
Abstract
This paper computes satisfied life expectancy at age 30 (LE30) and at age 65 (LE65) in order to assess inequality in longevity by gender and education level in Spain. We calculate abridged life tables and satisfied LE using conventional life tables and Sullivan’s method. Population and mortality records for 2012 from the Spanish National Institute of Statistics’ (INE) are combined with prevalences of life satisfaction using the 2013 European Union Statistics on Income and Living Conditions. Satisfaction was defined through a single question about life satisfaction on a scale of 0–10. Results show that the smoothed age-specific prevalences of satisfaction increased with higher education level for both genders. Generally, women tended to report higher levels of satisfaction than men. Spanish women also have a higher LE, regardless of education, but the gender gap is larger among the highest educated. Highly educated women are expected to live 7.3 years more than men at the age of 30. Differences in satisfied LE favor women over men at both ages. The higher the education level is, the largest the satisfied LE. Among the highly educated, women at 30 will live happily 7.5 years more than men. To our knowledge, this is the first study that estimates subjective LE according to education level in Spain. We conclude that even though people in Spain are living longer and healthier than ever before, health inequalities still persist as only those with high education attainments will spend more years feeling satisfied with their lives than unsatisfied.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Improving the well-being of a population by reducing inequalities across different socio-demographic groups is a social challenge in most of the developed countries worldwide. Well-being depicts the existence of good conditions of life characterized by health, happiness or prosperity. Therefore, health, happiness or welfare contributes to our general state of well-being. Recently, a growing number of publications on happiness and life satisfaction have come out, with several studies documenting who is happy and satisfied (Easterlin et al. 2010; Diener 2009; Kahneman et al. 1999; Koopmans et al. 2010; Hamplová 2018).
High levels of happiness might reduce mortality through several direct and indirect mechanisms, and therefore influence life expectancy. For instance, Koopmans et al. (2010) found that increased levels of happiness predicted a lower mortality rate, and therefore happier people lived longer. In general, lower levels of life satisfaction, or dissatisfaction, is associated with increased (disease) mortality or health problems (Mojon-Azzi and Sousa-Poza 2011; Koivumaa-Honkanen et al. 2000); therefore, higher levels of life satisfaction might be associated to living a longer and healthier life. Individuals with poor self-rated health, physical disabilities, depressive symptoms, and other common health conditions tend to report having lower levels of happiness than others (Strine et al. 2008). Being happy has also been associated with having lower incidence of chronic conditions (Siahpush et al. 2008). When looking at older ages, academic studies on this topic have shown that happiness starts declining at around age 70 (Gerstorf et al. 2010). Today, the length of life is higher than ever before, and the ‘long-lived’ population continues to grow rapidly in many countries thanks to mortality reductions, particularly among the elderly (Robine and Jagger 2017; Mathers et al. 2015). However, people’s longer life in developed countries is not always translated into healthier lives (Solé-Auró and Alcañiz 2015), and no clear international evidence exists about if those extra years of life may be accompanied with satisfied or unsatisfied years with life.
Moreover, the influence of educational gradient in life expectancy persists among socioeconomic groups (Mäki et al. 2013). Life expectancy has increased on average by three months per years over the past century. Nonetheless, this gain has been uneven across education groups. Jasilionis and Shkolnikov (2016) have attempted to provide an international overview on longevity across educational groups. They concluded that people with high levels of education, who generally show the highest life expectancy levels, have been the leading the way towards a lengthening of life for the remaining population groups. In addition, there are substantial gender differences in health. Women universally enjoy longer lives than men (Verbrugge 1984; Barford et al. 2006; Oksuzyan et al. 2008; Crimmins and Solé-Auró 2013), but men’s health status tend to be better than that of woman (Crimmins et al. 2011). Compared to women, men have been shown to have superior physical performance on handgrip and walking speed tests (Bohannon et al. 2006), fewer difficulties performing activities of daily living and instrumental activities of daily living (Palacios-Cena et al. 2012), and substantially lower levels of depression and deprived self-rated health (Crimmins et al. 2011; Oksuzyan et al. 2010).
Overall, the association between life expectancy and happiness across education groups is less explored in the literature. The aim of this paper is to contribute to this line of research by considering differences in satisfied life expectancy according to education level, and exploring whether there are any substantial gender differences in this association. We expect that those with higher education levels, who have been proved in general to live longer and in some cases healthier (Jasilionis and Shkolnikov 2016), would also live more satisfied with life. We use data for Spain, and several reasons justify the relevance of studying this research line in this country. First, in recent records, Spain had the fourth-highest life expectancy in the world (WHO 2016), and the highest healthy life expectancy among the EU-28 member states in 2012 (Eurostat 2015). Second, education levels of the Spanish population experienced an unprecedented increase since the mid-1990s. This raise was mainly due to the benefit from a comprehensive system of compulsory education until the age of 14 in 1970.Footnote 1 Nonetheless, differences in satisfied life expectancy according to education level has never been explored. Finally, we observe a gap in the literature regarding the association between subjective well-being, gender and education differences in Spain. So far, only one study has explored inequalities in longevity by education attainment in Spain (Martín et al. 2017), but it was focused on healthy LE at the age of 65, and we aim to explore satisfied life expectancy at ages 30 and 65 to advance the knowledge on wellbeing of populations.
