
Abstract
Background
Hypotension during hemodialysis is frequent in patients with cardiovascular disease who have a limited physiological compensatory response. Recent advances in technology allow non-invasive monitoring of cardiac output and derived hemodynamic parameters. This prospective study evaluated episodes of intradialytic hypotension using clinical data and continuous non-invasive hemodynamic monitoring by impedance cardiography.
Methods
Forty-eight chronic hemodialysis patients, with prevalence for intradialytic hypotensive episodes, underwent evaluation with non-invasive impedance cardiography (Physioflow®) before, during and after a regular dialysis session.
Results
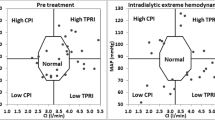
During continuous non-invasive cardiac monitoring, a fall of systolic arterial blood pressure of 20% or more at least once during hemodialysis was detected in 18 patients (37.5%)—thereafter identified as the “Unstable” group. In 30 patients—thereafter called the “Stable” group, the blood pressure did not change significantly. During hypotension, a decrease in cardiac output was found in 11 of the 18 unstable patients, and a significant fall in peripheral resistance in the remaining 7. End-diastolic filling ratio was significantly lower in the unstable group. The most significant predictors associated with intradialytic hypotension were the presence of ischemic heart disease (P = 0.05), and medication with beta blockers (P = 0.037) and calcium channel blockers (P = 0.018).
Conclusions
Hemodynamic changes in dialysis patients with hypotensive episodes included decreased cardiac output or decreased peripheral resistance. A lower end-diastolic filling ratio may be regarded as a marker for reduced preload in these patients. Non-invasive impedance cardiography may be used to evaluate risk factors for hypotension in dialysis patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hypotension during hemodialysis occurs frequently, affecting 15–30% of dialysis patients [1, 2]. The rate of occurrence of hemodialysis-induced hypotension remains high, probably because patients undergoing dialysis are older and sicker [3]. Intradialytic hypotension, which can occur early or late during dialysis, is often associated with vomiting, dizziness and muscle cramps but can also result in significant morbidity and is associated with increased mortality [2, 4, 5]. The causes of hemodialysis-induced hypotension are multifactorial but are based on an interaction between the patient and the dialysis procedure [3]. On one hand, the rate and amount of ultrafiltration will influence the patient’s fluid status; while on the other hand, the patient’s compensatory response to hypovolemia (cardiac, neurohumoral etc.) will determine the clinical manifestations. Normal cardiovascular regulatory mechanisms, such as increased heart rate, contractility and peripheral vascular tone, are required for an adequate response to hemodialysis-induced hypovolemia [2]. Patients may have inefficient compensatory mechanisms, such as sympathetic autonomic failure and increased parasympathetic activity, and thus be more sensitive to hypovolemia. Intradialytic hypotension is therefore more common in patients with cardiovascular disease and diabetes mellitus, because of their limited capability of physiological compensatory response. Furthermore, it has been demonstrated that further deterioration in systolic and diastolic left ventricular function during hemodialysis [6] may cause hypotension, pulmonary edema and/or bradycardic collapse (Bezold–Jarisch reflex) [2, 3]. Decreased venous capacitance and distribution of venous blood to central vessels is also an important mechanism for maintaining cardiac filling during dialysis (DeJager-Krogh phenomenon). This response has been found to be variable in dialysis patients [7]. Other abnormalities include ventricular arrhythmias, associated with increased cardiovascular mortality [8].
