
Abstract
Objectives
To report longitudinal outcomes of a population-based cohort of patients diagnosed with bilateral small renal masses from a period of over 11 years.
Patients and methods
Consecutive patients diagnosed with bilateral small renal masses (synchronous or metachronous) of a defined geographical area were recorded in a large database (TUCAN database) between January 2005 and December 2016. Patients had a unique identifier number and followed during this period using an agreed upon protocol. Clinicopathological characteristics and outcomes of bilateral small renal masses on active surveillance were analysed and compared to propensity score-matched sporadic unilateral small renal masses. Data were analysed for renal mass growth rate, rate of intervention and development of metastatic disease and patient survival.
Results
A total of 1060 patients were diagnosed with renal cancer, of which bilateral small renal masses accounted for 70 (6.6%) cases. Synchronous SRMs were observed in 63 patients, whereas metachronous lesions were found in seven patients during the study period. Metachronous lesion mean time to appearance was 62 ± 41 months (range 9–149 months). While most cases were sporadic, four were found to be hereditary. Growth rate of bilateral small renal masses did not differ from that of unilateral sporadic small renal masses. Similarly, there were no differences between the groups for rate of interventions and survival.
Conclusions
Progression, rate of metastases and survival for patients diagnosed with bilateral small renal masses are similar to those diagnosed with unilateral disease.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is an extensive body of the literature reporting on the topic of unilateral renal cancers. However, there are a limited number of reports that have studied outcomes of patients diagnosed with bilateral renal cell carcinomas [1,2,3]. The natural histories of metachronous and synchronous small renal masses (< 4 cm) are incompletely understood. Most reports on these topics consist of a single or small case series discussing outcomes relating to partial nephrectomy [4, 5]. As such, there has been a rise in the prevalence of bilateral renal cancers due to a number of contributing factors including overall growth of renal cancer incidence rates, early detection due to cross-sectional imaging, increased life expectancy and longer follow-up periods of cancer survivors [6, 7]. These and other factors have resulted in an increasing number of people at risk of developing metachronous or synchronous bilateral primary renal cancer.
Optimal clinical management of patients presenting with cancers affecting both renal units is challenging. Preservation of renal function, optimal oncological control and providing long-term cancer recurrence-free survival are the main objectives of management [8,9,10,11]. However, the decision-making process during this care can be confounded by effects of age, co-morbid conditions and preferences of patients. Further complicating patient care strategies, the rate of progression and interventions for incidentally detected small renal masses (SRMs) found in contralateral renal units during initial or follow-up imaging of treated renal cancers remain poorly understood. While there have been reports out of Norway and Sweden that have analysed large patient datasets [12], crucial information such as histology, grade of cancer, type of intervention including surgical management and long-term follow-up renal function is lacking. Finally, recent data suggest there is a 17-fold increased risk of developing contralateral renal tumours in certain patients under 40 years of age. How multifocal disease with an underlying genetic predisposition should be managed remains open to question. Therefore, to understand and answer some of these questions, we analysed a large database of renal cancer patients in a well-defined geographical area with a population of more than 400,000 provided by a single National Health Services (NHS) Health board in Scotland.
The two primary aims of this study were to (1) identify the incidence of synchronous and metachronous small renal masses in a large population and (2) provide details on long-term outcomes of patients diagnosed with these lesions.
