
Abstract
This study was undertaken to determine the association of four chlorophenol pesticides with cardiometabolic risk factors and obesity in children and adolescents. This cross-sectional study was conducted in 2016 on 242 children and adolescents, aged 6 to 18 years. The concentrations of 2,4-dichlorophenol (2,4-DCP), 2,5-dichlorophenol (2,5-DCP), 2,4,5-trichlorophenol (2,4,5-TCP), and 2,4,6-trichlorophenol (2,4,6-TCP) in the urine were examined and their association with indices of obesity and cardiometabolic risk factors was determined. Multivariate linear regression and multinomial logistic regression analyses were applied. Overall, 242 participants with mean (SD) ages of 11.3 (2.5) years completed the survey. After adjustment for confounders, a significant positive association was found between body mass index (BMI) z-score and waist circumference (WC) with 2,5-DCP (0.07 (95% CI 0.04, 0.1)) and 0.79 (95% CI 0.54, 1.03), respectively. A significant association of 2,4,5-TCP was only found with WC (0.23 (95% CI 0.0, 0.46), but the relationship with 2,4-DCP was not significant. 2,5-DCP had a significant relationship only with obesity (1.09 (95% CI 1.1, 1.19)), while 2,4-DCP and 2,4,5-TCP showed no significant correlation with overweight or obesity. 2,4-DCP showed a significant positive relationship with high density lipoprotein-cholesterol (HDL-C). Moreover, 2,5-DCP showed a significant negative relationship only with systolic blood pressure and 2,4,5-TCP had a statistically significant inverse association with total cholesterol and HDL-C (−0.71 (95% CI −0.98, −0.45)). This study suggests potential associations of chlorophenol pesticides with overweight, obesity, lipid profile, and blood pressure in children and adolescents. Longitudinal studies are necessary to assess the clinical impact of these findings.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Obesity is a risk factor for a number of health problems, including heart disease, high blood pressure, type 2 diabetes, some cancers, and reproductive problems. In addition to that in developed countries, the rate of obesity in developing countries has increased rapidly. It has been estimated that the number of overweight people worldwide is greater than those who suffer from malnutrition (Snell 2013). Obesity is caused through a complex interaction of genetic, environmental and behavioral factors and the increased obesity rate cannot be interpreted only through changes in food intake and reduced physical activity. Although there is a genetic component for obesity, genetics has failed in the last decade to explain this epidemic (Newbold et al. 2007; Heindel 2003).
There is emerging evidence that exposure to various industrial chemicals that disrupt the endocrine system may contribute to the obesity epidemic. Among these industrial chemicals, organochlorine (OC) pesticides are of special interest (Lee et al. 2012). Chlorophenols (CPs) are ubiquitous environmental pollutants which are widely used as raw materials or intermediate products for agricultural, industrial, and home use purposes (Guo et al. 2016). 2,4-dichlorophenol (2,4-DCP) is primarily used as an intermediate material in the manufacture of 2,4-dichlorophenoxy acetic acid (2,4-D), a commonly used herbicide in the phenoxyacetic acid class. The main source of 2,4-DCP is the decomposition of 2,4-D in polluted soil and water. In addition, 2,4-DCP is also commonly reported as a product of the photodecomposition of triclosan, an antibacterial and antifungal agent (Wei et al. 2014; Pirsaheb et al. 2014).
2,5-dichlorophenol (2,5-DCP) is an urinary metabolite of 1,4-dichlorobenzene (1,4-DCB) or paradichlorobenzene (ρ-DCB) which is used in mothballs, room and toilet deodorizers, and in the past as an insecticide fumigant. Traces of ρ-DCB have been detected in home appliances, bathrooms, and new buildings in ambient air (Wei and Zhu 2016a). The CPs 2,4,5-trichlorophenol (2,4,5-TCP) and 2,4,6-trichlorophenol (2,4,6-TCP) are urinary metabolites of chemicals such as hexachlorobenzene (HCB) and hexachlorocyclohexane (HCHs). 2,4,5-TCP has been used as a biocide and as an intermediate in the production of 2,4,5-trichlorophenoxyacetic acid, one of the most widely used herbicides in the 20th century (Karn and Reddy 2012). 2,4,6-TCP is normally found in industrial wastewater from the paint, pharmaceuticals, pesticides, wood, pulp, and paper industries as well as water purification processes (Krishnaiah et al. 2013).
