
Abstract
Introduction
Improvement in esophageal cancer staging is needed. Positron emission tomography (PET), computed tomography (CT), and endoscopic ultrasound (EUS) in the staging of esophageal carcinoma were compared.
Methods
PET, CT, and EUS were performed and interpreted prospectively in 75 patients with newly diagnosed esophageal cancer. Either tissue confirmation or fine needle aspiration (FNA) was used as the gold standard of disease. Sensitivity and specificity for tumor, nodal, and metastatic (TNM) disease for each test were determined. TNM categorizations from each test were used to assign patients to subgroups corresponding to the three treatment plans that patients could theoretically receive, and these were then compared.
Results
Local tumor staging (T) was done correctly by CT and PET in 42% and by EUS in 71% of patients (P value > 0.14). The sensitivity and specificity for nodal involvement (N) by modality were 84% and 67% for CT, 86% and 67% for EUS, and 82% and 60% for PET (P value > 0.38). The sensitivity and specificity for distant metastasis were 81% and 82% for CT, 73% and 86% for EUS, and 81% and 91% for PET (P value > 0.25). Treatment assignment was done correctly by CT in 65%, by EUS in 75%, and by PET in 70% of patients (P value > 0.34).
Conclusions
EUS had superior T staging ability over PET and CT in our study group. The tests showed similar performance in nodal staging and there was a trend toward improved distant disease staging with CT or PET over EUS. Assignment to treatment groups in relation to TNM staging tended to be better by EUS. Each test contributed unique patient staging information on an individual basis.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction, Background, and Significance
Despite the advances in surgical treatment and the improvements in perioperative care for esophageal cancer, the long-term prognosis of this disease remains poor. The overall survival rate is 10% or less at five years unless aggressive management is undertaken [1]. Commonly, patients present in advanced stage at the time of diagnosis with multiple lymphatic sites of involvement. Accurate staging of esophageal cancer is important because survival, optimal management, and degree of responsiveness to chemoradiation closely correlates with tumor, nodal, and metastatic (TNM) stage [1]. Stage-dependent treatment protocols require the most complete and accurate staging possible. Although treatment options continue to change, some standard treatment protocols entail curative treatment of esophageal carcinoma with surgical intervention either directly (stages I and IIA) or indirectly after chemoradiation (stages IIB and III). Surgical resection for esophageal carcinoma may include a three-field lymphadenectomy (cervical, thoracic, and abdominal). Patients with distant metastases do not benefit from surgical resection. Therefore the optimal staging modality for esophageal cancer would be the one that could best categorize patients into one of three treatment groups: surgery alone, chemoradiation followed by surgery, or chemoradiation alone. Furthermore, accurate staging is needed for proper planning of a surgical approach (limited versus extensive) or to determine the appropriate field of radiation for those who undergo chemoradiation.
Computed tomography (CT) scanning is commonly used for detection of distant and nodal metastases, and endoscopic ultrasound (EUS) for assessment of locoregional disease if there is no evidence of metastatic disease [2]. Good arguments have been made for including 2-deoxy-2-[F-18]fluoro-d-glucose (FDG)-positron emission tomography (PET) in initial staging as well. After having computed tomography (CT) and EUS staging, there are still quite a few patients with undiscovered distant metastases who undergo surgical intervention that is unlikely to result in cure [3]. Therefore, continued improvement of staging methods for esophageal carcinoma is important.
Some feel the accuracy of PET in the nodal staging of adenocarcinoma of the esophagus and the esophagogastric junction is limited because of low accuracy in staging of peritumoral and distant lymph nodes [4]. FDG-PET is unable to detect microscopic disease, and some involved lymph nodes adjacent to a hypermetabolic tumor mass have gone undetected. However, more accurate identification of distant nonnodal disease has made PET contribution significant [4]. In a recent metaanalysis done by Westreenen et al. [5], FDG-PET showed moderate sensitivity and specificity for the detection of locoregional metastases, and reasonable sensitivity and specificity in detection of distant lymphatic and hematogenous metastases. In the past, access to PET has also been fairly limited. Today, most large health care centers offer PET and even most rural health U.S. care systems have access to PET through widely disseminated mobile PET scanners [6]. This makes the importance of understanding PET in relationship to other imaging modalities an important issue. In this study, we assessed the comparative accuracy of esophageal cancer staging by CT, EUS, and PET, and also assessed the respective treatment implications.