1.1 How Does the Educational Gradient Influence on Health Inequalities?
Scholars have widely documented that health inequalities in Europe are associated with socioeconomic status. People with higher socioeconomic status experience longer lives, and they also have fewer health problems than those with lower status (Crimmins and Cambois 2003; Mäki et al. 2013). For instance, Cambois et al. (2016), using the global activity limitation indicator, have been found a disadvantage regarding health for the lower social classes compared to the rest of the population, while an advantage is found for the higher social classes (Cambois et al. 2016). Also, active aging is an important determinant; therefore, people with high levels of education tend to be considerably more active than those with lower levels of education (Erlinghagen and Hank 2006), and participation in social activities is beneficial for older people’s mental and physical health. Plus, engagement in social activities, which has been proved to be beneficial for older people’s health and subjective well-being (Han et al. 2017), appears to be larger among advanced aged people with high levels of education (Arpino and Solé-Auró 2019).
Moreover, in terms of health, women with low levels of education constitute the most disadvantaged group (Solé-Auró and Alcañiz 2016). Other researchers have documented declines in life expectancy experienced by low educated women (Montez et al. 2012; Olshansky et al. 2012). It may be that their health is worsening faster, compared to other educational groups, because of changes in their health behaviors (Montez et al. 2011; Ross and Mirowsky 2010).
1.2 Gender Differences in Subjective Well-Being
Research evidence of gender differences on subjective well-being has generated inconsistent findings. Some studies have demonstrated that women tend to be happier than men across geographic regions, although the size of the female advantage appears to be small (Arrosa and Gandelman 2016). Other works have shown that men are more satisfied with life or happier than women across all ages, but that the gender gap widens with age (Pinquart and Sörensen 2001). Research comparing countries across Europe indicates that mean levels of happiness are higher among women than among men in Western Europe (Arrosa and Gandelman 2016).
Past research on determinants of happiness suggested that male and females’ differences on level of happiness do not vanish when socioeconomic status is taken into account (Yang 2008). Considering happiness across the lifespan, studies that took a closer look into different life phases found that the beginning of life of women seems to be happier than the one for men, however it reverses and it ends less happy (Easterlin 2010). Authors have pointed at partnerships and family ties, rather than economic reasons, as possible explanation to these gender differences in happiness along the lifespan. Existing evidence suggests that women at middle adulthood tend to report higher levels of stress than men, which in turn may them feel less happy (Jacobs and Gerson 2004; Mattingly and Sayer 2006). In order to interpret these differences in men and women’s perceived stress and life satisfaction, some authors suggested that women’s increased participation in the labor market in combination with the persistence of traditional gender roles at home may be part of the broader explanation (Lozano et al. 2016; Mattingly and Sayer 2006).
Moreover, it is crucial to understand how gender differences in happiness may remain when measuring life expectancy in a happy or satisfied state. This conceptualization aims to denote a complete life evaluation rather than a specific domain in life (i.e.: work, work-life balance, marriage). For this reason, the study of satisfied life expectancy complements studies of gender disadvantages in the quality of life.
1.3 The Spanish Context: Life Expectancy, Healthy Life Expectancy, and Satisfaction with Life by Education Level
In Spain, life expectancy and healthy life expectancy for women at age 30 and at age 65 exceeds that for men (HMD 2017; EHLEIS 2015). Past research in this country has mainly focused on life or healthy life expectancy (Solé-Auró and Alcañiz 2015; Martín et al. 2017), and life expectancy according to the level of education (Requena 2017); however, as indicated above, our work aims to advance in the study of the determinants of people’s well-being by examining differences in satisfied life expectancy and its variation by gender according to education level.
Cuñado and Pérez de Gracia (2012) studied the impact of education on happiness in Spain and they found that in average women seem to be happier than men. However, the authors did not distinguish the sample by gender and education levels. Therefore, they cannot conclude whether Spanish women are happier than men for all levels or only for certain schooling attainments. Hence, with the current demographic trends Spain will continue to increase the share of the population in the older age ranges, therefore, it is crucial to understand how the expected lifecycles of the varying population subgroups are changing. Like healthy life expectancy, satisfied life expectancy is a summary measure of population well-being that combines data on the length and the quality of life (Robine 2006). Within this demographic context, we aim to contribute to the existing literature by stressing the importance of the influence of education on satisfaction and healthy wellbeing in a context of an aging population. Since living a prolonged life in good health conditions is a worldwide aim, we expect that having a more satisfied and healthier population will lead to reduced pressure on the public health system and identifying the most deprived groups will help policymakers for future policy designs.
1.4 Cross-National Differences in Subjective Well-Being According to Gender and Education Level
Concerns about quality of life, particularly in old age, have been investigated during the last decades in the social and behavioral sciences (Geroge 2006). Nowadays, the literature on subjective well-being is attracting more attention even among quantitative social scientist as we can take into account subjective indicators to better understand the well-being of our society.
