
Abstract
Mandibular repositioning appliances (tMRAs) designed with a titratable mechanism are effective to treat obstructive sleep apnea syndrome (OSAS) but are not widely used, although many studies have proven their value. The aim of the present study was to evaluate the efficacy of tMRAs in the treatment of OSAS on the criteria of the American Academy of Sleep Medicine (AASM; apnea/hypopnea index [AHI] < 5). Three hundred consecutive patients with a polysomnographic diagnosis of OSAS were referred for treatment with tMRAs between 2000 and 2003. Thirty-eight patients were excluded, and 262 concluded the titration protocol with tMRA that lasted 4 months. After titration, the patients were referred for a medical reassessment, and 83 patients (70 men) participated in the new polysomnographic exam with tMRA in place to access tMRA’s efficacy. The mean pre- and post-treatment AHI were 26 ± 17.7 and 4.8 ± 5.3 events per hour, respectively (p < 0.00005). Fifty-three (62.6%) of the 83 patients were treated successfully (AHI < 5). Twenty-three patients had severe OSAS, and 12 of them (52.1%) were treated successfully (AHI < 5). Forty patients had moderate OSAS, and 26 of them (65%) were treated successfully. Twenty patients had mild OSAS, and 15 (75%) were successfully treated. Even when applying more rigid criteria such as those of the AASM, the expressive success rate obtained with the treatment of different degrees of OSAS indicates that tMRAs are an additional valuable option even for cases of severe apnea in which the patient does not tolerate continuous positive airway pressure or cannot afford this treatment, a fact quite common in Brazil and other developing countries.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnea syndrome (OSAS) is highly prevalent and associated with cardiovascular morbidity and deaths [1–3]. Positive airway pressure (PAP) devices are the gold standard treatment. The American Academy of Sleep Medicine (AASM) considers abnormal an apnea/hypopnea index (AHI) above five events per hour, and to bring an OSAS patient to an AHI below five events per hour is one of the major goals when using PAPs [4]. Besides, highly efficacious PAPs are not fully accepted by the patients, and those who start treatment have a low compliance, meaning that they do not use the device all days in the week, and also around 4 h per night [5, 6]. Such poor compliance with PAP treatment may be the reason why a recent study suggests that PAPs for OSAS patients were not fully effective in preventing stroke and deaths of any causes [7].
Among the treatment options for OSAS, the mandibular repositioning appliances (MRAs) with a titration mechanism (tMRAs) are very promising, but important data demonstrating their role have appeared only in specialized journals. Actually, many studies regarding MRAs are published in journals where the main issue is dentistry, preventing the majority of the physicians from accessing essential information already available about MRAs in the treatment of OSAS [8–10].
tMRAs are designed to gradually advance (titration) the mandible forward. And the sleep specialist dentist works weekly with the patient to achieve the mandibular position that is comfortable for the patient to sleep with, and at the same time resolutive regarding the AHI that has to be less than five events per hour, considering AASM criterion [4, 9, 11, 12].
There are few studies about OSAS treatment with MRAs showing outcomes with AHI below five events per hour. Therefore, the main goal of this study is to verify the efficacy of two tMRAs (ARMIO™ and Klearway™) in reducing AHI to a level below five events per hour [13–15].
Materials and methods
Patients
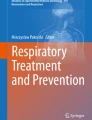
A total of 300 consecutive patients with a polysomnographic diagnosis of OSAS were referred for treatment with tMRA (260 were treated with ARMIO™ and 40 with Klearway™) between 2000 and 2003. Thirty patients were excluded from the treatment due to clinical–dental problems such as an insufficient number of teeth for stabilization of the appliance in the mouth, periodontal disease, and problems in the temporomandibular joints, and eight patients discontinued the use of the appliance already at the beginning of the protocol. Thus, 262 patients received a tMRA using a titration protocol that lasted 4 months. At the end of the titration period, the patient was referred for clinical reassessment and control polysomnography with the tMRA in place. After medical reassessment, 83 patients (62 treated with ARMIO™ and 21 with Klearway™) participated in a new polysomnographic exam (Fig. 1).

Fluxogram
The mean age of the 83 patients (13 women and 70 men) was 50.6 ± 11.2 years. OSAS was mild (AHI = 5–<15 episodes per hour) in 20 patients, moderate (AHI = 15–30 episodes per hour) in 40, and severe (AHI > 30 episodes per hour) in 23 (Table 1).
