
Abstract
Family affluence plays a crucial role in adolescent well-being and is potential source of health inequalities. There are scarce research findings in this area from a cross-national perspective. This study introduces several methods for measuring family affluence inequality in adolescent life satisfaction (LS) and assesses its relationship with macro-level indices. The data (N = 192,718) were collected in 2013/2014 in 39 European countries, Canada, and Israel, according to the methodology of the cross-national Health Behavior in School-aged Children study. The 11-, 13- and 15-year olds were surveyed by means of self-report anonymous questionnaires. Fifteen methods controlling for confounders were tested to measure social inequality in adolescent LS. In each country, all measures indicated that adolescent from more affluent families showed higher satisfaction with their life than did those from less affluent families. According to the Poisson regression estimations, for instance, the lowest inequality in LS was found among adolescents in Malta, while the highest inequality in LS was found among adolescents in Hungary. The ratio between the mean values of LS score at the extreme highest and lowest family affluence levels (Relative Index of Inequality) derived from the regression-based models distinguished for its positive correlation with the Gini index, and negative correlation with Gross National Income, Human Development Index and the mean Overall Life Satisfaction score. The measure allows in-depth exploration of the interplay between individual and macro-socioeconomic factors affecting adolescent well-being from a cross-national perspective.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
Family socioeconomic status (SES) including family affluence plays a crucial role in young people’s well-being and has a great impact on the development of their personality and aspirations. There is evidence that the richer, wealthier or higher SES of the family provides better health and well-being among children and adolescents (Levin et al. 2011; Viner et al. 2012). Differences in family SES across social groups and populations are a potential source of social inequalities in both health and quality of life (QoL) among young people (Koster et al. 2005; Hanson and Chen 2007; WHO 2010), this being of a major concern for public health and social policies in each country (Hosseinpoor et al. 2015).
Recent scientific literature extensively develops concepts and theory on social inequalities in health (Bartley 2004; Arcaya et al. 2015; Alonge and Peters 2015), however, findings are mostly based on research with adult populations (Mackenbach et al. 2008; Hosseinpoor et al. 2012; Choi et al. 2015). The effect of within country income inequality on adult QoL and well-being has also been analyzed (Diener and Biswas-Diener 2002; Schütte et al. 2014). It was found that adult life satisfaction (LS) is dependent on income level, which allows for basic needs to be met. From a cross-national perspective, it was demonstrated that national income was a greater predictor of individual LS among adults (Schyns 2002). As for children and young people, the data on social disparities in health, LS or QoL is clearly lacking and this population has received considerably less attention in the literature (Levin et al. 2011). Thus, it is useful to examine whether the findings from previous studies in adulthood may also apply to young people.
Socioeconomic inequalities in health and health behaviors during adolescence is one of the foci of the cross-national study Health Behavior in School-aged Children (HBSC) which involves a wide network of researchers from more than 40 countries and regions (HBSC 2017). The previous editions of the study have highlighted the effect of socioeconomic differences on the way young people grow and develop (Currie et al. 2012; Inchley et al. 2016). A significant positive association between LS and family affluence was found for both genders in nearly all participating countries and regions.
The existence of social inequality in adolescent health depends on the age-appropriate measure of family socioeconomic conditions, in addition to its numerical account depending on the method for evaluating the extent of social inequality (Spencer 2006). The Family Affluence Scale (FAS) is a measure that has been proposed in the HBSC framework; it has been demonstrated as a valid indicator for evaluating the socioeconomic position of the adolescents in cross-national surveys (Currie et al. 2008; Torsheim et al. 2016). The scale includes items on common material assets or activities of the adolescent family (HBSC 2013) (see more in Methods). However, the lack of an appropriate method for assessing socioeconomic inequalities in adolescent health is the principal cause of the lack of consensus in the literature of how health inequalities manifest within and between countries. Moreover, the lack of a valid method for measure socioeconomic inequalities in adolescents could cause these disparities to be underestimated (Alonge and Peters 2015; Elgar et al.2016). In this context, although some cut-off points have been suggested in order to classify groups in three categories (low-, mid- and high-level material wealth), due to the differences among the FAS distribution across countries a new method for employing the scale is being developed. As it was employed in the last HBSC report (Inchley et al. 2016), groups are created now by using ridit-scores, selecting the 20% of the population with the lowest scores as the group with low affluence, and the 20% of the population with the highest scores as the group with high family affluence in each country. The population with scores in the middle 60% of the distribution is considered as the group with medium affluence. The range in health outcome distribution between high and low-affluence groups was only used to measure the extent of health inequality, while its statistical significance was based on linear trends across all three family affluence groups. Although this common approach is simple to interpret and does not require any strong assumption about the distribution of the health measure or its measurement scale (the range approach), it is limited to exploring causal models of health inequalities given that it omits intermediate groups when there are more than two groups (Wagstaff et al. 1991; Alonge and Peters 2015). In addition, it does not account for the sample size of the groups. Finally, using a measure within two marginal groups of the population may not reflect health inequalities in relation to country’s income inequality and welfare benefits (Schyns 2002; Bartley 2004; Spinakis et al. 2011).
Furthermore, family structure and other factors may be potential confounders of the relationship between family affluence and LS among children and adolescents (Levin et al. 2011). Indeed, Burton and Phipps (2010) found positive association between family income and young teen happiness. The influence of gender in LS has been widely evidenced too. For example, gender has been found to be a predictor of adolescent LS, with boys more likely to show high LS (Reiss 2013; Moksnes and Espnes 2013; Klanšček et al. 2014). Along the same lines, previous findings have shown that older adolescents tend to report lower life satisfaction (Goldbeck et al. 2007). This drawback may disappear if the model is rigorously adjusted for confounders to assess health inequalities between family affluence groups.
