
Abstract
Purpose
To investigate the predictive value of preoperative serum neutrophil-to-lymphocyte ratio (NLR) on the development of postoperative infections in patients undergoing penile prosthesis implantation (PPI).
Methods
We retrospectively analyzed the data of 361 patients who underwent PPI over a 4-year period with at least 1-year follow-up. Demographics, blood results, and postoperative 1-year complications were recorded. Recommended cutoff values of NLR for early postoperative infectious complications were determined using receiver operating characteristic analysis.
Results
A total of 153 patients with the mean age of 56.4 ± 8 years were included in the study. Mean follow-up time was 56.7 ± 30.4 months (12–108 months). Early postoperative infectious complications were occured in 18 patients (11.8%). These infections were prosthesis infection in 8 patients (5.2%), wound infection in 6 patients (3.9%), and urinary tract infection in 4 patients (2.6%). All these complications were occured within the first year of the surgery. Mean NLR was statistically higher in patients with postoperative complications when compared with uncomplicated cases (7.2 ± 3.9 vs. 2.2 ± 1.4, p < 0.001, respectively) Using a cut point of 6.2, preoperative NLR predicted postoperative complications with a sensitivity of 67% and specificity of 99%.
Conclusions
This study is the first to investigate the relationship between NLR and early postoperative infection as a complication of PPI. The results demonstrated that the NLR value could be a potential laboratory parameter for predicting early postoperative infectious complications in patients undergoing PPI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Erectile dysfunction (ED) is the most common male sexual disorder after premature ejaculation. The incidence of ED is age-related and nearly affects more than half of men between 40 and 70 years of age [1, 2]. Surgical implantation of a penile prosthesis is the preferred option for definitive treatment of ED for men who do not respond to or are unwilling to consider pharmacologic or less-invasive treatment methods [3]. Patients who underwent penile prosthesis implantation have higher satisfaction levels than the patients using intracavernosal injections or phosphodiesterase type-5 inhibitors.(PDE5I) [4].
Although PPs have a high satisfaction rate for patients and their partners, like all implanted devices, PPs are potentially subject to postoperative infection [5]. Improvements in surgical procedure, device design, and antibiotic regime have decreased the incidence of infection. Despite these factors, the prevalence of penile prosthesis infection (PPI) in modern series is estimated to be between 1 and 20% [6, 7]. These rates may further decline dramatically with the use of drug-coated prostheses for both first time and repeat implantations [8, 9].
Infections of implants or prosthesis are one of the most challenging and particularly devastating complications associated with the implantation of these devices because they cannot be treated with antibiotics alone and require the revision surgeries or removal of all device components. All these interventions cause to high financial costs and patient comorbidities. In order to minimize these troubles, foresight of the prosthetic device infection prior to the implantation is crucial. In accordance with this purpose, preoperative inflammation markers have become the point of interest. In a systematic review and meta-analysis, Berbari et al. [10] reported that preoperative interleukin-6 (IL-6), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and white blood cell count have diagnostic accuracies for prosthetic joint infection in patients with a total hip or knee arthroplasty. Neutrophil-to-lymphocyte ratio (NLR) is an easy, cheap, widely available, robust, and convenient biomarker of the inflammatory response and has been shown to predict outcomes in oncology, digestive and cardiovascular diseases, and hematogenous infections [11–13]. Recently, a link between systemic inflammation and postoperative morbidity was identified by Moyes et al. [14]. In their study, the presence of the preoperative systemic inflammatory response itself independently predicted postoperative infectious complications in patients undergoing curative resection for colorectal cancer. In another study, Yombi et al. [15] suggested that NLR is potentially a better biomarker to follow-up of postoperative inflammation or early infection after total knee arthroplasty.
Above-mentioned studies present a complex link between systemic inflammation and postoperative morbidity. In our study, we aimed to investigate the relationship between systemic inflammatory response and early postoperative infectious complications in patients undergoing PPI. In this context, in order to reveal this relationship, we used NLR as a systemic inflammation marker.