Comparative studies conducted at population level have generated inconsistent findings on the question of whether national populations reporting higher levels of happiness also have longer and healthier lives (Danner et al. 2001). This no clear association between life expectancy and life satisfaction can be easily exemplified when comparing countries with high levels of life satisfaction (like the Netherlands and Ireland) with high and low levels of life expectancy, respectively.
There are different components, other than life expectancy, that can influence cross-country dissimilarities in happiness. Some of these variables that help to account for cross-country differences in happiness are population health (commonly measured by computing healthy life expectancies), the strength of social networks; personal freedom; social trust (measured by the public’s perception of corruption in government and business); and generosity (donating money to a charity) (Helliwell et al. 2018).
Regarding differences according to education, past studies showed that higher achievements are associated with a longer life: highly educated men and women tend to live longer than the less educated. In this context, cross-national differences are explained through variations in lifestyles and public expenses (OECD 2015). In general, higher education promotes, among other factors, a healthier lifestyle. In the European Union, higher education levels seem to particularly protect women from mortality, and females’ life expectancy was higher than males’ for those with greater education at all ages in Italy, Poland, Finland, Sweden and Norway (Corsini 2010). The same study showed that for Bulgaria, Estonia Hungary and Czech Republic, highly educated women’s life expectancy was notably different than other educational levels mostly at ages 50, 60 and 70. In Spain, the educational gap was found to be deeper among men than among women, but in general the higher the level of education attained, the lower the gap between men’s and women’s life expectancy (Requena 2017).”
2 Methods
2.1 Data
We combine data from the Spanish National Institute of Statistics (2012) and from European Union Statistics on Income and Living Conditions (EU-SILC 2013). The latter provides responses to the life satisfaction question from a large-scale national representative survey data, and it allows us to estimate prevalence-rated of satisfaction in Spain. The former gives us the population mortality rates, life tables and vital statistics for estimates of total life expectancy.
First, we use population records from the Spanish National Institute (INE) by five-year age groups for men and women in 2012. This institute publishes on its website (www.ine.es) figures of the populations resident in Spain every six months. We use data corresponding to July the 1st, 2012. Then, we calculate the proportion of three levels of education (low, medium and high) using INE’s statistics of education levels in 2012. Moreover, mortality rates by level of education was published by the Spanish Institute and it was distributed in January 2016 as the appendix of a public report. It aimed at explaining the statistic procedure that the Institute uses to assign the level of education to mortality rates.Footnote 2 This is the first time that INE assigned the level of education to the whole Spanish population.
Second, we estimate mortality rates by level of education using the Spanish National Registry of deaths. This information is provided by INE, and it is the result of three statistical questionnaires: (1) medical death certificate/statistical death register (CMD/BED), (2) Judicial Statistical Death Register (BEDJ), and (3) Statistical Bulletin of Infants who died within 24 h (BEP). Hence, for the deceased, education is derived through administrative data. We acknowledge that the use of death record-based reported information to assign the education level to the deceased may imply some limitations, since it could be over-estimated or under-estimated in some cases. However, the Spanish Statistical Office, in charge of this process, verifies the information, and ensures its credibility.
Mortality rates by level of education are calculated in the following way
Where dx represents the number of deaths by level of education, derived from INE statistics, occurring in 2012, and px represents the size of the population in which deaths occur also derived from INE registered population. “x” indicates the age in both cases, dx and px. We use a five-year age group, except for the final open-ended group of 80-plus.
Finally, the 2013 EU-SILC prevalences of life satisfaction by education level and five-year age groups are, therefore, extrapolated to the Spanish population data on the life table, using Sullivan’s method, to estimate the expected life years spent satisfied with life, which hereafter will be denoted as “satisfied life expectancy. Even though we are using two sources of data, happiness data from EU-SILC and mortality data from INE, the corresponding estimates are centered in 2012. In addition, the 2011 census data prevalence of the non-institutionalized proportions are taken into account. Sample data were weighted in all analyses to estimate the total Spanish adult population.
The two different data sources, mortality rates by level of education from INE and prevalences of life satisfaction by level of education from the EU-SILC data are combined using the Sullivan’s method (see more details below in the methodology section). Using this technique, we are able to compute life tables to estimate for each age, the probability of surviving and the remaining life expectancy in satisfied or unsatisfied states.
2.2 Measures
In our study, subjective well-being refers to an individual’s life satisfaction, measured through satisfaction with life.Footnote 3 The 2013 EU-SILC questionnaire asked respondents to evaluate their life satisfaction with the following question: “On a scale from 0 to 10 where 0 means not at all satisfied and 10 means fully satisfied, how satisfied are you with your current life?” As no standard criteria are available on an international basis, we dichotomized the responses as follows: those who rated their life satisfaction level as between eight and ten are coded as satisfied, while those who rated their life satisfaction level as between zero and seven are coded as less satisfied or unsatisfied.
Education serves here as an indicator of socioeconomic status due to different reasons. First, we argue that, contrary to occupation, education is more likely to remain constant during an adult lifespan. Second, it is also relatively well reported in questionnaires and survey data. Finally, other studies have shown that the likelihood of reverse causation is lower between education and health at older ages, than between income or occupation and health (Solé-Auró et al. 2015).