Many studies in developed countries have monitor CPs in the urine samples of different age groups and its association with obesity. One study conducted on children in Arkansas found that 27% of urine samples had detectable levels of 2,4-DCP (>1 μg/l) (Hill et al. 1989). A study on children aged 6 to 11 years in a national survey conducted in 2003–2004 in the USA, the 95th percentile of 2,4,5-TCP and 2,4,6-TCP urinary levels were 0.3 and 1.9 μg/l, respectively (CDC 2012). A similar study in 2007–2010 also showed that dichlorophenols was observed in 90% of urine samples. This study also investigated the relationship of phenolic compounds in urine associated with overweight and obesity in children and adolescents. It showed significant relationships between dichlorophenols and obesity, waist circumference (WC) and body mass index (BMI) (Buser et al. 2014).
The aim of the current study was to measure the urinary concentrations of 2,4-DCP, 2,5-DCP, 2,4,5-TCP, and 2,4,6-TCP and to determine their relationships with overweight and obesity indices as well as with the cardiometabolic risk factors of lipid profile and blood pressure in a population-based sample of children and adolescents.
Methods
Study population and health outcomes
This cross-sectional study was conducted in 2016 among children and adolescents aged 6 to 18 years living in Isfahan, Iran. The participants were selected from households in different areas of the city. The sample size was 242. Inclusion criteria consisted of being aged 6 to 18 years, having lived in the city of Isfahan for at least 1 year, and having no history of chronic disease or long-term medication use. The subjects were obtained by distributing invitations to households referring to a pediatrics clinic and obtaining parental consent. During a visit, a questionnaire consisting of questions about demographic characteristics and physical activity (PA) was completed through interviews with the parents. PA was introduced by asking “Have you engaged in physical activity for a few days (at least 30 minutes per day) in the past week?” Various types of PA were examined (Faghihimani et al. 2010; Motlagh et al. 2017).
The physical examination includes measurement of weight, height, waist circumference (WC) and blood pressure (BP) using standard protocols with calibrated instruments. The BMI was calculated as weight (kg) divided by height squared (m2). The BMI z-score was calculated according to age and gender identified obesity (BMI in the 95 percentile or higher) and overweight (BMI between the 85th and 95th percentile) according to the CDC (CDC, 2016). For biochemical tests, 2 ml of venous blood were taken from the children and adolescents. Fasting blood sugar (FBS) and a lipid profile that included total cholesterol (TC), low density lipoprotein-cholesterol (LDL-C), high density lipoprotein-cholesterol (HDL-C), and triglycerides (TG) were determined using an auto analyzer and standard kits (Pars Azmoun; Tehran). The mean arterial blood pressure (MABP) was calculated as (systolic blood pressure (SBP) + 2 diastolic blood pressure (DBP))/3. Participants were divided into two groups in terms of age, one for children aged 6–12 and one for adolescents aged 12–18 years.
Measurement of urinary concentrations of chlorophenols
Stoke solutions of 2,4-DCP, 2,5-DCP, 2,4,5-TCP, and 2,4,6-TCP were separately prepared and stored at temperatures below 0 °C until use. After being collected, spot urine samples were kept in 10-ml containers at − 20 °C until analysis. Urine specimens were fluid at room temperature and their supernatant was removed and centrifuged (5000 rpm for 5 min). To do this, 120 μl of concentrated sulfuric acid was added and the specimen was put in a sand bath at 100 °C for 60 min (Kontsas et al. 1995). The samples were kept at room temperature after the sand bath. The urine samples were diluted with distilled water after acid hydrolysis and were extracted using dispersive liquid-liquid microextraction (DLLME). Acetone and chlorobenzene were added to the samples as extraction and disperser solvents, respectively, and the samples were centrifuged (5000 rpm for 5 min). The extracted solution was dried using N2. Diazomethane was used as a derivatizing reagent (Kramer and Angerer 1995).
The urinary limit of detection (LOD) of 2,4-DCP, 2,5-DCP, 2,4,5-TCP, and 2,4,6-TCP was 0.33, 0.3, 0.13, and 0.3 μg/l, respectively and it was found that 94.6, 95, 85.1, and 38% of the participants, respectively, had urinary concentrations of above the LOD. The 2,4,6-TCP data were not analyzed statistically. All the urinary CP values below the LOD were obtained LOD/√2 (Verbovsek 2011; Katherine et al. 2010; Marsha 2015; Buser et al. 2014). In order to modify the changes caused by dilution of the spot urine samples, random creatinine levels in the urine were also evaluated. The urinary metabolites were tested in terms of μg/g of creatinine (μg/g cr) to allow adjustment to be carried out. Urinary creatinine levels were analyzed using an auto analyzer (Hitachi 912) by a Jaffe reaction. In this method, creatinine reacting with picric acid in an alkaline medium forms a color complex. The color change is directly proportional to the amount of creatinine and is measured through absorbance at 520 nm (Syal et al. 2013).
