
Abstract
In the United States, an estimated 100,000 anterior cruciate ligament (ACL) injuries occur every year. Despite decades of research, to this date, the mechanism or mechanisms of non-contact ACL injuries are not well understood. This is primarily because trials cannot be conducted on live subjects to understand the injury mechanism, and it is difficult to instrument a live human knee to measure the response of tissues during dynamic activities. In this paper, we present a dynamic knee injury simulator capable of in-vitro modeling of the ACL injury during jump-landing activity. This system was used to simulate jump-landing on cadaveric knees and to successfully test which conditions would result in isolated ACL injury. A restricted flexion of the hip (a hip that flexes minimally or not at all during landing), combined with low quadriceps and hamstring force levels during landing were found to be conducive to ACL injury. Elevated levels of quadriceps force prevented the injury from occurring even under restricted hip flexion conditions. The measured strain rates in the ACL tissue during injury causing activities were over 250%/s.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
The human anterior cruciate ligament (ACL) is one of the four ligaments of the knee that connects the femur to the tibia. The ACL is the primary restraint against the forward-sliding of the tibia relative to the femur (anterior tibial translation) and also against the inward rotation of the tibia relative to the femur (internal tibial rotation). Both of the tibial movements, mentioned above, occur frequently during athletic activities, and the knee capsule, its musculature, and its ligaments are normally completely capable of stabilizing the knee, resulting in smooth and sometimes incredible athletic movements without injury. However, in some instances, around 100,000–300,000 cases annually, the stability of the knee is compromised, and the ACL tears completely or partially. Astonishingly, about 70% of these failures are classified as non-contact (no external loads from collisions or other sources during the incident). These non-contact ACL injuries occur during activities such as pivoting or side-step cutting, decelerating while the knee is at an extended position, or landing from a jump. The reasons as to why these injuries occur when the injured person has performed the same activity countless times prior to the eventual injury are not yet known.
In a detailed review of the state of the art by Hewett et al. [1], it is clear that a large body of research and scientific activity has been devoted to neuromuscular control (or lack thereof) as a possible cause for the non-contact ACL injuries. The idea is that various muscles of the knee, i.e., the quadriceps group, hamstring group, gastrocnemius, as well as hip muscles must be activated at the proper time and with proper force to assist the ACL in maintaining the stability of the knee. If, for any reason, the firing pattern or the magnitude of the force by which the muscle pulls on the bones of the knee is improper, the ACL will then take the brunt of the load and in some instances it will tear. This area of research seems to be very promising in eventually solving the puzzle of the non-contact ACL failure because, after all, without proper muscle support, the ACL does not have any protection against dynamic failure. As a result, recent research has focused on the role of muscle activity as ACL agonist (protecting the ACL by reducing its strain) or as ACL antagonist (causing undesirable tensile strain on the ACL) during various activities.
The mechanism of ACL injury is rather complex due to the following reasons: (a) the knee is a complex joint capable of interrelated translation along and rotation about various axes, (b) the injury condition is dynamic, and (c) the duration of the injury event is short. Further, it is difficult to instrument a live human knee to measure the response of tissues during dynamic loading. To date, no one has been able to simulate the isolated disruption of the ACL, in-vitro (in an artificial environment outside the body such as in a cadaveric study), under physiological loading conditions, as related to a specific high-risk activity. Such in-vitro simulations, if possible, could shed light on the relevance and practicality of various ACL injury mechanisms mentioned above. These systems could also assist with developing training strategies for ACL deficient and reconstructed knees, as well as injury prevention strategies.
In this paper, we present a system capable of in-vitro simulation of the jump-landing activity including the activities of the quadriceps and hamstring muscles, the flexion of the hip, and the ground reaction force. The system uses an instrumented knee to monitor the strain on the ACL during the landing process. We also present our preliminary results showing success at injuring the ACL of an intact knee capsule under specific conditions during the jump-landing process.
2 Materials and Methods
2.1 Experimental Setup
The jump-landing simulator was designed to enable dynamic loading of cadaveric knee joints (similar to one-legged landing) with the ability to apply dynamic muscle forces. The setup was designed so that it simulates realistic jump-landing as closely as possible while allowing for slight variability in the simulated landing style. During a typical jump-landing activity, the knee is slightly flexed, the vertical ground reaction force (GRF) is applied to the tibia, and the muscles of the hip and the knee fire (contract) to stabilize the knee and the body (Fig. 1). To replicate this scenario, a simulator has to provide a means of (a) applying hamstring and quadriceps muscle forces and the GRF, (b) allowing the sagittal (side) plane rotation of the ankle and hip joints, and (c) adjusting various antero-posterior positions of the hip with respect to the ankle joint.

