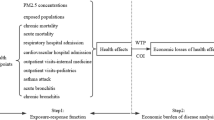
In this systematic review, we found that the common methods used to estimate the economic implications of haze-related mortality was the value of statistical life (VSL/VOSL) through willingness to pay (WTP) or human capital/amended human capital approach (HC/AHC). On the other hand, the economic impacts of haze-related morbidity were assessed via costs of illness (COI) and WTP (using contingent valuation method, CVM) approaches. With the exception of Hou et al. (2016), Hou et al. (2014), and Yin et al. (2015) who used AHC as their costing analysis for the mortality outcomes, other studies used VSL/VOSL as the measurement tools for costs associated with mortality attributed to air pollution. About 13 studies (54.2%) used COI approach and three studies (12.5%) used WTP approach to measure various morbidity outcomes. Two studies used exposure-response function based on computable general equilibrium (CGE) model to estimate labor loss and excess medical costs (Wang et al. 2016), and to measure the macroeconomics impacts based on additional health expenditure, total work loss, and health end points (Xie et al. 2016). There were 16 (66.7%) studies that used existing data from previous literatures as their main references for the economic unit values; especially costing that was associated with mortality assessment.
Economic burden, mortality, and morbidity valuation
The economic burden reported by articles included in this systematic review varies, depending on the method used to evaluate the haze-related impacts on morbidity and mortality. Five studies used VOSL as their outcome with the cost ranging from USD180 million to USD2.2 billion (Lee et al. 2011; Wadud and Khan 2013; Tang et al. 2014; Du and Li 2016; Etchie et al. 2017). Etchie et al. (2017) predicted that there would be an economic gain of USD1.1 billion in 2043 following the reduction of premature mortality due to air pollution episodes when mitigation measures were taken to reach the WHO air-quality standard. Meanwhile, Tang et al. (2014) and Wadud and Khan (2013) estimated an economic gain of USD596 million and USD409 million, respectively due to the reduction of VOSL loss from air pollution abatement and mitigation plans.
Six studies used COI to estimate the financial impacts of air pollution-related morbidity. The cost of impacts calculated using this method ranged from USD5.4 million to USD9.1 billion (Hedley et al. 2008; Sun et al. 2013; Othman et al. 2014; Wang et al. 2014; Kumar et al. 2016; Shen et al. 2017). Wang et al. (2014) revealed that the cost of hospital admission during the Asian dust storm (ADS) rose daily from USD 21,123 to USD 26,206 compared to non-ADS day, while Othman et al. (2014) and Wang et al. (2014) revealed that there was an economic loss of USD 4471 recorded per hazy day due to loss of productivity estimated based on patient’s average daily or monthly wages.
A more holistic approach to measure the economic burden of air pollution on health is to include both mortality and morbidity assessment through (i) VOSL and COI, (ii) VOSL and WTP, (iii) AHC and WTP, and (iv) AHC and COI approaches. Six studies included VOSL and COI, and found that the economic burden ranged from USD253 million to USD2.9 billion (Karimazadegan et al. 2008; Zhang et al. 2008; Gao et al. 2015; Lu et al. 2016; Maji et al. 2016, 2017). Li et al. (2016) recorded a total economic loss ranging from USD46.9 billion to USD66.4 billion by using VOSL and WTP approaches. The assessment of economic burden using a combination of AHC and WTP approaches by Hou et al. (2014) showed an economic loss of USD106.5 billion, while Hou et al. (2016) and Yin et al. (2015) who applied the AHC and COI approaches showed a total economic loss of USD10.4 billion and USD31.2 billion, respectively.
