
Abstract
Background and objective
Patients’ beliefs regarding their health are important to understand responses to chronic disease. The present study aimed to determine (i) whether beliefs about health differ between different renal replacement therapies in end-stage renal disease (ESRD) patients and (ii) whether these beliefs are associated with health-related quality of life (HQoL), as well as with mental health.
Methods
A sample of 89 ESRD patients, 41 on hemodialysis (HD) treatment and 48 on peritoneal dialysis (PD) treatment, completed the World Health Organization Quality of Life instrument, the General Health Questionnaire, the State-Trait Anxiety Inventory, the Center for Epidemiologic Studies Depression Scale, and the Multidimensional Health Locus of Control.
Results
Regarding differences in health beliefs between the two groups, HD patients focused more on the dimension of internal health locus of control than PD patients. This dimension was associated with better QoL (P = <0.01) and general health (P = 0.03) in the total sample. On the contrary, the dimension of important others in health locus of control was associated with higher depression (P = 0.02).
Conclusions
The beliefs that dialysis patients hold about their illness appear to be related to the type of renal replacement therapy. These cognitions are associated with HQoL and with mental health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
End-stage renal disease (ESRD) patients have a high burden of disease (particularly cardiovascular comorbidities) affecting their quality of life (QoL) and dramatically shortening their life expectancy [1–3]. Therefore, exploring QoL becomes an essential task in the management of this population.
These patients may be faced with serious stressors related to the illness and its treatment, arising from the chronic nature of ESRD and the intrusiveness of the medical treatment [4–10]. They are often confronted with limitations in food and fluid intake, with physical symptoms such as itching and lack of energy, with psychological stressors such as loss of self-concept and self-esteem, feelings of uncertainty about the future, feelings of guilt toward family members, and with problems in the social domain [11–14].
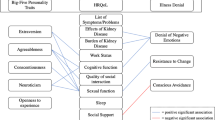
Recent studies in chronic diseases suggest that QoL and mental health may be related to patient’s cognitive representations of illness and treatment. When confronted with an illness, people create their own models and representations of the illness in order to make sense of and respond to the problems they are faced with [15–20].
Regarding health beliefs, it has recently been recognized that hemodialysis (HD) patients’ belief that one’s health is controllable was associated with less depression [21]. Further, after controlling for baseline level of depression, baseline internal health locus of control was not a significant predictor of depression in ESRD patients at follow-up [22].
In other studies, personal control was significantly and positively related to physical and social functioning, bodily pain, general health perception, and the physical component score in HD and peritoneal dialysis (PD) patients [4]. A higher personal control was also associated with a lower emotional response and a better understanding of the renal disease [13].
Finally, it has been indicated that better health-related quality of life (HQoL) in dialysis patients is associated with higher control beliefs, lower illness and treatment disruptiveness, lower consequences, and less symptoms [23].
The purpose of this study is to examine health beliefs in ESRD patients and their relation to QoL and mental health. We mainly hypothesize that a stronger internal health locus of control is associated with better QoL and mental health, indicating less symptoms of depression and anxiety.
Materials and methods
Study design
This study consists of two main parts. The first investigates the effect of duration of treatment on QoL and mental health of HD and PD patients. For this purpose, a cohort of 135 ESRD patients were recruited from dialysis units in three General Hospitals located within the broader area of Athens and consisted of: (a) 77 patients (57.0%) undergoing in-center hemodialysis (HD) and (b) 58 patients (43.0%) undergoing continuous ambulatory peritoneal dialysis (CAPD/PD). Patients on these two treatment modalities had low comorbidity and were undergoing current dialysis for a varied period of time. In this respect, participants could be categorized into four distinct groups regarding current treatment: (a) HD patients who recently commenced treatment (<4 years), (b) HD patients on long-term treatment (>4 years), (c) PD patients who recently commenced treatment (<4 years), and (d) PD patients on long-term treatment (>4 years).