Recent advances in technology allow completely non-invasive on-line beat-to-beat monitoring of cardiac output and derived hemodynamic parameters, which can assist in the diagnosis and management of hypotension during dialysis. Continuous digital pulse wave monitoring has been used during dialysis for non-invasive continuous monitoring [9]. Others have examined non-invasive hemodynamic monitoring during hemodialysis, using an admittance cardiograph [10]. Repeated measurements of hemodynamic variables and cardiac output have shown that in most subjects, reduction in parasympathetic nerve activity and an increase in total peripheral resistance are responsible for the maintenance of hemodynamics in chronic dialysis patients [10, 11]. In another study, impedance cardiography was used to assess patients’ fluid status during dialysis, using thoracic fluid content and cardiac output [12]. Karakitsos et al. compared impedance cardiography with echocardiography in hemodialysis patients [13]. They showed that impedance cardiography can estimate hemodynamics in hemodialysis patients with coronary artery disease and help predict outcome in certain patients. Physioflow® is a new generation technique of non-invasive measurement of aortic ejection by impedance cardiography [14]. This technique involves generation of an electrical signal and measurement of beat-to-beat changes of thoracic bioimpedance via dual sensors applied to the neck and thorax. Physioflow® performs continuous non-invasive measurements of the following hemodynamic parameters: heart rate, stroke volume, cardiac output/index, contractility index, filling index, ejection fraction, blood pressure profile (systolic, diastolic and mean), systemic vascular resistance/index, left cardiac index and calculations of end-diastolic filling ratio (EDFR) [14, 15], which has been used to non-invasively assess pulmonary capillary wedge pressure. Its accuracy when compared to the Fick method analysis has been found acceptable at rest and during exercise [14, 16]. Continuous non-invasive cardiovascular monitoring during hemodialysis may therefore demonstrate the pathophysiologic mechanisms of hemodynamic disturbances.
In this prospective sequential clinical study, we set out to evaluate clinical and hemodynamic parameters associated with intradialytic hypotension, using impedance cardiography.
Methods
The study was performed in a tertiary care hospital dialysis unit, which provides hemodialysis therapy for patients during hospital admissions and patients with multiple co-morbidities and special medical problems requiring close monitoring.
Dialysis protocol
All patients were dialyzed three or four times weekly, 3.5 to 5 h per session. The mean urea reduction rate (% URR) in all patients was 65–75%. The dialysis was performed using a polyamide high flux dialyser (1.3 m2). The ultrafiltration rate (% body weight reduction) during dialysis sessions was adjusted according to the presumed dry weight, assessed as the post-dialysis patient’s weight when normotensive and free of edema. The temperature of the dialysate was kept constant at 36°C, while the dialysate flow rate was kept at 500 ml/min. The dialysis sodium concentration was kept constant at 138–140 mmol/l; the dialysate chloride, bicarbonate and potassium concentrations were 108, 35 and 1.5 mmol/l, respectively.
Patients
Patients with end-stage kidney disease on chronic hemodialysis from the above subgroup, who consented to participate in the study, underwent evaluation with the non-invasive bioimpedance cardiography method (Physioflow®), before and during dialysis. Exclusion criteria were: acute febrile infectious illnesses, acute coronary syndromes, acute exacerbation of congestive heart failure, major surgery within the last 3 months, age under 18 and patients’ refusal to participate in the study.
Study definitions
The “Unstable” Group was defined as patients with at least one intradialytic decrease in systolic blood pressure (SBP) of 20% or more relative to the baseline value at the start of hemodialysis. All other patients were included in the “Stable” Group.
Data collection
Clinical data were obtained including: demographic data (age, sex, ethnic origin), physical signs (weight, height), clinical status (ambulatory or hospitalized), smoker or not, the indication for dialysis, the type of hemodialysis access used and dialysis vintage. Additional data included previous and current medical status, current medications especially cardiac agents—beta-blockers, calcium channel blockers, alpha blockers, antiarrhythmics, nitrates and angiotensin converting enzyme (ACE) inhibitors. Information about left ventricular (LV) systolic and diastolic function (obtained from echocardiograms of patients performed during the last year), the presence of chronic diseases such as hypertension, hyperlipidemia, arrhythmias, coronary bypass grafts were also documented. For each case, previous episodes of hemodynamic instability during dialysis were documented, including hemodynamic measurements, symptoms and interventions undertaken, using the hospital electronic database, medical files and documentation in the hemodialysis unit.
The following parameters were documented at the start of dialysis: blood flow of ultrafiltration in ml/min, hematocrit and serum sodium, calcium, phosphorus and albumin levels.
