
Abstract
Aim
The handling of renal creatinine in human beings has classically been described as the result of two particular physiological processes: glomerular filtration and proximal tubular secretion. However, there are particular physiological situations in which tubular creatinine reabsorption has been documented, such as in the case of healthy newborns and premature babies. We performed a prospective study in order to evaluate if there is tubular creatinine reabsorption in healthy elderly people.
Patients and method
We studied prospectively nine healthy volunteers, four of them young (20–33 years old) and the remaining five, old (65–73 years old). Since creatinine is secreted in the proximal tubules, and its secretion can be completely blocked by cimetidine administration, a creatinine clearance with cimetidine reliably represents the glomerular filtration rate. Therefore, if the ratio creatinine clearance (Ccr)/creatinine clearance with cimetidine (CcrWC) is higher than one, this would indicate net creatinine secretion, whereas a ratio lower than one would indicate a net renal creatinine tubular reabsorption; a ratio equal to one indicates creatinine filtration. Finally, the Ccr, CcrWC, and Ccr/CcrWC ratios were compared between the young and old group.
Statistical tests
Mann-Whitney and Wilcoxon tests were used.
Results
As expected, creatinine clearance in the elderly was significantly lower than in the young [Ccr: 74.4 ml/min (47.9–100.9) (old) vs. 153.8 ml/min (108.3–199.2) (young), p = 0.014]. Similarly, the creatinine clearance with cimetidine (CcrWC) was significantly lower in the elderly compared to the young [CcrWC: 81.8 ml/min (69.2–94.5) (old) vs. 122.5 ml/min (82.6–162.4) (young), p = 0.028]. The ratio of Ccr/CcrWC was 0.9 in the elderly vs. 1.26 in the young (p = 0.014), indicating net creatinine reabsorption in the elderly and net creatinine secretion in the young.
Conclusion
Our findings indicate that there seems to be a net reabsorption of creatinine in the renal tubules of healthy old persons.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The handling of renal creatinine in humans has classically been described as the result of two physiological processes: glomerular filtration and proximal tubular secretion [1].
However, there are certain physiological situations, such as in the case of healthy newborns and premature babies, in which tubular creatinine reabsorption has been documented [2–4].
On the other hand, in acute renal failure secondary to dehydration in young people, the blood urea level is increased with normal serum creatinine, a situation that normalizes with rehydration. The high serum urea level can be explained by the extensive urea tubular reabsorption induced by volume contraction [5]. However, acute renal failure secondary to dehydration in the elderly usually shows a different serum pattern that consists of an elevation not only of the serum urea level, but also of serum creatinine, and both altered values also normalize with rehydration [6]. Since the latter observation can be explained by a different tubular creatinine handling (i.e., creatinine reabsorption) in elderly compared to young patients, we decided to study prospectively if there is tubular creatinine reabsorption in healthy elderly people.
Materials and methods
We studied nine healthy volunteers, four of them young (20–33 years old) and the rest old (65–73 years old), who had already been accepted as kidney donors, and consequently had documented normal urinalysis, renal ultrasound, bladder voiding, and renal functional tests, and were taking no medication. The female/male ratio was 1.3 in each group.
All subjects signed a consent form approved by the hospital’s ethics committee.
Since creatinine is secreted in proximal tubules, and its secretion can be blocked by cimetidine administration because this drug competes with the creatinine tubular secretion mechanism, a creatinine clearance with cimetidine reliably represents the glomerular filtration rate [7]. Moreover, a ratio of creatinine clearance (Ccr)/creatinine clearance with cimetidine (CcrWC) higher than one shows a net renal creatinine secretion, whereas a ratio lower than one shows a net renal creatinine reabsorption [2].
We measured the Ccr, CcrWC, and Ccr/CcrWC ratio of each volunteer in timed urine samples.
To obtain timed-creatinine clearances, the following protocol was followed: after obtaining a basal blood sample, we initiated oral hydration using tap water (20 ml/kg) for over 30 min. At the end of the 30-min periods, patients were asked to void spontaneously (which usually shows a urinary flow of around 30 min). Time and volume data obtained from each micturition were accurately documented from two periods (in order to obtain an average value). Complete bladder voiding was documented by ultrasound. Creatinine clearance was calculated from these data applying the following formula:
creatinine clearance = urinary creatinine (mg/dl) × urinary volume (ml)/serum creatinine (mg/dl) × time (min)
The same protocol was performed for each volunteer a week later, after receiving on that occasion cimetidine by mouth (1,600 mg/day) 48 h before performing the glomerular filtration test.
