
Abstract
Objectives
To systematically review the efficacy and safety of acupuncture for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS).
Methods
PubMed, Cochrane library Central, Web of Science, Wang-fang Database, and CNKI were searched from their inception to June 30, 2016. Data of acupuncture for CP/CPPS following randomized controlled trials (RCTs) was included. The data were analyzed using the Cochrane Collaboration Review Manager. The primary data were the National Institute of Health-Chronic Prostatitis Index (NIH-CPSI) score at the end of follow-up.
Results
Ten RCTs were enrolled. Acupuncture was superior to the control in NIH-CPSI (MD −3.98, [95 % CI −5.78 to −2.19]; P < 0.0001) and response rate (RR 4.12, [95 % CI 1.67–10.18]; P = 0.002). Acupuncture was superior to sham acupuncture on NIH-CPSI, response rate, pain, urinary, and quality of life (QOL). Standard medication was inferior to acupuncture in terms of NIH-CPSI (MD −3.08, [95 % CI −5.57 to −0.60]; P = 0.02) and response rate (RR 2.03, [95 % CI 1.04–3.97]; P = 0.04), but standard medication was superior to acupuncture on improving urinary symptoms. There was no significant difference in the adverse events. Acupuncture/acupuncture plus standard medication significantly down-regulated IL-1β compared with standard medication in prostatic fluid.
Conclusion
Acupuncture treating CP/CPPS is effective and safe. The effects of acupuncture on NIH-CPSI, response rate, pain symptoms, and QOF were superior to the control, but standard medication significantly improved urinary symptoms compared with acupuncture. Acupuncture can decrease the IL-1β in prostatic fluid for CP/CPPS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) is a common disease in adult men. Its clinical symptoms include genitourinary pain, lower urinary tract symptoms, and/or sexual dysfunction [1]. It was reported that 2–15 % of adult men were disturbed by CP/CPPS [2, 3]. Due to its etiology and mechanism are unclear, there is no especially effective treatment for it [4–6]. Some studies showed that methods including 5-alpha reductase inhibitors, electrostimulation, surgery, and acupuncture were taken into treatment for CP/CPPS, but their effects were controversial [7].
Acupuncture is an alternative medicine approved in many countries, and is an important component of traditional Chinese medicine [8]. According to traditional Chinese medicine, acupuncture can activate the flow of Qi (energy) through the meridians. Some studies demonstrated that acupuncture had the function of neuromodulation, anti-inflammatory, and immune modulation. But the mechanism of acupuncture for CP/CPPS in modern medicine remains unclear [9].
Acupuncture was used for CP/CPPS for a long time, but has been limited to assess its efficacy due to lack of high-quality, well-designed randomized controlled trials (RCTs). The evidence level is still low. At present, three systematic review/meta-analysis of acupuncture for CP/CPPS published in English were searched. In 2012, a systematic review drew a conclusion that acupuncture was an encouraging therapy for CP/CPPS; however, the conclusion was limited due to the quantity and quality of the evidence [26]. In January 2016, a systematic review and meta-analysis showed that acupuncture has better efficacy for CP/CPPS compared with standard medical treatment [27]. The conclusion was not definite without a meta-analysis based on the subscores of NIH-CPSI. In March 2016, a systematic review revealed acupuncture was an effective treatment for CP/CPPS-induced symptoms, particularly in relieving pain [28]. These reviews did not include some high-quality RCTs published in Chinese in recent years and laboratory indicators such as TNF-α, IL-1β. Therefore, an overall systematic review and meta-analysis should be conducted. We performed this study to re-evaluate the efficacy and safety of acupuncture for treating CP/CPPS.
Materials and methods
Protocol
This study abided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA) [10].
