
Abstract
Purpose
Probiotics may reduce risk of urinary tract infection by preventing colonization of uropathogens. We aimed to determine the change in the ratio between uropathogens:Lactobacillus (U/L) within the lower urinary tract in response to oral probiotic.
Methods
This was a double-blinded randomized controlled trial of healthy pre-menopausal female volunteers. Participants provided daily voided urine for 3 months including three phases of the trial: 1—baseline, 2—intervention, 3—wash-out. Participants were randomized to an oral probiotic (Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14) versus placebo. The primary outcome was the U/L ratio of daily voided urine, as determined by an enhanced urine culture method. Analysis included t test of the ratios and separate generalized linear mixed effects models (GLMM) for microbiota diversity.
Results
481 samples of seven female participants with mean age 29.1 years (± 5.3 years) were included in the analysis (probiotic n = 4; placebo n = 3). No adverse events were reported. The placebo and probiotic groups had similar mean U/L ratios with no difference between placebo and probiotic groups in Phases 1–3 (p = 0.90, p = 0.58 and p = 0.72, respectively). The probiotic species were never identified in the voided urine. There were no changes between groups in terms of microbiota diversity.
Conclusion
For young healthy women, the use of oral probiotic did not affect the U/L ratio.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Urinary tract infection (UTI) is a common problem for the pre-menopausal female population. This problem is exacerbated by the rise in antimicrobial resistance of uropathogens that cause UTI, as well as the downstream side effects of antibiotic use on the microbiome [1]. Therefore, alternative treatments and prevention methods are greatly needed [2, 3].
Probiotics can be used to alter bacterial colonization. Probiotics are microbes, including species within the genus Lactobacillus, that provide benefits to neurological [4], gastrointestinal [5, 6], and immunological [7] health in humans [8]. Probiotics are usually taken orally but can be delivered using alternate routes, including vaginally. There are a few reports on the use of oral probiotics altering the vaginal microbiome [9] within as little as 1–2 weeks [10, 11]. The oral probiotic combination of L. rhamnosus and L. reuteri (former L. fermentum) was reported to alter the vaginal flora in women with bacterial vaginosis (BV) [10] and reduce vaginal coliforms and yeast within 4 weeks of oral probiotic use in asymptomatic pre-menopausal women [9]. Pre-menopausal women with UTI who were given a vaginal probiotic comprised of L. rhamnosus GR-1 and L. reuteri RC-14, along with antibiotic therapy, had decreased UTI recurrence from 47 to 21% [12]. In a similar study, weekly use of the L. rhamnosus GR-1/L. reuteri RC-14 probiotic reduced UTI recurrence from 6 to 1.6 per year [13]. A randomized controlled trial (RCT) of 252 postmenopausal women with recurrent UTI (rUTI) (7 UTIs in 12 months) tested the efficacy of the L. rhamnosus GR-1/L. reuteri RC-14 probiotic orally against daily prophylaxis with trimethoprim–sulfamethoxazole (480 mg once daily); patients who received antibiotics reported an average of 2.9 UTIs in 12 months, while the oral probiotic group averaged 3.3 UTIs, a result that did not meet the non-inferiority criteria [14]. However, an added benefit to taking the oral probiotic was a decreased level of antibiotic resistance [14].
Recent studies report the existence of resident microbial communities in the lower urinary tracts of adult women (female urinary microbiota, FUM) [15,16,17]. However, no RCTs have yet quantitatively evaluated the effect of oral probiotics on the FUM. Therefore, it is unclear whether the probiotic bacteria, when given orally, will colonize the adult female lower urinary tract and/or alter the existing FUM.
Here, we describe a pilot, double-blinded RCT of healthy pre-menopausal community women. The participants collected midstream voided urine specimens and peri-urethral swabs daily for 3 months, during which they were randomized in a 2:1 ratio to take an oral probiotic or placebo during the second month of the trial. We detected and identified microbes using our previously validated expanded quantitative urine culture (EQUC) method [18]. We hypothesized that use of oral probiotics would alter the FUM, by lowering the abundance of detectable uropathogens while increasing Lactobacillus levels.