Therefore, an average creatinine clearance of the timed samples (without and with pre-medication with cimetidine) was obtained for each subject. From these data, we calculated the Ccr/CcrWC ratio.
Finally, Ccr, CcrWC, and Ccr/CcrWC ratio were compared between the young and elderly groups. Statistical analysis was performed applying Mann-Whitney and Wilcoxon tests.
Results
Measured Ccr and CcrWC were significantly lower in the elderly group (69 ± 3 years old) compared with the young (25 ± 6 years old) one:
Ccr: 74.4 ml/min (47.9–100.9) (old) vs. 153.8 ml/min (108.3–199.2) (young), p = 0.014
CcrWC: 81.8 ml/min (69.2–94.5) (old) vs. 122.5 ml/min (82.6–162.4) (young), p = 0.028 (Tables 1 and 2)
Furthermore, the Ccr/CcrWC ratio was significantly lower in the elderly group compared with the young one: 0.9 (0.66–1.14) (old) vs 1.26 (1.20–1.32) (young), p = 0.014.
In the young group, CcrWC (122.5 ml-min) was significantly lower compared to Ccr (153.8 ml-min): (p = 0.0003).
Conversely, there was no significant difference documented between Ccr (74.4 ml-min) and CcrWC (81.8 ml-min) in the elderly group (p = NS) (Table 1).
There was no significant difference between the groups with regard to voiding time, serum creatinine, urine creatinine, and volume. However, regarding the latter two variables, they showed a tendency to be lower in the elderly group with a borderline p value (p = 0.08).
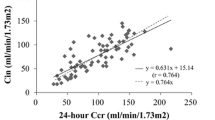
Finally, linear correlation between CcrWC and eGFR estimating either MDRD and CG (Cockroft-Gault) formulas showed a better correlation between CcrWC and eGFR by CG and MDRD formulas (r = 0.8) in the young group. In the latter group, a good correlation was documented only between CcrWC and MDRD formula (r = 0.4), but not between the CcrWC and CG formula (r = 0.1) (Table 3).
Discussion
In this study, Ccr and CcrWC were significantly lower in the aged group, reflecting the known reduction of glomerular filtration related to normal aging (Table 1) [8]. Regarding the various components of the creatinine clearance formula (serum creatinine, urinary creatinine and volume, and voiding time), there was no significant difference between the groups in their serum creatinine or in their collecting urine time, but there was a tendency to a lower value in urinary creatinine and urinary volume in the aged group compared with the young one (Table 4).
Since creatinine is only filtered and secreted in healthy young people, and a mega-dose of cimetidine blocks proximal tubule creatinine secretion, Ccr was significantly higher compared with CcrWC in the young group than in the old group (Table 1). Moreover, the Ccr/CcrWC ratio was higher than one (Ccr/CcrWC: 1.3) in the young group, indicating that creatinine was net secreted in this age group.
Conversely, there was no significant difference between Ccr (74.4 ml-min) and CcrWC (81.8 ml-min) in the elderly group (p = NS) (Table 1), and the ratio of Ccr/CcrWC was lower than one (0.9), thus indicating a net tubular creatinine reabsorption (or creatinine back leak) in this age group.
Tubular reabsorption of creatinine is a very unusual physiological phenomenon, but there are previous data that support its existence in premature and term infants, as well as dehydrated adults [2, 9]. In the former, it was attributed to slow urinary flow along the tubule at this age and particularly back-leak of creatinine along the immature tubular structure. In our study, since all volunteers were well hydrated during the timed creatinine clearance, dehydration could not explain the observation of creatinine reabsorption.
There are several tubular changes documented in the aging kidney, such as decreased tubular volume, length, and number, as well as tubular atrophy with simplification of its epithelium and thickening of its basement membrane. It is possible that these changes could make the aged tubules more susceptible to creatinine reabsorption, as happens in newborns, but in this case due to tubular immaturity [10–12].