Methods
Patients
Patients had to have newly diagnosed esophageal cancer and be over 18 years of age to be enrolled in the study. Patients who were diabetic, breast feeding, had an active infection, had renal failure, or had a prior history of another malignancy within five years were excluded. No referred patients were excluded based on these criteria.
Seventy-five patients were entered and assessed prospectively from November 2000 to July 2002 after signing consent forms. Patients were referred with the diagnosis of esophageal cancer after endoscopic biopsy. Six patients were excluded from the study due to the final surgical pathologic diagnosis of other primaries: gastric carcinoma (4), head and neck cancers (1), and nonsmall cell lung cancer (1). All patients underwent PET and CT within one month prior to EUS. All patients were followed up via their medical record for at least two years after initial staging. The study was approved by the Mayo Foundation institutional review board. Minorities were included.
PET Imaging
FDG-PET imaging was performed on a GE Advance PET Tomograph (General Electric Medical Systems, Inc., Milwaukee, WI, USA). FDG was performed on-site and was tested for sterility, pyrogenicity, and radiochemical purity on each production run. PET emission images of the body to include the neck, chest, abdomen, and pelvis were obtained 60 minutes after intravenous injection of 555–740 MBq of FDG.
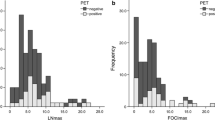
Emission images were reconstructed using iterative reconstruction. Attenuation correction was performed on all studies. Standard image corrections were made. Image pixel size was 4.25 mm and was displayed in a 128 × 128 array. Standard tomographic views as well as maximum intensity projections were reviewed on a computer for scan interpretation. Two readers visually interpreted the PET data, recording their interpretations on a standard data form, blinded to the results of all other imaging tests and if there were any inconsistencies, a consensus interpretation was made. As the lack of anatomic information on PET limited the reader’s ability to assess T stage in the standard fashion, size and intensity of the esophageal tumor were used as surrogate methods of classification of T stage. The following arbitrary criteria were employed: T1, uptake that was minimally to moderately above background, <1 cm; T2, moderate to intense, 1–2 cm in size; T3, intense uptake, 2–4 cm; T4, intense and greater than 4 cm or clearly in adjacent structures. Nodal uptake greater than background activity was considered positive. TNM disease was classified as demonstrated in Table 6.
CT Imaging
CT imaging was performed on subjects in supine position via a General Electric Light Speed Plus, CTI or High-Speed CT Scanner (General Electric Medical Systems). After obtaining a supine scout, the patient was given 60 mL of a pudding-consistency positive oral contrast agent (Esopho-Cat; 3.0% w/w; E-A-EM, Inc., Westbury, NJ, USA). A chest and abdomen CT was then obtained after an infusion of 150 mL nonionic contrast (Omnipaque, 300 mgI/mL; Amersham Health Inc., Princeton, NJ, USA). The CT protocol did not vary depending on the location of the known esophageal tumor. A 5-mm-thick slice was used. Exams were interpreted by using an off-line computer workstation, GE Advantage Windows (General Electric Medical Systems). Both readers, blind to the results of all other imaging tests, staged the known esophageal neoplasms, as described previously, and recorded their interpretations on a standard data form. For outside CT exams thought to be of adequate quality, readers (also blinded to the results of all other imaging tests) interpreted hard copy images on a light box, again completing the standard data form. TNM disease was classified as demonstrated in Table 6.
