
Abstract
From a list of the top prescribed drugs in Canada, 11 pharmaceuticals and two metabolites were selected for study in municipal sewage treatment plant effluents and receiving waters. Wastewater samples were collected from 16 wastewater treatment plants across Southwest Nova Scotia including the Annapolis Valley, South Shore, and Metropolitan Halifax. Samples were also collected between 100 and 200 m downstream of effluent outflows. Seven pharmaceuticals were found above μg/L levels with their highest concentrations as follows: metformin (10.6 μg/L), acetaminophen (28.9 μg/L), paraxanthine (18.2 μg/L), cotinine (3.10 μg/L), caffeine (115 μg/L), naproxen (29.1 μg/L), and venlafaxine (2.65 μg/L). Metformin, paraxanthine, caffeine, naproxen, ramipril, and venlafaxine were detected in every wastewater effluent sample. Statistical analysis revealed significant differences in pharmaceutical occurrence by treatment methods, weak dependence of pharmaceutical concentrations on populations, and the co-occurrence of some pharmaceuticals. Experimental results might indicate the limitation of primary only treatment methods in breaking down pharmaceuticals.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pharmaceuticals are a major component of health care costs incurred by Canadians. In 2009, over $29.6 billion was spent on prescription drugs, which resulted in more than $880 per capita in Canada (Canadian Institute for Health Information 2012). Pharmaceuticals are designed to improve health by inducing biological or physiological responses within the body. The pharmaceuticals differ in the ailments targeted, organs affected, modes of biological action, and chemical properties, which have implications on their metabolism within the body and their eventual fate in the environment.
Pharmaceuticals are introduced into the environment through a number of pathways including improper disposal of expired or unused drugs, pharmaceutical manufacturing wastewaters, and agricultural runoff, but they primarily originate from human excretion (Kim et al. 2007). Many drugs do not undergo complete metabolism prior to excretion and remain biologically active in the environment. Additionally, nearly 40 % of Canadians reported disposing of unused medications through flushing, garbage disposal, or burial, which can result in contamination in surface water and groundwater (Marshall 2008). Therefore, it is possible that unintended targets are exposed to active pharmaceuticals. Municipal sewage treatment plants (STPs) are not specifically designed to remove pharmaceuticals. Consequently, they are often ineffective for removing pharmaceuticals, because of the types of treatment available and resistance to microbial or chemical degradation. As a result, pharmaceuticals have been detected in municipal wastewater (Chen et al. 2006; Lajeunesse et al. 2008; Crouse et al. 2012) and surface water (Comeau et al. 2008; Yargeau et al. 2007) across Canada. Further, drinking and wastewater treatment plants often lie on the same body of water. As surface water serves as an important source of drinking water for many municipalities, it is important to investigate the risk of human exposure to pharmaceuticals released from STPs.
The environmental impact of estrogenic pharmaceuticals are well documented where adverse effects can occur even at low concentrations (ng/L level) such as immunosuppression in mussels (Gagné et al. 2006), female-biased sex ratios in frogs (Pettersson and Berg 2007), and reductions in fish fecundity culminating in population failures (Nash et al. 2004). In general, concentrations of pharmaceuticals found in surface water are present at the ng/L to μg/L concentration levels, which poses low acute human risk (Comeau et al. 2008; Crouse et al. 2012). However, there may be chronic effects or synergetic concurrent effects from mixtures of pharmaceuticals (Escher et al. 2011). The toxic effect of multiple pharmaceuticals at concentrations below thresholds of individual drug activity may produce significant effects beyond the model of simple addition. For example, fathead minnows exposed to six pharmaceuticals at environmentally relevant concentrations showed no effects on development or growth but showed significant increases in deformities for the subsequent generation including heart edema, spinal deformations, and missing fins (Parrott and Bennie 2009).
The pharmaceuticals chosen for this study included 11 of the top 20 most prescribed pharmaceuticals in Canada in 2008 (Carter and Campeau 2009), and the primary metabolites of caffeine and nicotine. Target compounds and their applications are listed in Table 1. The study was the first known wastewater study of metformin, salbutamol, ramipril, and quetiapine in Canadian wastewater. These compounds were reported for potential eco-toxicological effects on aquatic communities including fish, fleas, and invertebrates (Scheurer et al. 2012; Escher et al. 2011). Considering their high rates of consumption, it is important to study their presence in Canadian wastewater.
Although pharmaceuticals in the environment have been studied worldwide, there are major research gaps in the study of pharmaceuticals in rural areas and the impact of treatment methods. An initial study of six over-the-counter pharmaceuticals in the Annapolis Valley and Halifax was carried out in 2010 using gas chromatography–mass spectrometry (GC-MS) (Crouse et al. 2012). This study expands analyte selection to include essential prescribed pharmaceuticals enabled by a new analytical method based on high-performance liquid chromatography–tandem mass spectrometry (HPLC-MS/MS). It also includes much more STP sites across Southwest Nova Scotia especially rural areas. Situated between the Bay of Fundy and the Atlantic Ocean, Southwest Nova Scotia is characterized by a diverse cultural heritage, unique geographic landscapes, and intact ecosystems. It was designated as a Biosphere Reserve by the United Nations Educational, Scientific and Cultural Organization (UNESCO) in 2001. This was the first study of pharmaceuticals in the LaHave River watershed, Mahone Bay, Lunenburg, and Yarmouth. Further, various sewage treatment methods, urban versus rural communities, and correlation of pharmaceuticals are compared and discussed.