Simulated forces (solid arrows) and degrees of freedom (blank arrows) during jump landing simulation. The dotted arrows represent the option to lock that degree of freedom. For example, the hip joint could be either free to rotate or locked at a given hip flexion angle
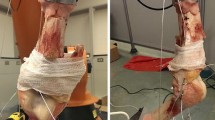
The setup, along with a cadaver knee joint mounted on it, is shown in Fig. 2. It consists of a frame that secures the cadaver knee joint in any desired position, electric actuators to simulate muscle action, and drop weight to simulate impact at landing. The tibial and femoral ends of the knee can be secured in steel cups and can be mounted on the frame using two coupler rods at both ends (shown schematically in Fig. 3). The coupler rods allow for adjustments in the length of the femur and the tibia. The ankle joint and the hip joint were simulated as simple hinges.

The dynamic knee injury simulator and some of its key features: (a) Femoral attachment; (b) Tibial attachment; (c) Knee; (d) Impact plate; (e) Actuator and load sensor

The schematic of dynamic knee injury simulator showing the design details in various regions: (a) Femoral attachment and hip joint; (b) Tibial attachment, U plate, yoke joint assembly; (c) Knee and DVRT; (d) Impact plate, impact sensor, and sensor plate
At the femoral end, the coupler rod is connected to a cylinder to represent the hip joint as schematically shown in Fig. 3(a). This will allow flexion-extension of the hip joint and has the ability to lock the hip joint at a specific angle. This cylinder can move in the slots of the frame and can be secured to the frame at any position if needed. This allows positioning of the desired antero-posterior hip position and desired initial hip flexion angle.
A close-up view of the tibial end arrangement is given in Fig. 3(b). The tibial end of the coupler rod is connected to an eye bolt, which in turn is free to rotate in the sagittal plane around a rod-‘U’ plate assembly. This simulates the unrestrained ankle flexion that takes place during one-legged jump-landing. The ‘U’ plate is slotted at the bottom and is connected to a yoke joint. This yoke joint allows for the knee to be secured in any valgus–varus angle [see enlarged coronal view of Fig. 3(b)]. The yoke end is in-turn movable in a slotted base plate. This makes any deired position of the ankle in the coronal (frontal) plane possible. The base plate, at either end, has linear bearings that move up-down on bearing shafts. This simulates relative change in vertical distance between the hip and ankle joints when the GRF is applied during landing. A piezoelectric impact load sensor (Model 200B05, PCB Piezotronics Inc, NY) is secured between the two coupler rods to measure the ground reaction force during landing (Fig. 3). A similar load sensor is placed on the femoral side of the knee.
In order to simulate the hamstring and the quadriceps muscle forces, two high-speed servo-electric actuators (TC3 Series, Danaher motions, IL) were used (Fig. 2). These actuators were controlled through a B8962 (Danaher motions, IL) programmable controller. The actuators have the capacity to operate in a position-controlled mode and/or to apply constant muscle forces. Two load cells (Honeywell Sensotec®, OH) are attached to the thrust rods to measure the muscle forces. Two P3500 (Vishay Measurement Group, CT) signal conditioners are used to condition the data from the load cells before recording it in a computer. In order to connect these thrust rods of the actuators to hamstring and quadriceps insertion sites, a series of pulley systems with steel cables (McMaster-Carr, GA) was used. To attach the knee to the cable, holes were drilled in the patella and tibia and stainless steel wires were used as connectors. In order to measure the strain in the ACL, a differential variable reluctance transducer (DVRT, Microstrain®) was used as shown in Fig. 3(c). A personal computer and a data acquisition system (National Instruments, TX) were used to record the data from the load cells and the DVRT.