Materials and methods
Study design
This was a single-site, IRB-approved (LU #209830), randomized, double-blind, placebo-controlled pilot trial conducted between the Loyola University Chicago Health Sciences Division and The Loyola University of Chicago’s Division of Female Pelvic Medicine and Reconstructive Surgery. We obtained an exemption from the US Food and Drug Administration’s investigational new drug regulations (i.e., investigational new drug exemption; approval #136454) to use the oral probiotic in this clinical trial. The trial was registered with clinicaltrials.gov (NCT03250208).
We recruited healthy pre-menopausal female volunteer participants from the community by flyers that were placed throughout the medical center campus, offering a brief description of the study and the research team contact information. Eligible participants met the following criteria: pre-menopausal (presence of menses at least once in the last 12 months) healthy community dwelling; age 18 years or older; agreement to daily specimen collections; agreement to daily oral probiotic or placebo use; ability to read and speak the English language. Participants were excluded if they met any of the following exclusion criteria: male; non-English speaking; allergy or contraindication to probiotic; pregnant, lactating or planning a pregnancy within 6 months; use of an indwelling catheter; planning time away for more than 7 days during the study; prior participation in the study; failure to pass the 3-day screening process (i.e., ability to obtain a ‘clean catch’ midstream voided urine). Participants were compensated for completion of the study. Completion was defined as missing no more than seven specimen collection days during the length of the study.
The study was divided into three phases: Phase 1 (days 1–20, “Baseline” phase), Phase 2 (days 21–60, “Treatment” phase), and Phase 3 (days 61–95, “wash-out” phase). Specimens were provided each day through day 74. From days 75–95, specimens were collected once per week. From days 21–95, an additional rectovaginal swab (per CDC guidelines [19]) was collected once per week. Eligible participants were instructed on proper specimen collection by watching a video at the recruitment visit.
Prior to study enrollment and following informed consent, we assessed each subject’s ability to provide the researchers with a ‘clean catch’ midstream voided urine specimen via a 3-day screening period. We anticipated that the bacterial flora of a properly collected ‘clean catch’ midstream voided urine specimen would appear distinct from the flora of the peri-urethral swab. Micobiota data were assessed using Bray–Curtis dissimilarity. We enrolled participants who provided specimens that obtained a score of > 0.8 (i.e., substantially dissimilar).
Participants completed a non-validated lifestyle questionnaire for each day of the study. This questionnaire included the following: alcohol consumption, menstruation (and hygiene article use), bathing and swimming, diet (presented as broad food categories), sexual activity, number of bowel movements, medications used, illness, and whether the participant urinated or had a bowel movement immediately before collection of the day’s specimens.
Probiotic
Participants were randomized in a 2:1 ratio to a probiotic versus placebo group by a statistician, who was otherwise uninvolved in the project. The probiotic used contained Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 at sum of 109 viable organisms to be taken orally twice daily. The probiotic capsules were purchased from www.iherb.com, and were sent directly to the in-patient pharmacy department. The capsules were stored at room temperature as per the manufacturer’s recommendations. The randomization scheme was chosen with the goal of having more subjects in the probiotic arm to maximize statistical power. The randomization scheme was by random permutated block, which would be balanced at the 2:1 ratio after completion of each block with block size = 3. The random allocation sequence was created by sequentially numbered containers.
Subjects and all study personnel were blinded to the group assignment, except for the statistician and pharmacist. The statistician gave the randomization scheme only to the one pharmacist, who prepared the capsules for the study. The probiotics were re-capsulated into capsules that were identical to the carbohydrate placebo capsules. Labels of the pill bottles included the subject name, date, and “placebo/probiotic.” To evaluate the success of blinding, the subjects were asked at the completion of the study to which group they thought they belonged.