Materials and method
Sampling sites and sample collection
Southwest Nova Scotia includes two rural areas, the Annapolis Valley and the South Shore, and one urban area, the Metropolitan Halifax. Most communities in the region are located beside rivers and basins where municipal wastewater is discharged. Major rivers include the Avon River, Annapolis River, Cornwallis River, LaHave River, and Sackville River. These rivers empty into the Minas Basin, Annapolis Basin, Bedford Basin, or directly into the Atlantic Ocean.
The Annapolis Valley has three large watersheds: the Annapolis River, the Cornwallis River, and the Avon River watersheds. This study included STPs in six major communities in the Annapolis Valley: Windsor, Wolfville, Berwick, Greenwood, Middletown, and Annapolis Royal. The South Shore is a major tourist destination and includes many coastal communities. Wastewater samples were taken from STPs in three communities along the LaHave River (New Germany, Cookville, and Bridgewater), two communities along the Mahone Bay (Mahone Bay and Lunenburg), and two other coastal communities on the South Shore (Yarmouth and Liverpool). Halifax Harbor is the largest harbor on Canada’s Atlantic coastline. It is surrounded by Bedford, Dartmouth, and Halifax, which constitute the Metropolitan Halifax, the urban part of the Halifax Regional Municipality. Two STPs at Bedford (Mill Cove) and Dartmouth, and three harbor sites at the Bedford Basin, the Ferry Terminal Park, and the Point Pleasant Park were sampled.
A total of 16 STPs in Southwest Nova Scotia were included in this study. They are numbered counterclockwise with a prefix of “S” as shown in Fig. 1. Their detailed geological locations, treatment methods, and flow rates are presented in Table 2. Wastewater samples were collected at the location of effluent outflows. Where access was possible in some sites, downstream samples were taken between 100 and 200 m from the effluent outflows. In addition, six reference samples were also collected either from the sources of rivers or receiving waters. All samples were collected within a 1-week span in June 2012. For each site, two bottles of water samples were collected in 1-L amber glass bottles with Teflon-lined caps obtained from Chromatographic Specialties (Brockville, ON). They were then transported in coolers to the laboratory and stored in a refrigerator at 4 °C.

Sampling sites in Southwest Nova Scotia, Canada
Reagents and standards
Calibration standards of acetaminophen, cotinine, paraxanthine, naproxen, quetiapine, and atorvastatin were obtained from Cerilliant (Round Rock, TX). Other calibration standards were purchased from Sigma-Aldrich (Oakville, ON). The internal standard, acetaminophen-D4, and surrogate standard, lorazepam-D4, were obtained from C/D/N Isotopes Inc. (Pointe-Claire, QC). All calibrations standards were certified reference material with 97 % purity or better. Five-level calibration was established using linear regression. Sodium hydroxide, sulfuric acid, sodium lauryl sulfate, and HPLC-grade methanol were obtained from Fisher Scientific (Ottawa, ON). Ultra-high purity nitrogen was obtained from Praxair (Bridgewater, NS). Ultrapure deionized water was used for HPLC analysis and sample preparation.
Sample preparation
A vacuum filter apparatus equipped with a 1.2-μm Millipore glass filter was used to filter out suspended solids in water samples. The pH of the sample was adjusted to 7.0 ± 0.2 using 1 M sodium hydroxide or 1 M sulfuric acid. Solid phase extraction (SPE) was performed with 3-mL Chromabond® HR-X (200 mg sorbent) columns. These SPE columns were conditioned with 6 mL methanol, 6 ml of DI water, and 4 mL of 4 mM sodium lauryl sulfate solution. Samples (500 mL) were pumped through the column at 5 mL/min under vacuum. Cartridges were washed with 6 mL of deionized water and dried for 30 min under vacuum. Analytes were eluted using 2 mL methanol for three times (a total of 6 mL). Eluent was collected and reduced to 1 mL with gentle nitrogen blow-down at 50 °C.
Analysis of pharmaceuticals and other water quality parameters
Pharmaceutical analysis was performed using an Agilent 1200 HPLC coupled with an Agilent 6410 triple quadrupole mass spectrometer. Chromatographic separation was performed using a 25-cm Agilent ZORBAX Eclipse Plus C18 column with a 4.6-mm internal diameter and 5-μm particles. The mobile phase consisted of 0.5 mM ammonium formate solution and methanol. The flow rate of mobile phase was 0.5 mL/min. A solvent gradient was programed as the following: start from 25 % methanol, increase to 35 % by 10 min, quickly ramp to 85 % by 15 min, and finally reach 100 % methanol by 27 min. The column was held at a constant temperature of 40 °C. Following separation, ionization was conducted with an electrospray ionization (ESI) source under 35-psi nebulizer pressure. Drying gas temperature was set to 350 °C with a flow rate of 12 L/min. The MS was operated in the positive mode and the capillary voltage was held at 4,000 V. Nebulizing gas and collision gas were 98 % nitrogen and ultra-high purity (UHP, 99.999 %) nitrogen. Precursor-to-product ion transitions were established for all target pharmaceuticals. To boost the sensitivity of analysis, only one transition was monitored for each compound. Fragmentor voltage and collision energy were carefully optimized to achieve maximum response for each transition. The MS parameters and transitions are shown in Table 1.