Search strategy
The search strategy was decided according to the guidance of the Cochrane Handbook. We electronically searched the following databases from their inception: PubMed, EMBASE, Cochrane Central Register of Controlled Trials, Web of Science, Wang-fang Database, and CNKI. All RCTs comparing acupuncture vs sham acupuncture or standard medication for CP/CPPS were searched in electronic databases by two authors independently. The key words included “acupuncture,” “electro-acupuncture,” “catgut embedding,” “prostatitis,” “chronic prostatitis,” “chronic pelvic pain syndrome.” There was restriction to publication language (English and Chinese). The search time was set from inception to June 30, 2016. We also consulted the references of published systematic reviews.
Eligibility criteria
Only randomized controlled trials (RCTs) that reporting acupuncture vs sham/placebo acupuncture, or acupuncture plus standard medication vs standard medication, or acupuncture versus standard medication for CP/CPPS were taken for inclusion. CCTs, cohort studies, and case reports were excluded. In addition, studies that did not report the primary outcomes or Jadad Scores <3 were also excluded [13].
Study identification
All titles of searched articles were firstly viewed by two authors independently. Secondly, article abstract associated with the topic was reviewed. Full article was reviewed if information in the abstract was insufficient. Divergence on eligibility of included studies was resolved by the third investigator.
Risk of bias evaluation and scores of methodology
Risk of bias was evaluated according to the Cochrane Collaboration guidelines with seven items: In this study, the methodological scores of eligible studies were calculated using Jadad scale [13] (Table 1). The cutoff value between high and low quality was score 3. The score of above 3 means high-quality trial, and the score of below 3 indicates low-quality trial. Two independent investigators performed the methodological evaluation, respectively. If there was the discrepancy, the third investigator was consulted to resolve it.
Data extraction
Data extraction was performed by two authors independently. If disagreement in outcome extraction occurred, we checked relevant studies until consensus was achieved.
Outcome measures
Primary outcomes contained assessment of total NIHCPSI score at the follow-up [11, 12]. Secondary outcomes included response rate, subscores of NIH-CPSI, IPSS [11, 12], and laboratory indicators. Adverse events were also recorded during the trials.
Statistical analysis
Data analyses were conducted using the Review Manager statistical 5.3 software (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). When there was no statistically significance (P > 0.1) on outcomes of heterogeneity test, a fixed-effect model was adopted in the meta-analysis. Otherwise, a random-effect model was used. Dichotomous outcomes were conducted using risk ratios (RRs) with 95 % CIs.
Results
Study selection
A total of 354 studies were searched, in which 115 duplications were removed and the titles and abstracts of 239 studies remained to be reviewed. The remaining studies were excluded for the following reasons: 150 were non-RCTs, 11 were non-human, and 32 were unrelated to the topic. After scanning titles and abstracts, the full texts of the remaining 46 studies were examined in more detail. It appeared that 29 studies were excluded because they were low-quality RCTs (Jadad score <3), six studies were excluded because they were meta-analysis and systemic review. One trial [14] was updated by a new trials [24] reported by the same author Ma Yong. In these two trials, the enrolled time of participants partially overlapped, so there may exist the possibility of some data reused. So we included the latest published trial. Therefore, a total of ten studies [15–24] were available for analysis in this review. See flow diagram, Fig. 1.

Flowchart of eligibility selection
Study description
There were ten trials [15–24] enrolled in this study: Six trials were from Malaysia, Korea, and Turkey published in English [15–20], and four trials were from China [21–24] published in Chinese, respectively. Treatment sessions were from 4 to 10 weeks. Seven trials set the follow-up period from 3 to 28 weeks.
Participants and patient characteristics
All studies were prospective randomized control trials. The included studies involved at total of 754 adult male participants (n = 376 vs. 378), and 704 participants were included in meta-analysis (n = 347 vs. 357). Demographic data (including age, treatment duration, frequency, treatment sessions, follow-up periods, and adverse events) are listed in Table 2. Acupoints and acupuncture methods are displayed in Table 3. Our results found that there was no significant difference in age, NIH-CPSI scores baseline, IPSS scores baseline, and withdrawal/lost to follow-up rate between acupuncture and control groups. However, duration, frequency, treatment sessions, acupoints, and follow-up periods were different.