The oral probiotic or placebo capsules were taken during phase 2 (days 21–60) only. To avoid errors in compliance reporting, the participants were told that perfect use was not expected and would not change their compensation.
Sample collection and bacterial identification
Each participant was given sufficient supplies for at-home specimen collection. ‘Clean catch’ midstream voided urine specimens were collected and placed in a BD Vacutainer® Plus C&S Preservative Tube (Becton, Dickenson and Co, Franklin Lakes, NJ). Peri-urethral swabs were collected using an ESwab Liquid Amies Collection and Transport System (COPAN, Murrieta, CA). These specimens were delivered to a locked collection box at the Loyola University Medical Center Urogynecology Clinic. Specimens collected during a weekend were kept at room temperature and delivered on the following Monday.
The microbiota of the collected biological specimens was determined using our EQUC protocol, as described previously [16]. Briefly, 10 ul of each urine specimen was spread quantitatively onto 5% sheep blood (BAP), chocolate, and colistin nalidixic acid (CNA) agars (BD BBL™ Prepared Plated Media) and incubated in 5% CO2 at 35 °C for 48 h; BAP incubated aerobically at 35 °C for 48 h; CDC Anaerobic 5% sheep blood (Anaerobic BAP) agar (BD BBL™ Prepared Plated Media) incubated anaerobically at 35 °C for 48 h. Each distinct colony morphology was sub-cultured at 48 h to obtain pure culture for microbial identification. Microbial identification was determined using a matrix-assisted laser desorption/ionization time-of-flight mass spectrometer (MALDI-TOF MS, Bruker Daltonics, Billerica, MA). Swab specimens were diluted in the Liquid Amies solution. 10 ul of the liquid solution was subjected to the protocol described above.
Dipstick urinalysis also was performed on each urine specimen using a Siemens Multistix® 10LS Pro Reagent Strip (Siemens Healthcare, Tarrytown, NY). Two milliliters of urine and the remaining liquid solution from the swab specimens were stored at − 80 °C for future analyses.
Sample size
This was a pilot RCT, as the outcome variable and variability were unknown; therefore, it did not have a power calculation. However, this sample was chosen based on our prior preliminary data from two graduate students (male and female) who self-collected and cultured their samples. These data will remain unpublished; however, they allowed the authors to gauge the daily fluctuations of the voided urine in young healthy women and design the screening phase of the study.
Statistical analyses
Student’s t test was performed to evaluate the association between microbial ratios and probiotic or placebo use. Chi-squared testing was used to compare categorical variables. One-way analysis of variance (ANOVA) was used to compare continuous variables. Correlations between variables were determined using the Pearson correlation test. Separate generalized linear mixed effects models (GLMM) were specified for microbiota outcome variables, including Shannon index, Simpson index, and percentage of Lactobacillus. Shannon and Simpson indices were used as the primary measures of microbiota alpha diversity. The primary effects of interest in GLMMs were treatment assignment, phase of study, and an interaction term. Models were adjusted for daily sexual activity and menstruation and included random intercepts for participants. Adjusted means and standard errors from GLMMs were plotted and significance test was reported using a Kenward–Roger degrees of freedom approximation due to sample size. All test results were considered significant using a p value of ≤ 0.05. All analyses were conducted using SAS 9.4 (Cary, NC).
Primary outcome and the designated uropathogens
The primary outcome was by a ratio of the concentrations of uropathogens to lactobacillus (U/L ratio). Uropathogens were defined in prior studies [18] and included all of the following: Actinobaculum schaalii (former Actinotignum schaalii), Aerococcus sp., Alloscardovia omnicolens, Candida sp., Citrobacter sp. Corynebacterium riegelii, Corynebacterium urealyticum, Enterobacter sp., Enterococcus faecalis, Escherichia coli, Klebsiella pneumoniae, Morganella morganii, Oligella urethralis, Proteus sp., Pseudomonas aeruginosa, Staphylococcus aureus, Staphylococcus lugdunensis, Streptococcus agalactiae, Streptococcus anginosus.