Several analyses of the HBSC data, using a multilevel approach, have shown the existence of cross-national variation in the relationship between family affluence and adolescent LS (Levin et al. 2011). Such analyses have also highlighted the importance of identifying and addressing country-level socioeconomic factors during adolescence. These findings suggest a possible relationship between social inequality in LS among adolescents and socioeconomic indices in a cross-national perspective. However, cross-national research in the field, especially with adolescent populations, is still scant and limited by measurement problems. Since the last HBSC report (Inchley et al. 2016) there have been no further attempts to compare adolescent health inequalities in detail. It is surprising that so little attention has been paid to the question of how social inequality is best measured among adolescents.
To overcome these shortcomings, our research has focused on adopting a broader concept of measuring and evaluating social inequalities in health (Wagstaff et al. 1991). Until recently, the two approaches to measuring health inequality are regression-based measures (e.g. the Slope Index) and aggregate measures (e.g. Health Concentration Index) (Wagstaff et al 1991; Kunst and Mackebach 1995; Mackenbach and Kunst 1997; Regidor 2004a, b). Therefore, there is little experience in adopting these approaches for assessing social inequalities in adolescent health (Due et al. 2009). Indeed, to date none have compared different health inequality measures with respect to correlations between their accounts and country-level socioeconomic indicators across adolescent samples.
The aim of our study is twofold:
-
1.
To compare socioeconomic inequality in adolescent LS across countries employing different measures.
-
2.
To determine the correlations between outcomes of tested measures and country level socioeconomic indices (e.g. Gross National Income, Gini index, etc.).
2 Data and Methods
2.1 Subjects and Study Design
The data presented here were obtained from the Health Behavior in School-aged Children (HBSC) study, a cross-national survey with support from the World Health Organization (WHO, Europe) which was completed in 2013/2014 in 42 countries, including 40 European countries and regions (considered alone as countries, i.e. England, Scotland and Wales), Canada, and Israel. More detailed background information about the study is provided in its international report (Inchley et al. 2016) and website: www.hbsc.org (HBSC 2017).
The population selected for sampling was 11-, 13- and 15-year old adolescents. Participants were selected using a clustered hierarchical sampling design, where the initial sampling unit was the school class. Data collection methods ensured that the samples of students were representative by age and gender. Specifically, the analyses presented here are based on the total number of 192,718 individual records (children with valid LS and FAS) obtained from 41 countries via HBSC Data Centre (Bergen University, Norway). Table 1 indicates the samples by countries (Armenia was excluded from the analysis due to deviance in FAS assessment).
The data were collected by means of self-report standardized questionnaires. The surveys were administrated in school classrooms ensuring students’ confidentiality. Response rates at the school, class and student level exceed 80% in the majority of countries (Inchley et al. 2016).
The study conformed to the principles outlined in the Declaration of Helsinki. National and local educational institutions agreed upon the study protocol. Ethical approval was obtained for each national survey according to the national guidance and regulations at the time of data collection. Researchers strictly followed the standardized international research protocol to ensure consistency in survey instruments, data collection and processing procedures (HBSC 2013).
2.2 Measures
At the individual level, the outcome variable was LS, and the explanatory variables were family FAS, family structure, gender and age. The analysis was stratified by country.
Students’ LS was rated using the measurement technique known as the Cantril (1965) ladder. They were asked to take a look at the drawn ladder, with steps numbered from zero (“0”) at the bottom to ten (“10”) at the top, with the instruction to suppose the top of the ladder represents the best possible life, and the bottom of the ladder represents the worst possible life. Respondents were asked to indicate the step of the ladder at which they would place their lives at present. Thus, the response was scored from 0 to 10 (an ordinary variable y), which was also dichotomized into a binary variable Y with codes: Y = 0 for LS score ≤ 5 (low LS), and Y = 1 for LS score > 5 (high LS). Both ordinary and binary variables were used as an outcome variable in the models of health inequality measure. In addition, their inverses (z = 10 − y, and Z = 0 for LS score > 5 (high LS) and Z = 1 for LS score ≤ 5 (low LS)) were used in regression-based models in order to adopt the Poisson and negative binomial distributions. On average, the proportion of missing cases for LS was 3.7%.
Family wealth was measured by the Family Affluence Scale (FAS), which was specially developed for the international nature of the HBSC study (Currie et al. 2008; Torsheim et al. 2016). The scale is simple and easy to answer even for young adolescents. FAS includes six questions with answers (assignment of points shown in parentheses): Does your family own a car, van or truck? “no” (0), “yes one” (1), “yes two or more” (2); Do you have your bedroom for yourself? “no” (0), “yes (1)”; During the past 12 months, how many times did you travel away on holiday (vacation) with your family? “not at all” (0), “once” (1), “twice” (2), “more than twice” (3); How many computers does your family own? “none” (0), “one” (1), “two” (2), “more than two” (3); How many bathrooms (room with a bath/shower or both) are in your home? “none” (0), “one” (1), “two” (2), “tree or more” (3); Does your family have a dishwasher at home? “no” (0), “yes” (1). A FAS score was calculated by summing the points to these six questions. Because the groups of respondents scored by 0–2 points and by 12–13 points were small they were combined into the FAS = 1 group and the FAS = 11 group, respectively. The groups of respondents scored from 3 to 11 points were assigned to groups FAS = 2 through FAS = 10, correspondingly. On average the proportion of missing cases in the total sample for FAS was 8.3% (for details see Online Resource 1).
To identify family structure, respondents were given a checklist to mark the people living in their home. Respondents were coded as living with “Both parents” (1) if both the mother and father were ticked in a checklist, “Not both parents” (2) in all other cases.