Materials and methods
Patients undergoing PPI for ED between August 2001 and September 2015 at a single institution were identified using a prospectively maintained database. These data were analyzed retrospectively, with additional information obtained from hospital records. Informed consent was obtained from all participants included in the study.
Indications for PPI were failure or intolerance of medical treatment, confirmation of ED by Doppler ultrasound or cavernosography, and severe ED. Patients with irregular follow-up, missing data and patients who had undergone secondary implant surgery were excluded from the study.
All men underwent medical and psychiatric counseling prior to penile prosthesis implantation. Insertion of a penile prosthesis was postponed if the urine was infected or patient’s inner thigh and perineal region showed evidence of skin rash, pimples, or infection. All operations were performed by two experienced surgeons in the single center under the intravenous antibiotic prophylaxis and spinal anesthesia. With a 10-min surgical scrub following intra-operative surgical shave and stringent surgical practice such as full protective head cover and limited theater traffic, the penile prosthesis was implanted. In most cases, a single penoscrotal incision was performed; an infrapubic incision was used for implantation of three-piece IPP. The device was irrigated with mixed antibiotics solution before implantation and prophylactic antibiotic was prescribed until the postoperative 7th day and activation of device was scheduled in the 6th week after surgery. The most commonly implanted PP types were AMS 600-650 followed by Mentor Acu-Form, AMS Ambicor, AMS 700 CX, AMS Ultrex, and AMS Ultrex Plus (AMS, Inc., Minnetonka, MN, USA; Mentor, Goleta, CA, USA).
All patients were followed up for a minimum of 12 months postoperative. All surgical complications such as prosthesis infection, wound infection or hematoma, and any revision or explantation surgeries were recorded. The data about preoperative assessment and postoperative complications were collected retrospectively from the patients’ records. Complete blood cell count (CBC) was measured at 1–7 days prior to the surgery, and the NLR was calculated as the absolute neutrophil count divided by the absolute lymphocyte count.
Statistical analysis
Data were analyzed with SPSS version 20.0 statistical software (SPSS Inc., Chicago, IL, USA). Comparability between groups was tested using the independent samples t test for continuous variables and the Chi-square test for categorical variables. Receiver operating characteristic (ROC) curve was generated to assess the predictive role of NLR for postoperative complications. A cutoff value for NLR was calculated using Youden index method.
Results
Totally, 361 patients underwent PPI surgery in our clinic. After the exclusion of patients with missing data, a total of 153 patients were included in the study. The mean age of the patients was 56.4 ± 8 years (28–72 years). The majority of patients (56 patients (36.6%)) underwent PPI due to diabetes mellitus. The remaining 43 patients (28.1%) underwent surgery for vascular diseases, and 39 patients (25.5%) had radical pelvic surgery. Forty-nine patients (32%) underwent malleable PPI, and 104 patients (68%) had semirigid PPI (Table 1).
Mean follow-up time was 56.7 ± 30.4 months (12–108 months). Early postoperative complications were occured in 18 patients (11.8%). These complications were prosthesis infection in 8 patients (5.2%), wound infection in 6 patients (3.9%), and urinary tract infection in 4 patients (2.6%) (Table 2). All these complications were occured within the first year of the PPI. On the infected prosthesis, the most commonly identified organisms were Escherichia coli (in 5 patients), Staphylococcus epidermidis (in 3 patients), and Staphylococcus aureus (in 2 patients) (Table 3). Of the complicated patients, 5 of them underwent revision surgery (3.3%) due to wound infection and abscess formation and 10 of them (6.5%) underwent prosthesis explantation.