Description of measures of diversity
Bacterial compositions were analyzed for diversity in addition to the primary outcome measure of U/L ratio. Diversity includes measures of species abundance, richness and evenness. Species abundance is the number of each organism present relative to the total amount of organisms. Richness describes the number of different species in a community. Evenness describes the distribution of species within the sample; communities with higher evenness contain multiple species with similar abundance. Two measures are commonly combined and represented via the Shannon (richness and evenness) and Simpson (richness and abundance) indices. Larger Shannon diversity values, close to 1, mean greater richness and greater evenness. Larger Simpson diversity values indicate that the sample contains greater richness and abundance. For each measure, larger value indicates more diversity in the sample; however, they are composed of slightly different sub-measures and, therefore, each was considered to be complete.
Results
Study and participant overview
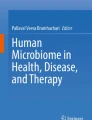
From July 2017 to December 2018, 12 participants were assessed for eligibility. Four participants did not meet the inclusion criteria and were, therefore, not enrolled in the study and did not perform any sample collections; one was outside the target age range and three were excluded because based on the 3-day screening period results they could not produce voided urine samples that were sufficiently distinct from their peri-urethral swabs. Thus, a total of eight participants were enrolled in the study and randomized. All participants completed the study and received full compensation. Due to resource and time constraints, one randomly chosen’s participant’s specimens were not cultured. This choice was made prior to unblinding the study and should have no effect on the outcomes of this study given that the participant was randomized to placebo. The samples of this participant were subjected to sequencing analysis only. Therefore, seven participants were included in the analysis here: four in the probiotic group and three in the placebo group. All participants completed the study within their assigned group and, therefore, there is no difference in analysis by intention to treat or by actual treatment. Figure 1 displays the consort diagram of patient flow through the study.

Consort diagram: this figure shows the number of participants invited to the study, as well as follow-up throughout the study course. After assessing eligibility with 12 women, 8 met inclusion criteria and were enrolled in the study and randomized. After completion of sample collection, one of these participants’ data were not included in the analysis because diversity was too high and bacterial counts were too large to complete the analysis
Baseline demographics were similar between groups (Table 1). The mean age of the participants’ was 29.1 years (± 5.2 years SD; median age was 28 years, with 25th and 75th percentiles at 25 years and 33 years, respectively). The participants had a mean BMI of 23.0 kg/m2 (± 2.8 kg/m2 SD). None of the participants had a prior history of gynecological surgery, kidney stones, recurrent UTI or symptoms of urinary incontinence. All of the participants were non-smokers, and all used alcohol occasionally.
The post-study survey was completed by all participants. All participants took the capsules almost every day during phase 2 (median pills missed = 4 out of 80 pills, range 0–20). When asked to which group they were randomized, the participants correctly guessed 3/8 (38%) times (two probiotic and one placebo). No adverse events or unexpected harms were reported.
Microbial characteristics
This was an intention-to-treat analysis. Table 2 shows the relative abundance of the most prevalent microbes for each participant throughout the study. The FUM of seven participants was predominated by at least one species of the genus Lactobacillus; in contrast, one participant’s (PROFUM 3) FUM lacked Lactobacillus and instead was predominated by a mixture of Streptococcus agalactiae (GBS), Staphylococcus epidermidis and Corynebacterium tuberculostearicum.
Prior to probiotic/placebo use (i.e., phase 1), no participants were colonized with the probiotic bacteria (i.e., L. rhamnosus and/or L. reuteri). Throughout the study (i.e., phases 2 and 3), these species remained undetected in any specimens (voided urines, peri-urethral swabs), while other Lactobacillus species (crispatus, jensenii, iners) flourished on the culture media used.