Intervention
Five trials compared acupuncture with sham acupuncture, three trials compared acupuncture with standard medication, one trial compared acupuncture with standard medication/sham acupuncture, and one trial compared acupuncture plus standard medication with standard medication. (Table 2)
Outcomes
In eight studies, the primary outcome was analyzed regarding total NIH-CPSI score (Table 4) at the baseline and study completion/follow-up endpoint. Two trials [16, 18] of these studies were excluded from pooled analysis due to using NIH-CPSI score reduction without raw scores. The secondary outcomes were assessed according to response rate, IPSS (Table 4), subscore of NIH-CPSI (Table 5), and laboratory indicators (Table 6) in some trials.
Risk of bias within studies
Two reviewers evaluated the included trials using the risk of bias (ROB) tool recommended by the Cochrane Handbook. Not all RCTs provided the full information. Ten trials were considered as having unclear risk of bias. Five RCTs, which compared acupuncture to standard medication or acupuncture plus medication to standard medication, were rated as high risk of bias without adequate blinding information [18, 21–24]. One RCT provided total NIH-CPSI score without subscores [24]. Five RCTs did not report adverse events [17–21], and three RCTs were short of drop-offs [18–20]. There was a risk of incomplete outcome data and/or selective outcome report. Two RCTs with a small size was rated as having a high risk in other sources of bias [16, 20].
Acupuncture versus control
-
1.
NIH-CPSI total score: Two trials in eight studies were excluded due to the lack of raw scores [16, 18]. A total of 521 participants from six trials were accepted the pooled analysis. This results revealed that acupuncture significantly decreased NIH-CPSI total score compared with the controls (−3.98, [95 % CI −5.78 to −2.19]; P < 0.0001) with moderate heterogeneity (I 2 = 72 %) [15, 17, 21–24] (Fig. 2).
Fig. 2 
Follow-up NIH-CPSI scores between acupuncture and control groups
-
2.
IPSS score: Total IPSS score in two trials were reported as a secondary outcome [15, 16]. Lee et al. reported total IPSS end-point score [15], but Lee et al. reported total IPSS score reductions from baseline to end-point [16]. So these two trials cannot execute a pooled analysis.
-
3.
Response rate: Response rates of 443 participants from five trials were performed the meta-analysis. The results showed favorable effects of acupuncture on increasing the response rate (RR 4.12, [95 % CI 1.67–10.18]; P = 0.002) with moderated heterogeneity (I 2 = 67 %) [15–17, 23, 24] (Fig. 3).
Fig. 3 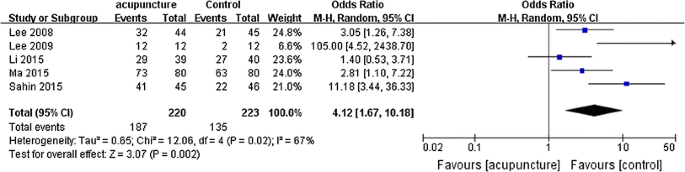
Responder rate between acupuncture and control groups
-
4.
NIH-CPSI pain, urinary, and quality of life domain subscore: Five RCTs involving 361 participants were performed the meta-analysis in NIH-CPSI pain, urinary, and quality of life domain subscore. The results revealed that acupuncture on alleviating pain was prior to control group (MD −2.12, [95 % CI −3.54 to −0.69]; P = 0.004) with high heterogeneity (I 2 = 82 %) [15, 17, 21–23] (Fig. 4). However, there was no difference in improving urinary between acupuncture and control group (MD −0.45, [95 % CI −1.32 to 0.42]; P = 0.31) with high heterogeneity (I 2 = 88 %) [15, 17, 21–23] (Fig. 5). In improving quality of life, acupuncture was prior to control group (MD −1.60, [95 % CI −3.02 to −0.18]; P = 0.03) with moderated heterogeneity (I 2 = 69 %) [15, 17, 21–23] (Fig. 6).