Matrix spikes, duplicates (analytical and field), and blank (field and laboratory) samples were used in analysis. Recovery means were 76–89% for the four CPs in urine. All the blanks attained values below the LOD for each analyte in urine. Duplicate samples had differences of less than 16% in all analytes in urine.
CP analysis was done using a gas chromatograph (Agilent 7890A) coupled to a mass spectrometer system (inert) and split/splitless injector system (Agilent 5975C). The column was a DB-5 (60 m × 0.25 mm × 0.25 μm; Agilent) and helium (99.9995%) was used as a carrier gas. Separation was performed at an initial temperature of 100 °C for 2 min, followed by ramping at 10 °C/min to 250 °C for a total run time of 15 min. The injector was operated in split mode with a split ratio 5:1 and the temperature was set at 260 °C. Mass spectrometer conditions were as follows: ion source temperature of 330 °C; transfer line temperature of 300 °C. Mass spectrometric measurement was performed in electron ionization mode.
Statistical analysis
Descriptive statistics including mean (SD) were calculated for the four CPs, BMI, BMI z-score, WC, clinical laboratory indices, and demographic characteristics. In addition, the geometric mean and 95th percentiles were evaluated for 2,4-DCP, 2,5-DCP, 2,4,5-TCP, and 2,4,6-TCP.
The Kolmogorov-Smirnov test was used to assess the assumption of fit to the normal distribution of outcome variables such as BMI z-score and WC. Multivariate linear regression was conducted to evaluate the relationship between 2,4-DCP, 2,5-DCP, and 2,4,5-TCP with BMI z-score and WC while controlling for MABP, FBS, PA, TC, HDL-C, and LDL-C stratified by age. Analysis was also conducted to evaluate the relationship between the three CPs mentioned with TC, LDL-C, HDL-C, TG, SBP, and DBP while controlling for sex, PA, and BMI stratified by age. Multinomial logistic regression also was used to assess the effect of environmental factors of 2,4-DCP, 2,5-DCP, and 2,4,5-TCP on the risk of overweight and obesity while controlling for MABP, FBS, PA, TC, HDL-C, and LDL-C. All analyses were evaluated at a confidence interval (CI) of 95%. In the univariate analysis, the variables having a p value < 0.2 were entered into the final model. Statistical analysis was performed using SPSS 20 (SPSS; USA).
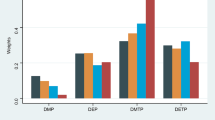
Results
The study participants consisted of 242 children and adolescents. Table 1 presents the characteristics of the participants as obese, overweight, or normal/underweight. It shows that 59.5% of total participants were 6 to 11 years of age and 42% of total participants were male. The average age was about 11 years. A total of 15% of participants were obese, 38% were overweight, and the rest were normal weight or underweight. The mean (SD) urinary concentrations of 2,5-DCP, 2,4-DCP, 2,4,5-TCP, and 2,4,6-TCP in all samples were, respectively, 8.6 (3.6), 3.1 (2.7), 1.6 (1.9), and 1.3 (2.2) μg/l. Moreover, the average urinary concentrations of these metabolites in obese subjects were, respectively, 10.2 (4.3), 4.9 (4.2), 2.3 (2.7), and 3.3 (3.4) μg/l and the same concentration levels for overweight subjects were, respectively, 8.7 (3.6), 3.6 (3.2), 1.8 (1.7), and 1.4 (2) μg/l. These concentration levels for normal weight and underweight subjects were 8 (3.1), 2.5 (2), 1.3 (1.6), and 0.6 (1.2) μg/l, respectively. These averages were higher in obese subjects than in those who were overweight and higher in overweight subjects than normal or underweight subjects. The mean (SD) of WC and BMI z-score were, respectively, 82.3 (12.7) cm and 1.36 (1.3) SD.