Polysomnography
Standard polysomnograms were obtained with a Neurotec apparatus (model EQSA-400), and the following parameters were recorded: electroencephalogram (C3, C4, A1, A2); right and left electrooculograms; submental and anterior tibial electromyogram; oral and nasal flow (thermistor); respiratory effort (piezoelectric belt sensors on the abdomen and chest); and electrocardiogram (modified D1). Sleep was staged according to the international criteria of Rechtschaffen and Kales [16]. Respiratory sleep disorders were diagnosed based on the criteria of the AASM [4].
Treatment
During the 4 months of the titration protocol, the patients were seen weekly at the office for titration of the tMRA according to their report of weekly progress. The tMRAs were titrated on an increasing scale until maximal mandibular advancement was achieved with comfort for the patient. Termination of the protocol was defined as the end of the fourth month of titration even when the patient still presented daytime symptoms, or before if the patient reported complete and subjective disappearance of the classical symptoms of OSAS. When symptoms of excessive daytime sleepiness or variable subjective complaints persisted even after the end of the titration period, the patients were referred to the responsible physician for reassessment and exclusion of other causes associated with the symptoms such as narcolepsy, restless leg syndrome, periodic limb movements during sleep, insomnia, and other clinical diseases [17].
After titration of the tMRAs, all patients were referred to their physicians for control polysomnographic reassessment with the appliance in place to determine the efficacy of treatment. During this phase, 83 patients returned for control polysomnography. After the end of the protocol, these patients returned to the dental office every 6 months on average for follow-up, revision of the appliance, and/or small repairs.
Patients presenting an AHI <5 events per hour upon control polysomnography were considered to have been treated successfully [4]. Although conceptually incorrect and not the therapeutic approach for our patients, treatment was also analyzed using a criterion called liberal, which was an AHI <10/h as widely used in other published studies.
Titratable mandibular repositioner appliances
The Brazilian titratable mandibular repositioning appliance ARMIO™ and the Klearway™ are custom oral appliances fabricated using the same criteria as described elsewhere [12, 17–19]. In short, these appliances were designed to maintain the mandible in a more anteriorized position than usual during sleep, increasing airway dimensions. Although the two appliances have different designs, both of them consist of two acrylic plates (ARMIO™ is made of hard acrylic and Klearway™ is made of thermoactive acrylic) completely covering the upper and lower arch, and a specific stainless-steel threaded screw mechanism of each appliance connected the two plates allowing only lateral movements for ARMIO™ and lateral and limited vertical movements for Klearway™. The possibility of weekly titration in tenths of millimeters during the treatment protocol is the major characteristic of these two appliances.
Variables studied
The explanatory variables used were gender (male and female), body mass index (BMI), pre- and post-treatment AHI, and age above and below 60 years.
Statistical analysis
The mean polysomnographic results were compared before and after treatment with the tMRAs by the t test. For descriptive analysis of the data, the absolute (AD = AHIpre − AHIpost) and relative differences [RD = (AHIpre − AHIpost) ÷ AHIpre] before and after treatment were considered, where AD is the absolute difference between polysomnographic recordings indicating how much the AHI decreased after treatment, and RD is the relative difference between polysomnographic recordings indicating the percent decrease in the AHI.
In addition to these variables, the pre-treatment AHI was classified as follows: 5 to <15/h = mild apnea; 15 to 30/h = moderate apnea; and >30/h = severe apnea [4].
A multiple linear regression model was used to determine the correlation between the post-treatment AHI (AHIpost) and the pre-treatment AHI (AHIpre), gender, age (years), and BMI (kg/m2) [20]. To adequately fit the model, logarithmic transformation of the pre- and post-treatment AHI was necessary, resulting in the following model: ln(AHIpost + 1) = ln(AHIpre + 1) + b 1 + b 2 + b 3 + K + Ý, where b 1 = age, b 2 = BMI, b 3 = gender, ln = natural logarithm, K = constant, and Ý = random error.
The final model shows the following relationship: AHIpost = (AHIpre)0,445. This formula is not a predictive equation but is used only to understand the results of the descriptive analysis, i.e., the poorer the initial state of the patient, the more effective the appliances.
To measure the efficacy of the appliances, treatment outcome was classified as follows: treated, patients presenting an AHI <5/h, and untreated, patients presenting an AHI ≥5/h.
Results
The mean pre- and post-treatment AHI were 26 ± 17.7 and 4.8 ± 5.3 events per hour (p < 0.00005). Fifty-three (63.8%) of the 83 patients were treated successfully (AHI < 5/h).