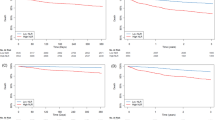
Preoperative neutrophil count and NLR were significantly higher in complicated group; however, lymphocyte count was significantly higher in uncomplicated group. Receiver operating characteristics (ROC) curves explored the relation between preoperative NLR and postoperative complications. Area under the curve was 0.91 (95% confidence interval (CI) 0.83–0.98; p < 0.001). Using a cut point of 6.2, preoperative NLR predicted postoperative complications with a sensitivity of 67% and specificity of 99% (Fig. 1).

Receiver operating characteristic (ROC) curves for NLR in predicting early postoperative infectious complications. The ROC curve is a graphic plot of the positive rate (sensitivity) versus the false-positive rate (specificity) for detection of early postoperative infection. The NLR of 6.2 had sensitivity of 67% and specificity of 99%. AUC was 0.91 (95% confidence interval (CI) 0.83–0.98; p < 0.001)
Discussion
The NLR represents a simple, robust, and convenient parameter of the inflammatory response [16]. Recent studies demonstrated that NLR may be used as marker of postoperative complications in patients undergoing colorectal surgery [17, 18]. However, the optimal cutoff value of NLR is unclear. Josse et al. [17] showed that the preoperative NLR ≥2.3 was found to be an independent predictor of major surgical complications in patients undergoing colorectal surgery. In this study, authors classified major complications as wound infection, gastrointestinal/genitourinary or cardiorespiratory complications, anastomotic leakage, and anemia/bleeding. In another study, Cook et al. [18] reported that the NLR with cutoff value ≥9.3 on the first day after an elective colorectal resection was associated with an increased risk of complications such as wound infection, catheter infection, intraabdominal sepsis, pulmonary edema, and arrhythmias. In our study, we investigated the potential predictive role of serum NLR in the diagnosis of postoperative complications in patients undergoing PPI surgery.
Several studies have demonstrated a correlation between systemic inflammation and complications after prosthesis or stent implantations [19, 20]. In a prospective study, Bottner et al [19] evaluated the roles of white blood cell count, the erythrocyte sedimentation rate and levels of C-reactive protein, interleukin-6, procalcitonin, and tumor necrosis factor (TNF)- in the diagnosis of deep implant infection in 78 patients with a revision total knee or hip replacement. As a result, they found that the combination of C-reactive protein and interleukin-6 measurement provides excellent screening tests for infection of a deep implant. However, Yombi et al. [15] reported that NLR was an easy and cheap biomarker to be included in the follow-up after total knee arthroplasty because it has a rapid return to normal values in the absence of complications. Furthermore, authors suggested that if NLR remains high, it is undoubtedly a sign of an underlying inflammatory or infectious problem. Another study was performed by Turak et al. [20] which investigating the association between preprocedural NLR and postprocedural complication after coronary stent implantation. In this study, authors demonstrated that NLR >2.73 had 80% sensitivity and 75% specificity in predicting in-stent restenosis [20]. The present study is the first to investigate the use of preoperative NLR to predict early postoperative complications in patients undergoing PPI (Table 4).
Infection rates continue to decline, but infection remains one of the most concerning complications with prosthetic surgery. The incidence of infection is about 0.8–8.9% [21, 22]. Most infections develop within the first 3 months after the implantation and vast majority will appear within the first year after surgery [23]. Risk factors for penile implant infection can be divided into patient-related and surgical factors. Postulated patient-related factors include diabetes, degree of diabetic sugar control, presence and treatment of pathologic nasal flora, long-term steroid use, patient preoperative cleansing with antiseptics, smoking history, HIV status, history of radiation therapy, revision versus virgin implantation, spinal cord injury, obesity, concomitant circumcision, and prior renal transplantation [24]. Surgical factors pertaining to risk of infection include hair removal strategies, presence of device coatings on implants, use of surgical drains, minimization of device contact with skin, surgical approach, skin preparation type, surgeon experience, perioperative antibiotics, postoperative antibiotics, surgeon hand cleansing, and institutional processes to decrease infection [24]. After the PP infections, most commonly identified microorganisms were S. epidermidis, S. aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa, E. coli, and Candida albicans [25]. In our study, postoperative infectious complication was observed in 18 patients (9.2%). Of these patients, 8 of them had prosthesis infection, 6 of them had wound infection, and 4 of them had urinary tract infection. In our series, S. epidermidis and E. coli were the most commonly identified agents. Our findings were consistent with the current literature.