Fig. 4 
Follow-up pain subscores between acupuncture and control groups
Fig. 5 
Follow-up urinary subscores between acupuncture and control groups
Fig. 6 
Follow-up QOL subscores between acupuncture and control groups





Acupuncture versus sham acupuncture
-
1.
NIH-CPSI total score: Four RCTs involving 247 participants compared acupuncture to sham acupuncture, one of which was excluded because of only recording total NIH-CPSI reduction score [16]. In total 224 participants from three RCTs accepted pooled analysis.
Meta-analysis showed a significant difference in favor of acupuncture (MD −7.80, [95 % CI −10.92 to −4.68]; P < 0.00001) with moderate heterogeneity (I 2 = 70 %) [15, 17, 22] (Fig. 7).
Fig. 7 
Follow-up NIH-CPSI scores between acupuncture and sham acupuncture groups
-
2.
Response rate: Three trials involving 204 participants compared response rate of acupuncture to sham acupuncture. A meta-analysis revealed that acupuncture significantly increased response rate compared with sham acupuncture (RR 1.93, [95 % CI 1.31–2.88]; P = 0.0008) with moderated heterogeneity (I 2 = 51 %) [15–17] (Fig. 8).
Fig. 8 
Responder rate between acupuncture and sham acupuncture groups
-
3.
NIH-CPSI pain, urinary, and quality of life domain subscore: Three RCTs involving 224 participants compared acupuncture to sham acupuncture. Meta-analysis showed a more favorable effects of acupuncture on reducing pain (MD −3.76, [95 % CI −6.81 to −0.70]; P = 0.02) with high heterogeneity (I 2 = 91 %) [15, 17, 22] (Fig. 9). A sensitivity analysis was performed in heterogeneity: One trial was conducted by Zhao and Song. Eliminating the previous trial conducted by Zhao and Song, the heterogeneity could be accepted and vanished (I 2 = 70 %) with a favorable effects of acupuncture (MD −2.30, [95 % CI −4.47 to −0.12]; P = 0.04) [15, 17] (Fig. 10). Acupuncture significantly decreased the urinary subscore compared with sham acupuncture (MD −1.61, [95 % CI −2.40 to −0.82]; P < 0.00001) with moderated heterogeneity (I 2 = 69 %) [15, 17, 22] (Fig. 11). Acupuncture significantly improved quality of life (MD −2.68, [95 % CI −4.59 to −0.77]; P = 0.006) with moderated heterogeneity (I 2 = 69 %) [15, 17, 22] (Fig. 12).
Fig. 9 
Follow-up pain subscores between acupuncture and sham acupuncture groups
Fig. 10 
Follow-up pain subscores between acupuncture and sham acupuncture groups
Fig. 11 
Follow-up urinary subscores between acupuncture and sham acupuncture groups
Fig. 12 
Follow-up QOL subscores between acupuncture and sham acupuncture groups






Acupuncture versus standard medication
-
1.
NIH-CPSI total score: Four trials compared acupuncture to standard medication, one of which was excluded because there was total NIH-CPSI reduction score without total score at the endpoint [18]. Only three RCTs involving 297 participants received pooled analysis. We found a significant difference in favor of acupuncture (MD −3.08, [95 % CI −5.57 to −0.60]; P = 0.02) with moderate heterogeneity (I 2 = 80 %) [22–24] (Fig. 13)
Fig. 13 
Follow-up NIH-CPSI scores between acupuncture and standard medication groups
-
2.
Response rate: Two trials involving 192 participants compared acupuncture to standard medication. We found that acupuncture significantly increased response rate compared with standard medication (RR 2.03, [95 % CI 1.04–3.97]; P = 0.04) with low heterogeneity (I 2 = 2 %) [23, 24] (Fig. 14)
Fig. 14 
Responder rate between acupuncture and standard medication groups
-
3.