At the country level, we used the indices reported in the Human Development Report (2015). Data referring to the year 2014 were compiled. The Gini coefficient served as an indicator of country-level economic inequality. The coefficient reflects the distribution of income among the population and varies between 0 (perfectly equal distribution) and 100 (the worst inequality of incomes). The Gross National Income (GNI) per capita served as a measure of economic level of each country (GNI in US dollars is calculated according to the World Bank Atlas method of conversion from national currency to US dollar terms). The Human Development Index (HDI) was employed as a summary measure of human development. It measures the average achievements in a country in three basic dimensions of human development: a long and healthy life, access to knowledge, and a decent standard of living. And finally, we used the Overall Life Satisfaction (OLS) mean score based on the responses of adult population (ages 15 and older) to a question about satisfaction with freedom of choice and life in a Gallup World Poll (the survey question is identical to the HBSC study). The same values of indices have been used for the two Belgian regions and the numbers for the United Kingdom have been assigned to England, Scotland and Wales. None of these indices were available for Greenland and Gini index was not found for Malta, leaving these countries out of analyses that include country level indices.
2.3 Statistical Analysis and Methods of the Measurement of Social Inequality
All analyses were performed with SPSS (version 20.0; SPSS Inc, Chicago, IL, 2010). Descriptive statistics (means and proportions with 95% confidence interval—95% CI) were estimated by country. Associations between country-level assessments were estimated using Spearman correlation coefficient ρ; p < 0.05 was considered statistically significant.
Two data files were used in analysis. The first file included 192,718 individual records from all countries. The second file (Online Resource 1) included 42 records, which represented aggregated data by 41 countries, and grand totals, which were estimated from individual records weighting them by the country sample size. The data of files were merged by country and FAS group if necessary to update individual records with aggregated variables (e.g. midpoints of FAS distribution).
In order to select appropriate methods for assessing inequality on adolescent LS the following requirements for each measure were taken into account:
-
1.
Incorporation of the actual sample size of each FAS category.
-
2.
Obtaining a statistical model with the appropriate goodness of fit.
-
3.
Adjustment for possible confounders.
-
4.
Estimation of statistical properties (average and variation) using standard SPSS procedures.
To fulfill the first requirement, the ordinal FAS measure was transformed into a continuous X variable scaled from 0 to 1, while incorporating appropriate population weights for each FAS category, as defined by Kunst and Mackenbach (1995). The FAS categories were ranked from lowest to highest; the weight of each category was proportional to its population size within a FAS scale category. The X variable was plotted on the horizontal axis representing the cumulative distribution of the population for each FAS category. Then, the dependent variable (e.g. y, Y or other) was plotted at the midpoint of each FAS group proportion range. The midpoints were calculated for each country separately and for the total sample as the ridit scores in the following way:
where ui (i = 1, 2, …, g) is a proportion of corresponding FAS group in the sample, and g is the number of FAS groups.
Then two types of summary statistics from the individual records data file were produced:
-
1.
Regression-based measures (models ‘R’), and
-
2.
Aggregate measures of dissimilarity of distributions (models ‘A’).
For the HBSC data, altogether 15 measures of social inequality in adolescent LS were chosen and tested. Table 2 presents models and measures that have been employed in the literature to date (Wagstaff et al. 1991; Spinakis et al. 2011; Regidor 2004a, b) and originally proposed by authors of the present study. Detailed description of the measures is presented in “Appendix”.
3 Results
The characteristics of samples by gender and family structure are outlined in Online Resource 1. In the total sample 48.8% of students were boys and 51.2% were girls. A negligible range between proportions of students’ gender was common in all countries, except Ireland for which the percentage of boys to girls (38.9 vs. 61.1%) was taken into account. Family structure distribution showed a wide variation across countries, ranging from 54.1% of adolescents living with both parents in Greenland to 93.2% in Albania (71.8% in the total sample).
With respect to countries, mean FAS ranged from 3.94 (95% CI 3.88; 4.00) in Albania to 8.80 (95% CI 8.74; 8.86) in Norway; its average in the total sample was 6.92 (95% CI 6.91; 6.93) (Table 1). The means of LS score ranged from 7.08 (95% CI 7.01; 7.14) in Belgium (Flemish) to 8.26 (95% CI 8.20; 8.31) in Republic of Moldova; the average in the total sample was 7.61 (95% CI 7.60; 7.62). The proportion of adolescents reporting high LS ranged from 79.9% (95% CI 78.8; 81.0) in Czech Republic to 93.2% (95% CI 92.5; 93.9) in Albania [85.8% in the total sample (95% CI 85.6; 85.9)]. Figure 1 shows the asymmetric negatively-skewed distribution of LS scores in the total sample (skewness = − 1.028).

Distribution of life satisfaction score in the total sample
There was a tendency for negative correlation at the country level between the means of FAS and that of the LS score (ρ = − 0.218; p = 0.172), while no correlation was found between mean of FAS score and proportions of high LS (ρ = 0.019; p = 0.908). In contrast, both correlations were positive in all countries at the individual level.
Midpoints of FAS were calculated for the total sample and for each country, reveling differences among countries. The extend of inequality in adolescent LS employing all the proposed models was assessed also for the total sample and for each of the 41 countries (see Online Resource 1). The impact of family affluence, family structure (living with both parents), gender, and age on adolescent LS was assessed by regression-based models comparing their goodness of fit. Results of this analysis revealed a dominant effect of family affluence over family structure, gender, and age, with these last variables also showing a significant effect on adolescent LS. In comparison with linear and logistic regression-based models, Poisson and negative binomial regression-based models had a much better goodness of fit (deviance value/df was closer to 1) regressing both LS score and bivariate LS. Results of this analysis in the total sample are shown in Table 3.