EUS Imaging
EUS examination was performed as per standard protocol for all patients with esophageal cancer at the Mayo Clinic (Rochester, MN). Initially, a forward-viewing endoscope was inserted to examine the esophagus, stomach, and duodenum to determine the proximal and distal extent of the tumor, obtain biopsies if not previously taken, and for dilatation if required to pass the echoendoscope. All patients obtained dilation of structure and allowed pass of echoendoscope except for six patients. These patients had incomplete EUS exam due to stenosis. Patients then underwent radial EUS examination (Olympus GF-UM30; Olympus America Corporation Inc., Melville, NY, USA) to assess the depth of primary tumor invasion (T stage), to detect malignant-appearing perigastric and mediastinal lymph nodes (N stage), and to search for celiac nodes or hepatic metastasis (M stage). The radial echoendoscope was advanced to the pylorus and slowly withdrawn while continuously imaging at 7.5 and 12 MHz. Minimal balloon inflation was used to limit tumor compression, which can reduce the accuracy of T staging. Whenever a nonperitumoral lymph node or hepatic lesion was detected, linear EUS (GF-UC30P; Olympus)-guided fine needle aspiration (8 cm long, 22-ga. needle with stylet, Echotip; Wilson-Cook, Winston–Salem, NC, USA) was performed to collect biopsy specimens for cytologic analysis. The radial and linear EUS exams and FNA were performed using standard techniques as previously described [7, 8]. After finishing TNM staging and sampling of visualized nodes, the EUS operator opened the sealed envelope to see if PET and CT had diagnosed any additional nodes or metastatic foci that could be assessed. If so, the operator sampled these areas thus allowing histopathologic evaluation of all detected nodes in all modalities. EUS scans were independently interpreted by two experienced physicians by using a video view station. Table 6 demonstrates TNM criteria used by EUS for staging. EUS staging was performed prior to FNA sampling. FNA of lymph nodes was done if accessible nodes were suspicious on EUS or reported on PET and CT after opening of envelope.
Disease Confirmation
PET and CT data were given to the EUS operator in a sealed envelope to be opened during EUS procedure after EUS diagnostic staging and FNA sampling was performed. After the EUS diagnosis was complete, the sealed envelope was opened in the EUS suite and the PET and CT data was reviewed and used to perform any additional biopsies of abnormalities on the PET or CT that may have not been sampled. This allowed the sampling of all suspicious nodes and metastases that were not detected with EUS. In three cases biopsy was performed as an independent procedure. Histopathologic data gained from FNA (55) or direct surgical procedures (14 patients) were used as gold standards (Table 1).
Data Analysis
CT and PET were interpreted by two experts in the respective fields and a TNM staging classification was determined for all included patients. Due to the real-time nature of EUS exam, only one expert gave final staging opinion. A TNM staging form was filled out that described the complete definitions of each TNM criteria for each location of esophageal cancer. Details of the tumor, specific site of nodal metastasis, and location of any distant metastasis were all recorded and sent to a central database for evaluation.
Discrepancies in staging were resolved using a consensus interpretation by the two experts. Sensitivity and specificity of each test for nodal and metastatic involvement was determined. The sensitivity and specificity data for nodal and metastatic disease were determined based on TNM staging criteria attained via either surgical pathology or FNA. Table 1 demonstrates the significance of detecting regional and nonregional lymph nodes for staging of esophageal cancer. Metastases to lymph nodes are considered N1 or M1 according to the origin of the tumor and site of the metastases (for example, celiac lymph nodes are M1 for thoracic cancer). The site of involvement is important rather than the number of nodes involved.
M stage was categorized as either M0 or M1, where M1a (distant nodal disease) and M1b (distant organ involvement) were considered equivalent for purposes of analysis. T staging was compared to surgical resection findings. The inability of FDG-PET to assess T stage accurately has been widely acknowledged in prior literature. T stage based on FDG-PET findings is of interest, but the validity of these criteria is unknown. T criteria were validated against pathologic assessments of T stage for those 14 patients who underwent surgical removal. This applies to only 14 patients (as is shown in Table 3). The reference standard for T staging in other patients who underwent neoadjuvant chemotherapy was not assessed.
To determine if the staging made by different imaging modalities could have changed final management, TNM staging results were classified into three groups that were concordant with the current treatment options that are used in our institution. Group A patients (Stage I, TII N0) receive surgical resection, group B patients (TIII N0 and NI M0) receive chemoradiation followed by surgery, and group C (M I) receive palliative chemoradiation (Table 2). Imaging modalities were compared using this treatment scheme to determine whether there were differences in how the tests would categorize patients into treatment groups based on the initial staging data. For patients who were eligible for surgery based on initial EUS and CT results, surgical pathology was used as the gold standard. Other patients had FNA as the pathologic standard. These were mostly performed by the EUS operator as described in “EUS Imaging.” The gold standard characterization for each of treatment groups is characterized in Table 1.
