
Abstract
Objective
To evaluate the outcomes of augmentation cystoplasty in patients with bladder contractures secondary to chronic ketamine abuse.
Method
Patients who had received augmentation cystoplasty to treat ketamine-related bladder contractures in two hospitals in our region were reviewed retrospectively. Their history of ketamine consumption, presenting symptoms, history of treatment, surgical information and post-operative conditions were retrieved from clinical records and then summarized.
Results
Between 2006 and 2011, four patients (three women and one man), aged 21–30 years (mean 27 years), underwent augmentation cystoplasty for ketamine-related bladder contractures. The duration of ketamine consumption ranged from 3 to 15 years, and all four patients resumed ketamine consumption after surgery. The mean maximal baseline and post-operative bladder capacity was 37.5 cc (range 25–50 cc) and up to 400–500 cc, respectively. Three patients experienced a further deterioration in renal function that was secondary to new-onset ureteral strictures in two cases and to sepsis in the other. At the time of the last follow-up, three patients could void spontaneously and one required regular intermittent catheterization.
Conclusion
Ketamine cystitis is an emerging medical condition that requires a multi-disciplinary approach to manage the patients. Simple surgical management of the physical component of the contracted bladder may produce only suboptimal results, and could even cause further problems in some patients. The importance of compliance with post-operative care and abstinence from drug use should be stressed to the patients before surgery. In view of the high complication rate, the option of a simple ileal conduit should also be discussed prior to surgical intervention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The recreational use of ketamine was first reported in North America in 1971, and has become increasingly common in the past 20 years [1]. While this is a worldwide phenomenon, it is especially popular in South-East Asia and in particular among young adults [2]. In Hong Kong, almost 60 % of substance abusers below the age of 21 years were found to be using ketamine [2]. The consumption rate in young adults was also increased from 0.8 in 2007/8 to 2.1 % in 2010/11 in the United Kingdom [3], where more than 30 % of 3,806 participants in a web-based survey reported ketamine use [4]. The most common route of use is nasal (snorting). Among the undesirable long-term adverse effects related to chronic ketamine use [5], voiding dysfunction is an increasingly recognized medical condition that has generated serious health care concerns. First reported in 2007, the typical symptoms of ketamine-related voiding dysfunction include irritative lower urinary symptoms, dysuria and pelvic pain [6, 7]. In its late and severe form, patients typically develop a severely contracted bladder and upper tract dilatations, with intractable symptoms and renal impairment. To date, a few hundred cases have been reported, especially in the United Kingdom, Hong Kong and Taiwan [3]. The prevalence of lower urinary tract symptoms in ketamine users was reported to be more than 25 % in a series in the United Kingdom [4]. The main line of therapy is drug detoxification and symptomatic treatment, including behavior therapy and medication such as antimuscarinic agents, non-steroidal anti-inflammatory agents and intravesical hyaluranic acid [8]. However, in patients who have severely contracted bladders, augmentation cystoplasty is considered to be a sustainable option to improve their symptoms and maintain their renal function. We report here on our experience of augmentation cystoplasty in four patients, to illustrate the complexities associated with their management.
Patients and methods
Patients who had received augmentation cystoplasty to treat ketamine-related bladder contractures in two hospitals in our region were reviewed retrospectively. Both centers had more than 10 years of experience in performing bladder reconstruction/cystoplasty, with more than 10 operations carried out every year. The history of ketamine consumption, presenting symptoms, history of treatment, surgical information and post-operative conditions of the patients were retrieved from clinical records and then summarized. The glomerular filtration rate (GFR) was calculated by the Modification of Diet in Renal Disease Study Group formula [9].
