
Abstract
Background
Impairment of the release of endothelium and platelet derived-nitric oxide (NO) increases thrombus formation that is rich in platelets in non-ST elevation acute coronary syndromes (NSTE-ACS). Since intracoronary thrombus formation and distal embolization increases risk of myocardial injury, we studied the relationship between NO levels and Tn-I in patients with NSTE-ACS.
Methods
Nitric oxide and Tn-I levels of 234 consecutive patients with NSTE-ACS were measured from venous samples at admission. The 137 patients whose Tn-I levels were below 0.20 ng/ml grouped as Tn-I negative and 97 patients whose Tn-I levels were equal to and above 0.21 ng/ml were grouped as Tn-I positive. Presence of visible thrombus, degree of flow in Thrombolysis in Myocardial Infarction (TIMI), and morphology of the lesion were evaluated with coronary angiographies.
Results
Presence of coronary thrombus, impaired TIMI flow, frequency of complex lesions, angina and ST-T changes were more frequent and associated with Tn-I levels in Tn-I positive patients. NO levels were lower in patients who were Tn-I positive, had angina and ST-T changes. NO levels were similar between patients with simple or complex lesions, but lower in patients who had coronary thrombus or TIMI flow grade <2. There was a negative correlation between levels of Tn-I and NO (r = −0.87, P < 0.001). Logistic regression analysis revealed that NO levels were independent predictors in the differentiation of Tn-I negatives and positives (r = 0.527, P < 0.001).
Conclusion
This study revealed that NO levels are associated with myocardial injury in patients with NSTE-ACS.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Non-ST elevation acute coronary syndrome (NSTE-ACS) is a heterogeneous disease. Rupture of intracoronary plaque and additional thrombosis accompany the clinical syndrome in most cases. Increased troponin levels are independent predictors of negative consequences, particularly of following myocardial infarctions and sudden death in these patients [1, 2]. It has been reported that increased troponin levels indicate presence of platelet-rich thrombus in the culprit lesion [3, 4], and that the cause of this increase was an indicator of myocardial injury due to distal vascular embolism of the thrombus [5, 6]. However, it is still unclear why coronary thrombus and distal embolism does not occur in troponin negative NSTE-ACS patients despite the similarity of all risk factors.
In NSTE-ACS, platelets, which are bound with subendothelium, are activated following the rupture of plaque, and further stimulate thrombus formation by producing thromboxane A2 (TxA2) and increasing thrombin formation. Endothelial products such as prostacyclins and nitric oxide (NO) play an important role in the regulation of platelet activation and aggregation [7]. Previous studies have shown that NO reversed the activation of glycoprotein IIb/IIIa, and prevented thrombosis by inhibiting platelet adhesion and aggregation [8]. However, in patients with ACS, not only the release of NO from endothelium is decreased, release of NO from platelets themselves is also impaired [9, 10]. Since platelet activation is the initial step in thrombus formation, and since intracoronary thrombus formation and its distal embolization increases the risk of myocardial injury, we planned to investigate the relationship between NO and Tn-I levels in patients with NSTE-ACS.
Methods
Patient selection
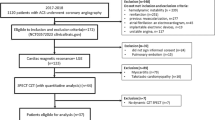
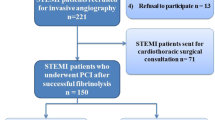
A total of 296 consecutive patients, who were admitted to our department with the complaint of chest pain and diagnosed as NSTE-ACS, were included in the study. NSTE-ACS was diagnosed with the presence of newly-onset severe or increasing angina, and rest angina within 48 h. These symptoms were taken into account when there were concomitant ECG changes indicative of ischemia (at admission or follow-up, transient or permanent >0.1 mV pathological ST depression or T negativity, absence of Q wave in at least 2 consecutive derivations). Measurements of CK and CK-MB levels at admission and during the following 3 days were used for diagnostic enzyme coding of WHO. Eight patients diagnosed with myocardial infarction at admission or follow-ups according to WHO criteria, 21 patients with cardiomyopathy, heart failure, CABG, or PTCA and renal failure, as well as 23 patients who received nitrate therapy within 48 h, and 10 patients in whom coronary angiography could not be performed were excluded from the study. Consequently, 234 patients participated in study analysis. Following the diagnosis aspirin, clopidogrel, low molecular weight-heparin and beta-blocker were begun in all patients. Venous blood samples were obtained in order to determine Tn-I levels at admission, in addition to 12 and 24 h after the onset of symptoms, which is the most appropriate time interval to identify myocardial injury. Coronary angiography was performed within 48 h following admission. All patients were informed verbally and their written consents were obtained.