Patients and methods
Study cohort
The study cohort was drawn from a well-defined geographical area over a defined time period. The population of the area was stable with < 1% migration and more than 98% registered with NHS through a unique identifier called CHI number (Community Health Index—CHI). For various indications, 160,820 abdominal imaging tests (CT, MRI, US) were carried out in a population of 118,600 as reported previously [13]. Since 2005, all new primary renal cancers in the region were managed within a single health board and each case was recorded at local multidisciplinary meetings run by a local urological cancer network (TUCAN). Any patient with renal mass (solid on cystic) on imaging is referred to a single point (department of urology) in the region, and none of these are managed in primary care. A MS Word file was generated for each patient and stored in computer on a shared password-protected computer drive following review of radiology and histopathology. The Word file contained unique identifier number (CHI), demographic details, type of presentation, stage, histology, grade, radiological finding and final consensus decision of the multidisciplinary team. Our previous reports have validated the data quality of this process including record linkage methodology through a common identifier (CHI number) using a deterministic record linkage strategy [13,14,15]. Figure 1 summarizes the study cohort, flow and systems used for record linkage. We Identified 1600 patients (treated and untreated) with a primary renal cancer during the study period. Some of these had no histological diagnosis, but imaging was convincing of RCC. TUCAN database captures all patients including those with radiographic masses with possibility of RCC. Out of the total sample, there were 70 patients with synchronous (presenting simultaneously at the same time) or metachronous (developing more than 6 months of initial treatment for unilateral renal lesion) small renal masses. We excluded patients diagnosed with large bilateral renal cancers (> 4 cm) with or without metastatic disease. Patients were also excluded if they demonstrated benign masses confirmed via histopathology analysis following biopsies. All aspects of this study were approved by the institutional review board (Caldicott/CSAppGN021211; Caldicott/IGTCAL2973).

Flow of cohort and record linkage with databases to update information including follow-up
Collected data included radiological details at diagnosis and follow-up imaging. Demographic characteristics, number and type of interventions, complications and follow-up outcomes were analysed. A primary interest of this study was to assess the growth rate of those masses on active surveillance as we have recently published on a larger cohort focusing on active surveillance [15].
All patients suspected to have small renal masses who were referred to the department were given detailed clinical evaluations, abdominopelvic CT scans with a defined protocol, chest X-ray and discussions in multidisciplinary meetings. Each patient was assigned a defined management plan, which included surgical approaches and active surveillance. Surgical approaches/interventions were radical nephrectomy, partial nephrectomy (open) and radiofrequency ablation. For those opting for active surveillance, follow-up imaging included CT scanning at 6-month intervals for 3 years and yearly thereafter. A group of patients diagnosed with bilateral small renal masses were compared with those diagnosed with unilateral disease using propensity score matching for variables known to influence growth such as size and location. Progression was defined as any increase in size on follow-up or change in tumour characteristic on follow-up imaging as described previously [13, 15].
For the active surveillance group, bilateral non-hereditary small renal masses were compared to a control group of patients diagnosed with unilateral sporadic lesions. Control group of patients was with unilateral small renal masses on active surveillance during the same period. Matching was accomplished using propensity score matching using SPSS version 21 software program and variables such as age, sex, size of SRMs, location, duration and co-morbidities. Progression, metastases, need for intervention and survival analyses were carried out.
Bilateral renal masses in this study were managed using following strategies: (1) for those with identified genetic abnormalities, a close radiological surveillance protocol was offered, which included minimally invasive interventions for larger masses (> 3 cm) at presentation or whenever they grow to this size. All patients were managed by a multidisciplinary team because there are other sites where abnormalities can develop such as central nervous system and other organs. Genetic counselling was also made available through a dedicated service; (2) all patients with SRMs < 3 cm were offered active surveillance and interventions were contemplated in those with growing masses or those reluctant to enter active surveillance (AS). Nephron sparing surgery was performed in most cases. This was achieved using a two-stage procedure (one side operating at one time and contralateral on a second setting) in most patients; and (3) image-guided biopsies were offered to all patients demonstrating a tumour size more than 2 cm.
Following surgical or minimally invasive ablations, abdominal CT or MRI and chest X-ray were taken every 3–6 months and then annually during the first 5 years and every 2 years thereafter for lifelong [14]. Recurrence, if noted, was re-discussed in multidisciplinary meetings and appropriate plans were made. Recurrence-free and overall survival was calculated for unilateral and bilateral renal masses (non-hereditary).