NIH-CPSI pain, urinary, and quality of life domain subscore: Two RCTs involving 137 participants compared acupuncture to standard medication. We found that there were no difference in reducing pain between acupuncture and standard medication (MD −2.47, [95 % CI −5.96 to 1.02]; P = 0.16) with high heterogeneity (I 2 = 93 %) [22, 23] (Fig. 15). But standard medication significantly improved urinary score compared with acupuncture (MD 0.53, [95 % CI 0.15–0.91]; P = 0.006) with low heterogeneity (I 2 = 0 %) [22, 23] (Fig. 16). There was no difference in improving quality of life between acupuncture and standard medication (MD −0.02, [95 % CI −0.60 to 0.55]; P = 0.93) with low heterogeneity (I 2 = 0 %) [22, 23] (Fig. 17).
Fig. 15 
Follow-up pain subscores between acupuncture and standard medication groups
Fig. 16 
Follow-up urinary subscores between acupuncture and standard medication groups
Fig. 17 
Follow-up QOL subscores between acupuncture and standard medication groups





Acupuncture plus standard medication versus standard medication
Only one trial involving 57 participants compared acupuncture plus standard medication to standard medication. Thus, we did not perform meta-analysis.
Laboratory indicators
Laboratory indicators played an important role in CP/CPPS. Six RCTs reported laboratory indicators effect of acupuncture on CP/CPPS (Table 6). Laboratory indicators in these studies include prostaglandin E2, β-endorphin, lecithin body, cortisol, leucine enkephalin, natural killer cell, TNF-α, IL-1β, and plasma substance P. Only TNF-α, IL-1β, and β-endorphin were reported by at least two trials. Three RCTs reported β-endorphin indicator, two of which [19, 24] used different measurement unit, and one trial [16] did not provide raw data, thus we did not perform meta-analysis of β-endorphin.
Two trials involving 136 participants compared acupuncture/acupuncture plus standard medication to standard medication, and were included to meta-analysis of TNF-α and IL-1β in prostatic fluid. The results showed baseline of TNF-α had a significant difference between acupuncture and medication groups (MD −6.93, [95 % CI −12.71 to −1.15]; P = 0.02) with no heterogeneity (I 2 = 0 %) [21, 23] (Fig. 18). Meta-analysis results revealed that there was no significant difference in TNF-α between two groups at the end of follow-up (MD −18.47, [95 % CI −37.76 to 0.81]; P = 0.06) with high heterogeneity (I 2 = 88 %) [21, 23] (Fig. 19). With regard to IL-1β, its baseline showed no significant difference between two groups (MD −2.53, [95 % CI −29.40 to 24.33]; P = 0.85) with low heterogeneity (I 2 = 12 %) [21, 23] (Fig. 20). Meta-analysis revealed there was a significant difference between two groups at the end of follow-up (MD −27.18, [95 % CI −36.30 to −18.06]; P < 0.00001) with moderated heterogeneity (I 2 = 56 %) [21, 23] (Fig. 21).

TNF-alpha level in pre-treatment between acupuncture or acupuncture plus standard medication and standard medication groups

TNF-alpha level in post-treatment between acupuncture or acupuncture plus standard medication and standard medication groups

IL-1beta level in pre-treatment between acupuncture or acupuncture plus standard medication and standard medication groups

IL-1beta level in post-treatment between acupuncture or acupuncture plus standard medication and standard medication groups
Adverse effects rates
Five of ten trials reporting adverse events (ADs) are listed in Table 2. We found no difference between acupuncture and control group in adverse events rate (0.79, [95 % CI 0.40–1.57]; P = 0.50) with low heterogeneity (I 2 = 0 %) [15, 16, 22–24] (Fig. 22). Likewise, there was no difference between acupuncture and standard medication in adverse events rate (0.53, [95 % CI 0.21–1.33]; P = 0.18) with low heterogeneity (I 2 = 0 %) [22–24] (Fig. 23).

Adverse events between acupuncture and control groups

Adverse event between acupuncture and standard medication groups
Publication bias
A test of publication bias was performed using funnel plots method. Results indicated a potential publication bias of the above outcome measure.