Hemodynamic monitoring
Electrodes were placed over the carotid artery, the right and left sternal borders, under the xyphoid and above the umbilicus, as indicated by the Physioflow® guidelines [14, 15]. Continuous monitoring of real-time multiple hemodynamic and cardiac indices 30 min before, during and 30 min after hemodialysis included: heart rate, systolic arterial blood pressure, diastolic arterial blood pressure, mean arterial blood pressure, filling index, cardiac output, cardiac output index, estimated ejection fraction, systemic vascular resistance, systemic vascular resistance index and calculation of the end-diastolic filling ratio (EDFR) during the pre-dialysis period. The EDFR was defined as the diastolic amplitude of the impedance cardiogram divided by the systolic amplitude × 100 in order to show a percentage [15]. EDFR is correlated with the end-diastolic pressure and is a measure of preload. Measurements were averaged every 20 beats in order to eliminate the effect of respiration [17]. Data were saved and analyzed using the Microsoft programming software of the Physioflow®.
The study was started after institutional review board approval.
Sample size analysis
Sample size was based on an expected difference between the two study groups in EDFR. Assuming that the difference in EDFR will be at least 10% with an SD of 10%, then 20 patients per group and an alpha (two tailed) of 5%, will provide a power of 87% to prove a statistically significant difference.
Statistical analysis
The cornerstone of the statistical analysis was defining the unstable subgroup, and then multidirectional analysis of the demographic, clinical and hemodynamic data. Student’s-test was used to compare continuous variables and Mann–Whitney U test for non-parametric analysis. The Fisher’s exact test was used to compare non-parametric categorical variables. Assuming 10 cases per variable, multivariate analysis was used to determine statistically significant factors associated with intradialytic hypotension as previously defined. All statistical analysis was performed using the SPSS Inc. statistical package version 14.0.
Results
Fifty-two patients consented to participate in the study. Four patients were excluded due to reading artefacts originating from a faulty cable. Patients’ demographic and clinical characteristics are shown in Table 1. Frequent intradialytic hypotensive episodes were documented in 43 (86.9%) of the remaining 48 patients before the study. In 35 patients the hypotensive episodes had been symptomatic, requiring intravenous saline administration. The recruited patients underwent full non-invasive cardiac monitoring before, during and after the hemodialysis session (mean duration 3 to 5 h). During the study, 18 (37.5%) patients fulfilled the criteria for the unstable group. 30 patients (62.5%) were stable during dialysis. In the unstable group, 2 patients had 1 episode, 7 had 2 episodes, 1 had 3 episodes, 1 had 4 episodes, 2 had 5 episodes, 2 had 6 episodes, 2 had 7 episodes, and one patient had 9 episodes of hypotension. Figure 1 represents baseline systolic blood pressure (SBP) measurements for patients included in the study, minimal SBP measurements and percent drop in SBP during dialysis.

Baseline systolic blood pressure and drops during dialysis, SAP—systolic arterial pressure. Patients with a drop of 20% or more in systolic blood pressure during dialysis are defined as the “unstable group” (right of the dotted vertical line-patient number 31)
Independent sample testing showed that multiple factors like age, gender, smoking, percent weight loss during dialysis, duration of dialysis, blood flow, percent change in heart rate, hematocrit, serum sodium, albumin, calcium and phosphorus did not affect the quality of dialysis and were not significantly different in the unstable when compared with the stable patients (Table 2). More patients with a history of ischemic heart disease (IHD) belonged to the unstable group (P = 0.05) (Table 2). Out of the 18 patients with hypotension, 15 suffered from IHD. More so, this subgroup of patients had more than one episode of hypotension during the study hemodialysis session (data not shown). Other conditions such as previous coronary bypass grafting, left ventricular systolic dysfunction, diastolic dysfunction, arrhythmias, hyperlipidemia and hypertension were not associated with an increased rate of hypotension during dialysis (Table 2).
More patients in the unstable group were taking beta blockers (12/18 patients, P = 0.037) and calcium channel blockers (12/18 patients, P = 0.018) (Table 2), but there was no difference in other drug groups.