In addition to the trace analysis of target pharmaceuticals, water samples were also analyzed for chemical oxygen demand (COD) and dissolved oxygen (DO). COD was measured using a HACH DR2800 spectrophotometer, while DO was tested using a HACH HQ40d portable meter.
Quality assurance and quality control
To assist with quality assurance and quality control, both deionized water and solvent blank samples were included and subjected to the same analytical method. Sampling bottles were pre-cleaned by manufacturers. These bottles and other glassware were thoroughly cleaned using deionized water and methanol and then baked at 200 °C before usage. Salinization of glassware was not performed because spiked samples did not show loss of target compounds.
Laboratory control samples were prepared by spiking a pharmaceutical mix, and recoveries of target pharmaceuticals were analyzed. High recoveries of target pharmaceuticals were achieved in sample preparation. These recoveries in control samples were reported, but results of field water samples were not adjusted. Both internal standard and surrogate were used to ensure the quality of instrumental analysis and sample preparation. Duplicates were included to verify the reproducibility of the analytical method. The analytical method was validated by repeating experiments in different days with various temperatures and humidity. Although some water samples had visible amount of suspended solids, they appeared to be similar after filtration and no matrix effect was observed.
Statistical analysis
One-way ANOVA with Tukey-Kramer comparison was used to conclude whether mean differences in effluent concentrations were statistically significant between treatment type and population served. A 95 % confidence level was used for both tests with analysis performed using Minitab 16. Spearman rank correlation was used to determine the statistical significance and strength of correlations between effluent concentrations and treatment parameters. Spearman rank correlation, ρ, coefficient is determined by
where n is the sample size and d is the difference in rank of variables. Sections of spearman coefficients, 0–0.3, 0.3–0.5, 0.5–0.7, 0.7–0.9, and 0.9–1.0, were interpreted as very weakly, weakly, moderately, strongly, and very strongly correlated, respectively. A 95 % confidence level was used with analyses performed using Origin 9.
Results and discussion
Method recoveries for all the pharmaceuticals targeted varied within the range of 74 to 104 % as reported in Table 3. Method detection limits (MDLs) were determined using the student t value (2.764, one sided) multiplied by the standard deviation calculated from 10 replicates of the lowest level of spike using a 99 % confidence level. Experimental results of MDLs, method recoveries, concentrations of target pharmaceuticals, COD, and DO are listed in Table 3. The pharmaceutical concentrations of interest are bolded and further discussed in this section.
Drug residues in the Annapolis Valley
Three STPs (S01 in Windsor, S02 in Wolfville, and S03 in Berwick) were sampled along the Avon River and Cornwallis watersheds ranging in populations served from 2,454 to 3,785 residents. Acetaminophen was not found in any effluent, but high levels (above 500 ng/L) of metformin, paraxanthine, caffeine, naproxen, and venlafaxine were detected in some effluents. Concentrations were the highest at the Wolfville STP including the metformin, paraxanthine, and naproxen present at 2.92, 4.16, and 1.12 μg/L, respectively. In a study conducted by Crouse et al. in November 2010, cotinine, caffeine, and naproxen were found at 245, 530, and 2,250 ng/L in Wolfville STP, respectively (Crouse et al. 2012). Results of this study in June 2012 were roughly half of the previous data for cotinine and naproxen, but the concentration of caffeine dropped further to about a fifth. Enrollment at Acadia University located in Wolfville effectively doubles the population of the town during the school year, which might be the major factor in the discrepancy. A similar seasonal variation of naproxen was observed by Carballa et al. They found naproxen concentration in the effluent of a STP in Galicia, Spain, varying from 0.80 to 4.8 μg/L (Carballa et al. 2004).
The Windsor STP had the highest concentration of caffeine (907 ng/L) of the three sites, while the Wolfville STP showed the highest level of paraxanthine (4,164 ng/L), the main metabolite of caffeine. The concentration of paraxanthine was only 18 ng/L at the Windsor STP. Caffeine is transformed to paraxanthine during human metabolism (about 80 % of the drug) and paraxanthine is not otherwise present in food or plants (Hillebrand et al. 2012). The difference in caffeine and paraxanthine concentrations between the Wolfville and Windsor STPs is not unusual. In septic treatment systems, the ratio of caffeine to paraxanthine is known to vary over a wide range between different treatment methods (Wilcox et al. 2009). Despite the discrepancy, both caffeine and paraxanthine are psychoactive central nervous system stimulants with comparable potencies (Orrú et al. 2013). Further, caffeine may be degraded to paraxanthine in the wastewater treatment process. Depending on the degradation rate of paraxanthine during treatment, it may accumulate as a high-concentration intermediate. Due to little rainfall, the Berwick STP was not operational with the effluent remaining stagnant for a week before sampling. Consequently, the effluent of this STP showed low levels of target pharmaceuticals. Metformin was detected at 472 ng/L while all other pharmaceuticals were below 50 ng/L.