Infections of implants are particularly devastating because they cannot be treated with antibiotics alone and require the removal of all device components. If a salvage procedure is not performed, explantation results in complete loss of erectile function and renders the patient unresponsive to oral and intracavernous medications [26]. Removal of space occupying cylinders coupled with the infectious process results in marked penile corporal fibrosis and shortening of up to 2 inches of length [26]. Subsequent IPP implantation is limited by the decreased penile size and extensive scarring in the surgical field [27]. Furthermore, it has been estimated that treating infected penile prostheses exceeds the cost of the original implant by more than sixfold [28]. In salvage procedure, after the removal of the all prosthetic materials followed by the use of Mulcahy salvage procedure, a new PPI is performed at the same session [29]. In our series, of the complicated patients 5 of them (3.3%) underwent revision surgery due to wound infection and abscess formation and 10 of them (6.5%) underwent explantation of the implants. Selection of the treatment modality was determined on the patient basis and experience of the surgeon.
Considering the significant economical costs and patient morbidities related with the PPI infections, preoperative prediction of the infectious complications is crucial. With this aim, Lynch et al. [30] investigated the association between glycosylated hemoglobin and PP infections, and reported that patients with glycosylated hemoglobin <11.5% more likely to have PP infection. In another study, Cakan et al. [22] demonstrated the increased PP infection risk in patients with >200 ng/ml morning glucose level. In our study, we analyzed the effects of systemic inflammatory process on the postoperative infectious complications after PPI. We used serum NLR as an inflammation marker. According to our results, serum neutrophil count and NLR were significantly higher in patients with complications. Furthermore, we performed ROC curve analysis to determine the cutoff level for NLR to predict the postoperative infectious complications, and found that preoperative NLR ≥6.2 had high specificity and sensitivity for predicting PPI-related early postoperative infection.
The association between elevated NLR and the development of postoperative infectious complication is likely complex and remains unclear; however, possible explanations exist. NLR, which is derived from the absolute neutrophil and absolute lymphocyte counts of a full blood count, is a routinely available marker of the systemic inflammatory response. The antibacterial responses of natural killer cells and activated T cells may be suppressed by increased number of neutrophils near the site of bacterial contamination [31]. A high NLR reflects both a heightened neutrophil-dependent inflammatory response and a decreased lymphocyte-mediated antibacterial immune reaction, which may weaken the lymphocyte-mediated antibacterial cellular immune response and contribute to increasing bacterial invasion and growth [32]. Also, circulating interleukin-6 level, which promotes the proliferation of immature neutrophils in the circulation and stimulates mature neutrophils to release superoxide anion as a reaction to surgical trauma, may contribute to oxygen radical-mediated tissue injury and bacterial invasion [32]. Although the exact mechanism remains unclear, the results of our study suggest that NLR, as a simple preoperative inflammatory biomarker, may identify patients at increased risk for postoperative infectious complications after PPI.
The strength of this study is that results were available for NLR allowing to compare this biochemical marker. All patients underwent the same type of surgery by the same surgeons.
Our study has some limitations. First, this study was conducted on a retrospective basis and represented a single-center experience. Second, we could not reach the data of whole patients, so that, the number of complicated patients without missing data is very low. Third, we did not study other inflammation markers. Because we do not routinely study all the inflammation markers prior to PPI, and retrospective design of the study, we do not have the data of other biomarkers.