Statistical analysis
Bilateral small renal masses diagnosed within 6 months of the first primary visit were categorized as synchronous, whereas the remaining cancers were categorized as metachronous. Patient outcomes for those with bilateral renal masses were compared with those with unilateral masses. Associations between clinicopathological characteristics and follow-up outcomes were analysed using univariate and multivariate cox proportional hazards regression models. The goal of the main analysis was to determine outcome of non-hereditary bilateral SRMs on active surveillance compared with the unilateral SRMs. To assess the adjusted relation, we performed propensity score matching with dependable variable being progression of SRMs. We included all variables which could potentially be confounding based on prior work and/or clinical reasoning. Matching consisted of three steps: (a) propensity scores were developed using covariates which predicted progression of SRMs; and a forward stepwise procedure was used to explore whether baseline characteristics of SRMs such as age, sex, size, duration, presentation, co-morbidities were also associated with progression at the p < 0.10 level. (b) This logistic regression model was used to calculate propensity scores representing the estimated probability of progression contingent on each baseline characteristics. Bilateral SRMs were matched to the unilateral SRMs with the closest propensity score on a ratio of 1:1 using a nearest neighbour greedy algorithm. (c) Various checks were performed to that model was adequate. These included means and variances of covariates after matching, standardized mean differences between bilateral and unilateral SRMs. A matching bias was kept to ≤ 5% to ensure an adequate model. Recurrence-free, cancer-specific and overall survival was assessed using Kaplan–Meier analysis using the log-rank test. Statistical significance was determined using an alpha level of 0.05. Statistical analyses were carried out using SSPS (version 21).
Results
Table 1 shows basic demographic characteristics of the cohort. Most patients demonstrated sporadic synchronous lesions and were predominantly present in males. More than half of the patients (37/70; 52.8%) had surgical excision (radical nephrectomy and nephron sparing surgery). Histological testing showed clear cell carcinoma in most patients. Excised tumours were of low grade in most patients. Thirty-three patients opted for active surveillance (AS) with a mean follow-up of more than 6 years. Figure 2 shows progression rate of bilateral small renal masses on AS in comparison with unilateral small renal masses. There were no statistically significant differences between the two groups. Increases in size of bilateral synchronous lesions were 0.2 cm/year compared to 0.25 mm/year for unilateral small renal masses. Patients with familial disease (n = 4) were managed using minimally invasive treatment options (radiofrequency ablation). Larger lesions (more than 3 cm) were targeted for ablation (radiofrequency ablation in most) on follow-up. None of the patients developed renal failure or metastatic disease. There were seven patients with metachronous lesions. Mean time for appearance of metachronous lesion was 62 ± 41 months (range 9–149 months).

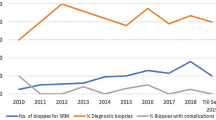
Use of image-guided biopsies usage in bilateral (non-hereditary) and unilateral small renal masses
In patients where a surgical approach was contemplated, the nephron sparing approach (partial nephrectomy) was the main surgical technique utilized. All partial excisions were carried out sequentially with mean duration of 7.0 ± 4.5 weeks between procedures. Seven patients had laparoscopic radical nephrectomy due to central location of tumours or where it was thought that partial excision will be risky with potential of higher morbidity. None of the patients undergoing bilateral partial nephrectomy required dialysis or renal replacement therapy.
Thirty-three patients with bilateral small renal masses on AS were compared with 30 patients with unilateral small renal masses. With a mean follow-up of more than 6 years, there were no differences in the rate of intervention, growth rate and development of metastatic disease (Fig. 3, supplementary).
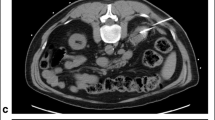
In four patients with non-sporadic disease (hereditary disorders) and multiple bilateral SRMs (Fig. 4, supplementary), interventions were tailored to the progression of disease. Radiofrequency ablation was offered to patients demonstrating larger masses on follow-up, whereas patients demonstrating small lesions (< 3 cm) were followed up using MRI/CT scan at regular intervals. All four cases are asymptomatic, preserved renal function and no evidence of metastatic disease (Table 2).