AASM criterion (AHI <5 events per hour)
Severe apnea
Twenty-three patients had severe OSAS, and 12 (52.1%) of them were successfully treated (Table 2). The mean number of obstructive events decreased from 39.3 ± 8.5/h to 1.5 ± 1.2/h in this group of treated patients, whereas in patients considered to be untreated, the mean number of events fell from 55.0 ± 26.4/h to 13.2 ± 6.9/h (Table 3).
Moderate apnea
Forty patients had moderate OSAS, and 26 (65%) were successfully treated (Table 2). The mean AHI fell from 22.2 ± 4.6/h to 1.8 ± 1.6/h in the treated group and from 21.6 ± 4.1/h to 9.1 ± 3.7/h in the untreated group (Table 3).
Mild apnea
Twenty patients had mild OSAS, and 15 of them (75%) were successfully treated (Table 2). The mean AHI fell from 10.4 ± 2.8/h to 1.9 ± 1.3/h in the treated group and from 12.5 ± 2/h to 7 ± 1.3/h in the untreated group (Table 3).
Liberal criterion (AHI <10 events per hour)
Severe apnea
Seventeen (65%) of the 23 patients with severe OSAS were treated successfully.
Moderate apnea
Thirty-five (86%) of the 40 patients with moderate OSAS were treated successfully.
Mild apnea
All (100%) of the 20 patients with mild OSAS were treated successfully with the tMRAs (Table 2).
The mean decrease in the AHI was 21 units in absolute terms, and the mean relative decrease was 80%.
The multiple linear regression model showed that only the pre-treatment AHI was significantly correlated with post-treatment AHI (p = 0.01). No correlation was observed between the post-treatment AHI and BMI, age, or gender.
Considering the categorized pre-treatment AHI, the box plots of the absolute and relative differences clearly show that the more severe the pre-treatment apnea, the greater the absolute and percent decrease in the AHI after treatment (Fig. 2). Taking into account the degree of apnea severity at the beginning of treatment, a decline in the percentage of treated subjects was observed with advancing disease.

Box plots of the AD and RD according to the severity of pre-treatment apnea
Considering the whole sample, the proportion of treated patients was estimated to be 64%, with a 95% confidence interval of 0.53 to 0.74.
Discussion
We have shown in this study that intra-oral appliances are efficacious in treating OSAS. These appliances bring 75% of patients with mild OSAS, 65% with moderate OSAS, and 52% with severe OSAS to an AHI that is considered normal. Information on the role of intra-oral appliances in treating OSAS is not yet readily available in the medical literature, but many patients all around the world would benefit greatly from this intervention.
One important point that may define the degree of success of this type of treatment is the final titration of the mandibular protrusion. This must always be done individually, exploring the maximum mandibular advancement possible, while at the same time respecting each patient’s limits [21]. In contrast with this principle of individuality, most randomized controlled studies that utilized MRAs for OSAS have reported a fixed and predetermined advancement for the mandible [22–26]. This may have been the reason why some studies demonstrated unsatisfactory results. In the present study, we chose the maximum mandibular advancement tolerated individually by each patient, which ranged from 8 to 11 mm in most patients [15].
Intra-oral appliances have good acceptance among patients, which is not the case with devices that apply PAP [18, 27–30]. The compliance to treatment using positive pressure varies greatly, and despite the documented efficacy of continuous positive airway pressure (CPAP), it has been estimated that more than 50% of the patients who start treatment with CPAP will not be using it 1 year later [18].
Studies have shown that the mean compliance to CPAP may vary from 3.4 to 4.7 h per night [6, 31, 5], whereas the compliance to tMRAs is around 6.8 h per night [18]. Thus, most patients with OSAS who are treated with CPAP spend 2 to 3 h per night without any treatment: a period of time that might have received treatment if another method had been used [3].
Although the real compliance to treatment with CPAP is not as good as expected, even this suboptimal treatment improves sleep structure and reduces O2 desaturation. On the other hand, it does not improve blood pressure, and this emphasizes the importance of ideal treatment that reduces cardiovascular sequelae [3, 7].
Why then is positive pressure therapy so popular and intra-oral appliances are not? The main reason is the high therapeutic efficacy associated with positive pressure. The AHI can be normalized in almost all patients after one night of titration using CPAP. This efficacy is undoubtedly necessary, but unfortunately, it cannot be confounded with efficiency. Nonetheless, the high efficacy of positive pressure is a message that is so strong that physicians almost forget about the other side of the treatment process: the patient. The patient behind the CPAP mask reacts to the side effects of this therapy and faces problems within his social environment and relationships through using CPAP, yet often hardly presents any perceptible signs and symptoms that could justify its daily use. Despite being made aware of the morbidity, mortality, and risk factors associated with OSAS, in most cases, patients cannot be convinced to adhere completely to treatment with CPAP.