For every country, all proposed measures indicated that adolescents from more affluent families have higher life satisfaction in comparison with their peers from less affluent families. However, regarding the first objective of this study, results showed variation in the amount of inequalities found in LS between countries, with these results also depending on the measure employed for assessing FAS inequalities. For example, according to the Relative Index of Inequality (RII) of Poison regression for the LS score (Model R3) the lowest inequality in LS was found among adolescents in Malta (RII = 1.024; 95% CI 0.926; 1.134), while the highest inequality in LS was found among adolescents in Hungary (RII = 1.812; 95% CI 1.684; 1.950). However, countries were ordered differently by their values of calculated LS inequality depending on the measure of inequality employed. Table 4 shows average values of inequality in LS measured by 15 different methods and nominates three countries with the lowest and highest values of the corresponding measures. Among the countries with the lowest social inequality in LS, Malta was nominated in 13, Belgium (Fl.) and Netherlands in 11 of 15 measures. Among the countries with the highest social inequality in LS, Hungary was nominated in 13 of 15 measures providing the significantly highest assessments of proposed measures. Relatively high estimations of social inequality in LS were also revealed in samples of students from Israel and the Republic of Moldova. For each country and in the total sample, the statistical estimations of family affluence inequality in adolescent LS, measured by 15 different methods, are presented in Online Resource 1.
At the country level, the measures were positively correlated (data not presented). Most of Spearman correlation coefficients showed significance at the level p < 0.01. An exception was the Health Concentration Index (HCI), which had a weak correlation with other measures. The regression-based measures for LS scores, as well as regression-based measures for binary LS score, were highly correlated (ρ > 0.9) within their groups, meaning that these indicators perform an almost identical role in the measurement of inequality.
The second goal of the present study was to examine the relationship between different measures of social inequality in adolescent LS and several country-level socioeconomic indices. For this purpose, four macro-level indices were chosen (the Gini coefficient, GNI, HDI, and OLS mean score), whose data were made available for HBSC participating countries. Table 5 shows the correlation between these indices and proposed measures of health inequality that were calculated at the country level. Any of the proposed measures of inequalities in LS showed a positive correlation with the Gini index, although there were no significant estimations of Spearman correlation. In addition, the proposed measures showed significant negative correlations with GNI, HDI, and OLS mean scores with the exception of HCI (Model A1), that showed a non-significant but positive correlation with GNI, HDI and OLS. In this respect, regression-based measures (models ‘R’) for LS scores demonstrated a noticeable correlation with macro-level indices. For instance, RII of Poisson regression for the LS score (Model R3) positively correlated with the Gini index (ρ = 0.100, p = 0.544), and negatively correlated with GNI (ρ = − 0.516, p = 0.001), HDI (ρ = − 0.495, p = 0.001) and OLS mean scores (ρ = − 0.404, p = 0.010). In contrast to the regression-based models, the range-based inequality measure (Model A5) did not correlate with country-level socioeconomic indices.
4 Discussion and Conclusion
Although cross-national variation in socioeconomic inequalities in LS among adults has been examined in many studies (Diener and Biswas-Diener 2002; Schyns 2002; Schütte et al. 2014), the literature to date in that field of research among adolescents is scarce (Levin et al. 2011). Thus the rationale of the present study was based on the need to get new insight into the social inequalities in adolescent LS across different countries. Within this context the aim of our study was twofold. Firstly, we sought to compare socioeconomic inequality in adolescent LS across countries employing different measures and controlling the effect of possible confounders (age, gender and family structure); and secondly, we examine if there were any correlations between outcomes of tested measures of LS inequalities among adolescents and country level socioeconomic indices (e.g. Gross National Income, Gini index, etc.).
The origin of the present study attempted to choose an appropriate method to measure social inequality in health and use it to measure family affluence inequality in LS among adolescents within data collected across HBSC countries (HBSC 2013; Inchley et al. 2016). Although numerous approaches and methods to measure inequality in health have been presented in literature (Wagstaff et al. 1991; Bartley 2004; Spinakis et al. 2011; Arcaya et al. 2015; Alonge and Peters 2015), little is known about their adequateness for application in specific cases. Thus, results responding the two research questions in this study were calculated using different approach for measuring FAS-based inequalities in order to compare the results obtained. As our data consisted of national samples, the main requirement for the selected methods was their adjustment for socioeconomic conditions and possible confounders.
Health inequalities are most frequently investigated with respect to the various socioeconomic groups that are formed in the society (Spinakis et al. 2011). This led several researchers to investigate inequalities using more sophisticated measures of inequality. The experts for measurement of health inequalities in the European Union have concluded that odds ratio (OR) of the logistic regression present the most adequate solution to the problem of measuring inequalities with respect to social categories (Spinakis et al. 2011). The well-known RII and SII are similar solutions that are also related to easy statistical modeling techniques (Kunst and Mackenbach 1995; Mackenbach and Kunst 1997). However, their application poses restrictions for linearity; otherwise, the magnitude of these indices would be biased (Regidor 2004b). Finally, there are some indices that are more known to the researchers involved in measuring inequalities in general (e.g. the HCI) (Wagstaff et al. 1991; Regidor 2004a, b). As suggested in much literature (Spinakis et al. 2011), different measures can give information about different aspects of health inequalities. The interpretation of health inequality can also be quite different, depending on the measure used. Several authors recommend that in order to have a fuller understanding of health inequalities, it is better to use more than one measure and combine their outcomes (Wagstaff et al. 1991; Spinakis et al. 2011). These findings highlight the importance of methodological issues in measuring social inequality in adolescent LS and in the exploration of the interplay between individual and macro-socioeconomic factors on adolescent well-being from the cross-national perspective.