Baseline hemodynamic variables obtained before the start of dialysis were similar in the stable and unstable groups, except for a lower end-diastolic filling ratio in the unstable group (Table 3). Changes in filling index, cardiac output, ejection fraction and systemic vascular resistance during dialysis were not significant between the two groups (data not shown).
When we examined the unstable group, we found two distinct subgroups of patients: those with decreased cardiac output (defined as patients with at least one episode of decreased cardiac output index during dialysis) were found to have a higher systemic vascular resistance. Those with a stable cardiac output were found to have reduced systemic vascular resistance (Table 4). These may represent separate groups of patients with different pathophysiologic mechanisms of intradialytic hypotension, such as increased vascular resistance associated with a failing or ischemic heart, or vasodilation due to autonomic dysfunction, inefficient compensatory vasoconstriction and sepsis.
Multivariate analysis was performed using two models, including clinical variables (1st model, Table 5a) and hemodynamic variables (2nd model, Table 5b). The use of beta blockers was associated with an increased risk of hemodynamic instability during hemodialysis, with an odds ratio of 4.067 (Table 5a). Patients on calcium channel blockers also had an increased risk of hemodynamic instability during hemodialysis (odds ratio of 6.19) (Table 5a). Multivariate analysis showed that the administration of beta and calcium channel blockers was more dominant than the presence of IHD per se.
In the hemodynamic model, the only significant factor was a reduced EDFR in the pre-dialysis period (Table 5b), where each percent increase in EDFR, reduced the risk of intradialytic hypotension by 0.97. This may represent a marker for lower left ventricular diastolic filling in the unstable group, which may predispose to intradialytic hypotension. Overall, 1-year mortality for patients in the unstable group was 9/18 (50%). Seven patients died of cardiovascular complications (78%) and 2 from sepsis. One-year mortality in the stable group was 40% P = 0.08. There was also a high 1-year mortality rate in the group of patients on beta blockers (58%).
Discussion
To better define the mechanisms of hemodynamic instability during hemodialysis, non-invasive continuous monitoring using cardiac impedance was performed in a selected group of hemodialysis patients with a history of frequent hypotensive episodes and multiple co-morbidities. Eighteen (37.5%) patients developed hypotensive episodes during the monitoring period.
The causes of intradialytic hypotension are multi-factorial, including reduced refilling and intravascular depletion [18, 19], autonomic [20] and diabetic neuropathy, poor cardiac reserve and arrhythmias. Other factors that may influence intradialytic hemodynamics include antihypertensive medications and the release of mediators such as lymphokines, nitric oxide and adenosine, as a result of contact with the dialyser membrane [21]. Appropriate therapy of intradialytic hypotension includes: stopping the dialysis, decreasing the ultrafiltration rate, raising the intravascular volume with infusion of fluids and placing the patient in the Trendelenburg position. Methods to prevent intradialytic hypotensive episodes include determination and correction of the dry weight of each patient on hemodialysis to avoid hypovolemia due to excessive ultrafiltration [18], the use of automatic feedback systems to assess and control blood volume changes during dialysis [22], where the ultrafiltrate volume of plasma is determined at an optimal rate for each patient, to minimize hemodynamic disturbances [23]. Intermittent sodium administration is an established method aimed at increasing refilling of the intravascular compartment [7, 24]. Sodium (Na) profiling and ramping has also been shown to reduce dialysis-induced hypotension [25–27]; however, these have been associated with fluid overload and hypertension [28, 29]. Straver et al. have shown that sodium-balanced Na-profiled hemodialysis maintains blood pressure without providing patients with a sodium load, most probably due to stroke volume preservation [29]. Rubinger et al. have examined the correlations between the long-term development of hypertension in dialysis patients, heart rate variability as a measure of autonomic dysfunction and exposure to high dialysate sodium concentrations [30]. They found that the development of hypertension after 1 year was only partly related to dialysate sodium concentrations, and that a subset of patients who developed hypertension exhibited increased heart rate variability. Na-profiling may therefore be used carefully for prevention of hypotensive episodes in certain hemodialysis patients; however, this may be associated with increased thirst, water intake and interdialytic weight gain.