Next, in order to investigate differences between the HD and PD treatment modalities, independently of treatment duration, 41 HD and 48 PD patients were selected from the total cohort of 135 participants, according to specified criteria to form two matched groups (see Fig. 1 sample selection flowchart).

Sample selection flowchart
Selection criteria included patients commencing dialysis treatment within a 4-year period and ensured a balanced ratio of men/women participants among the two groups. Following the selection procedure, the two groups were tested for significant differences regarding sociodemographic variables. As seen in Table 1, the groups can be considered equivalent, with no statistically significant differences between them (P > 0.05).
All subjects were informed of their rights to refuse or discontinue participation in the study, according to the ethical standards of the 1983 Helsinki Declaration. Ethical permission for the study was obtained from the scientific committees of the hospitals.
Measurements
The measurement tools included:
-
1)
The World Health Organization Quality of Life instrument (WHOQOL–BREF) [24] is a self-report generic QoL inventory of 26 items, validated for Greek populations [25]. The items fall into 4 domains: (a) physical health, (b) psychological well-being, (c) social relationships, and (d) environment. Two of the items provide a facet measuring overall QoL/health. Higher scores indicate a better QoL.
-
2)
The General Health Questionnaire (GHQ-28) is a widely used self-report measure of general health, developed by Goldberg in 1978 [26], and validated for Greek populations [27]. It may identify short-term changes in mental health and is often used as a screening instrument for psychiatric cases in medical setting and general practice. The 28-item version used in this study consists of four sub-scales: (a) somatic symptoms, (b) anxiety/insomnia, (c) social dysfunction, and (d) severe depression. Higher scores indicate a worse general health status.
-
3)
The State-Trait Anxiety Inνentory (STAI 1/STAI 2) consists of 20 items referring to self-reported state anxiety and 20 items referring to trait anxiety [28, 29]. State anxiety reflects a “transitory emotional state or condition of the human organism that is characterized by subjective, consciously perceived feelings of tension and apprehension, and heightened autonomic nervous system activity”; it may fluctuate over time and can vary in intensity. In contrast, trait anxiety denotes “relatively stable individual differences in anxiety proneness” and refers to a general tendency to respond with anxiety to perceived threats in the environment [28]. Higher scores mean that patients are more anxious.
-
4)
The Center for Epidemiologic Studies Depression Scale (CES-D) [30–32] is a 20-item self-report measure of depression. A higher score means that the patient is more depressed. A value above 18 is required for a subject to be classified as depressed [32].
-
5)
The Multidimensional Health Locus of Control (MHLC) is a self-report tool measuring a patient’s beliefs about control over health outcomes. Health locus of control is one of the widely used measures of individuals’ health beliefs and has been designed to determine whether patients are internalists or externalists. The inventory consists of 18 items, which comprise 4 categories of beliefs: (a) internal locus, (b) chance, (c) doctors, and (d) important others. The last three refer to external locus of control [33, 34]. The brief description of the theory explores the fact that health locus of control is a degree to which individuals believe that their health is controlled by internal or external factors. Whether a person is external or internal is based on a series of statements. The statements are scored and summed to find the above. Externals refer to belief that one’s outcome is under the control of powerful others (i.e., doctors) or is determined by fate, luck, or chance. Internals refer to the belief that one’s outcome is directly the result of one’s behavior [33, 34]. The 4 categories are not mutually exclusive, and scores may weight in a particular direction. Higher scores indicate stronger presence of the specific dimension of beliefs.
Statistical methods
Kolmogorov–Smirnov tests were performed in order to check whether the values of the sample would fall within a normal distribution. Next, the analyses performed were aimed to:
-
a)
investigate differences between HD and PD patients, using two groups comprised of selected cases from the total cohort of 135 patients, equivalent for length of treatment and sociodemographic characteristics. Independent sample t-test was performed in order to check for significant differences in the variable of health locus of control examined in the study. Further, stepwise regression analysis was used to assess that the association between internal health beliefs and renal replacement modality is independent from depressive symptoms. A model was constructed using renal replacement modality as dependent variable. Independent variables included depression (CES-D) and internal health locus of control. A P value of 0.05 or less was considered to indicate statistical significance.