The mean, geometric mean, and 95th percentile of the urinary metabolites were calculated (μg/l and μg/g creatinine). The geometric means of 2,5-DCP and 2,4-DCP were, respectively, 7 and 2 μg/l and for the 95th percentile were 14 and 7.5 μg/L in the unadjusted state with urine creatinine. In the adjusted state, the mean (SD) of 2,5-DCP and 2,4-DCP were, respectively, 12.3 (5.1) and 17.7 (15.9) μg/g cr. Their geometric mean and 95th percentiles were 10 and 4.7 μg/g cr and 20 and 26.7 μg/g cr, respectively. The geometric mean and 95th percentile of 2,4,5-TCP and 2,4,6-TCP in the unadjusted state were, respectively, 0.81, 0.49, 4.6, and 6.8 μg/l. But in the adjusted state with urinary creatinine, the mean (SD) of 2,4,5-TCP and 2,4,6-TCP were, respectively, 5.8 (4.4) and 3.7 (6.7) μg/g cr. Their geometric mean and 95th percentile were 1.8 and 1.6 μg/g cr and 16.1 and 20.1 μg/g cr, respectively.
All subjects showed statistically significant correlations between WC with 2,5-DCP and 2,4,5-TCP and BMI z-score with 2,5-DCP. A 0.07 SD (0.04, 0.1) increase in BMI z-score and a 0.79 cm (0.54, 1.03) increase in WC were observed for 2,5-DCP. The results also showed that 2,4,5-TCP increased WC by 0.23 cm (0.0, 0.46). There was a statistically significant relationship between 2,5-DCP and WC and BMI z-score in both age groups. For 2,4,5-TCP, in the 6–11 year age group, there was no significant relationship between 2,4,5-TCP and these two indicators. In the 12–18 age group, 2,4,5-TCP significantly correlated only with WC. There was no significant correlation between WC and BMI z-score parameters and 2,4-DCP urinary metabolites, except that the relationship between BMI z-score and 2,4-DCP was significant for the 6–11 year age group (Table 2).
The results of adjusted multivariate linear regression for the relationship between 2,4-DCP, 2,5-DCP and 2,4,5-TCP with TG, TC, HDL-C, LDL-C, SBP, and DBP are shown according to age in Table 3. In all cases, the relationships between 2,5-DCP and the mentioned parameters were not significant except for SBP, which showed a negative association (β coefficient = −0.04). For 2,4-DCP, only the relationship with HDL-C was significant (p = 0.03; β coefficient = 0.18). This was not significant for the 6–11 age group (p = 0.3). 2,4,5-TCP had statistically significant associations with TC and HDL-C which were also negative.
The multinomial logistic regression model showed that there was no significant relationship between 2,4-DCP and 2,4,5-TCP and overweight and obesity. There was no significant relationship between 2,5-DCP and overweight, but there was with obesity, which increased obesity risk by 1.09-fold. For the 6–11 year age group, 2,4-DCP and 2,5-DCP showed a significant relationship with obesity with an odd’s ratio (OR) of 0.91 and 1.23, respectively, but 2,4-DCP had an inverse relationship. However, there were no significant relationships with overweight in this age group. In the 12–18 year age group, 2,4-DCP was not significantly related to overweight or obesity and 2,5-DCP was only significantly related to overweight (OR = 1.1). In both age groups, 2,4,5-TCP showed a significant relationship only with obesity (Table 4).
Discussion
This study demonstrated significant associations for the level of some urinary metabolites of CP pesticides with obesity and some cardiometabolic risk factors both groups.
Buser et al. studied children and reported geometric mean concentrations of 2,5-DCP and 2,4-DCP to be 8.8 and 1 μg/l, respectively (Buser et al. 2014). The findings of the current study (7 and 2 μg/l, respectively) are consistent with the results of their study. Twum et al. reported the 75th percentile of 2,5-DCP and 2,4-DCP in the urine of children and adolescents to be 74.6 and 3.7 μg/l, respectively (Twum and Wei 2011). In the current study, these values were 11.4 and 4.6 μg/l, respectively (data not shown). Wei and Zhu investigated 2,5-DCP metabolites in diabetic and non-diabetic adults and reported geometric means of 9.8 and 6.3 μg/l, respectively (Wei and Zhu 2016a). In another study, these two researchers reported the geometric mean of urinary concentration of 2,5-DCP in subjects aged 20–29 years to be 7.4 μg/l (Wei and Zhu 2016b). Wei et al. studied adults and reported that geometric mean concentrations for 2,5-DCP and 2,4-DCP to be 2.5 and 0.09 μg/g cr, respectively (Wei et al. 2014).