From a practical point of view, our findings indicate that, contrary to what happens in healthy young persons, a measured creatinine clearance underestimates the glomerular filtration rate value in elderly individuals.
The Cockroft-Gault formula for the estimation of creatinine clearance has been widely used, and even though its use has been questioned because it overestimates the rate of decline in the glomerular filtration rate in the oldest old, it correlates well with clearance measured with 99Tc diethylenetriamine penta-acetic acid (DTPA) in old and very old people [13, 14]. On the contrary, the modified Diet in Renal Disease (MDRD) formula has not yet been validated in persons aged over 70 years [14, 15]. In our study, both formulae showed a very good correlation (r = 0.8) with timed creatinine clearance with cimetidine in healthy young persons, but not in the old ones (Table 3).
One of the limitations of this study is the small number of studied volunteers (nine). However, despite the small number, the observed difference between these groups was statistically significant. Furthermore, the fact that the obtained values were obtained by a reliable method of creatinine clearance measurement (timed creatinine clearance) further strengthens the reliability of our findings.
Conclusion
In conclusion, our findings indicate that it seems to be a net reabsorption of creatinine in the renal tubules of healthy elderly persons.
References
Rennke HG, Denker BM (2007) Review of renal physiology. In: Helmut GR, Denker BM (eds) Renal pathophysiology: the essentials. Lippincott Williams and Wilkins, Philadelphia, pp 1–30
Matos P, Duarte-Silva M, Drukker A et al (1998) Creatinine reabsorption by the newborn rabbit kidney. Pediatr res 44(5):639–641
Alt JM, Colenbrander B, Forsling M, MacDonald A (1984) Perinatal development of tubular function in the pig. Q J Exp Physiol 69:693–702
Coulthard MG, Hey E, Ruddock V (1985) Creatinine and urea clearances compared to inulin clearance in preterm and mature babies. Early Hum Dev 11:11–19. doi:10.1016/0378-3782(85)90114-8
Faber M, Gopal Kuppin W, Krishna Narins R (1993) The differential diagnosis of acute renal failure. In: Lazarus JM, Brenner BM (eds) Acute renal failure. Churchill Linvingston, New York, pp 133–192
Musso CG, Liakopoulos V, Ioannidis I, Stefanidis I (2006) Acute renal failure in the elderly: characteristics. Int Urol Nephrol 38(3–4):787–793. doi:10.1007/s11255-006-0084-4
Hilbrands LB, Artz MA, Wetzles JFM et al (1991) Cimetidina improves the reliability of creatinine as a marker of glomerular filtration. Kidney Int 40:1171–1176. doi:10.1038/ki.1991.331
Macías Nuñez JF, Lopez Novoa J (2008) Physiology of the healthy aging kidney. In: Macías Nuñez JF, Cameron S, Oreopoulos D (eds) The aging kidney in health and disease. Springer, New York, pp 93–112
Sjöström PA, Odlind BG, Wolgast M (1988) Extensive tubular secretion and reabsorption of creatinine in humans. Scand J Urol Nephrol 22:129–131
Silva FG (2005) The ageing kidney : a review–Part I. Int Urol Nephrol 37:185–205. doi:10.1007/s11255-004-0873-6
Silva FG (2005) The ageing kidney: a review–Part II. Int Urol Nephrol 37:419–432. doi:10.1007/s11255-004-0874-5
Zhou XJ, Laszik ZG, Silva FG (2008) Anatomical changes in the aging kidney. In: Macías Núñez JF, Cameron JS, Oreopoulos D (eds) The aging kidney in health and disease. Springer, New York, pp 39–54
Cockroft DW, Gault MN (1976) Prediction of creatinine clearance from serum creatinine. Nephron 16:31–41. doi:10.1159/000130554
Macías Núñez JF, López Novoa JM (2008) Physiology of the healthy aging kidney. In: Macías Núñez JF, Cameron JS, Oreopoulos D (eds) The aging kidney in health and disease. Springer, New York, pp 93–112
Lebey AS, Bosh JP, Lewis JB, Greene T, Rogers N, Roth DA (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med 130:461–470
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Musso, C.G., Michelángelo, H., Vilas, M. et al. Creatinine reabsorption by the aged kidney. Int Urol Nephrol 41, 727–731 (2009). https://doi.org/10.1007/s11255-008-9508-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-008-9508-7