-
b)
investigate the relation between health beliefs and QoL as well as mental health. Thus, correlation analysis was performed using Pearson’s rho. Multiple stepwise regression analysis was also used to assess that the association between internal health beliefs and overall QoL/health is independent from depression. Initially, simple correlations were examined between variables referring to health beliefs, QoL as well as mental health (depression, state-trait anxiety, and general health) in the total sample of ESRD patients. Correlation analysis was also performed in order to investigate the above relation in the groups of HD and PD patients separately. As some of these variables were not significantly related to overall QoL/health, they were excluded as predictors from the final regression analysis. A model was constructed using overall QoL/health facet as dependent variable. Independent variables included these domains of WHOQOL-BREF, which were correlated to overall QoL/health, sub-scales of GHQ-28, depression (CES-D), state-trait anxiety (STAI 1/STAI 2), and internal health locus of control. A P value of 0.05 or less was considered to indicate statistical significance.
All analyses were performed with the Statistical Package for the Social Sciences (SPSS 13.0 for Windows).
Results
The values of the total cohort were found to pass the normality distribution test. With regard to illness beliefs, a significant difference was observed in HD patients presenting higher scores in the dimension of internal health locus of control, compared to PD patients. Both groups presented a similar pattern of illness beliefs, according to which higher values were identified in the internal and chance dimensions followed by the dimensions of doctors and important others (Table 2). A stepwise regression analysis was also performed (Table 3). Only internal health beliefs proved to be significantly associated with renal replacement modality.
Investigating the relation between the dimensions of health locus of control and QoL as well as mental health in the total sample, internal health locus of control was associated positively with QoL and more specifically with the domain of psychological health (r = 0.35, P = <0.01) and the overall QoL/health facet (r = 0.48, P = <0.01). Internal health beliefs were also related negatively to general health, measured by GHQ-28 questionnaire, and more specifically to the sub-scale of somatic symptoms (r = −0.22, P = 0.03). On the other hand, the dimension of important others appeared to have positive correlation with depression, measured by CES-D scale (r = 0.28, P = 0.02) (Table 4).
A multiple stepwise regression analysis was also performed (Table 5). Only psychological health proved to be significantly associated with overall QoL/health facet of our patients as well as internal health beliefs.
Further investigation was performed in the two groups of patients, separately. In HD patients, internal health locus of control was associated positively with QoL, especially with the domains of physical (r = 0.37, P = 0.01) and psychological health (r = 0.48, P = <0.01), as well as the overall QoL/health facet (r = 0.59, P = <0.01). Also, internal health beliefs were related negatively to general health and more specifically to the sub-scales of somatic symptoms (r = −0.34, P = 0.02), social dysfunction (r = −0.31, P = 0.04), and severe depression (r = −0.33, P = 0.03) as well as the total score of GHQ-28 (r = −0.37, P = 0.01) in HD patients. Furthermore, we found that internal health locus of control had negative connection with state anxiety (r = −0.49, P = 0.04) (Table 6).
A multiple stepwise regression analysis was also performed in the group of HD patients (Table 7). Only psychological health proved to be significantly associated with overall QoL/health facet.
With regard to PD patients, the results showed a positive relation between the overall QoL/health facet and the internal health locus of control (r = 0.45, P = <0.01). However, the dimension of important others appeared to have negative correlation with the domain of psychological health, measured by WHOQOL-BREF (r = −0.31, P = 0.03). This dimension was also related positively to the GHQ-28 sub-scale of anxiety/insomnia (r = 0.32, P = 0.02), the total score of GHQ-28 (r = 0.31, P = 0.03) as well as to depression, measured by CES-D scale (r = 0.41, P = <0.01) (Table 8).