All participants also collected rectovaginal swabs at various times during the intervention phase and the wash-out phase. While these samples were cultured and the microbiota data results were recorded, they were not part of the primary outcome analysis here and will be presented at a later paper. However, it is important to report here that the probiotic species were also never detected on any of these rectovaginal specimens.
Uropathogenic bacteria and Lactobacillus
With one exception (PROFUM 3), uropathogens were rarely present when compared to the total colony counts throughout all three phases of the study. Table 3 shows the average daily percentage of Lactobacillus, total uropathogens, and Gardnerella per participant and per phase. Gardnerella was included because of its prevalence in some participants. The percentage of days that E. coli was detected is also included in Table 3, as this species was the most commonly detected uropathogen. Figure 2 shows the % Lactobacillus per phase for all the participants. Contrary to our hypothesis, we observed an increase in % Lactobacillus in the placebo group through the course of the study. Within each phase, there were no differences in between placebo and probiotic groups in phase 1 (baseline), phase 2 (treatment), and phase 3 (wash-out), with p values of p = 0.9, p = 0.58 and p = 0.72, respectively.

Percent Lactobacillus by group and phase. This figure shows all specimens collected per phase (“baseline” = phase 1, “treatment” = phase 2, “wash-out” = phase 3). The wide error bars of each phase show that the proportion of Lactobacillus varied greatly between specimens throughout the study. There was no trend toward increased proportion of Lactobacillus noted amount the probiotic assignment participants. p value for the group effect at each time point in a generalized linear mixed effects model adjusted for menstruation and sexual activity and including random intercepts for individuals. Control = placebo group
Figure 3 shows the daily U/L ratio for participants randomized to the probiotic group (i.e., PROFUM 1, 4, and 7). The fourth member of this group (PROFUM 3) did not have any Lactobacillus and thus could not be included. Figure 4 shows the mean U/L ratio values in graphical format. The U/L ratio was similar between the two groups all throughout the study (phase 2: p = 0.640, t test). There was significant fluctuation throughout the study as indicated by the standard deviation for each bar. Phase 2, the intervention phase, had the highest U/L ratio for both groups; however, this was not statistically significant. The change in the ratio from phase 1 to phase 2 was + 0.206 and + 0.33 for the placebo and probiotic groups, respectively.

Daily ratio of uropathogen to Lactobacillus per participants ProFUM 1, 4 and 7 who all had probiotic assignment. Days 21–60 are marked as the probiotic administered days (phase 2)

Uropathogen to Lactobacillus ratio per group per phase
To assess changes in microbiota diversity, we used the Simpson and Shannon indices, which measure alpha diversity. Figures 5 and 6 model these values for the duration of the study and consider confounding factors, including menstruation and sexual activity. The Simpson’s index (Fig. 5) was remarkably similar between the placebo group and the probiotic group throughout the study. There was no difference between placebo and probiotic groups in phase 1 (“baseline”), phase 2 (“treatment”), and phase 3 (“wash-out”), with p values of p = 0.59, p = 0.88 and p = 0.47, respectively. The Shannon index (Fig. 6) also showed no change between the placebo and probiotic groups in phase 1 (“baseline”), phase 2 (“treatment”), and phase 3 (“wash-out”), with p values of p = 0.7, p = 0.75 and p = 0.8, respectively.

Simpson index by group and phase. p value for the group effect at each time point in a generalized linear mixed effects model adjusted for menstruation and sexual activity and including random intercepts for individuals. Control = placebo

Shannon index by group and phase. In a generalized linear mixed effects model, the Shannon diversity index showed wide error bars for each phase and did not differ between the groups (probiotic vs. placebo). p value for the group effect at each time point in a generalized linear mixed effects model adjusted for menstruation and sexual activity and including random intercepts for individuals. Control = placebo
Discussion
In this pilot study of pre-menopausal community women, the use of an oral probiotic containing L. rhamnosus GR-1 and L. reuteri RC-14 at a sum of 109 viable organisms did not show changes in the U/L ratio or alpha diversity of the lower urinary tract microbiota.