In a study on children aged 6–11 years, NHANES (2003–2004) reported that the 2,4,6-TCP urinary level at the 95th percentile was about 1.9 μg/l and the 2,4,5-TCP urinary level at the 95th percentile to be 0.3 μg/l (Hill et al. 1989). In contrast, the current findings showed that at the 95th percentile, the level for 2,4,6-TCP and 2,4,5-TCP were 3.5 and 15 times higher, respectively, than their levels in the NHANES study. Frederiksen et al. reported that the 24 h urine arithmetic mean concentration of 2,4,5-TCP in children and adolescents aged 6 to 21 was 0.1 μg/l and the 95th percentile and maximum level were 0.38 and 3.7 μg/l, respectively (Frederiksen et al. 2013a). The average concentration of 2,4,5-TCP in the current study was 16 times more than the average concentration in Frederiksen et al. Frederiksen et al. also reported the average, 95th percentile and maximum level of 2,4,5-TCP to be 0.04, 0.37 and 0.8 μg/g cr, respectively, in children aged 6–11 years (Frederiksen et al. 2013b). These values for the 6–11 year age group were much higher in the current study; for example, the average was about 100 times higher.
Given that there are few studies on 2,4,5-TCP and 2,4,6-TCP metabolites in children and adolescents, a series of studies on adults also was carried out. Gou et al. examined adults and reported that the geometric mean, 95th percentile and maximum level of 2,4,6-TCP were 1.9, 7.3, and 40.6 μg/g cr, respectively. These parameters for 2,4,5-TCP were less than the LOD at 0.2 and 6.6 μg/g cr. (Guo et al. 2016). If the range and average geometric data for 2,4,6-TCP are compared between Guo et al. and the present study, the geometric means of 1.9 and 1.1, respectively, are relatively close, but 2,4,5-TCP was significantly different and its concentration in this study was higher than for Gou et al.
From these studies, which monitored 2,5-DCP and 2,4-DCP compounds in urine, it can be understood that urinary concentrations of these metabolites were higher in previous studies than in studies conducted in the past few years. This suggests that the exposure of parent compounds of these two metabolites was higher in the past and their use has likely decreased. In the current study, the concentrations were similar to those obtained in the NHANES studies in recent years. The present study and these previous is that the 2,5-DCP concentrations were higher than those of 2,4-DCP, which may be due to high exposure to its parent compound (1,4-DCB) compared with 2,4-D. These studies on trichlorophenols also suggest that urinary concentrations of 2,4,6-TCP and 2,4,5-TCP in the current study were higher than in other studies, which may result from high exposure to the parents of these metabolites in Isfahan. A few similar studies on pesticides in Iran have shown that lindan, which is a parent compound of 2,4,6-TCP, 2,4,5-TCP, and 2,4-D has been detected in Iranian rivers (Dehghan Abkenar et al. 2014; Keshavarzifard et al. 2012; Yagoubzadeh and Safar 2015). Lindan also has been detected in the breast milk of mothers in Tehran (Afshar et al. 1997).
The present study investigated the relationship between BMI z-score, which is the main indicator of overweight and obesity in children and adolescents, and WC, which is a key component of 2,4-DCP, 2,5-DCP, and 2,4,5-TCP metabolites. The results showed a significant correlation between WC and BMI z-score and 2,5-DCP, but no relationship between them and 2,4-DCP metabolite (except for the 6–11 year age group). Buser et al. concluded that there was a significant relationship between WC and BMI z-score with both urinary metabolites of 2,4-DCP and 2,5-DCP in children and adolescents (Buser et al. 2014). In a study on non-diabetic adults, Wei and Zhu found a significant relationship between WC and 2,5-DCP (Wei and Zhu 2016b). Arrebola et al. found a significant quadratic relationship between OC pesticides in adipose tissue, such as HCB, p,p-DDE, and b-HCH, with BMI (Arrebola et al. 2014). In the current study on children and adolescents, 2,4,5-TCP, which is a urinary metabolite of HCB and HCH, was significantly related to WC, but not to BMI z-score. On the other hand, this metabolite significantly correlated with obesity in the 12–18 year age group. Kim also reported no significant relationship between BMI and 2,4,5-TCP urinary metabolite in adults (Kim et al. 2014).
One potential pathway by which ρ-DCB could affect metabolic risk is the ability to change lipid metabolism. The results of Wei and Zhu showed that urinary 2,5-DCP had a negative association with serum HDL-C; however, no association was found in the current study. Wei and Zhu observed no significant relationships between urinary 2,5-DCP and serum TG, SBP, and DBP (Wei and Zhu 2016a). Arrebola et al. indicated that TC and LDL-C had significant associations with adipose tissue HCB, but TG and HDL-C did not (Arrebola et al. 2014). The results of the current study were different from this; 2,4,5-TCP (a urinary metabolite of HCB) showed a negative significant association with TC and HDL-C.