The recent HBSC report (Inchley et al. 2016) has already applied a range-based measure to evaluate inequality in health behavior outcomes among adolescents by comparing two marginal family affluence groups in each of the countries. Due to a large variation of this summary statistic across countries, including analysis of inequalities in LS, we adjusted data for sample size of family affluence groups in each country. As recommended by Mackenbach and Kunst (1997), we used regression-based models for this purposes. Owing to the very asymmetric distribution of the LS variable, we applied a novel solution of adapting a negative binomial regression for the present study. In contrast with linear regression and logistic regression, the assessment of model goodness of fit confirmed the appropriateness of using this regression as well as the Poisson regression.
Several aggregate measures of health inequality were introduced as alternatives to the regression-based measures. In addition to the well-known measures, such as the HCI and range based, we introduced two new measures: difference between averages of the midpoints in groups of subjects with high LS and low LS (Model A2), and loss of positive cases due to health inequalities (Model A3). Although these two measures were based on common statistical approaches, their assessments across countries had a weak correlation with country-level socioeconomic indices, likely due to inadequate dichotomization of LS score.
As there were several possible confounders mediating the relationship between family affluence and LS, all proposed models of social inequality in health were adjusted for them. In the present study family structure, gender, and age were regarded as confounders. The prevalence and mediating influence of these variables differed cross-nationally (Inchley et al. 2016). The current study found that gender, age, and family structure defined inequalities in adolescent LS considerably, however in a smaller magnitude than family affluence. It was documented that gender has a moderating effect in the relationship between adult LS and income (Diener and Biswas-Diener 2002; Schyns 2002) and this was also observed among adolescents in analysis of relationship between family affluence and LS among boys and girls (Levin et al. 2011). Family structure also confounds the relationship, as missing at least one of the parents is more likely to result in lower family affluence. Even after adjusting models for gender, age, and family structure (living with both parents) we found a consistent inequality in LS related to different level of family affluence.
This study revealed a substantial variation in the strength of family affluence inequality in LS among adolescents across countries, however, this variance and ordered rank of countries differ by the inequality measure chosen. Most of all, the difference is seen when comparing the regression-based measures with aggregate measures, as well as when comparing the regression-based models for the LS score with those for the binary LS estimation. Theoretically, linear, Poisson, and negative binomial regression based measures should generate identical assessments, but this was not achieved due to the dissimilarity between real LS score distributions and corresponding theoretical distribution (e.g. the key assumption of linear regression is a normal distribution of at least the dependent variable, but our data did not fulfill this requirement; violence of requirements for linear regression is reflected by poor model goodness-of-fit).
Finally, our study examined if several methods of inequality measurements reveal different patterns of association between family affluence inequality in adolescent LS and country level socioeconomic indices. In this study we report that regression-based models for the ordinal LS score are relevant for measuring family affluence inequality in adolescent LS. The outcomes of these measures correlate with country-level socioeconomic indices, such as Gini index, GNI, HDI and OLS mean score. The measure based on Poisson regression model for LS score is the one that better shows this association. The use of the Poisson regression in the analysis of inequalities in health has been also justified in several other studies (Mackenbach and Kunst 1997; Mackenbach et al. 2008; Hosseinpoor et al. 2012).
In contrast to the models for the ordinal LS score, the measures of inequality with the models for the binary LS did not demonstrate an impressive correlation with country-level socioeconomic indices. This is also noted for the range-based inequality measure (Model A5) that was described in the HBSC report (Inchley et al. 2016). The failure of this model might be explained by inadequate dichotomization of the LS score, when too high of a proportion of subjects with high LS was provided. Indeed, further research is required to meet the challenge of optimizing the scaling of the LS score.
In our study we found a positive correlation between family affluence inequality in LS among adolescents and in the Gini index. Moreover, the results indicated higher inequality in those countries that had a more unequal income distribution of income. The negative correlation with GNI gives indication on higher inequality in poorer countries. These results resonate with the findings of a study by Levin et al. (2011) for the HBSC survey in 2006; they are also in line with the previous findings among adults (Diener and Biswas-Diener 2002; Schyns 2002). Our study, in addition to the findings described in the above references, revealed that inequality under consideration also had a relationship with summary country-level statistics like the HDI, as well as with responses of adult population to the identical question about LS. We note that family affluence inequality in adolescent LS had a reduced magnitude in countries with declared a higher HDI and OLS mean score.
4.1 Limitations
We hereby note two kinds of limitations of this study.
The limitations of the first kind are related to the survey methodology. There are differences between countries in various aspects of data collection, and some of these might affect the size of inequalities in health and LS. The main concern was the family affluence assessment, which was constructed by students’ self-reported items that are sensitive to the cultural and structural surroundings. Some studies have shown, however, that the FAS, that was used in our study, is a reliable measure among adolescents and is recommended in studies on health inequalities (Boyce et al. 2006; Torsheim et al. 2016).
The limitations of the second kind are related to the data processing and analysis of the relationship between individual LS, family affluence, and country-level socioeconomic indices, in particular. While data are available from many countries, the most appropriate approach for the analysis of such relationships might be the multilevel modeling, such as those demonstrated in other studies (Due et al. 2009; Levin et al. 2011). In the present study we did not use the multilevel modeling because of specific objectives in our study. Future work is recommended to examine potential mediators in order to identify groups of adolescents with the highest social inequality in LS.
4.2 Conclusions
This study revealed a substantial variation of the magnitude of family affluence inequality in adolescent LS across countries. However, the variance and ordered rank of countries varied also by the inequality measurement chosen. We suggested that regression-based measures (e.g. the Poisson regression-based model) for LS scores are the most suitable for assessment of family affluence inequality in adolescent LS. Our findings indicate the need for continued research about social inequalities in adolescent health, and particularly in the exploration of the interplay between individual and macro-socioeconomic factors on adolescents’ well-being from the cross-national perspective. Research in this field is considered to be crucial for adolescent health by all policy planners.