Quality analysis using CHEC
The results of methodological quality assessment are shown in Table 1. Out of 24 studies, none managed to get a full CHEC score. The highest score was 17, obtained by Xie et al. (2016), whose study fulfilled 17 out of 19 criteria listed in the CHEC scoring. The lowest score was ten, which were obtained by six articles. Almost all the articles (n = 23, 95.8%) described the study population well; however, only few studies delineated the competing alternatives in their studies (n = 10, 41.7%) and posed well-defined research questions (n = 15, 62.5%). Most of the authors (n = 14, 58.3%) also did not clearly identify the alternatives being compared in their studies. Less than half of the studies (n = 11, 45.8%) used an appropriate study design with full economic evaluation that compares the costs and effects of two or more interventions based on primary research. The majority did their study in an appropriate time horizon (n = 23, 95.8%) and actual perspective (n = 17, 70.8%). Despite not being mentioned explicitly, many of the studies were performed from a societal perspective, while others (n = 7, 29.2%) considered the provider’s perspective. All studies reported a clear cost and outcome components, and how they were measured. Future cost and outcome discounting were done by most of the studies (n = 21, 87.5%) except three studies which did not report any discount rate. Out of 24 studies, only one study (0.04%) by Xie et al. (2016) performed incremental analysis. Nine studies (37.5%) had appropriately subjected important variables with uncertain values to sensitivity analysis. Less than half of the studies discussed the generalizability of their results to other settings (n = 11, 45.8%). Nonetheless, except from Etchie et al. (2017), all authors concluded their studies precisely according to the data reported. Lastly, very few authors (n = 7, 29.2%) elaborated the ethical aspects and the characteristics of population having the disease, which may give important information to the policy makers in making decisions for the pollution-related health issues.
Discussion
Overall, there were 22 articles which used respiratory symptoms and illnesses as the main health outcomes, with 16 articles including cardiovascular system (CVS) illnesses, and four articles including CVA as the other outcomes. The health impacts of air pollution are more prominent in respiratory system compared to CVS and CVA. The healthcare utilization related to CVA and CVS illnesses was mainly inpatient cases rather than outpatient, as most of the conditions required patients to be admitted for further monitoring and assessments.
In contrast, utilization of healthcare facilities due to respiratory illnesses involved both inpatient and outpatient cases and resulted in substantial financial burden to the healthcare system. Exposure to air pollution can cause immediate impact towards respiratory systems thus making it easier for the researchers to attribute the episode of attack to air pollution (Adar et al. 2014; Sahani et al. 2014). The main reasons for outpatient visits and hospital admissions were asthmatic attack, acute exacerbation of chronic obstructive pulmonary disease (AECOPD), acute bronchitis, pneumonia, and bronchiolitis (in infants), with exacerbation of asthma and COPD accounting for majority of the cases (Peacock et al. 2011; Anderson et al. 2012; Mehta et al. 2013; Laumbach and Kipen 2014). This explains why most of the studies took respiratory illnesses as their main health outcome to determine the financial impact of air pollution on health.
Majority of the studies also looked at premature mortality as the other parameter to evaluate economic burden attributed to air pollution. Premature mortality can be due to respiratory cause or natural cause. Premature mortality due to respiratory causes responsible for an immediate mortality impact (one to 2 days after exposure to air pollution) usually occurred among those with underlying respiratory illnesses such as asthma and COPD (Sahani et al. 2014). As for the natural causes, it usually occurs 2 to 5 days following exposure to air pollution and affects vulnerable groups such as young children, elderly, pregnant ladies, and those from low socioeconomic status (Sahani et al. 2014). Based on the summary listed in Table 2, we can see that the economic loss due to premature mortality was huge, and incurred higher cost compared to hospital admission and outpatient visit, and should be considered as an important outcome in measuring health and economic burden associated with air pollution.
Almost half of the studies in this review were conducted in China. As one of the biggest countries with high population density, air pollution is a major problem for China. Rapid urbanization, fast-growing industrial and manufacturing activities together with other ecological factors worsened the air quality especially in their major cities like Shanghai and Beijing (Li et al. 2016). The financial implication due to air pollution is a major concern to their government. In the healthcare sector, the medical cost increased by USD1 billion with every 10 μg m−3 increase in PM2.5 concentration, with the total medical cost attributed to air pollution ranging from USD2.8 billion to USD9.1 billion (approximately 1.1% of total national health expenditure in 2014) (Shen et al. 2017). China also recorded a huge amount of Gross Domestic Product (GDP) loss of USD209 million due to labor loss and excess medical expenses, and societal output loss of USD 656 million due to air pollution (Wang et al. 2016). Therefore, plans are needed to reduce the air pollution impact. Most of the studies in China projected the economic gain by introducing mitigating and averting plan to achieve better air quality standard (Chen et al. 2007; Sun et al. 2013). A study by Xie et al. (2016) found that without any mitigation plan, the healthcare cost associated with air pollution would be USD25.2 billion (0.11% of GDP) in 2030 compared to only USD6.5 billion (0.027% of GDP) if mitigation plans were implemented. In another study by Tang et al. (2014), improvement in total VOSL loss were recorded in Taiyuan, China from USD1.1 billion in 2001 to USD504 million in 2010 after the implementation of the air pollution abatement policy in 2001.