Twum and Wei (NHANES 2003–2006) found no significant relationship between 2,4-DCP and obesity in children aged 6 to 19 years, but there was a significant interquadratic relationship between 2,5-DCP level and obesity (Twum and Wei 2011). The current findings on the relationship between urine concentrations of these metabolites with obesity are consistent with these findings and were somewhat consistent with the results of Buser et al. (NHANES 2007–2010). Their study showed that concentrations of 2,4-DCP and 2,5-DCP were significantly related to obesity, but this relationship did not exist in the case of overweight (Buser et al. 2014). The difference between the results of the current study and that of Buser et al. is that 2,4-DCP was not found to be significantly related to obesity. Wei et al. (NHANES 2005–2008) studied adults and showed that concentrations of 2,4-DCP did not correlate with obesity, but 2,5-DCP was significantly correlated with obesity, which is consistent with current findings (Wei et al. 2014).
The development of obesity involves an interaction between genetic and environmental factors, including physical and social environment. Many chemicals, such as dichlorophenols, are endocrine disruptive factors. Because they have the same structure as estradiol, they can affect the body weight control system. Some chlorinated pesticides such as 2,4-D and 1,4-DCB, which are the parent compounds of 2,4-DCP and 2,5-DCP, respectively, have been reported to effect thyroid gland function and eventually metabolic processes. Some environmental chemicals act through the peroxisome proliferator-activated gamma receptors that are the main regulator of adipogenesis (Charles et al. 1996; Croes et al. 2015; Wei and Zhu 2016b). There is also a possible connection between lower birth weight and risk of obesity during childhood and adolescence. Some studies have shown that there is a significant relationship between prenatal urinary concentrations of 2,4-DCP and 2,5-DCP and low birth weight (Wolff et al. 2008; Philippat et al. 2012). Considering the foregoing, as well as the results of recent studies, it can be stated that these metabolites, particularly 2,5-DCP may be involved in overweight and obesity in children and adolescents along with behavioral and genetic factors.
There were several limitations to this study. The main limitation was its cross-sectional design because all data were obtained at a specific point in time; hence, causation cannot be assumed. Moreover, it was not possible to examine the pubertal status of participants. Only three CPs were studied, although compounds such as dioxins, polychlorinated biphenyls, and other chlorophenols may also cause overweight and obesity. Another limitation was the use of spot urine values, which might not reflect long-term exposure. It must be taken into account that these substances can be stored in fat tissues; thus, overweight and obese people may have higher accumulations of these compounds.
Conclusion
In this study, 94.6, 95, 85.1, and 38% of the participants had urinary concentrations above the LOD, respectively, for 2,4-DCP, 2,5-DCP, 2,4,5-TCP, and 2,4,6-TCP. It can be stated that the urinary concentrations of trichlorophenols in subjects in Isfahan was higher than those in other countries; thus, it appears that there is high exposure to the parents of these metabolites. Further research is needed to biomonitor and determine exposure routes in Iran. Also, given that these compounds may impose different effects, they should be monitored in terms of their biological components and their relationships with resulting problems. The current findings show a potential association between 2,4-DCP, 2,5-DCP, and 2,4,5-TCP with weight indices and a few metabolic syndrome components. Because of the cross-sectional nature of the study, the relationships found cannot be considered to be causal; thus, there is need for cohort and case-control studies with bigger sample sizes.