Although EQUC can grow both L. reuteri and L. rhamnosus, we did not detect these probiotic species before, during, or after use. Therefore, it is unlikely that the probiotic organisms had a direct effect on the lower urinary tract. In contrast, the probiotic organisms could have had an indirect effect, possibly by altering the gut microbiota, which we did not measure in this study. Intriguingly, a slight trend towards increased uropathogen presence was observed during probiotic use; however, given the small sample size, this finding may not be clinically relevant.
Strengths of the study include the participants’ high level of compliance with collection of daily biological specimens, completion of questionnaires, and consumption of probiotic/placebo capsules. In addition, the study was designed in a randomized and double-blinded fashion. As a result, the participants were successfully blinded, as evident by the post-study survey. Furthermore, our study utilized a robust culture-dependent method (i.e., EQUC) to analyze microbial composition and provided us with an in-depth analysis of the specimens. Despite the low participant sample size, the number of collection days far exceeds any other study in the literature, thus ruling out any biases in choosing particular collection days to study, and improving the strength of our conclusions. We standardized urine specimen collection for this study by performing a pre-study screening phase using peri-urethral swab similarity as a measure of compliance.
In contrast to our results, Reid et al. [9] concluded that probiotic use significantly reduced the prevalence of yeast and coliforms. This was a randomized double-blinded control study in which 64 women were assigned to either the same oral probiotic used in our study or a placebo. The primary outcome measure consisted of microscope analysis of vaginal swabs to determine their Nugent score; this was done on days 0, 7, 28, 60, and 90. The Nugent score classifies vaginal flora on a spectrum from 0 to 10 as containing high counts of Lactobacillus versus high counts of Gram-negative or Gram-variable rods (i.e., bacterial vaginosis). The results showed an increased restoration from bacterial vaginosis to a Lactobacillus-predominant microbiota (37% vs. 13% in the probiotic vs. placebo group, p = 0.02). They showed a significant reduction of yeast and coliforms in the probiotic group versus placebo group at 28 days and 60 days of the therapy.
The Reid et al. [9] study differed from ours in that their samples were analyzed via microscopy of vaginal swab samples instead of EQUC of urine samples. We believe our method of detection is more rigorous. Whereas Reid and co-workers observed bacteria that looked morphologically like Lactobacillus, we could identify individual isolates to species level with the EQUC method. Another difference is that our study analyzed urine rather than a vaginal swab. Therefore, it is possible that the probiotic never transferred from the GI tract into the urine. However, we also did not detect this species on any of the rectovaginal swabs. Additionally, a significant fraction of the women in the Reid et al. [9] study suffered from BV, while the majority of the subjects in our study were already Lactobacillus predominant. It is possible that the effect seen in the Reid et al. [9] study results from the probiotics helping women with BV rather than healthy patients. Finally, the statistical methods of Reid et al. [9] assume that the results of the day 7, 28, 60, and 90 swabs are independent of each other.
Another study that had comparable goals to ours was Beerepoot et al. [14] who performed a non-inferiority trial with randomized double-blinded control study design of postmenopausal women with rUTI to compare probiotic supplements and prophylactic antibiotics. The authors recruited 252 women who were assigned to prophylactic trimethoprim–sulfamethoxazole versus probiotic and the outcome measure was a survival analysis of the incidence of UTI over the course of 12 months. Both groups had a reduction of UTI; however, a larger decline was seen in the antibiotic group. Indeed, in comparing the antibiotic and probiotic arm, the probiotic did not meet non-inferiority margin. Additionally, the authors found similar rates of adverse events between the probiotic and antibiotic arm.