Patients with congestive heart failure and poor myocardial contractile reserve are more prone to hemodynamic disturbances and hypotension during hemodialysis than other categories of patients [31, 32]. In one study, dobutamine stress echocardiography in 18 hypotension-prone dialysis patients was compared with that of 18 hypotension-resistant patients [31]. Impaired myocardial contractile reserve rather than ischemia was found to be the major mechanism for hypotension. Short-term regulatory mechanisms to acute hypovolemia during dialysis include decreased venous capacitance, increased vascular resistance and increased heart rate and contractility [33]. In a mathematical model using blood volume decrease, heart rate and mean arterial blood pressure, Cavalcanti et al. have shown that patients may be divided into three groups: hypovolemia-sensitive patients, patients with delayed hypotension and hypotension-resistant patients [33] based on their regulatory mechanisms to hypovolemia. Straver et al. have evaluated hemodialysis patients using impedance cardiography [34, 35]. They have shown that symptomatic intradialytic hypotension was associated with a significant decrease in systemic vascular resistance and reduced venous return, most probably caused by an inadequate response to ultrafiltration. They did not find evidence of autonomic dysfunction in these patients. A recent paper that examined the baroreflex mechanism during intradialytic hypotension showed that these mechanisms remain intact and suggests other mechanisms, such as ventricular failure and reduced vascular tone, as risk factors for intradialytic hypotension [36]. Our data suggest that patients in the unstable group demonstrated either decreased cardiac output, which may be due to cardiac ischemia or vasoconstriction, or maintained cardiac output associated with decreased peripheral vascular resistance, which may represent inefficient compensatory mechanisms, autonomic dysfunction or sepsis (Table 4). More patients in the unstable group had a history of ischemic heart disease, which may represent a sicker group of patients with diminished cardiac reserve. The very high mortality in this group of patients supports the previously reported association between intradialytic hypotension and increased mortality [37].
An additional important factor is the baseline central blood volume (CBV). Correlations have been found between CBV and intradialytic hypotension. Cordtz et al. have assessed CBV using thoracic admittance and cardiac function using central venous saturation [38]. They found that reduced baseline thoracic admittance was associated with intradialytic hypotension, and that the central venous saturation was reduced in these patients, suggesting a decrease in cardiac output. Our study has demonstrated a reduced baseline end-diastolic filling ratio (EDFR) in the unstable group. EDFR is a marker of preload and should typically increase in patients with fluid overload and congestive heart failure [15]. A decreased EDFR shows a reduced blood volume, which may be associated with hypotension. The reduced pre-dialytic EDFR in the unstable group may be regarded as a marker for decreased preload predisposing these patients to hypotension. Significant differences were not found in the baseline and intradialytic filling index, cardiac output and systemic vascular resistance between the two groups.
Multiple studies in the last years have shown that beta-blockers and calcium-channel blockers can reduce morbidity and mortality [39, 40]. However, our study has shown that patients who suffer from IHD and those who are treated with beta-blockers and/or calcium channel blockers may have a greater tendency towards hemodynamic instability during dialysis. As mentioned earlier, we hypothesized that one of the main reasons for hypotension and hemodynamic instability during hemodialysis is autonomic dysfunction, most severe in diabetic patients. Diabetes, however, was not found to be statistically associated with hypotension during hemodialysis (P = 0.385).
One of the limitations of our study is the fact that the patient population was heterogeneous, with different pathophysiology, as we have shown. More so, many patients had co-morbidities, as can be expected in a hospital-based dialysis unit and as can be deduced from the high overall mortality. This may therefore limit the capability to obtain uniform prognostic parameters for this group of patients as a whole. We chose to use percent systolic blood pressure drop and not absolute blood pressure measurements to define the “unstable group”, as patients who have high or normal baseline systolic blood pressures may still experience symptomatic hypotension during dialysis. Our primary endpoint for statistical power was based on the difference in EDFR between the two groups. We did not calculate the power for other specific calculations.