Another strong reason for the popularity of CPAP is the economic question surrounding this technology. Companies strive to promote the best solution for each problem or complication, with the objective of bringing greater comfort in using a device that is hard to tolerate on a day-to-day basis. This continual effort towards improving the equipment promotes an image of care and concern for each patient’s health. Although this is true, such efforts cannot fail to constitute a strong advertising message that dazzles patients and suggests that they have no option other than positive pressure therapy. Moreover, the message suggests that certain difficulties can be attenuated through desensitization, more adequate masks, accessories for the positive pressure device, and cognitive approaches, among other measures. Economic interests and the low involvement of many physicians who feel that their work ends with the prescription account for this incredible diffusion of CPAP treatment. Nonetheless, this treatment only really works for patients with significant diurnal symptoms such as somnolence, and is ineffective for asymptomatic patients (the majority), who are recognized to be at greater cardiovascular risk because of the respiratory disturbance to sleep that they present [1–3, 7].
Efficiency (E) is not a concept that is widely understood. It is often confounded with and taken to be the same as efficacy (I). The efficiency of a type of treatment also takes into account the precision of the diagnosis (D) for the disease undergoing treatment, the compliance (C), and the access to treatment (A). Efficiency can therefore be calculated according to the following equation: E = I × D × C × A.
The efficiency associated with treatment using PAP, and particularly CPAP, would be (without considering access): E = 100% × 100% × 25% = 25%, where I = 100%, D = 100%, and C = 25%.
The efficiency for tMRAs, taking the mean adherence to be 80% [32, 33] and the efficacy of 64% from the present study, would be (again, without considering access): E = 64% × 100% × 80% = 51%, where I = 64%, D = 100%, and C = 80%.
The access factor was not taken into consideration in these calculations because it is very variable and depends on the socioeconomic development of different countries.
Surprisingly, the efficiency of intra-oral appliances is twice the efficiency of CPAP treatment. However, intra-oral appliances are not publicized among physicians. The principal consequence of this is that many patients are not receiving adequate treatment and continue to be exposed to the risks of OSAS and disease progression. Patients with low AHI, few diurnal symptoms, and healthy teeth and temporomandibular joints would fare better with intra-oral appliances. On the other hand, patients with severe apnea, excessive diurnal somnolence, and no claustrophobia or other significant symptoms relating to pressure, flows, and masks would fare better with positive pressure therapy.
In conclusion, titratable intra-oral appliances are efficacious and potentially effective for treating OSAS. They need to be more widely publicized among physicians involved in diagnosing and treating OSAS, and we suggest that well-designed studies for analyzing the efficiency of tMRAs should be conducted within future research.
References
Peppard PE, Young T, Palta M, Skatrud J (2000) Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 342(19):1378–1384
Hoffstein V, Rubinstein I, Mateka S, Slutsky AS (1988) Determinants of blood pressure in snorers. Lancet 29:992–994
Becker HF, Jerrentrup A, Ploch T et al (2003) Effect of nasal continuous positive airway treatment on blood pressure in patients with obstructive sleep apnea. Circulation 107:68–73
The report of an American Academy of Sleep Medicine Task Force (1999) Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. Sleep 22:667–689
Stepnowsky CJ, Marler MR, Ancoli-Israel S (2002) Determinants of nasal CPAP compliance. Sleep Med 3:239–247
Kribbs NB, Pack AI, Kline LR et al (1993) Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis 147(4):887–895
Yaggi HK, Concato J, Kernan WN et al (2005) Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 353(19):2034–2041
Mayer G, Meier-Ewert K (1995) Cephalometric predictors for orthopaedic mandibular advancement in obstructive sleep apnoea. Eur J Orthod 17:35–43
Ivanhoe JR, Attanasio R (2001) Sleep disorders and oral devices. Dent Clin North Am 45(4):733–758
De Almeida FR, Lowe AA, Otsuka R et al (2006) Long-term sequelae of oral appliance therapy in obstructive sleep apnea patients. Part 2: study model analysis. Am J Orthod Dentofac Orthop 129(2):205–213