References
Afshar M, Taheri E, Alani D (1997) Investigation of organochlorine pesticide residues in samples of 40 nursing mothers residing in Tehran. Tehran Univ Med J 6:13–18 (in Persian)
Arrebola JP, Ocana-Riola R, Arrebola-Moreno AL, Fernandez-Rodríguez M, Martin-Olmedo P, Fernandez MF, Olea N (2014) Associations of accumulated exposure to persistent organic pollutants with serum lipids and obesity in an adult cohort from Southern Spain. Environ Pollut 195:9–15. https://doi.org/10.1016/j.envpol.2014.08.003
Buser MC, Murray HE, Scinicariello F (2014) Association of urinary phenols with increased body weight measures and obesity in children and adolescents. J Pediatr 165(4):744–749. https://doi.org/10.1016/j.jpeds.2014.06.039
Centers for Disease Control and Prevention (2012) Fourth National Report on Human Exposure to Environmental Chemicals, volume 1. https://www.cdc.gov/exposurereport/. Accessed 15 Oct 2012
Centers for Disease Control and Prevention (2016) Overweight and Obesity. https://www.cdc.gov/obesity/childhood/defining.html. Last updated: October 2016
Charles JM, Bond DM, Jeffries TK, Yano BL, Stott WT, Johnson KA, Cunny HC, Wilson RD, and Bus JS (1996) Chronic dietary toxicity/oncogenicity studies on 2, 4-dichlorophenoxyacetic acid in rodents. Funda Appl Toxicol 33:166–172. https://doi.org/10.1006/faat.1996.0154
Croes K, Den Hond E, Bruckers L, Govarts E, Schoeters G, Covaci A, Loots I, Morrens B, Nelen V, Sioen I, van Larebeke N, Baeyens W (2015) Endocrine actions of pesticides measured in the Flemish environment and health studies (FLEHS I and II). Environ Sci Pollut Res Int 22(19):14589–14599. https://doi.org/10.1007/s11356-014-3437-z
Dehghan Abkenar S, Hosseini M, Esmaili Gholzoom H, Khoda Bakhshi GA, Mehrdadi N (2014) Determination of organochlorine pesticides in river waters by GC-ECD after solid phase extraction, Mazandaran. J Environ Stud 40(3):765–773 (in Persian)
Faghihimani Z, Nourian M, Nikkar AH, Farajzadegan Z, Khavariyan N, Ghatrehsamani S et al (2010) Validation of the child and adolescent international physical activity questionnaires in Iranian children and adolescents. ARYA Atheroscler J 5(4):163–166
Frederiksen H, Aksglaede L, Sorensen K, Nielsen O, Main KM, Skakkebaek NE et al (2013a) Bisphenol A and other phenols in urine from Danish children and adolescents analyzed by isotope diluted TurboFlow-LC-MS/MS. Int J Hyg Environ Health 216:710–720
Frederiksen H, Nielsen JKS, Mørck TA, Hansen PW, Jensen JF, Nielsen O, Andersson AM, Knudsen LE (2013b) Urinary excretion of phthalate metabolites, phenols and parabens in rural and urban Danish mother-child pairs. Int J Hyg Environ Health 216(6):772–783. https://doi.org/10.1016/j.ijheh.2013.02.006
Guo J, Wu C, Lv S, Lu D, Feng C, Qi X et al (2016) Associations of prenatal exposure to five chlorophenols with adverse birth outcomes. Environ Pollut 214:478–484. https://doi.org/10.1016/j.envpol.2016.04.074
Heindel JJ (2003) Endocrine disruptors and the obesity epidemic. Toxicol Sci 76(2):247–249.
Hill RH Jr, To T, Holler JS, Fast DM, Smith SJ, Needham LL, Binder S (1989) Residues of chlorinated phenols and phenoxy acid herbicides in the urine of Arkansas children. Arch Environ Contam Toxicol 18(4):469–474. https://doi.org/10.1007/BF01055011
Karn SK, Reddy MS (2012) Removal of 2,4,5-trichlorophenol by bacterial isolates from the secondary sludge of pulp and paper mill. J Basic Microbiol 52:1–6
Katherine FL, William WB, Michael RW, Dave AB, Teryl GG, James GS (2010) A comparison of techniques for assessing central tendency in left-censored data using PCB and p,p'-DDE contaminant concentrations from Michigan’s Bald Eagle Biosentinel Program. Chemosphere 80:7–12
Keshavarzifard M, Mashinchian Moradi A, Fatemi SMR, Esmaeili Sari A (2012) Investigation of organochlorine pesticides in sediments of the southern shores of the Caspian Sea. J Environ Sci Technol 14(2):107–113 (in Persian)
Kim K, Park H, Lee JH (2014) Urinary concentrations of trichlorophenols in the Korean adult population: results of the National Human Biomonitoring Survey 2009. Environ Sci Pollut Res 21(4):2479–2485. https://doi.org/10.1007/s11356-013-2180-1
Kontsas H, Rosenberg C, Pfaffli P, Jappinen P (1995) Gas chromatographic-mass spectrometric determination of chlorophenols in the urine of sawmill workers with past use of chlorophenol-containing anti-stain agents. Analyst 120(6):1745–1749. https://doi.org/10.1039/AN9952001745