Image-guided renal biopsy testing was used to confirm histopathology in 12 patients (18 renal units) in the AS group. Most of these showed the presence of renal cell carcinoma. There were four patients, where biopsy-confirmed benign oncocytoma and further interventions were avoided and discharged from secondary care (not part of this study).
Figure 5 (supplementary) shows benign oncocytoma confirmed on histopathology in an 80-year-old lady with previous contralateral nephrectomy for centrally located kidney tumour.
There were no differences in metastasis-free, disease-specific or overall survival between those with unilateral small renal masses in comparison with bilateral disease (Fig. 6, supplementary).
Discussion
The present longitudinal population-based study assessed the outcomes of bilateral small renal masses and found no marked differences between non-hereditary bilateral synchronous and sporadic propensity-matched unilateral renal masses in terms of progression, development of metastatic disease and need for interventional procedures including surgery. When patients diagnosed with bilateral synchronous SRMs opting for active surveillance were compared with those diagnosed with unilateral disease, progression rate and development of distant metastases did not differ between the two groups.
Managing bilateral small renal masses with underlying hereditary abnormalities is a challenging issue. The approach of managing hereditary lesions should be aimed at maintaining quality of life and keeping morbidity as low as possible. Active surveillance along with minimally invasive interventions as described in a small number of cases in this study should preserve renal function and provide metastasis-free survival. Alternate option of aggressive approach of bilateral radical nephrectomy and renal transplantation should be reserved for locally advanced and larger masses. Our approach (active surveillance with minimally invasive intervention on growth) of managing is similar to described by others [16,17,18] and is based on the assumption (backed by reports in the literature) that tumour size < 3 cm shows low rate of metastases and progression. Small renal masses with hereditary genetic abnormalities seen in our series were very aggressive and some demonstrated interval growth of more than 3 cm. They required on average four procedures per patient over a mean period of 46 months of follow-up. All these procedures were day case and patients had no complications. Further studies in larger cohort of patients are required to confirm the proposed benefits of this approach.
Non-hereditary bilateral synchronous SRMs showed no striking differences to unilateral SRMs in terms of progression and development of metastatic disease when they opted for active surveillance. This is noteworthy and consistent with findings of Blute et al. [19]. Observations in this study suggest that despite bilateralism, SRMs behaviour in a particular size range (< 4 cm) remains the same. In our experience, most of the metastases develop within first 2 years of follow-up and some of these may be missed subtle disease in distant organs at the time of first detection [20]. In contrast to hereditary disease, where growth is fast and multiple interventions are anticipated, non-hereditary disease with bilateral synchronous renal cell carcinoma can be managed by a single nephron sparing surgery with acceptable morbidity.
The rate of metachronous lesion was low compared to reports in the literature [12, 19, 21]. This can be explained by the fact that present study cohort restricted study inclusion to small renal masses as opposed to including renal masses of all sizes. Furthermore, we did not include patients with hereditary or familial predisposition to development of contralateral disease. Small size of the present study may be another contributing factor. Metachronous lesion, however, did show up even after 5 years of treatment of localized small renal masses, highlighting the importance of long-term follow-up of treated small renal masses. This again is similar to evidence from a previous report [22]. An interesting hypothesis and perhaps ongoing debate that metachronous lesion may represent metastatic disease remains to settled. There is need for molecular genetic data to confirm or refute this, and in the absence of further scientific proof, this cannot be confirmed. Most patients in metachronous disease in the present study (6/7) had similar histology (clear cell carcinoma) to the previous contralateral tumours. In one remaining case, there was papillary cell carcinoma in the metachronous lesion. In contrast to Boorjian et al. [23], most of bilateral synchronous tumours were clear cell renal cell carcinoma in non-hereditary synchronous lesions.