Kato J, Isono S, Tanaka A et al (2000) Dose-dependent effects of mandibular advancement on pharyngeal mechanics and nocturnal oxygenation in patients with sleep-disordered breathing. Chest 117(4):1065–1072
Ferguson KA, Lowe AA (2005) Oral appliances for sleep-disordered breathing. In: Kryger MH, Roth T, Dement WC (eds) Principles and practice of sleep medicine, 4th edn. Elsevier Saunders, Philadelphia, USA, pp 1098–1108
Ng AT, Gotsopoulos H, Qian J, Cistulli PA (2003) Effect of oral appliance therapy on upper airway collapsibility in OSA. Am J Respir Crit Care Med 168:238–241
Engleman HM, McDonald JP, Graham D (2002) Randomized crossover trial of two treatments for sleep apnea/hypopnea syndrome: continuous positive airway pressure and mandibular repositioning splint. Am J Respir Crit Care Med 166:855–859
Gotsopoulos H, Chen C, Qian J, Cistulli PA (2002) Oral appliance therapy improves symptoms in OSAS: a randomized, controlled trial. Am J Respir Crit Care Med 166:743–748
Rechtschaffen A, Kales A (1968) A manual of standardized terminology, techniques and scoring system for sleep stages of human subjects. NIH Publication 204. US Government printing office, Department of Health Education welfare, Washington
Machado MA, Carvalho LB, Juliano ML et al (2006) Clinical co-morbidities in obstructive sleep apnea syndrome treated with mandibular repositioning appliance. Respir Med 100(6):988–995 (Jun)
Lowe AA, Sjoholm TT, Ryan CF et al (2000) Treatment, airway and compliance effects of a titratable oral appliance. Sleep 23:172–178
Machado MAC, Carvalho LBC, Francisco S et al (2004) Quality of life of patients with obstructive sleep apnea syndrome treated with an intraoral mandibular repositioner. Arq Neuro-Psiquiatr 62:222–225
Neter J, Kutner MH, Nashtsheim CJ, Wasserman W (1996) Applied linear statistical models, 4th edn. McGraw-Hill, Boston, pp 1408
Barnes M, McEvoy RD, Banks S et al (2004) Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit Care Med 170:656–664
Ferguson KA, Ono T, Lowe AA (1996) A randomized crossover study of an oral appliance vs CPAP in the treatment to mild–moderate OSAS. Chest 109:1269–1275
Ferguson KA, Ono T, Lowe AA et al (1997) A short-term controlled trial of an adjustable oral appliance for the treatment of mild to moderate obstructive sleep apnea. Thorax 52:362–368
O’Sullivan RA, Hillman DR, Mateljan R et al (1995) Mandibular advancement splint: an appliance to treat snoring and obstructive sleep apnea. Am J Respir Crit Care Med 151:194–198
Clark GT, Blumenfeld I, Yoffe N et al (1996) A crossover study comparing the efficacy of CPAP with anterior mandibular positioning devices on patients with OSA. Chest 109:1477–1483
Randerath WJ, Heise M, Hinz R, Ruehle KH (2002) An individually adjustable oral appliance vs CPAP in mild-to-moderate OSAS. Chest 122:569–575
Engleman HM, Kingshott RN, Wraith PK et al (1999) Randomized placebo-controlled crossover trial of continuous positive airway pressure for mild sleep apnea hypopnea syndrome. Am J Respir Crit Care Med 159:461–467
Pancer J, Al-Faifi S, Al-Faifi M, Hoffstein V (1999) Evaluation of variable mandibular advancement appliance for treatment of snoring and sleep apnea. Chest 116(6):1511–1518
Walker-Engstrom ML, Tegelberg A, Wilhelmsson B, Ringqvist I (2002) 4-year follow-up of treatment with dental appliance or uvulopalatopharyngoplasty in patients with obstructive sleep apnea. Chest 121(3):739–746
Marklund M, Sahlin C, Stenlund H et al (2001) Mandibular advancement device in patients with OSAS: long term effects on apnea and sleep. Chest 120:162–169
Reeves-Hoche MK, Meck R, Zwillich CW (1994) Nasal CPAP: an objective evaluation of patient compliance. Am J Respir Crit Care Med 149(1):149–154
Fransson AM, Tegelberg A, Leissner L et al (2003) Effects of a mandibular protruding device on the sleep of patients with obstructive sleep apnea and snoring problems: a 2-year follow-up. Sleep Breath 7(3):131–141
Marklund M, Stenlund H, Franklin KA (2004) Mandibular advancement devices in 630 men and women with obstructive sleep apnea and snoring: tolerability and predictors of treatment success. Chest 125(4):1270–1278
Acknowledgment
We would like to thank Mr. David George Elliff for the English translation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Machado, M.A.C., Juliano, L., Taga, M. et al. Titratable mandibular repositioner appliances for obstructive sleep apnea syndrome: are they an option?. Sleep Breath 11, 225–231 (2007). https://doi.org/10.1007/s11325-007-0109-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-007-0109-y