The GRF during landing is delivered to the tibial end through an impact plate-lever setup. A schematic of the impact plate-lever setup is given in Fig. 3(d). The setup consists of an impact plate which slides up-down a bearing shaft through linear bearings. The impact plate has a central rod which can be used to add weights to get the desired impact force. The impact plate can be raised to the desired height manually, and then dropped. The plate then hits a lever arm. The other end of the lever arm rises up rapidly to apply the GRF to the tibial base plate. A sheet of bubble wrap is placed between the lever plate and the base plate to attenuate the impact force so that the ground reaction force raises gradually as in a real life situation (due to muscles and tendons in the ankle). The thickness of this bubble wrap sheet is adjusted so that the GRF is applied in about 0.1 s, as in case of a typical jump-landing activity. An optional simple mechanism was designed to ‘anticipate’ the impact, so that the muscle actuators can be activated just before the impact. This simulates the concentric muscle contraction before landing. A steel rod of specific length (impact sensor) was loosely mounted on the impact plate. During the fall, the steel rod comes in contact with an aluminium sensing plate just before the impact plate hits the lever arm [Fig. 3(d)]. This will close a control circuit that activates the actuators to develop the muscle forces. The time duration between this activation and actual impact can be controlled by varying the length of the steel rod. In some tests, a high speed camera capable of 500 frames per second (A504k from Basler Inc, PA) was used to follow the path of the knee in the sagittal plane after impact.
In the above setup, the landing is simulated in a manner opposite to how it happens during the actual activity. During actual landing, just before contact, the knee is slightly flexed and impact is initiated by the body’s contact with the ground (the body moves and the ground is stationary). Obviously, in-vitro, it is very challenging to accelerate a flexed knee and allow it to impact the ground; thus, alternatively, the option of keeping the knee stationary (at a flexion angle similar to that observed in-vivo) and allowing the ground to initiate the impact was used in this design. Biomechanically, these situations are equivalent.
2.2 Experimental Procedure
Nine fresh-frozen cadaveric knees (both male and female subjects were used) from five donors were obtained. The ages of all donors were between 26 and 67 years. The knees had no signs of prior injury or knee degeneration. The knees were thawed overnight before the experiments and all the soft tissue around the knee joint was dissected; the knee capsule was left intact. The knees were mounted on the frame and the actuators were connected to the muscle insertion sites. A calibrated DVRT was mounted on the ACL when the knee was at approximately 20° flexion (with no muscle forces) and the initial length was recorded. This was considered as the reference length (thus we are excluding the strain that would occur due to 20° flexion of the knee). The strain was measured by dividing the elongation measured by the DVRT by the reference length. Furthermore, the ACL strain was measured in two parts: (1) before impact due to action of the applied pre-tension (static strain) and (2) during impact due to simulated landing (dynamic strain).
The aim of the experiments was to cause isolated ACL injuries on cadaveric knees during jump-landing by controlling the muscle forces and hip flexion and to find out which combinations of these factors result in isolated ACL injury. Accordingly, several trials were performed for each knee with various amounts of initial flexion angles (10–40°), applied impact force (1,100–1,400 N), various amounts of quadriceps/hamstring pre-tensions, different valgus angles (0–10°), and with free or locked hip flexion. The forces from the load cells and the strain from the DVRT were synchronously measured. Whenever an abnormal response from the DVRT was recorded, the ACL was examined to confirm its integrity.
For reference, at flexion angles around 20°, the peak quadriceps load is 20–40% of its maximum value [2]. It has been shown that under strict and non-physiological conditions (without ground reaction forces at a locked flexion angle) a static quadriceps force of 4,500 N can cause injury to the ACL [3]. Thus, in this paper, the pre-tension levels used for the quadriceps are considered “large” if they are 20–40% of the projected failure load of 4,500 N. Also, for reference, the forces generated during landing activities are 2–4 times the body weight [4]. A landing force of 1,200 N represents, more than twice the body weight of a 60 kg person and is considered a “moderate” landing or ground reaction force.
3 Results
Out of the nine knees that were tested, the first five knees were used to fine-tune the procedure of the experiments and to cause isolated injuries under various conditions at various degrees of flexion. In this first series of experiments, all of which were under a free hip flexion protocol, our attempts to cause isolated ACL injuries were not successful. The tests revealed that the knee joint in general is very stable and very protective of the ACL. Even under a combination of extreme valgus (∼10°), large quadriceps pre-tension (∼1,500 N), and moderate ground reaction loads (∼1,400 N), the ACL could not be injured. Although none of the ACLs failed, the visual analysis of the knees during this first series of tests provided the authors with ideas and directions to take toward isolated damage of the ACL. One such direction was to restrict the hip flexion levels during the landing process and test various quadriceps loads.