Discussion
This study is an updated systemic review/meta-analysis on the efficacy and safety of acupuncture for patients with CP/CPPS. The result of meta-analysis including six trials reveals that compared with sham acupuncture/standard medication, acupuncture can bring better outcomes regarding NIH-CPSI, response rate, pain symptoms, and quality of life for CP/CPPS. It was suggested that acupuncture is a better treatment method for patients with CP/CPPS compared with sham acupuncture/standard medication, especially in aspects of relieving pain symptoms and improving the QOL. But the results show no significant difference on urinary symptoms between acupuncture and the control. The result of response rate was limited because there were different defining standard in these trials. Six-point decrease in NIH-CPSI total score was defined as the responder in two trials [15, 16] and 50 % decrease in NIH-CPSI total score from baseline in two trials [17, 18] was defined (Table 4). Our pooled results showed that acupuncture was superior to sham acupuncture in many aspects including NIH-CPSI, response rate, pain and urinary symptoms, and quality of life. But placebo effects of acupuncture for CP/CPPS cannot be completely eliminated due to specificity of acupuncture. For example, it is hard to execute an exact blinding of participants or personnel. We also found that acupuncture significantly decreased NIH-CPSI total score and increased response rate compared with standard medication, but standard medication was superior to acupuncture in improving urinary symptom, and no difference occurred in reducing pain and improving quality of life. Qin et al. reported that there was no difference in improving urinary symptoms between acupuncture and standard medication [27], which was out of accord with our result. We noted possible causes. Firstly, the drugs used were different in various studies. The review reported by Qin et al. showed that drugs used included levofloxacin, tamsulosin, and ibuprofen used for CP/CPPS; however, our report included tamsulosin and celecoxib. Secondly, assessment criteria were various. The score reduction was used as assessment criteria by Qin et al. and was estimated by using the Cochrane Handbook for Systematic Reviews of Interventions and an imputed correlation coefficient of 0.5 (R¼0.5) according to raw data. The score at end-point of follow-up was adopted in our studies, but one trial adopted the score reductions as assessment measure [18]. The investigators attempted to contact with corresponding author to obtain the raw data once a week (at least three times) and did not get response. So this trial was excluded from pooled analysis. Thirdly, the limited RCTs number and sample size might be associated with the conflicting results.
The theory of traditional Chinese medicine showed acupuncture can stimulate the Qi (energy flow) through meridians. However, the exact mechanism of the beneficial therapeutic effects of acupuncture on CP/CPPS remains unknown [9]. Increasing evidence showed that acupuncture affected laboratory indicators including TNF-α and IL-1β. We found the evidence supported that acupuncture down-regulated IL-1β in prostatic fluid. But pool review showed that there was no difference in TNF-α content between acupuncture/acupuncture plus standard medication and standard medication for CP/CPPS. It may be in contact with the various baselines in TNF-α. Nadler et al. [25] demonstrated that the IL-1β and TNF-α level in prostatic fluid in CP/CPPS are higher than the level in normal people. In addition, the other indicators involving endomorphin-1, β-endorphin, encephalin, and serotonin were reported. Acupuncture increased endomorphin-1, β-endorphin, encephalin, and serotonin contents and had the activities such as analgesia and sedation [8, 19]. In our study, two trials showed acupuncture significantly reduced β-endorphin level, but one trial revealed that acupuncture reduced β-endorphin level without statistical significance [19, 24]. One trial reported that acupuncture significantly reduced prostaglandin E2 level in post-massage urine in patients with CP/CPPS [16]. One trial reveals that acupuncture significantly increased serum NK cell [20].