Conclusion
The NLR seems to be a compelling, convenient, and cheap biomarker for the prediction of the early postoperative infectious complications after PPI surgery. A higher preoperative NLR value of ≥6.2 may be an optimal value for determining the PP implanted patients who are at the risk of postoperative infectious events. The NLR may be a predictor tool that could be used in combination with other predictor tools, such as age, serum glucose level, or glycosylated hemoglobin to aid in clinical decision making, prompting surgeons to employ different strategies in the hope of mitigating the occurence or severity of the postoperative complications. Further prospective studies with larger series and inflammation markers are required to evaluate the clinical implications of our findings.
References
Antonini G, Busetto GM, De Berardinis E, Giovannone R, Vicini P, Del Giudice F et al (2016) Minimally invasive infrapubic inflatable penile prosthesis implant for erectile dysfunction: evaluation of efficacy, satisfaction profile and complications. Int J Impot Res 28:4–8
Simsek A, Kucuktopcu O, Ozgor F, Ozkuvanci U, Baykal M, Sarilar O et al (2014) Self and partner satisfaction rates after 3 part inflatable penile prosthesis implantation. Arch Ital Urol Androl 86:219–221
Evans C (1998) The use of penile prostheses in the treatment of impotence. Br J Urol 81:591–598
Kucuk EV, Tahra A, Bindayi A, Onol FF (2016) Erectile dysfunction patients are more satisfied with penile prosthesis implantation compared with tadalafil and intracavernosal injection treatments. Andrology 4:952–956
Bozkurt IH, Arslan B, Yonguç T, Kozacıoglu Z, Degirmenci T, Gunlusoy B et al (2015) Patient and partner outcome of inflatable and semi-rigid penile prosthesis in a single institution. Int Braz J Urol 41:535–541
Minervini A, Ralph DJ, Pryor JP (2006) Outcome of penile prosthesis implantation for treating erectile dysfunction: experience with 504 procedures. BJU Int 97:129–133
Natali A, Olianas R, Fisch M (2008) Penile implantation in Europe: successes and complications with 253 implants in Italy and Germany. J Sex Med 5:1503–1512
Carson CC 3rd, Mulcahy JJ, Harsch MR (2011) Long-term infection outcomes after original antibiotic impregnated inflatable penile prosthesis implants: up to 7.7 years of followup. J Urol 185:614–618
Nehra A, Carson CC 3rd, Chapin AK, Ginkel AM (2012) Long-term infection outcomes of 3-piece antibiotic impregnated penile prostheses used in replacement implant surgery. J Urol 188:899–903
Berbari E, Mabry T, Tsaras G, Spangehl M, Erwin PJ, Murad MH et al (2010) Inflammatory blood laboratory levels as markers of prosthetic joint infection. J Bone Joint Surg Am 92:2102–2109
Bhat T, Teli S, Rijal J, Bhat H, Raza M, Khoueiry G et al (2013) Neutrophil to lymphocyte ratio and cardiovascular diseases: a review. Expert Rev Cardiovasc Ther 11:55–59
Lowsby R, Gomes C, Jarman I, Lisboa P, Nee PA, Vardhan M et al (2015) Neutrophil to lymphocyte count ratio as an early indicator of blood stream infection in the emergency department. Emerg Med J 32:531–534
Guthrie GJ, Charles KA, Roxburgh CS, Horgan PG, McMillan DC, Clarke SJ (2013) The systematic inflammation-based neutrophil-lymphocyte ratio: experience in patients with cancer. Crit Rev Oncol Hematol 88:218–230
Moyes LH, Leitch EF, McKee RF, Anderson JH, Horgan PG, McMillan DC (2009) Preoperative systemic inflammation predicts postoperative infectious complications in patients undergoing curative resection for colorectal cancer. Br J Cancer 100:1236–1239