Results
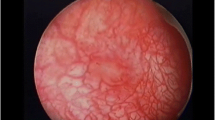
Between 2006 and 2011, four patients (three women and one man) aged 21–30 years (mean 27 years) underwent augmentation cystoplasty for ketamine-related bladder contractures. The duration of ketamine consumption ranged from 3 to 15 years, and the mean duration of symptoms prior to surgery was 37.3 months (range 8–56 months). All of the patients presented with marked irritative urinary symptoms, including frequency, nocturia and urgency. One patient also had severe pelvic pain and dysuria. All patients had taken courses of anti-inflammatory agents, antimuscarinic agents and analgesics, with no significant clinical improvement. Pre-operative urodynamic studies showed marked detrusor overactivity in all patients. The mean maximal bladder capacity was 37.5 cc (range 25–50 cc). Bilateral vesicoureteral reflux was demonstrated in one patient (Patient 1). Cystoscopy was performed on three patients, all of whom showed marked erythematous mucosa; a bladder biopsy performed on two patients confirmed cystitis-type changes only. All of the patients showed hydronephrosis by ultrasound, which was bilateral in two cases and exclusively on the left side in the other two. Additional investigations showed no ureteral obstruction in any of the patients. Pre-operative creatinine levels were normal (59–72 mmol/L) in the three female patients. Patient 1 had an elevated serum creatinine level (around 160 mmol/L), with a creatinine clearance of 61 mL/min before surgery. Two patients (Patients 2 and 3) claimed to have stopped ketamine use prior to surgery (Table 1).
In view of the severely contracted bladders and intractable symptoms, augmentation cystoplasty was decided for all patients after discussion. The operations were performed using an open approach in two of the patients and a robot-assisted laparoscopic approach in the other two. Augmentation cystoplasty using the ‘clam technique’ was performed with a 30–40-cm section of the ileum. Both the ileo-ileal anastomosis and the augmentation were performed by suture, either manually or using robot-assisted laparoscopy. The mean operation time was 216.4 min (range 175–270 min) with no significant blood loss. The post-operative period was unremarkable in all of the cases. A cystogram was performed to confirm that there was no leakage prior to the removal of the urethral catheter on Day 7 to Day 14. Two patients required clean intermittent catheterization (Patients 1 and 4) after surgery, while the other two were able to void by straining, with satisfactory bladder emptying. Their serum creatinine remained stable with no sign of metabolic acidosis during the initial post-operative period.
Unfortunately, all four patients resumed ketamine consumption after surgery, and all of them defaulted from follow-up at some stage in their treatment. The mean post-operative follow-up time was 35.3 months (range 9–76 months). Three patients had experienced further deteriorations in their condition and renal function, while the remaining patient was lost to follow-up 9 months after surgery (Table 2). A brief summary of the post-operative course is given in Table 2. Some unexpected findings were observed in these patients: two developed ureteral strictures (Patients 1 and 2) after surgery, which may have contributed to the renal impairment [serum creatinine levels: Patient 1—raised from a post-operative level of 173 mmol/L (GFR = 43 mL/min/1.73 m2) to 1,067 mmol/L (GFR = 5 mL/min/1.73 m2) and Patient 2—raised from a post-operative level of 83 mmol/L (GFR = 81 mL/min/1.73 m2) to 145 mmol/L (GFR = 42 mL/min/1.73 m2)]. Patient 1 underwent surgery and his serum creatinine level improved to 350 mmol/L (GFR = 19 mL/min/1.73 m2; Table 1). Unfortunately, Patient 2 refused ureteral stenting and defaulted from follow-up. However, the capacity of the ileocystoplasty was relatively well maintained in our patients. For Patients 1 and 2, who had a longer follow-up, bladder capacity was maintained at around 450–500 cc, with no clinical evidence of contractures of the augmented bladder (intestinal) wall.
Discussion
Ketamine cystitis, first reported in 2007, has become an increasingly important urological condition [6, 7], the characteristic features of which include severe irritative voiding symptoms associated with dysuria or pelvic pain. In acute cases, patients may develop a severely contracted bladder, hydronephrosis and renal impairment [10]. In earlier and less severe cases, the symptoms may improve after ketamine abstinence and medical therapy. However, in late cases that involve a severely contracted and fibrotic bladder, the symptoms do not respond to conservative management. Augmentation cystoplasty may need to be considered to improve the capacity and compliance of the bladder and to avoid further damage to the upper tract.