A multiple stepwise regression analysis was also performed in the group of PD patients (Table 9). Only psychological health proved to be significantly associated with overall QoL/health facet as well as internal health beliefs.
Discussion
The present study examined the nature of illness cognitions in ESRD patients on different types of renal replacement therapy and their associations with QoL and mental health.
Regarding health beliefs, HD patients indicated a greater preference to the internal dimension, focusing more on their own personal control to regulate their health condition. This may reflect a stronger need of these patients to counterbalance the imposed dependence on the dialysis procedure and the restrictive dietary regimen by exercising control over their illness. Further investigation into this hypothesis is necessary.
Concerning the relation between the dimensions of health locus of control and QoL in the total sample, it seems that internal health beliefs may help the patients to face their problems related to ESRD and evaluate in a positive way their QoL and the status of general health, showing better psychological health and less somatic symptoms. These results correspond to previous findings that internal health locus of control is associated with better QoL and understanding of patients’ illness [13]. On the other hand, focusing on important others’ control and responsibility over one’s condition seems to indicate depressive mood. ESRD patients are reported in the relevant literature to present depressive symptomatology [35–41].
In further investigation that was performed in the two groups of patients separately, the above conclusions are confirmed. Specifically, in HD patients, internal health locus of control contributes to a positive perception of their QoL, indicating better physical and psychological health as well as overall QoL/health. Also, internal health beliefs help HD patients to evaluate more favorably not only their status of general health with less somatic symptoms, social dysfunction, and severe depression but also their mental health showing less state anxiety. In the relevant literature, it has been suggested that personal control is significantly and positively related to physical and social functioning and general health perception in these patients [4, 42–44].
As far as PD patients are concerned, internal health locus of control relates to a positive cognition regarding overall QoL/health. However, the dimension of important others leads to a negative evaluation of QoL and mental health, indicating more depressive symptoms, anxiety, and insomnia.
Further, it is important to point out that psychological health seems to play a substantial role in patients’ QoL and more specifically in the favorable way that HD and PD patients evaluate the level of their overall QoL and health.
Limitations of the study may include the lack of investigating the effect of clinical factors, such as adequacy of dialysis, hemoglobin level, dialysis vintage, presence of diabetes mellitus, or other clinical parameters on the patients’ perceptions of QoL and mental health. There is also a need for future research to use prospective and longitudinal study designs to examine the interaction of illness and treatment cognitions and outcomes and how these change over time, during the course of the illness.
Another methodological issue is related to the sample representativeness. Studies on the broader ESRD population and recruiting even larger samples to enable effective multi-group analysis should be pursued in future research.
Finally, regarding limitations of the study, it is important to say that STAI 1/STAI 2, CES-D, and MHLC questionnaires are not validated in Greek ESRD population, thus not informing about the sensitivity and the internal consistency of these measurements. Future studies are needed, using the above methods in patients with ESRD, in order to make generalized conclusions on mental health and health beliefs of this population.
Despite its limitations, the present study demonstrates the importance of understanding the illness and treatment beliefs of patients with ESRD and the contribution of these beliefs to HQoL. This suggests the interest for investigating whether individually-based or group-based interventions that are aimed at specific, inaccurate, individual illness perceptions can improve perceived QoL in dialysis patients.