In this review, VOSL is the most common method used to evaluate the monetary value of preventing mortalities. It can be determined either through WTP approach or HC approach. All studies in this review, except by Hou et al. (2014), Hou et al. (2016), and Yin et al. (2015), used WTP to determine VOSL in their study population. Previously, HC approach was widely used to measure VOSL because it is clear and simple, its data can be obtained easily which could save time to complete the research. Nevertheless, a few disadvantages limit the applicability of HC nowadays, as it could not give a true reflection on the medical costs due to specific illnesses; no individual validation was done; and the studies also ignored those that were not part of the labor force such as pensioners and unemployed persons. These limitations explain why most of the studies used WTP approach since it is more holistic as the value of life is determined based on the individual’s willingness to pay to reduce the risk of dying. Apart from that, WTP is also preferred due to the availability of data from previous literatures that can be used to measure the economic impact of premature mortality attributed to air pollution.
As for the morbidity assessment, there were 13 studies which used COI approach to estimate the economic impact of air pollution on health. The costs measured were direct medical cost, direct non-medical cost, and indirect cost. Estimation of economic burden based on COI approach is more conservative, and usually has lower cost estimation compared to using the WTP approach. Nevertheless, many researchers opted for this approach as most of the information needed to calculate the cost was readily available from published literatures and financial reports by healthcare providers. In addition, COI can also be used to estimate WTP value based on the widely used WTP/COI ratio of two or three (Kochi et al. 2009). In addition, most of the economic evaluation studies on the health impact of air pollution were focusing mainly on the morbidity and healthcare utilization due to the illnesses. Consideration and focus should also be given to the loss of productivity as the consequent of the illnesses caused or aggravated by air pollution.
Quality assessment
CHEC score was used as the quality assessment for the selected articles. The essential parts of costing techniques were expected to be present and included in the studies. Most of the articles described the study population clearly and used appropriate time horizon to include all relevant costs and outcomes. The methods and valuation techniques used to measure all the costs and outcomes were also clearly stated and described in majority of them. Almost all articles also did an appropriate discounting by converting all the costs and outcomes to a single year. These are all the basic components of doing an economic evaluation study. Fulfilling these criteria is a good indication that the researchers were familiar with the fundamental aspects of their research, and managed to produce a good quality outcome from their study (Evers et al. 2005).
On the other hand, mixed results were seen in other components of the CHEC list. Some studies did not include the assessment of competing alternatives or interventions. Since their outcomes were mainly descriptive, no comparison of costs was made. On top of that, the perspective of study which determined the point of view that economic evaluation study was done is also important. The best way is to perform the study from a societal perspective. However, some studies only performed their evaluations from a provider’s perspective due to time and budget constraints. Another important component in the CHEC list is the sensitivity analysis. Surprisingly, almost half of the studies in this review did not undergo this step, thus reducing the validity of their results and findings. Variations of results were also seen in few other criteria such as the generalizability of results, the potential conflict of interest with funders, and also the ethical issues related to the studies. Some studies mentioned these issues explicitly while others did not. These issues relate more to the technical aspect of the research process itself rather than the quality aspect of the methodology used in the evaluation study (Evers et al. 2005).