Four STPs (S04 in Greenwood, S05 in Middleton, S06 in Annapolis Royal, and S07 in Digby) were sampled along the Annapolis River serving communities with populations ranging from 481 to 7,463 residents. Quetiapine was not detected in any water samples. Metformin, caffeine, naproxen, atorvastatin, and venlafaxine were found above 500 ng/L in some effluents. The effluent from the Middleton STP showed high concentrations of most pharmaceuticals, especially atorvastatin at 860 ng/L, which was the highest level of atorvastatin detected in the study. Despite being the most dispensed prescription drug, atorvastatin is almost entirely metabolized in the body and only 2 % of the drug is excreted unchanged (PDR Staff 2008). High concentrations of pharmaceuticals in the Middleton STP effluent were likely caused by inadequate airflow which reduced treatment efficiency. The Digby STP effluent had the highest metformin concentration (1.98 μg/L). Concentrations of naproxen and cotinine were comparable to those reported in Crouse et al.’s 2010 study (Crouse et al. 2012). However, the caffeine concentration increased from 51 to 857 ng/L in the Annapolis Royal STP effluent, while it decreased from 910 to 77 ng/L in the Digby STP effluent, which indicated possible seasonal variation in treatment efficiency or caffeine consumption considering population change due to visitors.
Three samples (S04D, S05D, and S06D) were taken downstream from STPs along the Annapolis River. Due to dilution with river water, downstream concentrations of pharmaceuticals in this study were consistent with other downstream sample studies which found 70–85 % lower concentration of downstream samples in comparison to effluent samples (Brun et al. 2006). S06D, the downstream of the Middletown STP, did not show much of a dilution effect for some pharmaceuticals; metformin even had a slightly higher concentration in the downstream sample than the effluent. Effluent from the Middletown STP was discharged into a small stream, and the downstream sample was taken from a small reverse bar where flow was relatively stagnant. Lack of mixing at this location might explain the lack of dilution effect for some pharmaceuticals. It is also interesting to notice that atorvastatin’s level decreased from 860 ng/L in the effluent to 22 ng/L in the downstream. This significant drop might due to accumulation of the pharmaceutical to sorptive material at the downstream site.
Three reference samples were collected upstream of the Cornwallis River (S01) and the Annapolis River (R02), and the Annapolis Basin (R03). The upstream sites were located at the sources of the rivers where human impact was minimal. Therefore, R02 showed no pharmaceutical except an ultratrace level of caffeine (14 ng/L) and atorvastatin (8 ng/L). Acetaminophen, paraxanthine, caffeine, and naproxen were all detected at very low levels in the Annapolis Basin. It was also the only site in the watershed where acetaminophen was detected at 61 ng/L. The Annapolis Basin sampling site was the docking point for the ferry between Digby, NS, and Saint John, NB. Acetaminophen might be contributed by the ferry operation. More investigation is needed to identify potential sources of acetaminophen including the sewage wastewater emitted by vessels and wastewater discharged from onshore facilities.
Drug residues in the South Shore
Three STP sites (S10 in New Germany, S11 in Cookville, and S12 in Bridgewater) were sampled along the LaHave River watershed with populations served from 447 to 8,241 residents. The highest concentrations of pharmaceuticals were detected in effluent from the Bridgewater STP including metformin (10.6 μg/L), paraxanthine (2.69 μg/L), caffeine (10.0 μg/L), naproxen (4.99 μg/L), and venlafaxine (1.47 μg/L). The level of metformin at the Bridgewater STP was the highest detected in this study. The Cookville STP serves primarily a commercial area including a shopping mall, school, and hotel. It is the only STP in this study that uses membrane bioreactor (MBR) technology where an ultrafiltration membrane is used to separate bacteria-enriched activated sludge from effluent (Ghoshdastidar et al. 2012; Ghoshdastidar and Tong 2013; Brown et al. 2013). Its effluent showed moderate levels of pharmaceuticals but had the highest concentration of venlafaxine (2.65 μg/L) in the study. A comparison of conventional activated sludge and MBR STPs serving similar sized populations with similar average flow rates showed little difference in the overall removal rates of venlafaxine (Rúa-Gómez et al. 2012). Venlafaxine has an octanol-water partition coefficient (LogK ow, Table 1) of 3.20. Compounds with LogK ow more than 3 may be absorbed by microorganisms and sludge in the treatment system (Comeau et al. 2008). High concentration of venlafaxine was likely due to a low capacity of microorganisms in the treatment system (Gasser et al. 2012).
Two downstream samples were collected for the Cookville STP (S11D) and Bridgewater STP (S12D). These two samples were relatively clean, especially the Bridgewater STP. Six drugs were detected in the Cookville downstream sample with caffeine the highest at 177 ng/L. Only caffeine (16 ng/L) was detected downstream from the Bridgewater STP.