Our study has shown that continuous non-invasive hemodynamic monitoring using impedance cardiography can help evaluate critical parameters that may contribute to hemodynamic dysfunction during dialysis. We have shown that the end-diastolic filling ratio may be a predictor of hemodynamic instability during dialysis, suggesting reduced left ventricular filling. We have also demonstrated that cardiovascular instability may be explained by different physiopathological mechanisms (reduced cardiac output or reduced vascular resistance), which may be diagnosed with this non-invasive technique and used to guide specific preventive measures. Other factors, such as the presence of IHD, and the use of beta-blockers and calcium-channel blockers, were found to be associated with hemodynamic instability during dialysis, whereas the use of other drugs or the presence of diabetes were not. These findings provide us with the ability to optimize the treatment of patients on chronic hemodialysis who require therapy for hypertension, congestive heart failure and ischemic heart disease.
Non-invasive impedance cardiography may be used to evaluate risk factors for intradialytic hypotension and to assess hemodynamic changes in hypotension-prone patients. Further research is needed to assess different pathophysiological mechanisms of hemodynamic changes during dialysis and the optimal interventions required.
References
Orofino L, Marcen R, Quereda C et al (1990) Epidemiology of symptomatic hypotension in hemodialysis: is cool dialysate beneficial for all patients? Am J Nephrol 10:177–180
Daugirdas JT (2001) Pathophysiology of dialysis hypotension: an update. Am J Kidney Dis 38:S11–S17
Santoro A (2006) Cardiovascular dialysis instability and convective therapies. Hemodial Int 10(1):S51–S55
Henrich WL (1986) Hemodynamic instability during hemodialysis. Kidney Int 30:605–612
van der Sande FM, Kooman JP, Leunissen KM (2000) Intradialytic hypotension–new concepts on an old problem. Nephrol Dial Transplant 15:1746–1748
Galetta F, Cupisti A, Franzoni F et al (2006) Acute effects of hemodialysis on left ventricular function evaluated by tissue Doppler imaging. Biomed Pharmacother 60:66–70
Sherman RA (2002) Intradialytic hypotension: an overview of recent, unresolved and overlooked issues. Semin Dial 15:141–143
Makaryus AN (2006) Ventricular arrhythmias in dialysis patients. Rev Cardiovasc Med 7:17–22
Burkert A, Scholze A, Tepel M (2006) Noninvasive continuous monitoring of digital pulse waves during hemodialysis. ASAIO J 52:174–179
Yoshii M, Minami J, Ishimitsu T et al (2005) Non-invasive monitoring of hemodynamic changes during hemodialysis by the use of a newly developed admittance cardiograph. Ther Apher Dial 9:154–160
Chou KJ, Lee PT, Chen CL et al (2006) Physiological changes during hemodialysis in patients with intradialysis hypertension. Kidney Int 69:1833–1838
Wynne JL, Ovadje LO, Akridge CM et al (2006) Impedance cardiography: a potential monitor for hemodialysis. J Surg Res 133:55–60
Karakitsos D, Wachtel M, Zerefos N et al (2008) Prognostic utility of impedance cardiography measurements in elderly hemodialysis patients with coronary artery disease. Am J Nephrol 29:426–433
Charloux A, Lonsdorfer-Wolf E, Richard R et al (2000) A new impedance cardiograph device for the non-invasive evaluation of cardiac output at rest and during exercise: comparison with the “direct” Fick method. Eur J Appl Physiol 82:313–320
Woltjer HH, Bogaard HJ, Bronzwaer JG et al (1997) Prediction of pulmonary capillary wedge pressure and assessment of stroke volume by noninvasive impedance cardiography. Am Heart J 134:450–455
Richard R, Lonsdorfer-Wolf E, Charloux A et al (2001) Non-invasive cardiac output evaluation during a maximal progressive exercise test, using a new impedance cardiograph device. Eur J Appl Physiol 85:202–207
Verschoor N, Woltjer HH, van der Meer BJ et al (1996) The lowering of stroke volume measured by means of impedance cardiography during endexpiratory breath holding. Physiol Meas 17:29–35