We searched three systematic review/meta-analysis published in English about acupuncture for CP/CPPS. In January 2012, a systematic review included nine Asian RCTs; the evidence that acupuncture is effective for CP/CPPS is encouraging but not conclusive because of several caveats such as the quantity and quality of the existing evidence [26]. For example, the included trials were published in Chinese except for one trial in English [15], and their quality was low. In January 2016, a systematic review included seven RCTs, of which four were published in English and three in Chinese; this result showed that acupuncture has better efficacy for CP/CPPS than standard medical treatment and may serve as a standard treatment [27]. This review did not perform the meta-analysis on the subscore of NIH-CPSI. We sought all relevant trials and found that one trial [14] was updated by the same author in 2015. In March 2016, a systematic review included seven RCTs (4 published in English, 3 published in Chinese); current evidence supports acupuncture as an effective treatment for CP/CPPS-induced symptoms, particularly in relieving pain [28]. This review is a high-quality meta-analysis, but some high-quality RCTs published in Chinese in recent years did not included. Laboratory indicators were considered as biochemical parameter to evaluate the efficacy of acupuncture for CP/CPPS. Hence, it is necessary to perform a new meta-analysis to re-evaluate efficacy and safety of acupuncture for CP/CPPS.
Limitations
Firstly, many factors including different types of acupuncture, frequency of administration, duration of each session, location of acupoints, manipulation of the needle, experience of manipulators, and the qualities of original studies may potentially impact clinical effects of acupuncture. Secondly, it is difficult to conduct subgroup analysis or Meta regression due to the limitation of trial number and information. Thirdly, it is difficult to implement strictly double-blind trial due to the features of acupuncture.
Conclusion
In summary, the current study indicates that compared with sham acupuncture/standard medication, acupuncture is an effective and safe treatment for CP/CPPS patients, especially in relieving pain symptoms and improving quality of life. Standard medication significantly improved urinary symptoms compared with acupuncture. Acupuncture can decrease the IL-1β in prostatic fluid for CP/CPPS. But it still needs more studies to execute a subgroup analysis of various kinds of acupuncture and medicines.
References
Rees J, Abrahams M, Doble A et al (2015) Diagnosis and treatment of chronic bacterial prostatitis and chronic prostatitis/chronic pelvic pain syndrome: a consensus guideline. BJU Int 116:509–525
Krieger JN, Riley DE, Cheah PY et al (2003) Epidemiology of prostatitis: new evidence for a world-wide problem. World J Urol 21:70–74
Liang CZ, Li HJ, Wang ZP et al (2009) The prevalence of prostatitis-like symptoms in China. J Urol 182:558–563
McNaughton Collins M, MacDonald R, Wilt TJ (2000) Diagnosis and treatment of chronic abacterial prostatitis: a systematic review. Ann Intern Med 133:367–381
Nickel JC, Krieger JN, McNaughton-Collins M et al (2008) Alfuzosin and symptoms of chronic prostatitis–chronic pelvic pain syndrome. N Engl J Med 359:2663–2673
Cohen JM, Fagin AP, Hariton E, Niska JR, Pierce MW et al (2012) Therapeutic intervention for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS): a systematic review and meta-analysis. PLoS One 7(8):e41941
Herati AS, Moldwin RM (2013) Alternative therapies in the management of chronic prostatitis/chronic pelvic pain syndrome. World J Urol 31:761–766
Cabyoglu MT, Ergene N, Tan U (2006) The mechanism of acupuncture and clinical applications. Int J Neurosci 116:115–125
Blanchet KD (2012) Acupuncture: gaining acceptance in urology: proves effective for a number of chronic conditions. BJU Int 109:ii–v
Shamseer L, Moher D, Clarke M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 349:g7647
Litwin MS, McNaughton-Collins M, Fowler FJ et al (1999) The National Institutes of Health chronic prostatitis symptom index: development and validation of a new outcome measure. Chronic Prostatitis Collaborative Research Network. J Urol 162:369–375