Measurement of serum Tn-I levels
Serum obtained from venous blood samples were used for measurements. Tn-I levels were measured quantitatively with the IMMULYTE Analyzer (EUROAPCUK) kit. Since levels below 0.20 ng/ml could not be measured quantitatively with the kit, these levels were considered to be negative. Tn-I levels ≥0.21 ng/ml were determined quantitatively and considered to be positive. Quantitatively measured Tn-I levels were divided into 4 groups (Group I = Tn-I < 0.20, Group II = 0.21 < Tn-I < 1.0, Group III = 1.0 < Tn-I < 2.0, Group IV = Tn-I > 2.0).
Measurement of NO production
Nitric oxide production was assayed indirectly by measuring nitrite production. The amount of NO induced in plasma was quantitated by the Griess reagent method [11]. Briefly, equal volumes of plasma and the Griess reagent (1% sulfanilamide, 0.1% naphthylethylene diamine dihydrochloride, 2.5% H3PO4) (50 μl each) were mixed in 96-well plates, and the absorbance associated with color change was measured within 10 min at a 550-nm wavelength in a microplate auto reader spectrophotometer. Nitrite concentration was determined with reference to a standard curve by using concentrations sodium nitrite in plasma.
Angiographic analyses
Angiographic images were evaluated visually by two experienced cardiologists and one cardiovascular surgeon, who were blinded to clinical information and Tn-I or NO levels of the patients. Angiographies were classified according to Thrombolysis in Myocardial Infarction (TIMI) flow, morphology of causative lesion and presence of visible thrombus. Classification by lesion morphology was performed according to Ambrose and Israel [12] and American Heart Association/American College of Cardiology (AHA/ACC) criteria, and all stenoses with a diameter loss of more than 30% were evaluated. First, lesions were classified as simple or complex. Following characteristics were accepted as complexity criteria: 1. Edges with irregular morphology or notches or both, 2. Lesions with sudden indentations into vascular wall, 3. Ulcerations, 4. Filling defect compatible with intracoronary thrombus. Filling defects or haziness observed in at least two images were evaluated as coronary thrombus. On the other hand, lesions that did not comply with criteria of complex lesions were accepted as simple lesions. ACC/AHA lesion types (A, B1, B2, and C) were classified according to morphologic characteristics including angulation, bifurcation, calcification, long lesion more than 20 mm in length, eccentricity, irregularity, ostial lesion, thrombus-containing lesion, and chronic total lesion. Coronary vessels were divided into 16 segments and patients were classified as one-vessel, two-vessel or three-vessel-disease patients according stenoses more than 50% at these segments.
Statistical analysis
Continuous variables were expressed as mean ± SD. Student’s t-test was used in the evaluation of continuous variables that showed normal distribution. Since NO did not show normal distribution, Mann–Whitney U test was used in the comparison of two groups and Kruskal–Wallis variance analysis and Mann–Whitney U test with Bonferroni correction were used in the comparison of more than two groups. Significance levels were accepted as P < 0.05 for Mann–Whitney U test and Kruskal–Wallis variance analysis, and P < 0.016 for Mann–Whitney U test with Bonferroni correction. Chi-square test was used to evaluate differences between groups with non-continuous variables. Correlation between the continuous variables was evaluated using Spearman Correlation Analysis. Exponential regression analysis was performed to evaluate whether NO levels had predictive value in determining Tn-I levels, and logistic regression analyses was performed to evaluate whether NO levels were independent predictors in differentiation of Tn-I positive and negative cases.