Yombi JC, Schwab PE, Thienpont E (2016) Neutrophil-to-lymphocyte ratio (NLR) distribution shows a better kinetic pattern than C-reactive protein distribution for the follow-up of early inflammation after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 24:3287–3292
Paramanathan A, Saxena A, Morris DL (2014) Asystematic review and meta-analysis on the impact of pre-operative neutrophil lymphocyte ratio on long term outcomes after curative intent resection of solid tumors. Surg Oncol 23:31–39
Josse JM, Cleghorn MC, Ramji KM, Jiang H, Elnahas A, Jackson TD et al (2016) The neutrophil/lymphocyte ratio predicts major perioperative complications in patients undergoing colorectal surgery. Colorectal Dis 18:O236–O242
Cook EJ, Walsh SR, Farooq N, Alberts JC, Justin TA, Keeling NJ (2007) Post-operative neutrophil-lymphocyte ratio predicts complications following colorectal surgery. Int J Surg 5:27–30
Bottner F, Wegner A, Winkelmann W, Becker K, Erren M, Götze C (2007) Interleukin-6, procalcitonin and TNF-alpha: markers of peri-prosthetic infection following total joint replacement. J Bone Joint Surg Br 89:94–99
Turak O, Ozcan F, Isleyen A, Tok D, Sokmen E, Buyukkaya E et al (2012) Usefulness of the neutrophil-to-lymphocyte ratio to predict bare-metal stent restenosis. Am J Cardiol 110:1405–1410
Chung E, Van CT, Wilson I, Cartmill RA (2013) Penile prosthesis implantation for the treatment for male erectile dysfunction: clinical outcomes and lessons learnt after 955 procedures. World J Urol 31:591–595
Cakan M, Demirel F, Karabacak O, Yalçinkaya F, Altuğ U (2003) Risk factors for penile prosthetic infection. Int Urol Nephrol 35:209–213
Sadeghi-Nejad H (2007) Penile prosthesis surgery: a review of prosthetic devices and associated complications. J Sex Med 4:296–309
Levine LA, Becher E, Bella A, Brant W, Kohler T, Martinez-Salamanca JI et al (2016) Penile prosthesis surgery: current recommendations from the international consultation on sexual medicine. J Sex Med 13:489–518
Donlan RM, Costerton JW (2002) Biofilms: survival mechanisms of clinically relevant microorganisms. Clin Microbiol Rev 15:167–193
Martinez DR, Mennie PA, Carrion R (2012) Erectile function significant enough for penetration during sexual intercourse after removal of inflatable penile prosthesis. J Sex Med 9:2938–2942
Martinez-Salamanca JI, Mueller A, Moncada I, Carballido J, Mulhall JP (2011) Penile prosthesis surgery in patients with corporal fibrosis: a state of the art review. J Sex Med 8:1880–1889
Carson CC (2003) Diagnosis, treatment and prevention of penile prosthesis infection. Int J Impot Res 15(Suppl 5):S139–S146
Mulcahy JJ, Brant MD, Ludlow JK (1995) Management of infected penile implants. Tech Urol 1:115–119
Lynch MJ, Scott GM, Inglis JA, Pryor JP (1994) Reducing the loss of implants following penile prosthetic surgery. Br J Urol 73:423–427
Shau H, Kim A (1988) Suppression of lymphokine-activated killer induction by neutrophils. J Immunol 141:4395–4402
Djeu JY, Serbousek D, Blanchard DK (1990) Release of tumor necrosis factor by human polymorphonuclear leukocytes. Blood 76:1405–1409
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. AnnSurg 240:205–213
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares that he has no conflict of interests, including specific financial interests or relationships and affiliations relevant to the subject matter or materials discussed in the manuscript. No funding was received toward the writing of this letter.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Bolat, D., Topcu, Y.K., Aydogdu, O. et al. Neutrophil to Lymphocyte Ratio as a predictor of early penile prosthesis implant infection. Int Urol Nephrol 49, 947–953 (2017). https://doi.org/10.1007/s11255-017-1569-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-017-1569-z