There are numerous differences between our study and the work of Beerepoot et al. [14] that makes comparing the studies difficult. Primarily, Beerepoot et al. [14] examined patients that were both older and had higher risk factor for UTI than the women in this study. As noted in the previous paragraph, this could suggest that probiotics have some beneficial effects for at-risk patient populations. For the variety of reasons presented here, we believe that there is insufficient information at this time to adequately compare the results of our study to that of Reid et al. [9] or Beerepoot et al. [14] and believe these intriguing differences merit further investigation to fully understand the effects of probiotic Lactobacillus on vaginal and urine flora.
Limitations of the study include the use of midstream voided urine instead of transurethral catheterized urine. This is a limitation because midstream voided urine samples both the bladder and urethra and the contribution of microbes from each niche is currently unclear. Though we view the use of the 3-day screening period as a benefit of this study, it may also be seen as a limitation. Participants whose microbes were similar between their midstream voided urine and peri-urethra were excluded because we could not be sure that they had properly collected specimens. However, it is unclear if some women normally present with microbial overlap in these sites. Thus, we may have sampled a subgroup of pre-menopausal community women. Nevertheless, this method provided a level of standardization. In future studies, providing a few catheterized urine specimens for comparison may resolve this issue.
Conclusion
The use of oral probiotic (L. rhamnosus GR-1 and L. reuteri RC-14) does not affect the U/L ratio or microbiota diversity within the lower urinary tract of a young pre-menopausal healthy female population. Future studies should use a similar longitudinal design, but focus on more clinically relevant patient groups who are at higher risk of UTI. Additionally, it may be necessary to consider vaginal probiotic administration.
References
Wilton L, Kollarova M, Heeley E, Shakir S (2003) Relative risk of vaginal candidiasis after use of antibiotics compared with antidepressants in women: postmarketing surveillance data in england. Drug Saf 26:589–597
Foxman B, Cronenwett AE, Spino C, Berger MB, Morgan DM (2015) Cranberry juice capsules and urinary tract infection after surgery: results of a randomized trial. Am J Obstet Gynecol 213:194.e1–194.e8
Beerepoot M, Geerlings S (2016) Non-antibiotic prophylaxis for urinary tract infections. Pathogens. https://doi.org/10.3390/pathogens5020036
Akbari E, Asemi Z, Daneshvar Kakhaki R, Bahmani F, Kouchaki E, Tamtaji OR, Hamidi GA, Salami M (2016) Effect of probiotic supplementation on cognitive function and metabolic status in alzheimer’s disease: a randomized, double-blind and controlled trial. Front Aging Neurosci 8:256
Heiser CR, Ernst JA, Barrett JT, French N, Schutz M, Dube MP (2004) Probiotics, soluble fiber, and l-glutamine (GLN) reduce nelfinavir (NFV)- or lopinavir/ritonavir (LPV/r)-related diarrhea. J Int Assoc Physicians AIDS Care (Chic) 3:121–129
Pawlowska J, Klewicka E, Czubkowski P, Motyl I, Jankowska I, Libudzisz Z, Teisseyre M, Gliwicz D, Cukrowska B (2007) Effect of lactobacillus casei DN-114001 application on the activity of fecal enzymes in children after liver transplantation. Transplant Proc 39:3219–3221
van Baarlen P, Troost F, van der Meer C, Hooiveld G, Boekschoten M, Brummer RJ, Kleerebezem M (2011) Human mucosal in vivo transcriptome responses to three lactobacilli indicate how probiotics may modulate human cellular pathways. Proc Natl Acad Sci U S A 108(Suppl 1):4562–4569