In the second series of tests, an ACL tear was achieved (emanating from the condylar roof through the mid-substance) when the initial knee flexion angle was 20°, the quadriceps pre-tension was about 165 N, hamstring pre-tension was not applied, a ground reaction force of 1,120 N was applied, and the hip flexion was restricted (not allowed or minimally allowed during impact). In this series a maximum dynamic ACL strain of 11.6% was recorded. In the third series, we used identical conditions (hip flexion was restricted) but we started with a larger quadriceps pre-tension (650 N compared to 165 N in the previous case). This condition did not yield large ACL strains; on the contrary, as pre-tension increased above 650 N, the strain in the ACL decreased. When larger quadriceps pre-tensions and a moderate ground reaction force (exceeding 1,300 N) were applied simultaneously, under a restricted hip motion condition, the femur fractured without any damage to the ACL. In the fourth series, an isolated ACL tear was again achieved with a quadriceps pre-tension of 40 N. The pattern of failure was similar to that observed in series two but there was also damage in the form of avulsion at the tibial attachment site. The corresponding maximum dynamic strain was measured to be 10.7%. In the fifth series, a quadriceps pre-tension of 50 N was applied. The corresponding measured dynamic strain was approximately 9.0%. However, in this case, no visible ACL tear was observed but the ACL was stretched to a point that the knee was completely lax (slack). Considering that the antero-medial bundle of the ACL, where the DVRT is mounted, undergoes minimum strain when compared to other parts of the ACL, this is a significantly large strain.
In addition to the failure tests, the following observations were made from non-injury-causing experiments in which hip flexion was allowed (normal landing conditions): the strain in the ACL increases as the quadriceps pre-tension increases before the actual landing process (static strain); i.e., a positive correlation coefficient, r, is calculated between quadriceps pre-tension and the static strain as shown in Fig. 4 (R 2 = 0.83, r = +0.91). Conversely, during the landing phase (when the GRF is applied), the dynamic ACL strain was found to be negatively correlated to the maximum quadriceps force; one such case in which the hamstring pre-tension is also zero is shown in Fig. 4 (R 2 = 0.72, r = −0.84).

The relationship between the maximum ACL strain and quadriceps force before (static strain) and during (dynamic strain) landing
4 Discussion
This is the first published report on the success of simulating isolated ACL injuries during jump-landing under physiological conditions. Published literature exists about success in replicating the knee dynamics on cadaveric knees using custom-built dynamic knee simulators [5]. However, their use is limited to the study of less dynamic activities such as walking and stair climbing. One recent report by Withrow et al. [4] has been on the simulation of jump-landing activity using a custom-built simulator. In their experiments, they have not reported successful isolated ACL tears. We believe that this is mostly because, in their experiments, all tests were performed under a freely flexing hip condition and the muscle forces were high.
The capabilities of our system as far as control of various input parameters such as hamstring and quadriceps pre-tensions, drop height, impact mass, knee orientation, and actuation rates were tested in this research. The observable output variables such as dynamic impact force and ACL strain are also measured using the system. The system has flexibility to test a wide variety of conditions and theories.
The biomechanical data gathered during the testing of knees reveal certain important issues. The first issue is that the ACL strain must be monitored in two distinct parts: a pre-impact, muscle-based, static part and a during-impact, dynamic part. This separation is helpful in recognizing the role of the quadriceps muscle during jump-landing. Correspondingly, the results show that increasing pre-tension in the quadriceps increases the tensile strain in the ACL prior to impact (r = +0.91; Fig. 4). This result is consistent with other findings in literature. Renstrom et al. [6] reported that isolated quadriceps force of 400 N increased the strain in the ACL at flexion angles of 0–45°. Durselen et al. [7] reported that at 140 N quadriceps load, the ACL strain (2.5%) was at its maximum at about 25° flexion. Draganich and Vahey [8] also reported a similar observation. All of the above observations are under static conditions. Based on such observations, it is widely accepted in the research community that higher quadriceps forces play a major role in ACL injury. Based on these assumptions, DeMorat et al. [3] showed that the ACL can be injured at an isolated quadriceps load of 4,500 N under the strict condition that knee flexion is fixed. However, all the above-cited experiments neglect the effect of the GRF and thus do not replicate a realistic mechanism of injury.
According to our results, the dynamic component of strain reduces with increasing quadriceps force and thus, contrary to common belief, large quadriceps forces play a protective role during the landing process (r = −0.84; Fig. 4). The only condition under which quadriceps forces could injure an ACL is if the quadriceps pre-tension before landing is unrealistically high to the point where the ACL will fail before landing (not possible under normal landing conditions). During landing, when GRF is present, under a large quadriceps force, the ACL failure is unlikely to happen because the anterior force vector of the quadriceps muscle on the tibia, which causes anterior tibial translation, decreases as the tibia moves forward and at a certain point, vanishes. Any further increase in the quadriceps muscle force can only help in increasing the joint compression force which is a positive influence in maintaining the stability of the joint and protecting the ACL. Further, quadriceps muscle contraction before landing is usually accompanied with hamstring contraction thus preventing the anterior tibial translation.