To compute the life tables, as stated above, we use data from INE to calculate the proportion of education within different education levels and 5 years age groups. We classify our respondents into three education groups using the level of education achieved based on the International Standard Classification of EducationFootnote 4: First, cases classified into “Low Education” corresponded to those with primary and lower secondary credentials as well as illiterate individuals, corresponding to codes from 1 to 4 in the original data source. Second, “Medium Education” category includes individuals with higher secondary credentials and vocational training, which are codes 5–8 provided by INE. Finally, “High Education” group corresponds to codes 9–12, and are those cases with university degrees at all levels, BA graduated, masters’ and Ph.D.).Footnote 5
2.3 Methodology
We first estimate life expectancy by level of education and gender for the year 2012. Age is top-coded in a big age group at 80-plus years in the EU-SILC, therefore our abridged life table closes up to this age. We calculate life expectancy at age 30 and 65 by computing the average number of years lived at 30 and 65 years old. As it has been stated above, life satisfaction prevalences and the standard errors by five years age groups and sex are obtained from the 2013 EU-SILC data.
Using Sullivan’s method (Jagger 1999; Sullivan 1971), a prevalence-based method of dividing life-table years lived in an age interval into years with and without satisfaction with life based on the life satisfaction prevalences of that five-year age group, we estimate the satisfied life expectancy in Spain. Mathematically, the remaining life-time years (LE) at age x spent in a state j (satisfied or unsatisfied) can be calculated as:
where \( l_{x} \). denotes the survivor function of a life table calculated through the number of people who survived at age x, \( \pi_{i} \) is the prevalence of a givesatisfaction condition (satisfied or unsatisfied) at age i.
Finally, the 2013 EU-SILC prevalences of life satisfaction by education level and five-year age groups are, therefore, extrapolated to the Spanish population data on the life table, using Sullivan’s method, to estimate the expected life years spent satisfied with life, which hereafter will be denoted as satisfied life expectancy The 95% confidence intervals are estimated for life expectancy with satisfied and unsatisfied. Expected years lived unsatisfied at age 30 and at age 65 are computed by summing up the years lived in these particular states as well as for each age group. Years lived with satisfaction were estimated in the same way.
3 Results
The main sociodemographic characteristics of our sample, for which we estimated mortality (INE 2012) are the following. The sample includes a few more women (51.5%) than men (48.4%) aged 30-plus. The distribution of education shows similar size of the proportion of men and women in the higher education category (26.7% for men and 26.3% for women), more females in the lower education category (24.8% vs. 30.1%) and fewer females in the medium education category (48.5% vs. 43.7%).
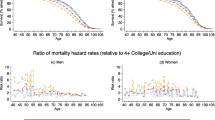
3.1 Prevalence of High Life Satisfaction by Gender and Education Level
The proportion of individuals satisfied with life by gender, 5-years age groups and education level in 2013 is presented in Fig. 1. We calculated smoothed age-specific prevalence of high life satisfaction to show the change in reported satisfaction by gender in the three educational groups. In general, the smoothed age-specific prevalences of high satisfaction with life was lower for low levels of education and higher for high levels of education. This pattern repeats for both men and women, but differences in the prevalences of high satisfied with life between education groups showed to be larger among men than women. In most of the age groups and levels of education women tended to report higher levels of being satisfied with life than men. However, we found the largest gender differences in the prevalences of high life satisfaction at ages over 60 years and particularly for medium and high levels of education. In general, being highly satisfied increases with age for both genders and in all education groups, with the highest records being reported during the later years in life.

Source: EU-SILC 2013
Smoothed age-specific prevalence of high life satisfaction by gender and education level. Note: “Low Ed” is low education, “Mid Ed” is medium education, “High Ed” is high education.
3.2 Gender Differences in Life Expectancy by Level of Education in 2012
According to data from INE, in 2012, Spanish life expectancy at age 30 was 50.0 years for men and 55.6 years for women; while Spanish life expectancy at age 65 was 18.5 years for men and 22.4 years for women (Table 1). However, we find substantial differences when we stratify the life expectancy by level of education for men and women.
Women always reported higher life expectancy than men—in all education groups and in both ages (30 and 65). 30 years old men with a low education level were expected to live 48.4 years while their men counterparts with a high education level were expected to live up to 56.0 years (49.9 years was for medium education). For women, these values were 55.4 years and 63.3 years (56.8 years), respectively. At the age of 65, men’s life expectancy with low levels of education was 18.5 years and 23.0 for women with a low education level (18.5 years was for medium education). In contrary, for those with the highest levels of education, life expectancy was 22.8 for men and 29.8 for women (23.7 years was for people with a medium education level).
At age 30, women-men differences in life expectancy ranged from the lowest 6.9 years in medium education to the highest 7.3 years in high education. The corresponding ranges at age 65 were from 4.5 years for low education and 7.0 years for high education. Therefore, the smallest gender differences in life expectancy by education level were in the low education level at age 65, and largest in the high education level at age 30. Overall, no matter the age, the largest gender differences in life expectancy were reported by people with high levels of education and it was always in favor of women.