References
Alonge, O., & Peters, D. H. (2015). Utility and limitations of measures of health inequities: a theoretical perspective. Global Health Action, 8, 27591.
Arcaya, M. C., Arcaya, A. L., & Subramanian, S. V. (2015). Inequalities in health: Definitions, concepts, and theories. Global Health Action, 8, 27106.
Bartley, M. (2004). Health inequality: An introduction to theories, concepts and methods. Cambridge: Polity Press.
Boyce, W., Torsheim, T., Currie, C., & Zambon, A. (2006). The Family Affluence Scale as a measure of national wealth: Validation of an adolescent self-report measure. Social Indicators Research, 78(3), 473–487.
Burton, P., & Phipps, S. (2010). From a young teen’s perspective: Income and the happiness of Canadian 12 to 15 Year olds. http://myweb.dal.ca/phipps/Happy_Teens.pdf. Accessed 1 March 2017.
Cantril, H. (1965). The pattern of human concern. New Jersey: Rutgers University Press.
Choi, H., Burgard, S., Elo, I. T., & Heisler, M. (2015). Are older adults living in more equal counties healthier than older adults living in more unequal counties? A propensity score matching approach. Social Science and Medicine, 141(9), 82–90.
Currie, C., Molcho, M., Boyce, W., Holstein, B., Torsheim, T., & Richter, M. (2008). Researching health inequalities in adolescents: The development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Social Science and Medicine, 66(6), 1429–1436.
Currie, C., Zanotti, C., Morgan, A., Currie, D., de Looze, M., Roberts, C., et al. (Eds.) (2012). Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) Study: International Report from the 2009/2010 Survey. Copenhagen: World Health Organization Regional Office for Europe. (Health Policy for Children and Adolescents, No. 6).
Devaux, M., & Sassi, F. (2013). Social inequalities in obesity and overweight in 11 OECD countries. European Journal of Public Health, 23(3), 464–469.
Diener, E., & Biswas-Diener, R. (2002). Will money increase subjective well-being? Social Indicators Research, 57(2), 119–169.
Due, P., Damsgaard, M. T., Rasmussen, M., Holstein, B. E., Wardle, J., Merlo, J., et al. (2009). Socioeconomic position, macroeconomic environment and overweight among adolescents in 35 countries. International Journal of Obesity, 33(10), 1084–1093.
Elgar, F. J., McKinnon, B., Torsheim, T., Schnohr, C. W., Mazur, J., Cavallo, F., et al. (2016). Patterns of socioeconomic inequality in adolescent health differ according to the measure of socioeconomic position. Social Indicators Research, 127(3), 1169–1180.
Goldbeck, L., Schmitz, T. G., Besier, T., Herschbach, P., & Henrich, G. (2007). Life satisfaction decreases during adolescence. Quality of Life Research, 16(6), 969–979.
Hanson, M. D., & Chen, E. (2007). Socioeconomic status and health behaviors in adolescence: A review of the literature. Journal of Behavioral Medicine, 30(3), 263–285.
Hayes, L. J., & Berry, G. (2002). Sampling variability of the Kunst–Mackenbach relative index of inequality. Journal of Epidemiology and Community Health, 56(10), 762–765.
HBSC (2013). Health behaviour in school-aged children study: A World Health Organization Cross-National study. Internal Research Protocol for the 2013/2014 Survey. Scotland: University of St. Andrews. https://sites.google.com/a/hbsc.org/members/documents/protocols/2013-2014_internalprotocol. Accessed 1 March 2017.
HBSC (2017). Health behaviour in school-aged children: World Health Organization Collaborative Cross-national survey. http://www.hbsc.org. Accessed 1 March 2017.
HDR (2015). Human development report 2015: Work for human development. http://hdr.undp.org/sites/default/files/hdr_2015_statistical_annex.pdf. Accessed 1 March 2017.
Hosseinpoor, A. R., Bergen, N., & Schlotheuber, A. (2015). Promoting health equity: WHO health inequality monitoring at global and national levels. Global Health Action. https://doi.org/10.3402/gha.v8.29034.
Hosseinpoor, A. R., Stewart Williams, J. A., Itani, L., & Chatterji, S. (2012). Socioeconomic inequality in domains of health: Results from the World Health Surveys. BMC Public Health, 12, 198.
Inchley, J., Currie, D., Young, T., Samdal, O., Torsheim, T., Augustson, L., et al. (Eds.) (2016). Growing up unequal: gender and socioeconomic differences in young people‘s health and well-being. Health Behaviour in School-aged Children (HBSC) study: International report from the 2013/2014 survey. Copenhagen: World Health Organization Regional Office for Europe. (Health Policy for Children and Adolescents, No. 7).
Klanšček, H. J., Ziberna, J., Korošec, A., Zurc, J., & Albreht, T. (2014). Mental health inequalities in Slovenian 15-year-old adolescents explained by personal social position and family socioeconomic status. International Journal for Equity in Health, 13, 26.
Koster, A., Bosma, H., van Lenthe, F. J., Kempen, G. I., Mackenbach, J. P., & van Eijk, J. T. (2005). The role of psychosocial factors in explaining socio-economic differences in mobility decline in a chronically ill population: Results from the GLOBE study. Social Science and Medicine, 61(1), 123–132.
Kunst, A. E., & Mackenbach, J. P. (1995). Measuring socio-economic inequalities in health. Copenhagen: World Health Organisation.
Levin, K. A., Torsheim, T., Vollebergh, W., Richter, M., Davies, C. A., Schnohr, C. W., et al. (2011). National income and income inequality, family affluence and life satisfaction among 13 year old boys and girls: a multilevel study in 35 countries. Social Indicators Research, 104(2), 179–194.
Mackenbach, J. P., & Kunst, A. E. (1997). Measuring the magnitude of socio-economic inequalities in health: An overview of available measures illustrated with two examples from Europe. Social Science and Medicine, 44(6), 757–771.