Statistical analysis
MC Nemar test was used for statistical comparison of each modality with another one. T, N, M, and final treatment were compared separately between two modalities. P value and confidence intervals were provided. We used the significance level of 0.05, and to obtain a power of 80% to detect 10% difference between imaging modalities, 75 patients were recruited for the study.
Results
Pathologic diagnoses were adenocarcinoma in 62 patients (90%) and squamous cell carcinoma in seven patients (10%). Fourteen patients (20%) were eligible for surgery alone (group A). Twenty-nine patients (42%) received neoadjuvant chemoradiation (group B). Twenty-six (38%) patients received palliative treatment (group C). At the end of follow-up of the study (June 2004) 13 patients were alive. Fifty patients were dead and six patients were lost to follow-up. There were five inconsistencies in TNM staging between two CT readers and three inconsistencies between PET readers that were resolved. Correct T staging was performed by EUS in 71% and by CT and PET in 43% (Table 3). Sensitivity for detecting nodal involvement was 86% in EUS, 84% in CT, and 82% in PET. Specificity for detecting nodal involvement was 67% in CT and EUS and 60% in PET (Table 4). Sensitivity and specificity rates for detecting distant metastasis were 81% and 82% for CT, 73% and 86% for EUS, and 81% and 91% for PET (Table 5). Treatment assignment using staging criteria from the tests was done correctly by CT in 65%, by EUS in 75%, and by PET in 70% of patients (Table 6). None of the P values for comparisons made for T, N, M, and correct treatment assignment between CT, PET, and EUS were less than 0.05. The range was between 0.14 and 0.5.
Metastatic Disease
Similar results for detection of distant metastatic disease by CT, EUS, and PET was observed. Some of the differences are as follows. For five patients who had distant metastasis missed by CT, one patient had distant disease seen on PET only, two had disease seen on EUS only, and two had disease seen by PET and EUS. In seven patients who had distant disease missed by EUS, two patients had disease seen by PET only and five had disease seen by PET and CT (Fig. 1). In five patients with metastasis missed by PET, two had disease seen by EUS only and three had disease seen by EUS and CT. In three patients with M1a disease on EUS that was not consistently seen by PET or CT, PET missed one case, CT missed one case, and both missed the other case. There were six patients who where M1a, with malignant celiac lymph nodes on EUS but had M1b disease on PET and CT. In three patients who had M1b disease on EUS that was not consistently seen by PET or CT, PET missed one case, CT missed one case, and both missed one case. Correct overall staging in assigning patients to each treatment group, A, B, or C was achieved by EUS in 75%, followed by PET in 70%, and then CT in 64%. . In some cases more extensive distant disease was seen on the different imaging modalities, which may or may not have any effect on patient care (Fig. 2).

CT of abdomen (a) showed low-attenuation lesions throughout the liver consistent with simple cysts (black arrows). EUS-described T3N1M0 disease. PET images (b) show esophageal cancer and a liver metastasis. Coronal PET image (right) and axial PET image (left image) show focal uptake in the liver (white arrow). This was a biopsy-proven liver metastasis.

(a) CT shows tumor in the esophagus (black arrow), celiac lymphadenopathy (white arrow), and an interoaortocaval node (M1b) (dashed arrow). (b) PET demonstrates esophageal uptake, positive nodes in the celiac axis, retroperitoneum (solid arrow), and paraacetabular region (dashed arrow) (M1b). EUS stage was T3N1M1a. Celiac node FNA was positive. The patient died two months later.