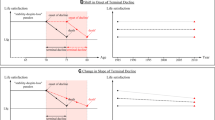
3.3 Decomposition of Life Expectancy at Age 30 and at Age 65 in (Un)satisfied Life Expectancy by Education Level in 2012
Figure 2 decomposes the life expectancy at age 30 and at age 65 into the number of years lived in a satisfied and in an unsatisfied state by level of education for both men and women. The satisfied life expectancy varied considerably across educational levels, gender and by age. Males and females with the highest education level were the only group who spent more years in a highly satisfied than in an unsatisfied state. The relative percentages corresponding to satisfied life expectancy were 55.0% and 60.0% for men at age 30, and 60.5% and 71.0% for women at age 65, respectively. In the rest of the groups, satisfied life expectancy was below 40% for those with low levels of education and under 50% for those with medium education. This repeats at both ages and for men and women. 30 years old Spanish women with low levels of education showed the worse scenario as they are the ones who are expected to spend the largest number of years in an unsatisfied state (34.6 years) (in absolute and relative terms). Overall, for both genders, a gradient pattern is seen as the higher the level of education you have, the largest is the satisfied life expectancy (Fig. 2).

Source: INE, 2012. EU-SILC, 2013. Note: “Low Ed” is low education, “Mid Ed” is medium education, “High Ed” is high education. The % shows the proportion of years lived in a satisfied state
Life expectancy, satisfied life expectancy, and unsatisfied life expectancy at age 30 and 65 by gender and level of education.
Particularly, at age 30, the unsatisfied life expectancy for men with low levels of education was 30.1 years (62.3% of the expected remaining time). However, those with medium or high education levels improved gradually as the number of years on an unsatisfied state were reduced compared to the lower education group (55.7% and 45%, respectively). For men with 65 years of age, similar patterns are observed; however, the expected remaining time on an unsatisfied state is slightly lower than the one corresponding for males with 30 years of age (Fig. 2). A similar pattern is seen for women at age 30 and at age 65; however, no matter of age, women with high levels of education are the ones who are expected to be spent the least number of years in an unsatisfied state.
The female-male differences in satisfied life expectancy were the largest among those with a high level of education (7.5 years at age 30 and 7.4 years at age 65). Female-male differences in satisfied life expectancy were also high among those with medium level of education (4.6 years at age 30 and 3.3 years at age 65), but the lowest gender differences in satisfied life expectancy were seen among individuals with low levels of education (2.6 years and 1.6 years, respectively). Regarding female-male differences in unsatisfied life expectancy, these differences were in favor of men only for those with a high level of education (− 0.2 years at age 30 and − 0.5 years at age 65). The female-male differences in unsatisfied life expectancy were 4.5 years and 2.9 years for individuals with low education levels at age 30 and 65, respectively.
4 Discussion
Longevity, and particularly healthy aging, is a key dimension of people’s well-being and one of the main drivers of progress in living standards in developed societies. To our knowledge, this is the first study that estimates subjective life expectancy according to education level and gender in Spain. Our aim was to understand gender inequality in longevity by comparing satisfied life expectancy at two different age groups (age 30 and at age 65) across three education levels.
We provided empirical evidence on an interesting and relevant aspect of the health literature for contemporary societies, where life expectancy is high, and the length of life continues to increase but differently for men and women across educational groups. Our findings confirm that Spanish women have longer life expectancy, regardless of education and age. Moreover, the largest gender gap in life expectancy was among the highest educated. Particularly, the size of the advantage varied greatly. For instance, Spanish women with high levels of education were expected to live 7.3 years more than men in the same category at age 30 (22.8 years for males and 29.8 years for females, a difference of 7.0 years at the age of 65). Spanish women had also an advantage in satisfied life expectancy, regardless of education (except for the low educated that no significant gender differences were found). The largest gender gap in satisfied life expectancy was also among the highly educated. Women with high levels of education at 30 were expected to live highly satisfied 7.5 years more than men, and 7.4 years at the age of 65, respectively. Despite this women’s advantage in terms of life satisfaction over men, the larger share of the remaining years of life of Spanish people was expected to be spent in an unsatisfied state, regardless of gender. Only those with higher levels of schooling were the only ones who spent more years in a satisfied than unsatisfied state, with advantage of women over men at both age groups. In particular, among high educated women at the age of 30, 60.5% were expected to live satisfied during their lifespan (and 39.5% unsatisfied), and this goes up to 71% at the age of 65. Our favorable results in the years of satisfaction with life might result from a protective effect for those with high levels of education, particularly women. Education is a positional good, and our findings confirm previous results that respondents with the highest levels of education are significantly more satisfied with life. One possible explanation of this protector effect could be linked to the fact that people who report high levels of life satisfaction are people who are satisfied where they live and with what the country could offer. For instance, living in a country like Spain with a high quality social health system, rated among the best in the world, and where the health care spending is high (York and Bell 2014; Botha 2014), seems to act as a good protector in qualifying your life.