Four STPs effluents (S08 in Yarmouth, S09 in Liverpool, S13 in Mahone Bay, and S14 in Lunenburg) were sampled along the South Shore costal line with populations served ranging from 943 to 25,275 residents. The Yarmouth STP, a primary treatment plant, had much higher concentrations of pharmaceuticals than the Liverpool STP which utilized aerated lagoon treatment and served a smaller population. Yarmouth effluent had high concentrations of metformin (1.92 μg/L), acetaminophen (7.90 μg/L), paraxanthine (4.13 μg/L), cotinine (1.16 μg/L), caffeine (27.7 μg/L), and naproxen (3.19 μg/L). The only drug that had comparable concentrations between the Yarmouth and Liverpool sites was metformin, which might indicate that efficiency of aerobic treatment for breaking down metformin was low. However, since STP influents were not included in this study, metformin’s treatment efficiency could not be quantified, which will be addressed in future studies. Further, the Yarmouth effluent sample showed the highest of COD (286 mg/L) in this study. Its effluent contained the lowest DO level (1.29 mg/L) of all samples indicating an anaerobic environment which limited the efficiency of aerobic treatment. The Lunenburg STP had higher concentrations of pharmaceuticals in its effluent than the neighboring Mahone Bay STP. Concentrations of metformin, acetaminophen, paraxanthine, cotinine, caffeine, and naproxen were above the μg/L level. The Lunenburg STP’s metoprolol (995 ng/L) was the highest concentration detected in this study. Only caffeine (1.36 μg/L) in the Mahone Bay effluent exceeded the μg/L level. Finally, effluent sample taken from Lunenburg harbor had 28.4 μg/L of caffeine, while its downstream also showed high level of caffeine at 4.02 μg/L. As caffeine is an important marker of wastewater contamination (Brown et al. 2013), the presence of caffeine in downstream might indicate significant contamination of shoreline waters.
Drug residues in the Metropolitan Halifax
Mill Cove STP (S15) and Dartmouth STP (S16) were sampled in the Halifax region. These two STPs serve a much larger population than rural sites in Nova Scotia. Three reference sites spread across the Halifax Harbor including R04 near S15 in the Bedford Basin, R05 at the Ferry Terminal Park on Alderney Drive, and R06 at the Point Pleasant Park. The Dartmouth STP, an advanced primary treatment site, had the highest level of caffeine (115 μg/L) in this study. The caffeine concentration was much higher than the maximum caffeine concentration (1.9 μg/L) found in 14 municipal STP effluents in Germany (Ternes et al. 2001). This significant difference may be related to consumption or treatment technology used. Concentrations of seven other pharmaceuticals (acetaminophen, paraxanthine, cotinine, naproxen, ramipril, and quetiapine) in the Dartmouth STP were also the highest of all study sites. Acetaminophen, a rarely found compound in other sites, was present at 28.9 μg/L. That being said, ramipril at 102 ng/L and quetiapine at 225 ng/L were considered relatively low in the environment. Both ramipril and quetiapine are heavily metabolized within the body. Ramipril itself is inactive and only 2 % of ramipril is excreted unchanged from the body, although 68 % of an intravenously administered dose is excreted as ramiprilat, the active metabolite (Griensven et al. 1995). The Dartmouth STP effluent also showed a high COD (208 mg/L) and low DO (1.41 mg/L). The results were similar to the other primary treatment plant, Yarmouth STP, which demonstrated the limitation and inadequacy of primary treatment method in degrading pharmaceuticals.
The Mill Cove STP has been the most extensively studied site for pharmaceuticals in Nova Scotia. Samples taken in 2003 reported detections of pharmaceuticals including ibuprofen, salicylic acid, gemfribozil, and benzafibrate (Brun et al. 2006). Naproxen was not detected in the sample collected in May 2003, but it was reported at 1.70 μg/L in sample collected in September 2003. Acetaminophen was not detected in either sampling activities with a MDL of 10 ng/L. A study in the summer of 2005 showed median concentrations of 5.10 μg/L and 610 ng/L for naproxen and caffeine, respectively (Comeau et al. 2008). Crouse et al. investigated the Mill Cove STP in November 2010. Naproxen, caffeine, and cotinine were discovered at 3.20 μg/L, 17.0 μg/L, and 570 ng/L, respectively (Crouse et al. 2012). Results of these pharmaceuticals in this study can be compared with that in the previous studies. Naproxen was detected at 1.12 μg/L and remained consistently at a single-digit μg/L level. The concentration of caffeine (3.86 μg/L) was lower than the 2010 result, but higher than the 2005 number. The level of cotinine dropped to 124 ng/L and acetaminophen remained undetected. The Mill Cove STP had the second highest concentration of metformin (8.17 μg/L), with Dartmouth STP closely behind (8.08 μg/L). Concentrations of three other pharmaceuticals, caffeine, naproxen, and venlafaxine, were also above the μg/L level.