Discussion
We found that EUS, CT, and PET had similar sensitivities for nodal disease as well as distant metastatic disease. Other studies have described the low sensitivity of PET for local peritumoral nodal disease in the range of 22–63% as compared to our 82% [9, 10]. These differences may be explained by defining the methodologies used in these studies. Kneist et al. [10] reported a low PET sensitivity (33%) for local nodal disease. However, only patients with resectable disease by CT underwent PET. This introduced a selection bias because included patients with nodal disease would presumably have smaller lymph nodes involved, or they would have been identified by CT. Presumably, any small lymph nodes with metastatic disease could be more difficult to detect by PET and therefore PET would show a reduced sensitivity as compared to any nonselected group of esophageal cancer patients. Heeren et al. [11] used the same selection criteria as we did (included all patients) and reported a sensitivity of 55% for locoregional disease. In the study conducted by Rasanen et al., a sensitivity of only (37%) for PET detecting local nodal disease was noted and could be explained by the fact that half of the patients did not have PET attenuation correction which, is known to improve sensitivity [4]. In the study done by Vazquez et al. (in our institution), EUS FNA was more sensitive (83% vs. 29%; P < 0.001) than CT and more accurate than CT (87% vs. 51%; P < 0.001) or EUS (87% vs. 74%; P = 0.012) for nodal staging. Direct surgical resection was contraindicated in 77% of these patients due to advanced locoregional/metastatic disease, as likewise seen in our study group. The discrepancy between their data and ours may be due partly to different study inclusion and exclusion criteria. The Vazquez study excluded patients where larger tumors limited EUS distally. Perigastric and celiac lymphadenopathy could not be assessed in those severely stenotic tumors. In our study, these patients were included to represent the utility of the tests in the whole spectrum of disease.
Finally, in a recent metaanalysis done by Westreenen et al. [5], FDG-PET showed moderate sensitivity and specificity for the detection of locoregional metastases, and reasonable sensitivity and specificity in detection of distant lymphatic and hematogenous metastases.
The rigorous blinding of observers to the results of other imaging studies was a strength in our study that restricted potential biases. However, it was also a potential weakness—specifically with respect to interpretation of the PET studies. Before the advent of PET/CT, FDG-PET studies were rarely interpreted without reference to the conventional CT examinations that had typically been performed before PET. The ability of observers to discriminate a physiologic signal from a pathologic signal is greatly facilitated by reference to the anatomical images. Accordingly, the PET interpreters in our study were put at some disadvantage during their interpretations by comparison with the “standard of care” approach. A trial design that might have addressed this problem would have had the PET images first interpreted blindly and then reinterpreted with benefit of the diagnostic CT examinations.
We found that EUS had nearly comparable sensitivity and specificity with CT and PET for detecting metastatic disease. That is partly explained by the fact that EUS detected M1a lesions (nodal metastasis) and some adjacent hepatic metastasis well and probably also because our study was designed to sample all the visualized nodes in any imaging modality in hopes of obtaining a better definition of their accuracy in regions that may not otherwise be sampled.
Diagnostic specificity for local lymph node and distant metastasis was higher for PET when compared to CT or EUS in some previous studies (90–100%) [10]. In our study, the tests all had equivalent specificities for local nodal disease. The equal specificity for nodal disease in our study may stem from the fact that we rigorously sought biopsies of PET-positive findings given our protocol scheme. Perhaps some of the PET findings in other studies may have been unconfirmed by tissue diagnosis. A higher sampling rate for PET positive findings may more accurately reflect the specificity of PET (Fig. 3).

PET (upper image) shows esophageal primary (black arrow). No nodal involvement is identified. Probable left malignant lung nodule is demonstrated (white arrow). CT image (lower image) shows a nonspecific indeterminate nodule that may represent metastases (black arrow). Biopsy was negative. EUS showed a T1 lesion only. Surgical pathology stage was T1NOMO. Follow-up assessment showed the true nature of this pulmonary lesion to be a granuloma.
This study provided the opportunity to perform biopsies of lymph nodes that were positive on PET or CT imaging by EUS FNA, as soon as the diagnostic EUS was complete. Full lymph node dissection as a gold standard is less achievable in esophageal cancer patients because they are less likely to have limited locoregional disease amenable to direct surgical intervention. Certainly, the lack of complete nodal dissection in all of our patients is a weakness in our study. However, the unique opportunity to sample lymph nodes that may be out of a standard surgical field or not visualized on EUS was possible in our study because all the suspicious nodes seen on imaging were sampled.