Litwin MS (2002) A review of the development and validation of the National Institutes of Health Chronic Prostatitis Symptom Index. Urology 60(6 Suppl):14–18 (discussion 18–19)
Jadad AR, Moore RA, Carroll D et al (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17:1–2
Ma Y, Sun ZX, Men B et al (2014) Efficacy observation on chronic pelvic pain syndrome of damp-heat stagnation pattern treated with acupoint catgut embedding therapy (Chinese). Chin Acupunct Moxib 34:351–355
Lee SW, Liong ML, Yuen KH et al (2008) Acupuncture versus sham acupuncture for chronic prostatitis/chronic pelvic pain. Am J Med 121(79):E1–E7
Lee SH, Lee BC (2009) Electroacupuncture relieves pain in men with chronic prostatitis/chronic pelvic pain syndrome: three-arm randomized trial. Urology 73:1036–1041
Sahin S, Bicer M, Eren GA et al (2015) Acupuncture relieves symptoms in chronic prostatitis/chronic pelvic pain syndrome: a randomized, sham-controlled trial. Prostate Cancer Prostatic Dis 18:249–254
Kucuk EV, Suceken FY, Bindayi A et al (2015) Effectiveness of acupuncture on chronic prostatitis-chronic pelvic pain syndrome category IIIB patients: a prospective, randomized, nonblinded, clinical trial. Urology 85:636–640
Lee SW, Liong ML, Yuen KH et al (2011) Validation of a sham acupuncture procedure in a randomised, controlled clinical trial of chronic pelvic pain treatment. Acupunct Med 29(1):40–46
Lee SW, Liong ML, Yuen KH et al (2014) Acupuncture and immune function in chronic prostatitis/chronic pelvic pain syndrome: a randomized, controlled study. Complement Ther Med 22:965–969
Qi XL, Pan FT, Wu WZ (2012) Effect of acupuncture on cytokine in patients with chronic nonbacterial prostatitis (Chinese). Shandong J Tradit Chin Med 31:418–420
Zhao JY, Song CS (2014) Clinical observation of Jiao Xue acupuncture treatment on IIIB prostatitis (Chinese). Chin J Hum Sex 23:57–59
Li SL, Tang L, Ye HX (2015) Clinical study of “Qing Zhuo Qu Du” Pills combined acupuncture for chronic non-bacterial prostatitis (Chinese). J Guangzhou Univ Tradit Chin Med 06:1035–1039 + 1046
Ma Y, Li XY, Li FQ et al (2015) Clinical study of catgut embedding treatment of male chronic pelvic pain syndrome (Chinese). Chin Acupunct Moxib 06:561–566
Nadler RB, Koch AE, Calhoun EA et al (2000) IL-1beta and TNFalpha in prostatic secretions are indicators in the evaluation of men with chronic prostatitis. J Urol 164(1):214–218
Posadzki P, Zhang J, Lee MS et al (2012) Acupuncture for chronic nonbacterial prostatitis/chronic pelvic pain syndrome: a systematic review. J Androl 33:15–21
Chang S et al (2016) The efficacy of acupuncture in managing patients with chronic prostatitis/chronic pelvic pain syndrome: a systemic review and meta-analysis. Neurourol Urodyn. doi:10.1002/nau.22958
Qin Z et al (2016) Systematic review of acupuncture for chronic prostatitis/chronic pelvic pain syndrome. Medicine 95(11):e3095
Acknowledgments
This work was supported by Guangdong Provincial Science and technology Foundation of China (Grant No. 2010B031600268).
Author contributions
BP Liu, YT Wang, and SD Chen contributed equally to this study; BP Liu contributed to study design, data analysis and interpretation, manuscript drafting and revision, and statistical analysis support; YT Wang contributed to literature search, data acquisition and analysis, and manuscript drafting; SD Chen contributed to data acquisition, methodology assessment of included studies, interpretation, and statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interests exists.
Ethical statement
The present study is a meta-analysis of pooled data and systemic review of published data, the authors did not apply for ethics review committee.
Additional information
Bu-ping Liu, Yun-ting Wang, and Si-da Chen contributed equally to this study.
Rights and permissions
About this article

Cite this article
Liu, Bp., Wang, Yt. & Chen, Sd. Effect of acupuncture on clinical symptoms and laboratory indicators for chronic prostatitis/chronic pelvic pain syndrome: a systematic review and meta-analysis. Int Urol Nephrol 48, 1977–1991 (2016). https://doi.org/10.1007/s11255-016-1403-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-016-1403-z