Results
Among 234 patients included in study analysis, 97 (41.5%) were determined to be Tn-I positive and 137 (58.5%) Tn-I negative. Baseline clinical characteristics of the patients are presented in Table 1. There was no significant difference between groups in terms of the frequency of risk factors of coronary artery disease and timing of catheterization.
There was no significant difference between Tn-I positive and negative groups in terms of the distribution of culprit lesions or multi-vessel disease. Angiographic complex lesions were more prevalent in Tn-I positive patients, however the two groups were found to have similar A, B1, B2, and C type lesions. No patient with a TIMI flow grade of 0 was found in either of the groups. However the prevalence of patients with TIMI flow grade <2 was significantly higher in Tn-I positive group as compared to Tn-1 negative group. Angiographically visible thrombus was observed in 24.7% in Tn-I positive group and in 7.3% in Tn-I negative group, and there was a significant difference between the two groups in terms of the frequency of thrombus observation (x 2 = 5.3, df = l, P < 0.012, OR = 2.1 (1.06 < OR < 3.8) (Table 2).
We observed that as Tn-I levels increased, the prevalence of visible coronary thrombus and complex lesions also increased, whereas TIMI flow grade decreased significantly. A similar association was also determined between Tn-I levels and patients who had chest pain and ST changes at admission (Table 3).
Nitric oxide levels were not different in comparison of patients have or not traditional coronary risk factors (Table 4). Baseline levels of NO in Tn-I positive patients were significantly lower than those of Tn-I negatives (16.4 ± 9.8 μM vs. 52.6 ± 15.0 μM, P < 0.001). NO levels of patients whose Tn-I levels were equal to or above 2.0 ng/ml (5.3 ± 2.5 μM) were different from those of patients whose Tn-I levels were below 0.20 ng/ml (52.6 ± 15.0 μM, P < 0.001) or between 0.21–0.99 ng/ml (26.2 ± 4.8 μM, P < 0.001). However, NO levels of patients, whose Tn-I levels were equal to or above 2.0 ng/ml did not differ from those of patients with Tn-I levels between 1.0 and 1.99 ng/ml (11.9 ± 2.1 μM, P > 0.17) (Fig. 1).

Comparison of NO Levels according to percentiles of Troponin I levels (*P < 0.001 vs. Tn ≤ 0.20 ng/ml and Tn = 0.21–0.99 ng/ml)
Nitric oxide levels of patients whose TIMI flow grade was 3 (45.1 ± 19.1 μM) were found to be higher as compared to patients whose TIMI flow grade was 2 (28.7 ± 20.4 μM, P < 0.001) or 1 (20.9 ± 18.5 μM, P < 0.001). There was no significant difference between NO levels of patients whose TIMI flow grade was 2 or 1 (P > 0.019) (Fig. 2).

Comparison of NO Levels according to TIMI flow grading (*P < 0.001 vs. Tn ≤ 0.20 ng/ml and Tn = 0.21–0.99 ng/ml)
Nitric oxide levels of patients with one-vessel (35.7 ± 22.8 μM), two-vessel (35.7 ± 19.4 μM) or three-vessel (40.3 ± 25.9 μM) disease were found to be similar (P > 0.13) (Fig. 3A). Similarly, there was no significant difference between NO levels of patients with type A (39.4 ± 20.1 μM), type Bl (37.7 ± 23.6 μM), type B2 (35.2 ± 23.0 μM) and type C (38.7 ± 21.1 μM) lesions (P > 0.81) (Fig. 3B). Moreover, NO levels of patients who had angiographically complex (34.0 ± 23.5 μM) or simple (40.5 ± 20.5 μM) lesions were also similar (P < 0.032).