Schwenger EM, Tejani AM, Loewen PS (2015) Probiotics for preventing urinary tract infections in adults and children. Cochrane Database Syst Rev. 12:CD008772
Reid G, Charbonneau D, Erb J, Kochanowski B, Beuerman D, Poehner R, Bruce AW (2003) Oral use of lactobacillus rhamnosus GR-1 and L. fermentum RC-14 significantly alters vaginal flora: randomized, placebo-controlled trial in 64 healthy women. FEMS Immunol Med Microbiol. 35:131–134
Reid G, Bruce AW (2001) Selection of lactobacillus strains for urogenital probiotic applications. J Infect Dis 183(Suppl 1):S77–S80
Reid G, Beuerman D, Heinemann C, Bruce AW (2001) Probiotic lactobacillus dose required to restore and maintain a normal vaginal flora. FEMS Immunol Med Microbiol 32:37–41
Reid G, Bruce AW, Taylor M (1992) Influence of three-day antimicrobial therapy and lactobacillus vaginal suppositories on recurrence of urinary tract infections. Clin Ther 14:11–16
Bruce AW, Reid G (1988) Intravaginal instillation of lactobacilli for prevention of recurrent urinary tract infections. Can J Microbiol 34:339–343
Beerepoot MA, ter Riet G, Nys S, van der Wal WM, de Borgie CA, de Reijke TM, Prins JM, Koeijers J, Verbon A, Stobberingh E, Geerlings SE (2012) Lactobacilli vs antibiotics to prevent urinary tract infections: a randomized, double-blind, noninferiority trial in postmenopausal women. Arch Intern Med 172:704–712
Wolfe AJ, Toh E, Shibata N, Rong R, Kenton K, Fitzgerald M, Mueller ER, Schreckenberger P, Dong Q, Nelson DE, Brubaker L (2012) Evidence of uncultivated bacteria in the adult female bladder. J Clin Microbiol 50:1376–1383
Hilt EE, McKinley K, Pearce MM, Rosenfeld AB, Zilliox MJ, Mueller ER, Brubaker L, Gai X, Wolfe AJ, Schreckenberger PC (2014) Urine is not sterile: use of enhanced urine culture techniques to detect resident bacterial flora in the adult female bladder. J Clin Microbiol 52:871–876
Fouts DE, Pieper R, Szpakowski S, Pohl H, Knoblach S, Suh MJ, Huang ST, Ljungberg I, Sprague BM, Lucas SK, Torralba M, Nelson KE, Groah SL (2012) Integrated next-generation sequencing of 16S rDNA and metaproteomics differentiate the healthy urine microbiome from asymptomatic bacteriuria in neuropathic bladder associated with spinal cord injury. J Transl Med. 10:174
Price TK, Dune T, Hilt EE, Thomas-White KJ, Kliethermes S, Brincat C, Brubaker L, Wolfe AJ, Mueller ER, Schreckenberger PC (2016) The clinical urine culture: enhanced techniques improve detection of clinically relevant microorganisms. J Clin Microbiol 54:1216–1222
Perez-Moreno MO, Pico-Plana E, Grande-Armas J, Centelles-Serrano MJ, Arasa-Subero M, Ochoa NC, Led By Mo Perez-Moreno MOTSGG (2017) Group B streptococcal bacteriuria during pregnancy as a risk factor for maternal intrapartum colonization: a prospective cohort study. J Med Microbiol. 66:454–460
Funding
NIDDK #RO1 DK104718.
Author information
Authors and Affiliations
Contributions
BJW: project development, data collection, and manuscript writing. TP: project development, data collection, and manuscript writing. CJJ: statistical analysis and manuscript writing. AJW: project development and manuscript writing. ERM: project development and manuscript writing.
Corresponding author
Ethics declarations
Conflict of interest
AJ Wolfe: Investigator Initiated Trials from Astellas Scientific and Medical Affairs and from Kimberly Clark Corporation. ER Mueller: Astellas: Investigator initiated research. Boston Scientific: Advisory Board. UroCure: Safety Monitoring Board. UpToDate: Royalties. Butler Snow/Ethicon: Legal Consultation.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wolff, B.J., Price, T.K., Joyce, C.J. et al. Oral probiotics and the female urinary microbiome: a double-blinded randomized placebo-controlled trial. Int Urol Nephrol 51, 2149–2159 (2019). https://doi.org/10.1007/s11255-019-02282-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-019-02282-3