Augmentation cystoplasty is a classical and effective surgical treatment for the management of small contracted bladders, with poor compliance and/or detrusor overactivity [11]. The main indications include neurogenic or non-neurogenic bladder dysfunction that does not respond to conservative management, congenital bladder abnormalities and infective and inflammatory disorders. The procedure involves creating a wider bladder opening (‘clam’ technique) and then applying an isolated segment of the intestinal tract to the free edge of the bladder to increase the capacity [12]. Reconstruction is most commonly carried out using a 25–40-cm segment of the ileum from the ileocecal valve. While the beneficial effect of ileocystoplasty has been well documented, it may also lead to some serious complications [11]. The possibilities of metabolic disturbances and renal impairment related to the reabsorption of urinary constituents by the ileum require close monitoring of the patients, particularly during the initial phase after surgery.
The presentation of a ketamine-related bladder contracture is similar to that of some other inflammatory processes, such as post-tuberculosis and post-irradiation symptoms, which suggests that it should be a good candidate for the application of augmentation cystoplasty. However, the outcomes of our patients were not as satisfactory as we would have expected from the literature [13]. Three of the four patients experienced a deterioration of renal function and other severe complications after the surgery, which is a much higher incidence than that reported in the literature [13]. Augmentation cystoplasty would therefore appear to be unsuitable in these patients.
We believe that at least two factors, the disease and the patient, contributed to the poor outcomes observed in our series. Although two patients had stopped using ketamine before surgery, all four resumed ketamine abuse thereafter. Therefore, compared with post-tuberculosis or post-irradiation bladder contractures, the disease process in our patients was not yet stable and may even have been progressing, which might account for the development of ureteral strictures in two of the patients (Patients 1 and 2), after surgery, the reasons for which are not understood. All patients had pre-operative hydronephrosis, but investigations (including either an intravenous urogram or an antegrade pyelogram) showed no ureteral obstruction. Only Patient 1 underwent a micturation cystogram, which demonstrated bilateral ureteral reflux. Therefore, the pre-operative diagnosis of hydronephrosis in these patients was due to vesicoureteral reflux secondary to the contracted bladder. Moreover, as only augmentation cystoplasty was performed in these patients, the ureters were not mobilized during the operations, and the likelihood of iatrogenic ureteral injury during surgery was therefore lessened. No evidence of retroperitoneal fibrosis was found in Patient 1 during surgery, only a short segment stricture at L2/3. The final pathology of the ureteral stricture showed an intense transmural inflammatory response and fibrosis, with no other anomaly. Therefore, the exact cause of the ureteral stricture was still unknown. However, one of the postulated reasons was the recirculation of ketamine and its metabolites, which lead to higher levels of ketamine in the urine and cause chemical irritation to the urothelium [10]. Ketamine and its metabolites are excreted in urine after metabolism [14, 15], and they could be reabsorbed by the ileum, resulting in recirculation in the body, which might lead to prolonged exposure of the urothelium to ketamine and subsequent stricture formation. In contrast, we did not observe any obvious contracture in the ileal segments of the augmentations in our series, which might suggest that they were more resistant to the effects of ketamine. Oral ketamine is a recognized treatment option for patients with chronic pain [16], and the observed incidence of its gastrointestinal tract side-effects is not high. However, the duration of ketamine use in most of these patients is shorter than that in our ketamine abusers. Because the deterioration in renal function occurred after the resumption of ketamine use and the function of the augmented bladder remained satisfactory at the time of reporting, we believed that this degeneration of renal function was probably related to the resumption of ketamine use and also to the development of ureteral strictures in these patients.
The excellent review by Greenwell et al. [17] clearly pointed out the importance of patient selection and counseling before surgery. The authors recommended that augmentation cystoplasty should ideally be offered only to cooperative and motivated patients with a full understanding of the procedure and its consequences, who should also be willing to comply with clean intermittent catheterization and lifelong surveillance. Unfortunately, due to the underlying psychological problems and poor social support among substance abusers, there is a high risk of treatment non-compliance [18–20]. These characteristics probably account for the poor compliance with clean intermittent catheterization and follow-up of our patients, which led to a further deterioration in their conditions. As a result, augmentation may even be harmful to patients with poor compliance. Therefore, psychiatric and social interventions, including detoxification programs, should be offered to all such patients before any surgical intervention.