Comparison of NO Levels according to number of diseased vessel (A) and angiographically lesion type (B)
Nitric oxide levels of patients who were found to have intracoronary thrombus were significantly lower than those without coronary thrombus (20.8 ± 15.6 μM vs. 45.6 ± 20.2 μM, P < 0.001). NO levels of patients who had chest pain at admission were lower as compared to patients who had not (28.3 ± 7.9 μM vs. 49.4 ± 8.2 μM, P < 0.001). Similarly, NO levels of patients who showed ischemic ST-T changes at admission were lower than patients who did not show any such changes (32.8 ± 9.4 μM vs. 42.5 ± 11.9 μM, P < 0.001).
Spearman correlation analysis revealed that there was a negative correlation between quantitative Tn-I and NO levels in Tn-I positive patients (r = −0.87, P < 0.001). Logistic regression analyses showed that NO levels in patients with NSTE-ACS were independent predictors in the differentiation of Tn-I positives and negatives (r = 0.527, P < 0.001). In addition, exponential regression analyses demonstrated that NO levels had substantial predictive value in determining Tn-I levels (r = 0 85, r 2 = 0.72, P < 0.0001).
Discussion
In this study we determined that NO levels of Tn-I positive NSTE-ACS patients at admission were significantly lower than those of Tn-I negative patients. It is known that endothelium and platelet dependent NO impairment is common in the presence of coronary risk factors and ACS in the presence of atherosclerotic diseases [8–10]. However our study was first to show the negative relationship between levels of Tn-I and NO in patients with NSTE-ACS. We demonstrated that NO levels had significant predictive value in determining Tn-I levels and differentiating Tn-I positives and negatives in NSTE-ACS patients. Presence of complex lesions was more prevalent among Tn-I positive patients as compared to Tn-I negatives, however there was no significant difference between NO levels of patients with complex or simple lesions in both Tn-I positives and negatives. Similar findings were also observed in single-vessel or multi-vessel disease patients. NO levels, however, were found to be associated with high vascular risk such as impaired TIMI flow and presence of coronary thrombus. This suggests that increased Tn-I levels may be related with NO levels, rather than the severity of coronary artery disease.
Increased Tn-I levels in NSTE-ACS patients are associated with the increase in vascular risk [3, 4] as well as high risk of cardiac events [1, 2]. In our study the presence of angiographically visible thrombus and impaired TIMI flow in Tn-I positive NSTE-ACS patients has been shown to be more prevalent and related with Tn-I levels. This was consistent with results of previous studies [13, 14]. In addition, previous studies demonstrated that impaired TIMI flow could be corrected with Glycoprotein IIb/IIIa antagonists without any coronary intervention in Tn-I positive NSTE-ACS patients [15–17]. Results of angioscopy have revealed that the most distinctive event in the differentiation of Tn-I positive and negative patients was the presence of coronary thrombus [5]. Such platelet-rich thrombi lead to embolism to distal vascular beds, which is among the causative mechanisms of myocardial injury defined by high levels of Tn-I in NSTE-ACS patients [3, 5, 6].
Presence of platelet-rich thrombus in the causative lesion indicates active thrombotic process, and evidence has shown that platelet-rich thrombus is more common in Tn-I positive NSTE-ACS patients as compared to Tn-I negatives [13, 14]. Despite similar mechanisms, cause of this difference is unclear. Our results suggest that this difference—at least partially—is related with NO levels of patients. The importance of platelet activation in NSTE-ACS was supported with definite clinical benefits provided by Glycoprotein IIb/IIIa antagonists and aspirin. Activation, adhesion and aggregation of platelets may follow plaque rupture in these patients, and these results in formation of platelet-rich thrombus. NO inhibits platelet aggregation and accumulation in the growing thrombus [7, 8]. Since platelet accumulation is the main event in increased intracoronary thrombus and distal embolism, it may be concluded that decreased NO levels are associated with myocardial injury in patients with NSTE-ACS.