For the three Halifax reference sites, each had at least five pharmaceutical detections. Most of these concentrations were negligible except that of caffeine. The caffeine concentration at the Point Pleasant Park (382 ng/L) was about double of the other two reference sites, because it is at the downstream of effluent water flow direction and close to downtown Halifax. Although the Point Pleasant Park is closer to open seawater than the other two reference sites, an obvious dilution effect was not observed. Despite major investment in the cleanup of the Halifax Harbor, minor incidents of untreated sewage dumping into the harbor have been reported in newspaper (Jeffrey 2012). However, caffeine concentrations in these three reference sites were lower than that in 11 German rivers and streams with a median of 530 ng/L (Ternes et al. 2001). Although Halifax municipal STP effluents had much more caffeine than German STP effluents, their receiving waters were contaminated less. This was likely due to a dilution effect in the Halifax harbor which is surrounded by a large amount of seawater.
Statistical analysis
Pharmaceuticals concentrations in STP effluents and receiving waters depend on many factors including population served, treatment technology, operational parameters (temperature, activated sludge, flow rate, hydraulic retention time, etc.), and flow rate of receiving stream. Treatment type, population served, and co-occurrences of drugs are chosen for statistical analysis to reveal relations between different STPs and drugs.
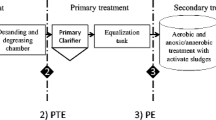
Drugs by treatment type
Wastewater treatment plants were divided into three categories: primary treatment (S08, S10, and S16), aerated lagoons (S01–S06, S09, and S13), and secondary treatment (S07, S11, S12, S14, and S15) for statistical analysis. One-way ANOVA with Tukey method comparison showed a significant difference between mean pharmaceutical concentrations in aerated lagoon treatment and primary treatment effluents for the following drugs: cotinine (p = 0.039) and caffeine (p = 0.043). Caffeine was readily degraded in aerated lagoons (>95 %) (Li et al. 2013; Conkle et al. 2008) and in conventional activated sludge-based secondary treatment plants (Thomas and Foster 2005). When primary treatment consisted mainly of settling processes, removal of caffeine was minimal at 15 % (Thomas and Foster 2005).
One-way ANOVA comparison showed a significant difference between the mean pharmaceutical concentrations in aerated lagoon treatment and secondary treatment effluents for the following drugs: metoprolol (p = 0.001) and venlafaxine (p = 0.004). Despite both treatment methods subjecting influents to biological treatment, metoprolol degradation in aerated lagoon systems has been shown to be greater than its degradation in conventional plants with clarification and activated sludge (Conkle et al. 2008; Bendz et al. 2005). Venlafaxine shows little difference in removal between primary and secondary wastewater treatment plants with efficiencies ranging from 7.8 and 39 % (Lajeunesse et al. 2008).
Drugs by population
Treatment plants were binned by population by service area into <2,000 (S05, S06, S10, S11, and S13), 2,000–5,000 (S01-S04, S07, S09, and S14), and >5,000 (S08, S12, S15, and S16). The amount of wastewater that a STP takes is roughly proportional to its serving population. Hence, the pharmaceutical concentration usually does not vary much with population. However, a large population community produces a high total flow of wastewater influent, which may exceed its STP’s treatment capacity and yield elevated pharmaceutical concentrations.
In correlation analysis, COD was found to moderately correlate with population (ρ = 0.58, p = 0.017). Three pharmaceuticals, metformin (ρ = 0.71, p = 0.048), cotinine (ρ = 0.55, p = 0.031), and ramipril (ρ = 0.66, p = 0.005), showed strong and moderate correlations with population. Of the four detections of acetaminophen in STP effluents, these occurred for plants serving high populations with the fewest treatment stages. Primary treatment plants at Yarmouth and Dartmouth, where treatment was limited, had high effluent concentrations.
Co-occurrence of drugs
Strong and positive correlations of many of the target pharmaceuticals were identified to a 95 % degree of confidence. Table 4 shows Spearman correlation coefficients, ρ, for major pharmaceutical compounds in Nova Scotia wastewater effluents; p values are in brackets. The strongest of these correlations included atorvastatin with quetiapine (ρ = 0.92, p = 0.002), caffeine with quetiapine (ρ = 0.89, p = 0.007), cotinine with quetiapine (ρ = 0.88, p = 0.007), cotinine with naproxen (ρ = 0.89, p = 0.0005), and cotinine with caffeine (ρ = 0.89, p = 0.0006). The co-occurrence cotinine and caffeine in central Indiana’s Upper White River watershed had an identical correlation to that found for Nova Scotia wastewater effluents (Bunch and Bernot 2011). While correlations of moderate strength were detected between many of the compounds, they have not been listed in Table 4. These strong correlations between pharmaceuticals indicate their co-occurrence in the environment, which may cause a more complex impact on the health of ecosystems due to synergetic effects.
Conclusions
All 13 target compounds were detected in Southwest Nova Scotia wastewater effluents across both rural and urban sites. Some concentrations were well above μg/L and might produce behavioral and morphological changes in aquatic wildlife. Although atorvastatin is the most dispensed prescription drug in Canada, it was found at relatively low levels with a maximum concentration detected of 860 ng/L, which was largely due to a high rate of metabolism in the body. In addition to caffeine and naproxen, the antidiabetic metformin and antidepressant venlafaxine were frequently detected in both effluent and downstream samples.