This result of gender difference in satisfied life expectancy in Spain contributes to the existing literature by bringing evidence that low educated women tend to spent their remaining years not only in unhealthy but also in unsatisfied states. In general, the higher the education level, the largest the satisfied life expectancy, and the largest the number of years in a satisfied state. This applies for both men and women and both age groups. In addition, our results showed that satisfied life expectancy largely increased in both absolute terms (number of years) and relative terms (proportion of life) as education increases as well for both adult ages examined.
Even though our data is limited to the Spanish case, several conclusions can be drawn beyond this particular context. First, gender gap in satisfied and unsatisfied life expectancy indicates that Spanish women live more satisfied than Spanish men for medium and high education groups. We can advance two possible explanations of why highly educated women are the ones recording a higher satisfied life expectancy. On the one hand, we point at the relationship between employment and subjective well-being. Highly educated women may also be the ones with higher labor force participation. According to data from the European Labor Force Survey provided by Eurostat, employment rate in Spain in 2012 was 75.2 among women with high education levels, and 48.3 for those with low level of schooling. Similar trends were recorded for the EU-28, females with high levels of education had an 81.9 percent of employment rate, and low educated registered 52.2. Past literature has documented the benefits of labor force participation, as it broadens social capital which in turns increases happiness (Bartolini et al. 2013), and it enhances social roles (Klumb and Lampert 2004). According to previous research, the successful combination of different roles may lead to higher life satisfaction. For instance, the ability to balance family demands and employment enhances self-confident and self-esteem (Klumb and Lampert 2004). On the other hand, high education levels are also associated with increases in personal income. Income affects well-being and, therefore, we can expect that better-off individuals may be happier (Easterlin 2001). Comparative research also indicates that national income and high levels of public expenditure are associated with increased happiness (Easterlin 1995), mainly in short-term periods, as these expenditures may strengthen social solidarity and increase levels of happiness through establishing a good education system or promoting health care services. However, a recent work by Easterlin et al. (2010) demonstrated that in developed countries and over the long-term no relationship is found between a country’s income rise and an increase in happiness. More rigorous statistical analyses and additional studies examining the potential combination between individual and contextual determinants of gender gap in life satisfaction are needed to address these issues.
Second, our results showed the importance of education, and it may point at the relevance to invest in individuals’ human capital as a way to improve general wellbeing. Similarly, Cuñado and Pérez de Gracia (2012) found a positive impact of education on perceived happiness for the case of Spain and interpreted this result as a possible indication of the effect of education on self-assurance and individual’s contentment with their own lives. Social expenditures on education may complement health policies, as more educated people will live their lives with a higher life satisfaction.
Finally, our study contributes to the debate on objective and subjective measures of health. Several developed countries are shown to have higher life expectancies, and healthier populations than ever before. Here, we found that women in Spain have a higher life expectancy in a satisfied state than men if they have medium or high education, and slightly lower if they are low educated. Our results aimed at shedding additional light on how differently Spanish men and women with different educational level live these added years of life in terms of life satisfaction. However, additional research is needed to determine under which circumstances women live more highly satisfied than men, and what is the relationship between objective health measures and perceived life satisfaction. Past findings found that full employment, and a generous and comprehensive social safety do increase happiness (Easterlin 2013). Nonetheless, these are not always proportionally distributed across population groups, and education-related inequalities persist. These inequalities may be also translated into health disparities. From this perspective, national health policies should view high satisfaction with life as an important determinant of health and wellbeing.
Finally, our study has some limitations that might affect our results. Highly satisfied people may be more willing to participate in the survey, and there may also be gender-specific patterns in participation rates and may be culturally influenced. Therefore, differences in survey participation and reporting styles may be reported differently according to men and women.
Notes
For a detailed description of the evolution in the educational attainment of the Spanish adult population between 1960 and 2010 see De la Fuente and Doménech (2015).
This report can be accessed here: http://www.ine.es/metodologia/t20/t2030306_niveduc.pdf.
Low Education: 1 "Analfabetos" 2 "Estudios primarios incompletos" 3 "Educción primaria" 4 "Primera etapa de educación secundaria y similar". Medium Education: 5 "Segunda etapa de educación secundaria con orientación general" 6 "Segunda etapa de educación secundaria con orientación profesional" 8 "Enseñanzas de educación profesional y títulos universitarios propios que precisan del título de bachiller". High Education: 9 "Grados universitarios de 240 créditos ECTS y similares" 10 "Grados universitarios de más de 240 créditos ECTS y similares" 11 "Másteres y similares" 12 "Doctorado universitario".
References
Arpino, B., & Solé-Auró, A. (2019). Education inequalities in health among older European men and women: The role of active aging. Journal of Aging & Health, 31(1), 185–208.
Arrosa, M. L., & Gandelman, N. (2016). Happiness decomposition: Female optimism. Journal of Happiness Studies, 17(2), 731–756.
Barford, A., Dorling, D., Smith, G. D., & Shaw, M. (2006). Life expectancy: Women now on top everywhere. BMJ, 332, 808.