Kouw PM, Kooman JP, Cheriex EC et al (1993) Assessment of postdialysis dry weight: a comparison of techniques. J Am Soc Nephrol 4:98–104
Begin V, Deziel C, Madore F (2002) Biofeedback regulation of ultrafiltration and dialysate conductivity for the prevention of hypotension during hemodialysis. ASAIO J 48:312–315
Rubinger D, Revis N, Pollak A et al (2004) Predictors of haemodynamic instability and heart rate variability during haemodialysis. Nephrol Dial Transplant 19:2053–2060
Noris M, Benigni A, Boccardo P et al (1993) Enhanced nitric oxide synthesis in uremia: implications for platelet dysfunction and dialysis hypotension. Kidney Int 44:445–450
Franssen CF, Dasselaar JJ, Sytsma P et al (2005) Automatic feedback control of relative blood volume changes during hemodialysis improves blood pressure stability during and after dialysis. Hemodial Int 9:383–392
Donauer J, Kolblin D, Bek M et al (2000) Ultrafiltration profiling and measurement of relative blood volume as strategies to reduce hemodialysis-related side effects. Am J Kidney Dis 36:115–123
Donauer J (2004) Hemodialysis-induced hypotension: impact of technologic advances. Semin Dial 17:333–335
Dheenan S, Henrich WL (2001) Preventing dialysis hypotension: a comparison of usual protective maneuvers. Kidney Int 59:1175–1181
Stiller S, Bonnie-Schorn E, Grassmann A et al (2001) A critical review of sodium profiling for hemodialysis. Semin Dial 14:337–347
Gong R, Lindberg J, Abrams J et al (1993) Comparison of hypertonic saline solutions and dextran in dialysis-induced hypotension. J Am Soc Nephrol 3:1808–1812
Sang GL, Kovithavongs C, Ulan R et al (1997) Sodium ramping in hemodialysis: a study of beneficial and adverse effects. Am J Kidney Dis 29:669–677
Straver B, De Vries PM, Donker AJ et al (2002) The effect of profiled hemodialysis on intradialytic hemodynamics when a proper sodium balance is applied. Blood Purif 20:364–369
Rubinger D, Backenroth R, Pollak A et al (2008) Blood pressure and heart rate variability in patients on conventional or sodium-profiling hemodialysis. Ren Fail 30:277–286
Poldermans D, Man in ‘t Veld AJ, Rambaldi R et al (1999) Cardiac evaluation in hypotension-prone and hypotension-resistant hemodialysis patients. Kidney Int 56:1905–1911
Schreiber BD (2003) Congestive heart failure in patients with chronic kidney disease and on dialysis. Am J Med Sci 325:179–193
Cavalcanti S, Cavani S, Santoro A (2002) Role of short-term regulatory mechanisms on pressure response to hemodialysis-induced hypovolemia. Kidney Int 61:228–238
Straver B, Roggekamp MC, de Vries PM et al (1998) Systemic vascular resistance in intradialytic hypotension determined by means of impedance cardiography. Blood Purif 16:281–289
Straver B, de Vries PM, ten Voorde BJ et al (1998) Intradialytic hypotension in relation to pre-existent autonomic dysfunction in hemodialysis patients. Int J Artif Organs 21:794–801
Sapoznikov D, Backenroth R, Rubinger D (2010) Baroreflex sensitivity and sympatho-vagal balance during intradialytic hypotensive episodes. J Hypertens 28:314–324
Shoji T, Tsubakihara Y, Fujii M et al (2004) Hemodialysis-associated hypotension as an independent risk factor for two-year mortality in hemodialysis patients. Kidney Int 66:1212–1220
Cordtz J, Olde B, Solem K et al (2008) Central venous oxygen saturation and thoracic admittance during dialysis: new approaches to hemodynamic monitoring. Hemodial Int 12:369–377
Spiecker M (2006) Heart failure in elderly patients. Exp Gerontol 41:549–551
Weber MA (2006) Hypertension treatment and implications of recent cardiovascular outcome trials. J Hypertens Suppl 24:S37–S44
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bayya, A., Rubinger, D., Linton, D.M. et al. Evaluation of intradialytic hypotension using impedance cardiography. Int Urol Nephrol 43, 855–864 (2011). https://doi.org/10.1007/s11255-010-9746-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-010-9746-3