Strengths and limitations of the review
To our knowledge, this is the first systematic review on the financial implications of air pollution on health that is focusing on studies from the Asian region. With different climates and sociodemographic backgrounds from the American and European regions, this review provides good information to reflect on the exact burden and scenarios that occurred in the Asian region. The results from this study were also in line and supported with the findings from previous literatures that described explicitly on the significant financial burden of air pollution on health. The results from this study were similar to previous literatures (Kochi et al. 2009, 2010) that found economic evaluations that used WTP as the outcome reported higher financial burden other than studies that used different economic outcomes. It is because WTP included costs for other intangible factors such as the cost of leisure time affected or the absence of pain and suffering in addition to the direct and indirect medical costs (Goodchild et al. 2018).
In addition, this review also has a good coverage of years, and extensive keywords were used for article searching to ensure that all relevant articles for the past 10 years had been included.
Nevertheless, the exclusion of non-English articles limits our findings since some articles from Asia were written in their native languages. On top of that, a few economic evaluation studies were not in the form of journal articles and thus, were not included in our review. We might have missed the information from these studies despite their interesting and important findings. Furthermore, the results obtained from a few studies included in this review were not really comparable to each other based on several factors. These factors include the methods of economic evaluation, type of costing analysis, the population involved, the coverage areas, as well as the different healthcare system used in each country.
Conclusion
In conclusion, this review provides an extensive evaluation on the financial impact of air pollution on health, specifically for the Asian countries. From the review, it is shown that air pollution is indeed one of the major concerns in the Asian region, especially among the healthcare providers due to its huge economic impacts from the significant deterioration of health quality among the Asians. Nevertheless, the qualities of the economic evaluation studies need to be improved so that the results could be more robust and reliable. This is important as the evaluations and projections of financial implications can be used by the policy makers to plan for strategic mitigating measures that need to be taken in order to reduce the level of air pollution in the future. The economic benefit of legislating and promulgating environmental policy and laws that reduces air pollution will help to reduce the healthcare costs and expenditures related to this problem especially in Asia.
References
Abdullah AM, Abu Samah MA, Jun TY (2012) An overview of the air pollution trend in Klang Valley, Malaysia. Open Environ Sci 6:13–19. https://doi.org/10.2174/1876325101206010013
Adar SD, Filigrana PA, Clements N, Peel JL (2014) Ambient coarse particulate matter and human health: a systematic review and meta-analysis. Curr Environ Heal reports 1:258–274. https://doi.org/10.1007/s40572-014-0022-z
Anderson JO, Thundiyil JG, Stolbach A (2012) Clearing the air: a review of the effects of particulate matter air pollution on human health. J Med Toxicol 8:166–175. https://doi.org/10.1007/s13181-011-0203-1
Atkinson RW, Kang S, Anderson HR, Mills IC, Walton HA (2014) Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: a systematic review and meta-analysis. Thorax 69:660–665. https://doi.org/10.1136/thoraxjnl-2013-204492
Chen C, Chen B, Wang B, Huang C, Zhao J, Dai Y, Kan H (2007) Low-carbon energy policy and ambient air pollution in Shanghai, China: a health-based economic assessment. Sci Total Environ 373:13–21. https://doi.org/10.1016/j.scitotenv.2006.11.030