Another advantage of our study was classifying the results into three groups representing theoretical treatment types patients would receive based on their clinical TNM stage. We hypothesized that if we categorized the patients as defined by treatment in our institution, we could assess the applicability of these imaging staging results in a more practical way. Although two staging results may differ slightly in the TNM criteria, they may lead patients to the same treatment grouping (esophagectomy, neoadjuvant therapy in addition to esophagectomy, or palliative chemotherapy alone) and are therefore equivalent in determining the direction of therapy. In contrast, if a modality missed a critical lymph node, treatment decision will change completely. For example, for a tumor originating in the distal third of the esophagus, cervical nodal involvement is considered metastatic disease (Table 1). Missing metastatic disease in such a lymph node would lead to the wrong therapy. Treatment assignment using staging criteria from the tests was done correctly by CT in 65%, by EUS in 75%, and by PET in 70% of patients. There were six patients that were correctly assigned treatment by PET but were underdiagnosed by CT. Even though the final treatment assignments were not statistically different, EUS had a trend toward better locoregional (T, N) staging that overwhelmed its slight disadvantage in detecting distant metastatic disease. The application of our data to our local treatment scheme certainly needs to be considered in light of different the therapeutic approaches that may be applied to esophageal cancer patients. Although this is a common treatment algorithm, it may not be true of all practices and therefore our data may not be generalizable to such practices in this respect.
The best approach from this data would appear to be consideration of the tests as complimentary, and we suggest the use of all of these staging tests to provide the highest likelihood of detecting disease with preference of EUS for detecting locoregional disease, and PET and CT for assessment of distant disease. PET is especially useful when there is suspicion of distant disease and CT for hepatic and intraabdominal nodal involvement.
Conclusion
PET, EUS, and CT showed similar performance in nodal staging. There was a trend toward improved locoregional assessment for EUS and better distant disease staging with CT or PET. However, each test contributed unique patient staging information on an individual patient basis.
References
Goldberg M, Farma J, Lampert C et al. (2003) Survival following intensive preoperative combined modality therapy with paclitaxel, cisplatin, 5-fluorouracil, and radiation in resectable esophageal carcinoma: A phase I report. J Thorac Cardiovasc Surg 126(4):1168–1173
Saltzman JR (2003) Section III: Endoscopic and other staging techniques. Semin Thorac Cardiovasc Surg 15(2):180–186
Lerut T, Coosemans W, Decker G et al. (2004) Extended surgery for cancer of the esophagus and gastroesophageal junction. J Surg Res 117(1):58–63
Rice TW (2000) Clinical staging of esophageal carcinoma. CT, EUS, and PET. Chest Surg Clin North Am 10(3):471–85
van Westreenen HL, Westerterp M, Bossuyt PM et al. (2004) Systematic review of the staging performance of 18F-fluorodeoxyglucose positron emission tomography in esophageal cancer. J Clin Oncol 22(18):3805–3812
Wallace MB, Nietert PJ, Earle C et al. (2002) An analysis of multiple staging management strategies for carcinoma of the esophagus: Computed tomography, endoscopic ultrasound, positron emission tomography, and thoracoscopy/laparoscopy. Ann Thorac Surg 74(4):1026–1032
Rosh T, (1994) Endoscopic ultrasonography. Endoscopy 26:148–168
Wiersema MJ, Giovannini VPM, Chang KJ, Wiersema LM (1997) Endosonography-guided fine-needle aspiration biopsy: Diagnostic accuracy and complication assessment. Gastroenterology 112:1087–1095
Lerut T, Flamen P, Ectors N et al. (2000) Histopathologic validation of lymph node staging with FDG-PET scan in cancer of the esophagus and gastroesophageal junction: A prospective study based on primary surgery with extensive lymphadenectomy. Ann Surg 232(6):743–752
Kneist W, Schreckenberger M, Bartenstein P, Grunwald F, Oberholzer K, Junginger T (2003) Positron emission tomography for staging esophageal cancer: does it lead to a different therapeutic approach? World J Surg 27(10):1105–1112
Heeren PA, Jager PL, Bongaerts F, van Dullemen H, Sluiter W, Plukker JT (2004) Detection of distant metastases in esophageal cancer with (18)F-FDG PET. J Nucl Med 45(6):980–987
Acknowledgements
We would like to thank Terry Brinkman for her administrative support of this project. This study was supported by Mayo Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lowe, V.J., Booya, F., Fletcher, J.G. et al. Comparison of Positron Emission Tomography, Computed Tomography, and Endoscopic Ultrasound in the Initial Staging of Patients with Esophageal Cancer. Mol Imaging Biol 7, 422–430 (2005). https://doi.org/10.1007/s11307-005-0017-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11307-005-0017-0