Previous studies have demonstrated that NO reversed Glycoprotein IIb/IIIa activation and prevented thrombosis by inhibiting adhesion and aggregation of platelets [8–10]. Chronic inhibition of NO formation is related with active thrombotic processes such as the increase in thrombin and tissue factor in addition to the impairment in fibrinolysis [18]. On the other hand, NO is synergistic with prostacyclin, which is a potent vasodilator and anti-aggregative, and prostacyclin behaves as a biologic antagonist of TxA2 [7]. Platelets produce NO themselves and inhibit platelet activation via negative feedback mechanism [9, 10]. However, not only release of NO from endothelium is impaired, but production of platelet derived NO is also diminished in patients with ACS [9, 10]. Parallel with these, it has been shown that aggregated platelets in patients with ACS produced less NO, and this led to an increase in thrombus formation, contributed to the development of ACS [9, 10] and is associated with poor prognosis [19]. Besides, NO inhibits the activation of leucocytes, which play a role in the interaction between platelets and vascular wall. This inhibition may limit the development of intracoronary thrombus. All of these results and our data support our hypothesis that, thrombi large enough to occlude distal vascular bed and cause myocardial injury may be related with NO levels of the patients.
Since increased troponin levels indicate poor microvascular perfusion [15, 20], we suggest that high NO levels determined in Tn-I negative NSTE-ACS patients probably improve microvascular perfusion. Administration of NO during experimental ischemia reperfusion models and cardiac surgery has decreased myocardial injury [21–23]. This effect was found to be related with the improvement in cardiac perfusion due to known vasodilator and anti-aggregative properties of NO [21–23]. In addition, nitrovasodilators demonstrated beneficial anti-thrombotic effects in combination with prostacyclin. Nitrovasodilator agents with known clinical efficacy show their effects after being converted into NO. It has been shown in various studies that positive effects of these agents on angina and ischemic ST-T changes in patients with ACS were related with the improvement in cardiac perfusion [23, 24]. This also clinically supports the low NO levels that we determined in patients who had chest pain and ST-T changes at admission.
As a result, our study has demonstrated that NO levels might be related with myocardial injury developed in patients with NSTE-ACS. Moreover, NO levels were related with high vascular risks such as impaired TIMI flow and presence of coronary thrombus, rather than the severity of coronary artery disease. This shows that NO may be a proper target in the treatment of high-risk NSTE-ACS patients with increased Tn-I levels.
References
Hamm CW, Ravkilde J, Gerhardt W et al (1992) The prognostic value of serum troponin T in unstable angina. N Engl J Med 327:146–150
Antman EM, Tanasijevic MJ, Thompson B et al (1996) Cardiac specific troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med 335:1342–1349
Benamer H, Steg PG, Benessiano J et al (1999) Elevated cardiac troponin I predicts a high risk angiographic anatomy of the culprit lesion in unstable angina. Am Heart J 137:815–820
Okamatsu K, Takano M, Sakai S et al (2004) Elevated troponin T levels and lesion characteristics in non-ST-elevation acute coronary syndromes. Circulation 109:465–470
Hamm CW, Braunwald E (2000) A classification of unstable angina revisited. Circulation 102:118–122
Topol EJ, Yadav JS (2000) Recognition of the importance of embolization in atherosclerotic vascular disease. Circulation 101:570–580