Du Y, Li T (2016) Assessment of health-based economic costs linked to fine particulate (PM2.5) pollution: a case study of haze during January 2013 in Beijing, China. Air Qual Atmos Heal 9:439–445. https://doi.org/10.1007/s11869-015-0387-7
Etchie TO, Sivanesan S, Adewuyi GO et al (2017) The health burden and economic costs averted by ambient PM2.5 pollution reductions in Nagpur, India. Environ Int 102:145–156. https://doi.org/10.1016/j.envint.2017.02.010
Evers S, Goossens M, De Vet H, Van Tulder M (2005) Criteria list for assessment of methodological quality of economic evaluations: consensus on health economic criteria criteria list for assessment of methodological quality of economic evaluations. Int J Technol Assess Health Care 21:240–245. https://doi.org/10.1017/S0266462305050324
Gao M, Guttikunda SK, Carmichael GR, Wang Y, Liu Z, Stanier CO, Saide PE, Yu M (2015) Health impacts and economic losses assessment of the 2013 severe haze event in Beijing area. Sci Total Environ 511:553–561. https://doi.org/10.1016/j.scitotenv.2015.01.005
Goodchild M, Nargis N, D’Espaignet ET (2018) Global economic cost of smoking-attributable diseases. Tob Control 27:58–64. https://doi.org/10.1136/tobaccocontrol-2016-053305
Hedley AJ, Mcghee SM, Barron B et al (2008) Air pollution: costs and paths to a solution in Hong Kong — understanding the connections among visibility, air pollution, and health costs in pursuit of accountability, environmental justice, and health protection air pollution: costs and paths to. J Toxicol Environ Heal Part B 71:544–554. https://doi.org/10.1080/15287390801997476
Hou Q, An X, Wang Y, Tao Y, Sun Z (2014) An assessment of China’s PM10-related health economic losses in 2009. Sci Total Environ 435–436:61–65. https://doi.org/10.1016/j.scitotenv.2012.06.094
Hou Q, An X, Tao Y, Sun Z (2016) Assessment of resident’s exposure level and health economic costs of PM10 in Beijing from 2008 to 2012. Sci Total Environ 563-564:563–564. https://doi.org/10.1016/j.scitotenv.2016.03.215
Karimazadegan H, Rahmatian R, Farhud DD, Yunesian M (2008) Economic valuation of air pollution health impacts in the Tehran area, Iran. Iran J Public Health 37:20–30
Lee YJ, Lim YW, Yang JY, Kim CS, Shin YC, Shin DC (2010) Evaluating the PM damage cost due to urban air pollution and vehicle emissions in Seoul, Korea. J Environ Manag 92:603–609. doi: https://doi.org/10.1016/j.jenvman.2010.09.028
Kochi I, Loomis J, Champ P, Donovan G (2009) Health and economic impact of wildfires: literature review and impact assessment. In: González-Cabán A (ed) 3rd international symposium on fire economics, planning, and policy: common problems and approaches. Colarado, United States of America, pp 1–14
Kochi I, Donovan GH, Champ PA, Loomis JB (2010) The economic cost of adverse health effects from wildfire-smoke exposure: a review. Int J Wildl Fire 19:803–817. https://doi.org/10.1071/WF09077
Kumar A, Gupta I, Brandt J, Kumar R, Dikshit AK, Patil RS (2016) Air quality mapping using GIS and economic evaluation of health impact for Mumbai City, India. J Air Waste Manag Assoc 66:470–481. https://doi.org/10.1080/10962247.2016.1143887
Laumbach RJ, Kipen HM (2014) Respiratory health effects of air pollution: update on biomass smoke and traffic pollution. J Allergy Clin Immunol 129:3–11. https://doi.org/10.1016/j.jaci.2011.11.021
Lee YJ, Lim YW, Yang JY, Kim CS, Shin YC, Shin DC (2011) Evaluating the PM damage cost due to urban air pollution and vehicle emissions in Seoul, Korea. J Environ Manag 92:603–609. https://doi.org/10.1016/j.jenvman.2010.09.028
Li L, Lei Y, Pan D, Yu C, Si C (2016) Economic evaluation of the air pollution effect on public health in China’s 74 cities. Springerplus 5:1–16. https://doi.org/10.1186/s40064-016-2024-9
Lu X, Yao T, Fung JCH, Lin C (2016) Estimation of health and economic costs of air pollution over the Pearl River Delta region in China. Sci Total Environ 566–567:134–143. https://doi.org/10.1016/j.scitotenv.2016.05.060
Maji KJ, Dikshit AK, Deshpande A (2016) Disability-adjusted life years and economic cost assessment of the health effects related to PM2.5 and PM10 pollution in Mumbai and Delhi, in India from 1991 to 2015. Environ Sci Pollut Res 24:4709–4730. https://doi.org/10.1007/s11356-016-8164-1