Mackenbach, J. P., Stirbu, I., Roskam, A. J., Schaap, M. M., Menvielle, G., Leinsalu, M., et al. (2008). Socioeconomic inequalities in health in 22 European countries. The New England Journal of Medicine, 358(23), 2468–2481.
Moksnes, U. K., & Espnes, G. A. (2013). Self-esteem and life satisfaction in adolescents-gender and age as potential moderators. Quality of Life Research, 22(10), 2921–2928.
Moreno-Betancur, M., Latouche, A., Menvielle, G., Kunst, A.E., & Rey, G. (2015). eAppendix for “Relative index of inequality and slope index of inequality: A structured regression framework for estimation”. http://download.lww.com/wolterskluwer_vitalstream_com/PermaLink/EDE/A/EDE_2015_04_01_MORENOBETANCUR_EDE14-467_SDC1.pdf. Accessed 3 March 2017.
Regidor, E. (2004a). Measures of health inequalities: Part 1. Journal of Epidemiology and Community Health, 58(10), 858–861.
Regidor, E. (2004b). Measures of health inequalities: Part 2. Journal of Epidemiology and Community Health, 58(11), 900–903.
Reiss, F. (2013). Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Social Science and Medicine, 90(1), 24–31.
Schütte, S., Chastang, J. F., Parent-Thirion, A., Vermeylen, G., & Niedhammer, I. (2014). Social inequalities in psychological well-being: A European comparison. Community Mental Health Journal, 50(8), 987–990.
Schyns, P. (2002). Wealth of nations, individual income and life satisfaction in 42 countries: A multilevel approach. Social Indicators Research, 60(1/3), 5–40.
Spencer, N. J. (2006). Social equalization in youth: Evidence from a cross-sectional British survey. European Journal of Public Health, 16(4), 368–375.
Spinakis, A., Anastasiou, G., Panousis, V., Spiliopoulos, K., Palaiologou, S., & Yfantopoulos, J. (2011). Expert review and proposals for measurement of health inequalities in the European Union–Full Report. European Commission Directorate General for Health and Consumers. Luxembourg. http://ec.europa.eu/health//sites/health/files/social_determinants/docs/full_quantos_en.pdf. Accessed 1 March 2017.
Torsheim, T., Cavallo, F., Levin, K. A., Schnohr, C., Mazur, J., Niclasen, B., et al. (2016). Psychometric validation of the Revised Family Affluence Scale: A latent variable approach. Child Indicators Research, 9(3), 771–784.
Viner, R. M., Ozer, E. M., Denny, S., Marmot, M., Resnick, M., Fatusi, A., et al. (2012). Adolescence and the social determinants of health. Lancet, 379(9826), 1641–1652.
Wagstaff, A., Paci, P., & van Doorslaer, E. (1991). On the measurement of inequalities in health. Social Science and Medicine, 33(5), 545–557.
WHO (2010). Environment and health risks: A review of the influence and effects of social inequalities. Mickey Leland Center for Environment Justice and Sustainability. http://www.euro.who.int/__data/assets/pdf_file/0003/78069/E93670.pdf?ua=1. Accessed 1 March 2017.
Acknowledgements
The HBSC study is an international study carried out in collaboration with WHO Europe. The international coordinator of the 2013–2014 survey was Professor Candace Currie from the University of St. Endriews, United Kingdom, and the international databank manager was Professor Oddrun Samdal from Bergen University, Norway. The HBSC survey was the personal responsibility of principal investigators in each of the 41 countries.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix
Appendix
Regression-based measures We considered eight regression-based models to measure inequality in adolescent LS. They measure absolute and relative differences in the estimation of the outcome variable at the extreme values of FAS. Four models explored the relationship between LS score and FAS, while the remaining four models examined the prevalence of low and high LS (dichotomized LS score) across 11 FAS group midpoints. All models were adjusted for gender, age and family structure variables (equations presented below omit these variables).
Model R1 was based on the linear regression for the mean value of LS score:
where X represents midpoints of FAS in the scale of cumulative distribution ranging from 0 to 1, α is the intercept (mean value of LS score at the extreme lowest hypothetical FAS (at X = 0), and β denotes the regression slope, which designated the Slope Index of Inequality (SII). Specifically, the SII is interpreted as the average increase in mean LS score in the population ranked from the extreme lowest FAS group to the extreme highest FAS group. A positive SII indicates an increase in adolescent LS corresponding to an increase in family wealth. Kunst and Mackenbach (1995), Mackenbach and Kunst (1997) defined the Relative Index of Inequality (RII):
as a measure of the influence of socioeconomic status on a health index. In the present study, it estimates the ratio between the mean value of LS score at the extreme highest FAS level (at X = 1) and at the extreme lowest FAS (at X = 0).
To calculate RII instead of the formula (1) we used the identity derived by Moreno-Batancure et al. (2015):
where \(\bar{y}\) is an average of LS score, which is relatively less sensitive to adjusting for confounders than intercept α in formula (1). Confidence interval (CI) for the RII was calculated using the formulas defined by Hayes and Berry (2002).
Model R2 was based on the linear regression for the proportion of high LS in the population ranked from the lowest FAS group to the highest. This model is an analog of the Model R1, in which the LS score was replaced by a binary measure: Y = 0 (low LS), Y = 1 (high LS). This model has been used in the literature to measure inequalities in health, such as mortality, self-assessed health (Mackenbach et al. 2008) and overweight prevalence (Due et al 2009; Devax and Sassi 2013). The SII and RII were calculated with the same formulas used for the model R1. Here, RII represents the ratio between those reporting high LS at the top rank of FAS (at X = 1) and at rank zero (at X = 0).