Kramer A, Angerer J (1995) Comparison of two different derivatization procedures for the determination of urinary chlorophenol excretions. Fresenius’ J Anal Chem 351(2-3):327–330. https://doi.org/10.1007/BF00321659
Krishnaiah D, Anisuzzaman SM, Bono A, Sarbatly R (2013) Adsorption of 2,4,6-trichlorophenol (TCP) onto activated carbon. J King Saud Univ Sci 25:251–255
Lee DH, Lind L, Jacobs DR Jr, Salihovic S, van Bavel B, Lind PM (2012) Associations of persistent organic pollutants with abdominal obesity in the elderly: the Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) study. Environ Int 40:170–178. https://doi.org/10.1016/j.envint.2011.07.010
Marsha KM (2015) Predictors of urinary levels of 2,4-dichlorophenoxyacetic acid,3,5,6-trichloro-2-pyridinol, 3-phenoxybenzoic acid, and pentachlorophenol in 121 adults in Ohio. Int J Hyg Environ Health 218:479–488
Motlagh ME, Ziaodini E, Qorbani M, Taheri M, Aminaei T, Goodarzi A, et al (2017) Methodology and early findings of the fifth survey of childhood and adolescence surveillance and prevention of adult noncommunicable disease: the CASPIAN-V study. Int J Prev Med 8:4. https://doi.org/10.4103/2008-7802.198915
Newbold RR, Padilla-Banks E, Snyder RJ, Phillips TM, Jefferson WN (2007) Developmental exposure to endocrine disruptors and the obesity epidemic. Reprod Toxicol 23(3):290–296. https://doi.org/10.1016/j.reprotox.2006.12.010
Philippat C, Mortamais M, Chevrier C, Petit C, Calafat AM, Ye X, Silva MJ, Brambilla C, Pin I, Charles MA, Cordier S, Slama R (2012) Exposure to phthalates and phenols during pregnancy and offspring size at birth. Environ Health Perspect 120(3):464–470. https://doi.org/10.1289/ehp.1103634
Pirsaheb M, Dargahi A, Hazrati A, Fazlzadehdavil M (2014) Removal of diazinon and 2,4-dichlorophenoxy-acetic acid (2,4-D) from aqueous solutions by granular-activated carbon. Desalin Water Treat 52(22-24):4350–4355. https://doi.org/10.1080/19443994.2013.801787
Snell MA (2013) Association between environmental toxins, obesity, weight loss, and chronic disease using canonical correlation analysis, factor analysis, and PCA logistic regression. Dissertation, New Mexico Institute of Mining and Technology
Syal K, Banerjee D, Srinivasan A (2013) Creatinine estimation and interference. Ind J Clin Biochem 28(2):210–211. https://doi.org/10.1007/s12291-013-0299-y
Twum C, Wei Y (2011) The association between urinary concentrations of dichlorophenol pesticides and obesity in children. Rev Environ Health 26(3):215–219
Verbovsek T (2011) A comparison of parameters below the limit of detection in geochemical analyses by substitution methods. Mater Geoenviron 58(4):393–404
Wei Y, Zhu J (2016a) Associations between urinary concentrations of 2,5-dichlorophenol and metabolic syndrome among non-diabetic adults. Environ Sci Pollut Res 23(1):581–588. https://doi.org/10.1007/s11356-015-5291-z
Wei Y, Zhu J (2016b) Urinary concentrations of 2,5-dichlorophenol and diabetes in US adults. J Expo Sci Environ Epidemiol 26:1–5
Wei Y, Zhu J, Nguyen A (2014) Urinary concentrations of dichlorophenol pesticides and obesity among adult participants in the U.S. National Health and nutrition examination survey (NHANES) 2005-2008. Int J Hyg Environ Health 217(2-3):294–299. https://doi.org/10.1016/j.ijheh.2013.07.003
Wolff MS, Engel SM, Berkowitz GS, Ye X, Silva MJ, Zhu C, Wetmur J, Calafat AM (2008) Prenatal phenol and phthalate exposures and birth outcomes. Environ Health Perspect 116(8):1092–1097. https://doi.org/10.1289/ehp.11007
Yagoubzadeh Z, Safar R (2015) Assessment biodegradation of chlorinated pesticides by isolated bacteria (Pseudomonas species) from the Mazandaran rivers. J Nat Environ 68(1):155–163 (in Persian)
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Philippe Garrigues
Rights and permissions
About this article

Cite this article
Parastar, S., Ebrahimpour, K., Hashemi, M. et al. Association of urinary concentrations of four chlorophenol pesticides with cardiometabolic risk factors and obesity in children and adolescents. Environ Sci Pollut Res 25, 4516–4523 (2018). https://doi.org/10.1007/s11356-017-0771-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-017-0771-y