Maji KJ, Dikshit AK, Deshpande A (2017) Assessment of city level human health impact and corresponding monetary cost burden due to air pollution in India taking Agra as a model city. Aerosol Air Qual Res 17:831–842. https://doi.org/10.4209/aaqr.2016.02.0067
Mehta S, Shin H, Burnett R, North T, Cohen AJ (2013) Ambient particulate air pollution and acute lower respiratory infections: a systematic review and implications for estimating the global burden of disease. Air Qual Atmos Heal 6:69–83. https://doi.org/10.1007/s11869-011-0146-3
OECD (2017) Consumer price annual inflation. Organ. Econ. Coop. Dev, In https://stats.oecd.org/index.aspx?queryid=22519#. Accessed 21 Nov 2017
Othman J, Sahani M, Mahmud M, Sheikh Ahmad MK (2014) Transboundary smoke haze pollution in Malaysia: inpatient health impacts and economic valuation. Environ Pollut 189:194–201. https://doi.org/10.1016/j.envpol.2014.03.010
Peacock JL, Anderson HR, Bremner SA, Marston L, Seemungal TA, Strachan DP, Wedzicha JA (2011) Outdoor air pollution and respiratory health in patients with COPD. Thorax 66:1–7. https://doi.org/10.1136/thx.2010.155358
Razak MI, Ahmad I, Bujang I et al (2013) Economics of Air Pollution in Malaysia 3:173–177
Sahani M, Zainon NA, Wan Mahiyuddin WR, Latif MT, Hod R, Khan MF, Tahir NM, Chan CC (2014) A case-crossover analysis of forest fire haze events and mortality in Malaysia. Atmos Environ 96:257–265. https://doi.org/10.1016/j.atmosenv.2014.07.043
Shen Y, Wu Y, Chen G, van Grinsven HJM, Wang X, Gu B, Lou X (2017) Non-linear increase of respiratory diseases and their costs under severe air pollution. Environ Pollut 224:1–7. https://doi.org/10.1016/j.envpol.2017.02.047
Sun Z, An X, Tao Y, Hou Q (2013) Assessment of population exposure to PM10 for respiratory disease in Lanzhou (China) and its health-related economic costs based on GIS. BMC Public Health 13:891–890. https://doi.org/10.1186/1471-2458-13-891
Tang D, Wang C, Nie J, Chen R, Niu Q, Kan H, Chen B, Perera F (2014) Health benefits of improving air quality in Taiyuan, China. Environ Int 73:235–242. https://doi.org/10.1016/j.envint.2014.07.016
Wadud Z, Khan T (2013) Air quality and climate impacts due to CNG conversion of motor vehicles in Dhaka, Bangladesh. Environ Sci Technol 47:13907–13916. https://doi.org/10.1021/es402338b
Wang C-H, Chen C-S, Lin C-L (2014) The threat of Asian dust storms on asthma patients: a population-based study in Taiwan. Glob Public Health 9:1040–1052. https://doi.org/10.1080/17441692.2014.951871
Wang G, Gu S, Chen J, Wu X, Yu J (2016) Assessment of health and economic effects by PM2.5 pollution in Beijing: a combined exposure–response and computable general equilibrium analysis. Environ Technol (United Kingdom) 37:3131–3138. https://doi.org/10.1080/09593330.2016.1178332
Xie Y, Dai H, Dong H, Hanaoka T, Masui T (2016) Economic impacts from PM 2.5 pollution-related health effects in China: a provincial-level analysis. Environ Sci Technol 50:4836–4843. https://doi.org/10.1021/acs.est.5b05576
X-Rates (2017) Currency calculator. X-Rates, In http://www.x-rates.com/. Accessed 21 Nov 2017
Yin H, Xu L, Cai Y (2015) Monetary valuation of PM10-related health risks in Beijing China: the necessity for PM10 pollution indemnity. Int J Environ Res Public Health 12:9967–9987. https://doi.org/10.3390/ijerph120809967
Zhang M, Song Y, Cai X, Zhou J (2008) Economic assessment of the health effects related to particulate matter pollution in 111 Chinese cities by using economic burden of disease analysis. J Environ Manag 88:947–954. https://doi.org/10.1016/j.jenvman.2007.04.019
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Nicholas Apergis
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Jaafar, H., Razi, N.A., Azzeri, A. et al. A systematic review of financial implications of air pollution on health in Asia. Environ Sci Pollut Res 25, 30009–30020 (2018). https://doi.org/10.1007/s11356-018-3049-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-018-3049-0