Alternatively, incontinence-type diversion, such as an ileal conduit, may be an alternative means to manage these patients with bladder dysfunction. The advantages of incontinence diversion over bladder augmentation include a faster recovery, the eradication of the need for intermittent catheterization and the relatively fewer metabolic complications. However, the necessity of the lifelong use of an external collecting bag may not be acceptable to these relatively young patients.
In conclusion, ketamine cystitis is an emerging medical condition that demands greater medical and public awareness and support. The complexity of its management is related not only to the diverse symptoms and the possibility of irreversible damage to the urinary tract, but also to the underlying psychosocial co-morbidities of the patients. Simple management of the physical component of the condition may produce only suboptimal results and could even cause further problems in some patients. Therefore, a multi-disciplinary approach that includes clinicians, psychiatrists and social workers would be beneficial to the management of these patients.
References
Kalsi SS, Wood DM, Dargan PI (2011) The epidemiology and patterns of acute and chronic toxicity associated with recreational ketamine use. Emerg Health Threats J 4:7107–7116
Wolff K (2012) Ketamine. In: Verster JC et al (eds) Drug abuse and addiction in medical illness: causes, consequences and treatment. Springer, New York, pp 201–211
Froster JA, Harrison SCW (2012) Ketamine uropathy: rising to the challenges of a new condition. BJU Int 109:1277–1278
Winstock AR, Mitcheson L, Gillatt DA, Cottrell AM (2012) The prevalence and natural history of urinary symptoms among recreational ketamine users. BJU Int 110:1762–1766
Lin M (2004) The underappreciated dangers of “club drugs”: what clinicians need to know. Adv Stud Med 4:191–198
Shahani R, Streutker C, Dickson B, Stewart RJ (2007) Ketamine-associated ulcerative cystitis: a new clinical entity. Urology 69:810–812
Chu PS, Kwok SC, Lam KM, Chu TY, Chan SW, Man CW, Ma WK, Chui KL, Yiu MK, Chan YC, Tse ML, Lau FL (2007) ‘Street ketamine’-associated bladder dysfunction: a report of ten cases. Hong Kong Med J 13:311–313
Middela S, Pearce I (2011) Ketamine-induced vesiculopathy: a literature review. Int J Clin Pract 65:27–30
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 130:461–470
Chu PS, Ma WK, Wong SC, Chu RW, Cheng CH, Wong S, Tse JML, Lau FL, Yiu MK, Man CW (2008) The destruction of the lower urinary tract by ketamine abuse: a new syndrome? BJU Int 102:1616–1622
Biers SM, Venn SN, Greenwell TJ (2012) The past, present and future of augmentation cystoplasty. BJU Int 109:1280–1293
Stein R, Schröder A, Thüroff JW (2012) Bladder augmentation and urinary diversion in patients with neurogenic bladder: surgical considerations. J Pediatr Urol 8:153–161
Stein R, Kamal MM, Rubenwolf P, Ziesel C, Schröder A, Thüroff JW (2012) Bladder augmentation using bowel segments (enterocystoplasty). BJU Int 110:1078–1094
Craven R (2007) Ketamine. Anaesthesia 62(Suppl 1):48–53
Adamowicz P, Kala M (2005) Urinary excretion rates of ketamine and norketamine following therapeutic ketamine administration: method and detection window considerations. J Anal Toxicol 29:376–382
Blonk MI, Koder BG, van den Bemt PM, Huygen FJ (2010) Use of oral ketamine in chronic pain management: a review. Eur J Pain 14:466–472
Greenwell TJ, Venn SN, Mundy AR (2001) Augmentation cystoplasty. BJU Int 88:511–525
DiMatteo MR, Lepper HS, Croghan TW (2000) Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med 160:2101–2107
Tabor PA, Lopez DA (2004) Comply with us: improving medication adherence. J Pharm Pract 17:167–180
Lucas GM (2011) Substance abuse, adherence with antiretroviral therapy, and clinical outcomes among HIV-infected individuals. Life Sci 88:948–952
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ng, CF., Chiu, P.K.F., Li, ML. et al. Clinical outcomes of augmentation cystoplasty in patients suffering from ketamine-related bladder contractures. Int Urol Nephrol 45, 1245–1251 (2013). https://doi.org/10.1007/s11255-013-0501-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-013-0501-4