Vane JR, Anggard EE, Botting RM (1990) Regulatory functions of the vascular endothelium. N Engl J Med 323:27–36
Keh D, Thieme A, Kurer I, Falke KJ, Gerlach H (2003) Inactivation of platelet glycoprotein IIb/IIIa receptor by nitric oxide donor 3-morpholino-sydnonimine. Blood Coagul Fibrinolysis 14:327–334
Freedman JE, Ting B, Hankin B, Loscalzo J, Keaney JF Jr, Vita JA (1998) Impaired platelet production of nitric oxide predicts presence of acute coronary syndromes. Circulation 98:1481–1486
Diodati JG, Dakak N, Gilligan DM, Quyyumi AA (1998) Effect of atherosclerosis on endothelium-dependent inhibition of platelet activation in humans. Circulation 98:17–24
Green LC, Wagner DA, Glogowski J, Skipper PL, Wishnok JS, Tannenbaum SR (1982) Analysis of nitrate, nitrite, and (15N) nitrate in biological fluids. Anal Biochem 126:131–138
Ambrose JA, Israel DH (1991) Angiography in unstable angina. Am J Cardiol 68:78B–84B
Lindahl B, Diderholm E, Lagerqvist B, Venge P, Wallentin L; FRISC II (Fast Revascularization during InStability in CAD) Investigators (2001) Mechanisms behind the prognostic value of troponin T in unstable coronary artery disease: a FRISC II substudy. J Am Coll Cardiol 38:979–986
Heeschen C, van Den Brand MJ, Hamm CW, Simoons ML (1999) Angiographic findings in patients with refractory unstable angina according to troponin T status. Circulation 100:1509–1514
Lehrke S, Giannitsis E, Katus HA (2004) Admission troponin T, advanced age and male gender identify patients with improved myocardial tissue perfusion after abciximab administration for ST-segment elevation myocardial infarction. Thromb Haemost 92:1214–1220
Hamm CW, Heeschen C, Goldmann B et al (1999) Benefit of abciximab in patients with refractory unstable angina in relation to serum troponin T levels. c7E3 Fab Antiplatelet Therapy in Unstable Refractory Angina (CAPTURE) Study Investigators, N Engl J Med 340:1623–1629
Newby LK, Ohman EM, Christenson RH et al (2001) Benefit of glycoprotein IIb/IIIa inhibition in patients with acute coronary syndromes and troponin T-positive status: the paragon-B troponin T substudy. Circulation 103:2891–2896
Corseaux D, Ollivier V, Fontaine V et al (2002) Hemostasis imbalance in experimental hypertension. Mol Med 8:169–178
Willoughby SR, Stewart S, Holmes AS, Chirkov YY, Horowitz JD (2005) Platelet nitric oxide responsiveness: a novel prognostic marker in acute coronary syndromes. Arterioscler Thromb Vasc Biol 25:2661–2666
Stoupakis G, Orlando J, Kalia H, Skurnick J, Saric M, Arora R (2003) Preservation of myocardial microcirculation during mechanical reperfusion for myocardial ischemia with either abciximab or eptifibatide. J Invasive Cardiol 15:476–480
Davani S, Yan Y, Bouhaddi M et al (2002) Effects of nitric oxide on cardioprotection prior to ischemia-reperfusion. Therapie 57:157–162
Pinelli A, Trivulzio S, Tomasoni L, Bertolini B, Brenna S, Bonacina E (2002) Cardiac necrosis markers associated with low nitric oxide levels in the plasma of rabbits after treatment with vasopressin: protective effects of nitroglycerin administration. Pharmacol Res 45:427–434
Kita Y, Ozaki R, Sakai S et al (1994) Antianginal effects of FK409, a new spontaneous NO releaser. Br J Pharmacol 113:1137–1140
Ishii H, Ichimiya S, Kanashiro M et al (2005) Impact of a single intravenous administration of nicorandil before reperfusion in patients with ST-segment-elevation myocardial infarction. Circulation 112:1284–1288
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yazici, M., Demircan, S. & Durna, K. Association between nitric oxide levels on myocardial injury in non-ST elevation acute coronary syndromes. J Thromb Thrombolysis 24, 145–151 (2007). https://doi.org/10.1007/s11239-007-0039-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11239-007-0039-3