The suggested protective role of the quadriceps with respect to the ACL is not altogether new. Aune et al. [9] reported that a higher anterior tibial force was needed to tear the ACL when an 889 N quadriceps load was applied, compared to when a 5 N quadriceps load was applied. However, some researchers criticise their findings because, with the exception of the ACL, patellar tendon, and the menisci, all surrounding knee capsule tissues were removed prior to testing. We believe that the work by Aune et al. [9] was accurate and the surrounding tissue that were cut played little role in their conclusions. Bodor [10] also supported the protective effect of the quadriceps using ultrasound techniques.
Our results are contradictory to those reported by Withrow et al. [4] who suggest that when dynamic strain data from eleven different knees (each tested 25 times), under simulated landing conditions, were plotted against the corresponding quadriceps force values, a strong positive correlation (R 2 = 0.74, r = +0.86) was observed. Thus their results indicate that as quadriceps force increases, the dynamic strain in the ACL during the landing process increases. It is important to note that since each cadaveric knee has a different joint geometry and a distinct ACL response (due to differences in properties), the correlation analysis would have been more meaningful if it had been performed individually for each knee and not collectively for all knees. The authors did not provide an individual correlation analysis for each knee, thus one cannot know whether this strong positive correlation also existed in each individual knee.
In all our successful injury simulations, in addition to low quadriceps pre-tension, the hip flexion was also restricted. Having only low quadriceps pre-tension or only restricted hip flexion failed to produce an ACL injury. A restricted hip flexion from a kinesiology point of view would occur when the subject relies on his or her hip musculature to decelerate during landing. In other words, instead of relying on the quadriceps muscle to keep the knee from excessive flexion, the subject relies on hip extensors to remain upright. Nyland et al. [11, 12] have shown a late onset of quadriceps and hamstring muscle activation in running and rapid-stop tasks due to fatigue. If these muscles activate late due to fatigue during landing, then the hip extensor muscles will have to fire to prevent the body from collapsing. Relying on hip muscles will restrict the angular rotation of the femur in the sagittal plane (stops hip flexion rapidly). When the hip flexion is restricted, the ground reaction force wants to flex the knee but cannot. As a result, large joint reactions forces will develop that will cause anterior tibial translation (the femur is locked in place and does translate posteriorly, thus the tibia must translate anteriorly). This was verified using high-speed photography during one of our injury simulations. With low quadriceps pre-tension, free hip flexion would result in no anterior tibial translation [Fig. 5(a) and (b)]. When the hip flexion was restricted, anterior tibial translation resulted and the ACL was injured [Fig. 6(a) and (b)]. If hip flexion is allowed, the GRF will be attenuated over a longer period of time and hence high joint reaction forces will not develop. This theory is also supported by a recent study by Yu et al. [13]. If the quadriceps pre-tension is high, it will keep the anterior tibial translation low through joint compression. It is very important to note that our results showed that restricted hip flexion alone can not cause ACL damage as long as high quadriceps muscle forces are at work. High quadriceps forces will protect the knee during jump-landing even if the hip flexion is restricted. Our observations also verified the protective nature of hamstring muscles in those cases that hamstring muscle was active.

High speed photographs during simulation with free hip flexion showing a minute relative anterior movement between a marker on the femur and a corresponding marker on the tibia

High speed photographs during simulation with restricted hip flexion showing a large relative anterior movement between a marker on the femur and a corresponding marker on the tibia
Analysis of the strain rate during physiological loading has never been performed in-vitro. The strain rates in the ACL during safe and injurious landing situations have been unknown. The analysis of our strain data measured through the duration of impact show that, under safe landing conditions, the strain rate is between 60 and 80%/s while during injury conditions, the strain rate increases to more than 250%/s. This is a very important point for the determination of ACL and ACL graft properties since such tissues are viscoelastic. The mechanical property tests should be performed at strain rates between the safe and injurious conditions.