In general, primary treatment plant effluents such as Yarmouth and Dartmouth were found to have higher concentrations of pharmaceuticals than rural aerated lagoon effluents. The highest concentrations of pharmaceuticals were detected in the Dartmouth effluent including a caffeine concentration of 115 μg/L. Several strong correlations between pharmaceutical concentrations in effluents and wastewater treatment plant characteristics demonstrated that the effectiveness of wastewater treatment is a complex process with a range of parameters responsible for optimal pharmaceutical removal. Secondary treatment is the most critical stage in biological treatment technologies. It is recommend to be added onto existing primary only STPs. Advanced biological treatment technologies such as membrane bioreactor should be evaluated on efficiency, cost-effectiveness, and population size. Aerated lagoons are common in rural communities. Their efficiency can be improved significantly by incorporating better air distribution. To further characterize treatment efficiencies in different STPs, wastewater influents and activated sludge will be included in future studies.
References
Bendz D, Paxéus NA, Ginn TR, Loge FJ (2005) Occurrence and fate of pharmaceutically active compounds in the environment, a case study: Höje River in Sweden. J Hazard Mater 122(3):195–204. doi:10.1016/j.jhazmat.2005.03.012
Brown K, Ghoshdastidar AJ, Hanmore J, Frazee J, Tong AZ (2013) Membrane bioreactor technology: a novel approach to the treatment of compost leachate. Waste Manag 33(11):2188–2194. doi:10.1016/j.wasman.2013.04.006
Brun GL, Bernier M, Losier R, Doe K, Jackman P, Lee HB (2006) Pharmaceutically active compounds in Atlantic Canadian sewage treatment plant effluents and receiving waters, and potential for environmental effects as measured by acute and chronic aquatic toxicity. Environ Toxicol Chem 25(8):2163–2176. doi:10.1897/05-426R.1
Bunch A, Bernot M (2011) Distribution of nonprescription pharmaceuticals in central Indiana streams and effects on sediment microbial activity. Ecotoxicology 20(1):97–109. doi:10.1007/s10646-010-0560-6
Canadian Institute for Health Information (2012) Drug expenditure in Canada, 1985 to 2011. Ottawa, Ontario
Carballa M, Omil F, Lema JM, Llompart MA, García-Jares C, Rodríguez I, Gomez M, Ternes T (2004) Behavior of pharmaceuticals, cosmetics and hormones in a sewage treatment plant. Water Res 38(12):2918–2926
Carter B, Campeau L (2009) The Top Rx Drugs in Canada. Pharmacy Practice:30–38
Chen M, Ohman K, Metcalfe C, Ikonomou MG, Amatya PL, Wilson J (2006) Pharmaceuticals and endocrine disruptors in wastewater treatment effluents and in the water supply system of Calgary, Alberta, Canada. Water Qual Res J Can 41(4):351–364
Comeau F, Surette C, Brun G, Losier R (2008) The occurrence of acidic drugs and caffeine in sewage effluents and receiving waters from three coastal watersheds in Atlantic Canada. Sci Total Environ 396(2):132–146. doi:10.1016/j.scitotenv.2008.02.031
Conkle JL, White JR, Metcalfe CD (2008) Reduction of pharmaceutically active compounds by a lagoon wetland wastewater treatment system in Southeast Louisiana. Chemosphere 73(11):1741–1748. doi:10.1016/j.chemosphere.2008.09.020
Crouse BA, Ghoshdastidar AJ, Tong AZ (2012) The presence of acidic and neutral drugs in treated sewage effluents and receiving waters in the Cornwallis and Annapolis River watersheds and the Mill CoveSewage Treatment Plant in Nova Scotia, Canada. Environ Res 112(1):92–99. doi:10.1016/j.envres.2011.11.011
Escher BI, Baumgartner R, Koller M, Treyer K, Lienert J, McArdell CS (2011) Environmental toxicology and risk assessment of pharmaceuticals from hospital wastewater. Water Res 45(1):75–92. doi:10.1016/j.watres.2010.08.019
Gagné F, Blaise C, Fournier M, Hansen P (2006) Effects of selected pharmaceutical products on phagocytic activity in Elliptio complanata mussels. Comp Biochem Physiol C: Toxicol Pharmacol 143(2):179–186. doi:10.1016/j.cbpc.2006.01.008
Gasser G, Pankratov I, Elhanany S, Werner P, Gun J, Gelman F, Lev O (2012) Field and laboratory studies of the fate and enantiomeric enrichment of venlafaxine and O-desmethylvenlafaxine under aerobic and anaerobic conditions. Chemosphere 88(1):98–105. doi:10.1016/j.chemosphere.2012.02.074
Ghoshdastidar AJ, Tong AZ (2013) Treatment of 2,4-D, mecoprop, and dicamba using membrane bioreactor technology. Environ Sci Pollut Res 20(8):5188–5197. doi:10.1007/s11356-013-1498-z
Ghoshdastidar AJ, Saunders J, Brown K, Tong AZ (2012) Membrane bioreactor treatment of commonly used organophosphate pesticides. J Environ Sci Health B 47(7):742–750. doi:10.1080/03601234.2012.669334