Surgical management of bilateral small renal masses may require a different approach in comparison with the literature described for larger bilateral masses. Nephron sparing surgery remains the mainstay of management as carried out in the present study. Radical nephrectomy, less common approach, is only reserved for technically difficult and centrally located lesions. However, options of minimally invasive interventions (radiofrequency ablation/cryo) should be considered as fundamental principle of surgical approach in these cases remains nephron sparing and preservation of renal function without compromising oncological outcomes. Whether surgery should be performed in one stage or in two stages depends on expertise and complexity of the cases. Careful planning and discussion with patient is important. The essential principles are: eradication of cancer, preservation of renal function and avoidance of dialysis and minimizing morbidity. Procedure should be staged in patients where there is high risk of acute kidney injury and prolonged hospitalization. RENAL nephrometry score should be consider as a guide to assess complexity of the lesions as post-operative complications and morbidity can be predicted through these score [24, 25]. As described above, patients with hereditary small renal masses, should have a combination of AS and judicious utilization of minimally invasive treatment options.
In a subset of patients with synchronous bilateral SRMs on active surveillance, image-guided biopsies were performed. In smaller renal masses < 2 m, no histological confirmation was available in the present cohort. This is a limitation of the study. Besides histological confirmation, biopsy may provide opportunity for molecular profiling of the SRMs and better risk stratification of therapeutic options and follow-up. Small size and single institutional design are the other limitations of the study. Nevertheless, data in the present cohort provide several insights into managements of hereditary and non-hereditary bilateral small renal masses including role of active surveillance.
Conclusions
Progression, rate of metastases and survival of bilateral small renal masses are similar to unilateral disease, and active surveillance is a safe option in these cases. Hereditary bilateral small renal masses have different growth trajectory and should be considered separate entity and managed using active surveillance and minimally invasive ablative procedures.
References
Hu XY et al (2017) Surgical strategy of bilateral synchronous sporadic renal cell carcinoma—experience of a Chinese University Hospital. World J Surg Oncol 15(1):53
Berczi C et al (2016) Bilateral renal cancers: oncological and functional outcomes. Int Urol Nephrol 48(10):1617–1622
Wells GM et al (2009) Bilateral renal-cell carcinoma associated with an acquired VHL mutation and long-term trichloroethylene exposure. Clin Nephrol 71(6):708–713
Jacobs SC, Berg SI, Lawson RK (1980) Synchronous bilateral renal cell carcinoma: total surgical excision. Cancer 46(11):2341–2345
Yu CC et al (1992) Simultaneous bilateral adrenal metastases from renal cell carcinoma. Surgical implications and review of the literature. Eur Urol 22(4):335–338
Tracy CR et al (2010) Durable oncologic outcomes after radiofrequency ablation: experience from treating 243 small renal masses over 7.5 years. Cancer 116(13):3135–3142
Hollingsworth JM et al (2006) Rising incidence of small renal masses: a need to reassess treatment effect. J Natl Cancer Inst 98(18):1331–1334
Wang B et al (2016) Bilateral synchronous sporadic renal cell carcinoma: retroperitoneoscopic strategies and intermediate outcomes of 60 patients. PLoS ONE 11(5):e0154578
Qi N et al (2017) Clinicopathologic features and prognosis of sporadic bilateral renal cell carcinoma: a series of 148 cases. Clin Genitourin Cancer 15(5):618–624
Pahernik S et al (2007) Bilateral synchronous sporadic renal cell carcinoma: surgical management, oncological and functional outcomes. BJU Int 100(1):26–29