This study has some major limitations. The focus of this research has been on the role of the quadriceps muscle because of the contradictory opinions and observations in literature. Thus, we assume that the subjects have very weak hamstring forces and offer no resistance to anterior tibial translation (the muscle activation is delayed). This condition can occur when the athlete is fatigued. In such cases, both quadriceps and hamstring muscle forces can be very low. The role of several other muscles such as calf muscles, knee abductors/adductors, and the ankle has been neglected in our system. Further improvements in the system can be made by adding more actuators to simulate more muscles actively. Since this was a pilot study which focused on finding the conditions conducive for ACL injury, and the availability of cadaveric knees was limited, not every knee was used in the same way. Different conditions were tried with different knees to successfully simulate the ACL injury. Now, that the conditions needed for successful simulation are known, more systematic studies can be conducted by the research community.
5 Conclusion
A new state of the art jump-landing simulation system capable of monitoring a large number of input variables and dynamically recording a significant number of output variables was designed, constructed, and tested. The results show that the quadriceps may have a protecting effect on the ACL due to joint compression during jump-landing. Accordingly, the results showed that non-contact isolated ACL injury can be simulated in the laboratory when the flexion rate of the hip is restricted, the quadriceps and hamstring muscle forces are kept low, and a moderate ground reaction force due to landing is applied. A restricted hip flexion rate is defined as either none allowed or stopped rapidly with a high angular deceleration rate (minimal hip flexion allowed). This may be considered as a new non-contact injury mechanism controlled primarily by sagittal plane loads but that could be exacerbated by coronal (varus/valgus) and transverse (internal/external rotation) plane loads. We also found that the strain rate in the ACL is high during both safe and injurious conditions (ranging from 60%/s for safe to 261%/s for injurious conditions). Future studies analyzing sex-based differences in the ACL injury may consider the post-landing hip flexion differences (hip flexion change from landing to complete stop) between sexes as one key parameter.
References
Hewett TE, Myer GD, Ford KR (2006) Anterior cruciate ligament injuries in female athletes. Am J Sports Med 34:299–311.
Zernick RF, Garhammer J, Jobe FW (1977) Human patellar tendon rupture. J Bone Jt Surg Am 34:312–315.
DeMorat G, Weinhold P, Blackburn T, Chudik S, Garrett W (2004) Aggressive quadriceps loading can induce noncontact anterior cruciate ligament injury. Am J Sports Med 32:477–483.
Withrow TJ, Huston LJ, Wojtys EM, Ashton-Miller JA (2006) The relationship between quadriceps muscle force, knee flexion, and anterior cruciate ligament strain in an in-vitro simulated jump landing. Am J Sports Med 34:269–74.
Maletsky LP, Hillberry BM (2005) Simulating dynamic activities using a five-axis knee simulator. J Biomech Eng 127:123–133.
Renstrom P, Arms SW, Stanwyck TS, Johnson RJ, Pope MH (1986) Strain within the anterior cruciate ligament during hamstring and quadriceps activity. Am J Sports Med 14:83–87.
Durselen L, Claes L, Kiefer H (1995) The influence of muscle forces and external loads on cruciate ligament strain. Am J Sports Med 23:129–136.
Draganich LF, Vahey JW (1990) An in-vitro study of anterior cruciate ligament strain induced by quadriceps and hamstring forces. J Orthop Res 8:57–63.
Aune AK, Cawley PW, Ekeland A (1997) Quadriceps muscle contraction protects the anterior cruciate ligament during anterior tibial translation. Am J Sports Med 25:187–190.
Bodor M (2001) Quadriceps protects the anterior cruciate ligament. J Orthop Res 19:629–633.
Nyland JA, Shapiro R, Stine RL, Horn TS, Ireland ML (1994) Relationship of fatigued run and rapid stop to ground reaction forces, lower extremity kinematics, and muscle activation. J Orthop Sports Phys Ther 20:132–137.
Nyland JA, Shapiro R, Caborn DNM, Nitz AJ, Malone TR (1997) The effect of quadriceps femoris, hamstring, and placebo eccentric fatigue on knee and ankle dynamics during crossover cutting. J Orthop Sports Phys Ther 25:171–184.
Yu B, Lin C, Garrett WE (2006) Lower extremity biomechanics during the landing of a stop-jump task. Clin Biomech 21:297–305.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hashemi, J., Chandrashekar, N., Jang, T. et al. An Alternative Mechanism of Non-contact Anterior Cruciate Ligament Injury During Jump-landing: In-vitro Simulation. Exp Mech 47, 347–354 (2007). https://doi.org/10.1007/s11340-007-9043-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11340-007-9043-y