Griensven JMT, Schoemaker RC, Cohen AF, Luus HG, Seibert-Grafe M, Röthig HJ (1995) Pharmacokinetics, pharmacodynamics and bioavailability of the ACE inhibitor ramipril. Eur J Clin Pharmacol 47(6):513–518. doi:10.1007/BF00193704
Hillebrand O, Nödler K, Licha T, Sauter M, Geyer T (2012) Caffeine as an indicator for the quantification of untreated wastewater in karst systems. Water Res 46(2):395–402. doi:10.1016/j.watres.2011.11.003
Jeffrey D (2012) Raw sewage still going in harbour. The Chronicle Herald
Kim Y, Choi K, Jung J, Park S, Kim P-G, Park J (2007) Aquatic toxicity of acetaminophen, carbamazepine, cimetidine, diltiazem and six major sulfonamides, and their potential ecological risks in Korea. Environ Int 33(3):370–375. doi:10.1016/j.envint.2006.11.017
Lajeunesse A, Gagnon C, Sauvé S (2008) Determination of basic antidepressants and their N-desmethyl metabolites in raw sewage and wastewater using solid-phase extraction and liquid chromatography–tandem mass spectrometry. Anal Chem 80(14):5325–5333. doi:10.1021/ac800162q
Li X, Zheng W, Kelly WR (2013) Occurrence and removal of pharmaceutical and hormone contaminants in rural wastewater treatment lagoons. Sci Total Environ 445–446:22–28. doi:10.1016/j.scitotenv.2012.12.035
Marshall J (2008) Disposal of household special wastes. vol 2, March 27, 2008 edn. Statistics Canada
Nash JP, Kime DE, Van der Ven LTM, Wester PW, Brion F, Maack G, Stahlschmidt-Allner P, Tyler CR (2004) Long-term exposure to environmental concentrations of the pharmaceutical ethynylestradiol causes reproductive failure in fish. Environ Health Perspect 112(17):1725
Orrú M, Guitart X, Karcz-Kubicha M, Solinas M, Justinova Z, Barodia SK, Zanoveli J, Cortes A, Lluis C, Casado V, Moeller FG, Ferré S (2013) Psychostimulant pharmacological profile of paraxanthine, the main metabolite of caffeine in humans. Neuropharmacology 67:476–484. doi:10.1016/j.neuropharm.2012.11.029
Parrott JL, Bennie DT (2009) Life-cycle exposure of fathead minnows to a mixture of six common pharmaceuticals and triclosan. J Toxicol Environ Health A 72(10):633–641. doi:10.1080/15287390902769428
Pettersson I, Berg C (2007) Environmentally relevant concentrations of ethynylestradiol cause female-biased sex ratios in Xenopus tropicalis and Rana temporaria. Environ Toxicol Chem 26(5):1005–1009. doi:10.1897/06-464R.1
PDR Staff (2008) Physicians' Desk Reference. PDR Network
Rúa-Gómez PC, Guedez AA, Ania CO, Püttmann W (2012) Upgrading of wastewater treatment plants through the use of unconventional treatment technologies: removal of lidocaine, tramadol, venlafaxine and their metabolites. Water 4(3):650–669. doi:10.3390/w4030650
Scheurer M, Michel A, Brauch H-J, Ruck W, Sacher F (2012) Occurrence and fate of the antidiabetic drug metformin and its metabolite guanylurea in the environment and during drinking water treatment. Water Res 46(15):4790–4802. doi:10.1016/j.watres.2012.06.019
Ternes T, Bonerz M, Schmidt T (2001) Determination of neutral pharmaceuticals in wastewater and rivers by liquid chromatography–electrospray tandem mass spectrometry. J Chromatogr A 938(1):175–185. doi:10.1016/S0021-9673(01)01205-5
Thomas PM, Foster GD (2005) Tracking acidic pharmaceuticals, caffeine, and triclosan through the wastewater treatment process. Environ Toxicol Chem 24(1):25–30. doi:10.1897/04-144R.1
Wilcox JD, Bahr JM, Hedman CJ, Hemming JDC, Barman MAE, Bradbury KR (2009) Removal of organic wastewater contaminants in septic systems using advanced treatment technologies. J Environ Qual 38(1):149–156. doi:10.2134/jeq2007.0365
Yargeau V, Lopata A, Metcalfe C (2007) Pharmaceuticals in the Yamaska River, Quebec, Canada. Water Qual Res J Can 42(4):231–239
Acknowledgments
The authors appreciate financial support from Acadia University and Canada Foundation for Innovation (CFI). The authors would also like to thank Brian Crouse and Martin Sichinga for technical assistance. The authors are grateful to numerous STP technicians and engineers who were very helpful in assisting sample collection.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Leif Kronberg
Rights and permissions
About this article

Cite this article
Ghoshdastidar, A.J., Fox, S. & Tong, A.Z. The presence of the top prescribed pharmaceuticals in treated sewage effluents and receiving waters in Southwest Nova Scotia, Canada. Environ Sci Pollut Res 22, 689–700 (2015). https://doi.org/10.1007/s11356-014-3400-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-014-3400-z