References
Covic A, Seica A, Mardare N, Gusbeth-Tatomir P (2006) A longitudinal study on changes in quality of life and illness representations in long-term hemodialysis patients with low comorbidity. Dialysis Mædica-J Clin Med 1:12–19
Covic A, Gusbeth-Tatomir P, Goldsmith DJ (2003) The challenge of cardiovascular risk factors in end-stage renal disease. J Nephrol 16:476–486
Theofilou P, Ginieri-Coccossis M, Synodinou C (2010) Sociodemographic variables, health beliefs, psychopathological symptoms: influence factors of quality of life in patients with chronic renal failure. In: Koulierakis G, Pashali A, Rotsika V, Ginieri-Coccossis M (eds) Clinical psychology and health psychology-research and practice. Papazisi, Athens (in Greek)
Timmers L, Thong SY M, Dekker WF, Boeschoten WE, Heijmans M, Rijken M, Weinman J, Kaptein AA (2008) Illness perceptions in dialysis patients and their association with quality of life. Psychol Health 23:679–690
Ginieri-Coccossis M, Theofilou P, Synodinou C, Tomaras V, Soldatos C (2008) Quality of life, mental health and health beliefs in hemodialysis and peritoneal dialysis patients: investigating differences in early and later years of current treatment. BMC Nephrol 9:1–9
Karamanidou C, Theofilou P, Ginieri-Coccossis M, Synodinou C, Papadimitriou G (2009) Anxiety, depression and health beliefs in end-stage renal disease (ESRD) patients. Paper presented at the 17th European congress of psychiatry, Lisbon, Portugal, 24–28 January 2009
Theofilou P (2011) The role of sociodemographic factors in health-related quality of life of patients with end-stage renal disease. Int J Caring Sci 4:40–50
Theofilou P (2010) Psychiatric disorders in chronic periodical hemodialysis. Vima Asklipiou 9:420–440 (in Greek)
Theofilou P, Panagiotaki E (2010) Factors affecting quality of life in patients with end-stage renal disease. Nursing 49:174–181 (in Greek)
Theofilou P (2010) Quality of life, mental health and health beliefs: comparison between haemodialysis and peritoneal dialysis patients. Interscientific Health Care 2:171–176 (in Greek)
Cameron S (1996) Kidney failure. Oxford University Press, New York
Christensen AJ, Ehlers SL (2002) Psychological factors in end-stage renal disease: an emerging context for behavioral medicine research. J Consult Clin Psychol 70:712–724
Covic A, Seica A, Gusbeth-Tatomir P, Gavrilovici O, Goldsmith DJ (2004) Illness representations and quality of life scores in haemodialysis patients. Nephrol Dial Transplant 19:2078–2083
Krespi R, Bone M, Ahmad R, Worthington B, Salmon P (2004) Haemodialysis patients’ beliefs about renal failure and its treatment. Patient Educ Couns 53:189–196
Cameron LD, Leventhal H (2003) The self-regulation of health and illness behaviour. Routledge, London
Cameron LD, Moss-Morris R (2004) Illness-related cognition and behavior. In: Kaptein A, Weinman J (eds) Health psychology. Blackwell Publishing and British Psychological Society, Oxford
Caress AL, Luker KA, Owens RG (2001) A descriptive study of meaning of illness in chronic renal disease. J Adv Nurs 33:716–727
Hagger MS, Orbell S (2003) A meta-analytic review of the common-sense model of illness representations. Psychol Health 18:141–184
Heijmans M, de Ridder D (1998) Assessing illness representations of chronic illness: explorations of their disease-specific nature. J Behav Med 21:485–503
Rees G, Fry A, Cull A, Sutton S (2004) Illness perceptions and distress in women at increased risk of breast cancer. Psychol Health 19:749–765
Christensen AJ, Turner CW, Smith TW, Holman JM, Gregory MC (1991) Health locus of control and depression in end-stage renal disease. J Consult Clin Psychol 59:419–424
Cvengros JA, Christensen AJ, Lawton WJ (2005) Health locus of control and depression in chronic kidney disease: a dynamic perspective. J Health Psychol 10:677–686
Griva K, Jayasena D, Davenport A, Harrison M, Newman PS (2009) Illness and treatment cognitions and health related quality of life in end stage renal disease. Br J Health Psychol 14:17–34