Bartolini, S., Bilancini, E., & Pugno, M. (2013). Did the decline in social connections depress Americans’ happiness? Social Indicator Research, 110(3), 1033–1059.
Bohannon, R. W., Peolsson, A., Massy-Westropp, N., Desrosiers, J., & Bear-Lehman, J. (2006). Reference values for adult grip strength measured with a Jamar dynamometer: A descriptive meta-analysis. Physiotherapy, 92(1), 11–15.
Botha, F. (2014). Life satisfaction and education in South Africa: Investigating the role of attainment and the likelihood of education as a positional good. Social Indicators Research: An International and Interdisciplinary Journal for Quality-of-Life Measurement, 118(2), 555–578.
Cambois, E., Solé-Auró, A., Brønnum-Hansen, H., Egidi, V., Jagger, C., Jeune, B., et al. (2016). Educational differentials in disability vary across and within welfare regimes: A comparison of 26 European countries in 2009. Journal of Epidemiology and Community Health, 70(4), 331–338.
Corsini, V. (2010). Highly educated men and women live longer. Life expectancy by educational attainment. Population and Social Conditions, Eurostat Statistics in focus, no 24. Catalogue number: KS-SF-10-024-ENN. Retrieved from https://ec.europa.eu/eurostat/documents/3433488/5565012/KS-SF-10-024-EN.PDF/f2caf9d2-3810-4088-bdbe-2f636e6ecc48.
Crimmins, E. M., & Cambois, E. (2003). Social inequalities in health expectancy. In J. M. Robine, C. Jagger, C. Mathers, E. M. Crimmins, & R. Suzman (Eds.), Determining health expectancies (pp. 111–126). Chichester: John Wiley & Sons Ltd.
Crimmins, E. M., Kim, J. K., & Solé-Auró, A. (2011). Gender differences in health: Results from SHARE, ELSA and HRS. The European Journal of Public Health, 21(1), 81–91.
Crimmins, E. M., & Solé-Auró, A. (2013). Life expectancy, health and functioning among the 85-plus in Europe and the United States. Public Policy and Aging Report, 23(2), 3–9.
Cuñado, J., & Pérez de Gracia, F. (2012). Does education affect happiness? Evidence for Spain. Social Indicators Research, 108(1), 185–196.
Danner, D. D., Snowdon, D. A., & Friesen, W. V. (2001). Positive emotions in early life and longevity: Findings from the nun study. Journal of Personality and Social Psychology, 80, 804–813.
De la Fuente, A., & Doménech, R. (2015). Education attainment in the OECD, 1960–2010. Updated series and a comparison with other sources. Economics of Education Review, 48, 56–74.
Diener, E. (2009). The science of well-being. The collected works of Diener. Dordrecht: Springer.
Easterlin, R. A. (1995). Will raising the incomes of all increase the happiness of all? Journal of Economic Behavior & Organization, 27(1), 35–47.
Easterlin, R. A. (2001). Income and happiness: Towards a unified theory. The Economic Journal, 111(473), 465–484.
Easterlin, R. A. (2010). Happiness, growth, and the life cycle. Europe Journal of Psychology, 7(2), 395–398.
Easterlin, R. A. (2013). Happiness, growth and public policy. Economic Inquiry, 51(1), 1–15.
Easterlin, R. A., McVey, L. A., Switek, M., Sawangfa, O., & Zweig, J. S. (2010). The happiness–income paradox revisited. Proceedings of the National Academy of Sciences, 107, 22463–22468.
EHLEIS. (2015). Country Reports Issue 9. Retrived January 2018. http://www.eurohex.eu/pdf/CountryReports_Issue9/Spain_Issue9.pdf.
Erlinghagen, M., & Hank, K. (2006). The participation of older Europeans in volunteer work. Ageing & Society, 26, 567–584.
Eurostat. (2015). Being young in Europe Today. Eurosat Statittical book, 2015 edition.
George, L. K. (2010). Still happy after all these years: Research frontiers on subjective well-being in later life life. Journal of Gerontology: Social Sciences, 65B(3), 331–339.
Geroge, L. K. (2006). Perceived quality of life. In R. H. Binstock & L. K. George (Eds.), Handbook of aging and the social sciences (6th ed., pp. 320–336). San Deigo, CA: Elsevier.
Gerstorf, D., Ram, N., Mayraz, G., Hidajat, M., Lindernberger, U., Wagner, G. G., et al. (2010). Late-life decline in well-being across adulthood in Germany, the United Kingdom, and the United States: Something is seriously wrong at the end of life. Psychology and Aging, 25(2), 477–485.
Hamplová, D. (2018). Does work make mother happy? Journal of Happiness Studies. https://doi.org/10.1007/s10902-018-9958-2.
Han, S. H., Tavares, J. L., Evans, M., Saczynski, J., & Burr, J. A. (2017). Social activities, incident cardiovascular disease, and mortality: Health behaviors mediation. Journal of Aging and Health, 29, 268–288.
Helliwell, J. F., Layard, R., & Sachs, J. (2018). World Happiness Report 2018. New York: Sustainable Development Solutions Network.