As distributions of outcome variables (LS score or binary LS) might differ from a normal distribution, it is preferable to generate RII values and their 95% CI using the Poisson regression and, alternatively, negative binomial regression.
Model R3 was based on the Poisson regression, which is commonly used in epidemiology to analyze health outcomes in Poisson counts. In the present study, the model was as follows:
where X and \(\bar{y}\) correspond to the values in model R1, and A and b are the parameters of Poisson regression. Then, RII = exp(b). In this context, the model R3 is equivalent to the model R1, and the RII meaning is the same.
Model R4 was based on the Poisson regression for the proportion of high LS. This model is an analog of the model R3 for a binary variable: Y = 0 (low LS), Y = 1 (high LS).
Models R5 and R6 were based on the negative binomial regression for the mean value of the LS score and for the proportion of a high LS. Similarly, to the models R3 and R4, the same estimations were computed.
Model R7 was based on the ordinal logistic regression for LS score, which estimates the association between the odd of the ordinal LS score y and continuous X value:
where P(y > i) and P(y ≤ i) (i = 0, 1, …, 9) denote the probability of the LS greater than i scores and probability of the LS score equal or lower i scores, correspondingly, and X represents family affluence in the scale of FAS cumulative distribution. A measure of health inequality derived by this model is OR = exp (c). A positive c value (or OR > 1) predicts the amount of increase in ratio P(y > i)/P(y ≤ i) while family affluence changes from the extreme lowest level (at X = 0) to the extreme highest level (at X = 1).
Model R8 was based on the binary logistic regression for the high LS group. The model estimates the association between continuous X value and binary LS: Y = 0 (low LS), Y = 1 (high LS). A measure of health inequality derived from this model is OR = exp (B), where B is the coefficient for X in the binary logistic regression equation.
All regression-based measures were calculated using the SPSS Generalized Linear Models procedure, using the model goodness of fit by a deviance (value/df). In order to adopt Poisson and negative binomial distributions the procedure was run with the inverse LS score (z = 10 − y, or Z = 0 (high LS) and Z = 1 (low LS)) as a response variable and the transformation 1 – Xi as a covariate. The sampling variability estimations were obtained from the procedure.
The aggregate measures of dissimilarity of distributions were alternatives to the regression-based measures.
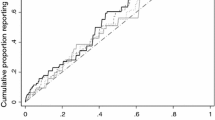
Model A1 The Health Concentration Index (HCI), or Concentration Index, has been widely used as a measure of income-related health inequality (Wagstaff et al. 1991; Regidor 2004b; Spinakis et al. 2011; Alonge and Peters 2015). The HCI is based on the concentration curve (as well as the Gini coefficient is based on Lorenz curve). The concentration curve plots the cumulative proportion of the population, value X as defined above, along the horizontal axis against the cumulative proportion of binary health measure (high life satisfaction) along the vertical axis. HCI is defined as twice the net area between the concentration curve and the diagonal (45o) line of equity. It is computed using the following formula:
where A denotes the net area between the concentration curve and the diagonal, AUC denotes the area under the concentration curve, yi is the cumulative proportion of the binary health measure in the ith FAS group, xi is the cumulative proportion of the population in the ith FAS group, and g is the number of FAS groups. Note that x0 = 0 and y0 = 0.
By definition (xi+1 – xi) = ni/N, the HCI may be calculated as
where \(\bar{t}\) is the mean of a new created variable ti = (yi+1 + yi)/2, N is the total number of subjects, and ni is the number of subjects within the ith FAS group. The marginal mean value \(\bar{t}\) and its variance were estimated by evaluating a General Linear Model (Univariate) while adjusting data for gender and family structure.
Model A2 This model estimates the difference between averages of the midpoints in groups of subjects with high LS (Y = 1) and low LS (Y = 0). The model can be expressed using the following formula:
where Xi is a midpoint of the ith FAS group, and f(Xi/Y = 1) and f(Xi/Y = 0) denote the rate of ith FAS group among subjects with high LS (Y = 1) and among subjects with low LS (Y = 0), respectively. The adjusted ΔE value and its 95% CI were estimated from the SPSS procedure General Linear Model (Univariate) contrasting results on LS group.
Model A3 Model A3 estimates the loss of positive cases, e.g. subjects with high LS, due to inequalities. Let’s denote by hi the proportion of subjects with high LS in the ith FAS group. There is a great assumption that for the last g-th FAS group the proportion H = hg takes its maximal value among all FAS groups. Than the loss L can be defined as an average proportion of positive cases lost due to inequality:
The adjusted L value and its 95% confidence interval were estimated through a General Linear Model (Univariate) as a grand mean.
Models A4 and A5 represent a ‘classical’ approach in measuring health inequalities. This is the most frequently encountered measure of inequality in the literature on health inequalities (Alonge and Peters 2015). Its use typically involves comparing the health outcomes of the top and the bottom socioeconomic groups. Sometime this comparison is presented in the form of the range itself. For example, in the recent HBSC report (Inchley et al. 2016) two groups of respondents have been compared in each country/region. The first group included young people in the lowest 20% (low affluence), and the second group included those in the highest 20% (high affluence) of the ridit-based FAS score in the respective country/region. In the present study we calculated the range in LS score (Model A4) and the range in high LS rate (Model A5) between selected groups, adjusting data for gender and family structure. Calculations were carried out using the SPSS procedure General Linear Model (Univariate), contrasting results on FAS groups.
Rights and permissions
About this article

Cite this article
Zaborskis, A., Grincaite, M., Lenzi, M. et al. Social Inequality in Adolescent Life Satisfaction: Comparison of Measure Approaches and Correlation with Macro-level Indices in 41 Countries. Soc Indic Res 141, 1055–1079 (2019). https://doi.org/10.1007/s11205-018-1860-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-018-1860-0