WHOQOL Group (2004) The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL Group. Quality of Life Research 13: 299–310
Ginieri-Coccossis M, Triantafillou E, Antonopoulou V, Tomaras V, Christodoulou GN (2003) Quality of Life Handbook in reference to WHOQOL-100. Medical Publications VIΤΑ, Athens (in Greek)
Goldberg DΡ (1978) Manual of the general health questionnaire. NFER-Nelson, Windsor, England
Garyfallos G, Karastergiou Α, Adamopoulou Α, Moutzoukis C, Alagiozidoy E, Mala Ο (1991) Greek version of the general health questionnaire: accuracy of translation and validity. Acta Psychiatr Scand 84:371–378
Spielberger GΟ (1970) The state-trait anxiety inventory. Consulting Psychologists Press, California
Liakos A, Giannitsi S (1984) Reliability and validity of the greek state-trait anxiety inventory of spielberger. Egephalos 21:71–76 (in Greek)
Radloff LS (1977) The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1:385–401
Hann D, Winter K, Jacobsen P (1999) Measurement of depressive symptoms in cancer patients: evaluation of the center for epidemiological studies depression scale (CES-D). J Psychosom Res 46:437–443
Hedayati S, Bosworth H, Kuchibhatla M, Kimmel P, Szczech L (2006) The predictive value of self-report scales compared with physician diagnosis of depression in haemodialysis patients. Kidney Int 69:1662–1668
Wallston BS, Wallston KA (1976) The development and validation of the health related locus of control (HLC) scale. J Consult Clin Psychol 44:580–585
Wallston BS, Wallston KA, DeVellis R (1978) Development of the multidimensional health locus of control (MHLC) scale. Health Educ Monogr 6:160–170
Arnold R, Ranchor AV, Sanderman R, Kempen GIJM, Ormel J, Suurmeijer TPBM (2004) The relative contribution of domains of quality of life to overall quality of life for different chronic diseases. Qual Life Res 13:883–896
Oikonomidou G, Zlatanos D, Vayopoulos H, Hatzidimitriou H (2005) Depression in patients with chronic renal failure. Dialys Living 14:22–32 (in Greek)
Yucedal C, Olmez Ν, Gezen G, Celik F, Altindag Α, Yilmaz ME, Kara IH (2003) Depression in dialysis patients. EDTNA ERCA J 29:160–164 (in Greek)
Oo TN, Roberts TL, Colling AJ (2005) A comparison of peritonitis rates from the United States Renal Data System data-base: CAPD versus continuous cycling peritoneal dialysis patients. Am J Kidney Dis 45:372–380
Theofilou P (2011) Depression and anxiety in patients with chronic renal failure: the effect of sociodemographic characteristics. International Journal of Nephrology (in press)
Theofilou P (2011) Quality of life in patients undergoing haemodialysis or peritoneal dialysis treatment. Journal of Clinical Medicine Research (in press)
Morales-Jaimes R, Salazar-Martinez E, Flores-Villegas FJ (2008) The role of depression in the quality of life among patients undergoing renal substitutive therapy. Gac Med Mex 144:91–98
Wiebe SJ, Christensen AJ (1997) Health beliefs, personality, and adherence in hemodialysis patients: an interactional perspective. Ann Behav Med 19:30–35
Bremer AB (1995) Absence of control over health and the psychological adjustment to end-stage renal disease. Ann Behav Med 17:227–233
Gencoz T, Astan G (2006) Social support, locus of control, and depressive symptoms in haemodialysis patients. Scand J Psychol 47:203–208
Acknowledgments
The author would like to thank the patients for their participation in the study and acknowledge the support given by the health professionals and the administration personnel of the dialysis participating units.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Theofilou, P. Quality of life and mental health in hemodialysis and peritoneal dialysis patients: the role of health beliefs. Int Urol Nephrol 44, 245–253 (2012). https://doi.org/10.1007/s11255-011-9975-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-011-9975-0