Jacobs BL et al (2009) Management of bilateral synchronous renal cell carcinoma in a single versus staged procedure. Can J Urol 16(1):4507–4511
Wiklund F et al (2009) Risk of bilateral renal cell cancer. J Clin Oncol 27(23):3737–3741
Leonard M et al (2013) Impact of multiple deprivations on detection, progression and interventions in small renal masses (less than 4 cm) in a population based study. Eur J Surg Oncol 39(10):1157–1163
Ganeswaran D et al (2014) Population-based linkage of health records to detect urological complications and hospitalisation following transrectal ultrasound-guided biopsies in men suspected of prostate cancer. World J Urol 32(2):309–315
Paterson C et al (2017) Predictors of growth kinetics and outcomes in small renal masses (SRM ≤ 4 cm in size): Tayside Active Surveillance Cohort (TASC) Study. Eur J Surg Oncol 43:1589–1597
Haas NB, Nathanson KL (2014) Hereditary kidney cancer syndromes. Adv Chronic Kidney Dis 21(1):81–90
Rednam SP et al (2017) Von Hippel–Lindau and hereditary pheochromocytoma/paraganglioma syndromes: clinical features, genetics, and surveillance recommendations in childhood. Clin Cancer Res 23(12):e68–e75
Walther MM et al (1999) Clinical and genetic characterization of pheochromocytoma in von Hippel–Lindau families: comparison with sporadic pheochromocytoma gives insight into natural history of pheochromocytoma. J Urol 162(3 Pt 1):659–664
Blute ML et al (2003) The effect of bilaterality, pathological features and surgical outcome in nonhereditary renal cell carcinoma. J Urol 169(4):1276–1281
Paterson C et al (2017) Predictors of growth kinetics and outcomes in small renal masses (SRM ≤ 4 cm in size): Tayside Active Surveillance Cohort (TASC) Study. Eur J Surg Oncol 43(8):1589–1597
Klatte T et al (2007) Metachronous bilateral renal cell carcinoma: risk assessment, prognosis and relevance of the primary-free interval. J Urol 177(6):2081–2086 (discussion 2086-7)
Kume H, Teramoto S, Kitamura T (2009) Metachronous bilateral renal cell carcinoma with an interval of more than 10 years. Int Urol Nephrol 41(4):843–846
Boorjian SA et al (2008) The impact of temporal presentation on clinical and pathological outcomes for patients with sporadic bilateral renal masses. Eur Urol 54(4):855–863
Canter D et al (2011) Utility of the R.E.N.A.L. nephrometry scoring system in objectifying treatment decision-making of the enhancing renal mass. Urology 78(5):1089–1094
Yoshida K et al (2016) Comparison of diameter-axial-polar nephrometry score and RENAL nephrometry score for surgical outcomes following laparoscopic partial nephrectomy. Int J Urol 23(2):148–152
Funding
Research study did not have any external funding
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest declared by authors for the work presented in this study.
Ethical approval
All data collected in the study involving human participants were in accordance with the ethical standards of the institutional approval, and approval numbers were Caldicott/CSAppGN021211; Caldicott/IGTCAL2973.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Fig.
3, supplementary: Outcomes of small renal masses (bilateral vs. unilateral) on follow-up. (JPEG 72 kb)
Fig.
4, supplementary: Multiple bilateral renal masses in a patient with VHL hereditary disease. Larger lesions were targeted using minimally invasive ablative technique. (JPEG 58 kb)
Fig.
5, supplementary: Image-guided biopsy-confirmed oncocytoma as seen on MRI in an eighty-year-old lady with history of previous laparoscopic radical nephrectomy for contralateral small renal mass. (PNG 305 kb)
Fig.
6, supplementary: Metastasis-free survival in unilateral vs. bilateral (non-hereditary) small renal masses (TIFF 838 kb)
Rights and permissions
About this article

{kind=link}
{kind=link}
{kind=link}
Cite this article
Sheikh, N.A., Khan, M.H., Pillai, S. et al. Outcomes of synchronous and metachronous bilateral small renal masses (< 4 cm): a population-based cohort study. Int Urol Nephrol 50, 657–663 (2018). https://doi.org/10.1007/s11255-018-1817-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-018-1817-x