HMD. (2017). Human mortality database. University of California, Berkeley and Max Planck Institute for Demographic Research. (www.mortality.org). Accessed 2.10.2017.
Jacobs, J. A., & Gerson, K. (2004). The time divide. Work Family and Gender Inequality. Cambridge, MA: Harvard University Press.
Jagger, C. (1999). Health expectancy calculation by the Sullivan method a practical guide. Tokyo: Nihon University, Population Research Institute.
Jasilionis, D., & Shkolnikov, V. M. (2016). Longevity and education: A demographic perspective. Gerontology, 62, 253–262.
Kahneman, D., Diener, E., & Schwarz, N. (1999). Well-being: Foundations of hedonic psychology. New York: Russel Sage Foundation.
Klumb, P. L., & Lampert, T. (2004). Women, work, and well-being 1950–2000: A review and methodological critique. Social Science and Medicine, 58(6), 1007–1024.
Koivumaa-Honkanen, H., Honkanen, R., Viinamäki, H., Heikkilä, K., Kaprio, J., & Koskenvuo, M. (2000). Self-reported life satisfaction and 20-year mortality in healthy Finnish adults. American Journal of Epidemiology, 152(10), 983–991.
Koopmans, T. A., Geleijnse, J. M., Zitman, F. G., & Giltay, E. J. (2010). Effects of happiness and all-cause mortality during 15 years of follow-up: The Arnhem elderly study. Journal of Happiness Studies, 11(1), 113–124.
Lozano, M., Hamplová, D., & Le Bourdais, C. (2016). Non-standard works schedules, gender, and parenta stress. Demographic Research, 34(9), 259–284.
Mäki, N., Martikainen, P., Eikemo, T., Menvielle, G., Lundberg, O., Öftergen, O., et al. (2013). Educational differences in disability-free life expectancy: A comparative study of long-standing activity limitation in eight European countries. Social Science and Medicine, 94(5 Suppl. 1), 1–8.
Martín, U., Domínguez-Rodríguez, A., & Bacigalupe, A. (2017). Desigualdades sociales en salud en población mayor: una aportación desde la salud pública al debate sobre el retraso de la edad de jubilación en España. Gaceta Sanitaria. https://doi.org/10.1016/j.gaceta.2017.10.010.
Mathers, C. D., Stevens, G. A., Boerma, T., & White, R. A. (2015). Causes of international increases in older age life expectancy. The Lancet, 385(9967), 540–548.
Mattingly, M. J., & Sayer, L. C. (2006). Under pressure: Gender differences in the relationship between free time and feeling rushed. Journal of Marriage and Family, 68(1), 205–221.
Mojon-Azzi, S., & Sousa-Poza, A. (2011). Hypertension and life satisfaction: An analysis using data from the survey of health, ageing and retirement in Europe. Applied Economics Letters, 18(2), 183–187.
Montez, J. K., Hummer, R. A., & Hayward, M. D. (2012). Educational attainment and adult mortality in the United States: A systematic analysis of functional form. Demography, 49(1), 315–336.
Montez, J. K., Hummer, R. A., Hayward, M. D., Woo, H., & Rogers, R. G. (2011). Trends in the Educational Gradient of the U.S. Adult Mortality from 1986 to 2006 by Race, gender, and age group. Research on Aging, 33(2), 145–171.
Myrskylä, M., & Margolis, R. (2014). Happiness: Before and after the kids. Demography, 51, 1843–1866.
OECD [Organisation for Economic Co-operation and Development]. (2015). Health at a Glance 2015: OECD Indicators. Paris: OECD Publishing.
Oksuzyan, A., Brønnum-Hansen, H., & Jeune, B. (2010). Gender gap in health expectancy. European Journal of Ageing, 7(4), 213–218.
Oksuzyan, A., Juel, K., Vaupel, J. W., & Christensen, K. (2008). Men: Good health and high mortality. Sex differences in health and aging. Aging Clinical and Experimental Research, 20(2), 91–102.
Olshansky, S. J., Antonucci, T., Berkman, L., Binstock, R. H., Boersch-Supan, A., Cacioppo, J. T., et al. (2012). Differences in life expectancy due to race and educational differences are widening, and many may not catch up. Health Affairs, 31(8), 1803–1813.
Palacios-Cena, D., Jimenez-Garcia, R., Hernández, V., Alonso-Blanco, C., Carrasco-Garrido, P., & Fernández-de-las-Peñas, C. (2012). Has the prevalence of disability increased over the past decade (2000–2007) in elderly people? A Spanish population-based survey. Journal of the American Medical Directors Association, 13(2), 136–142.
Pinquart, M., & Sörensen, S. (2001). Gender differences in self-concept and psychological well-being in old age: A meta-analysis. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 56(4), P195–P213.
Requena, M. (2017). La desigualdad ante la muerte: Educación y esperanza de vida en España. Perspectives Demogràfiques, 6, 1–4.
Robine, J. (2006). Summarizing health status. In D. Pencheon, C. Guest, D. Melzer, & G. Jam (Eds.), Oxford handbook of public health (pp. 160–168). Oxford: Oxford University Press.
Robine, J. M., & Jagger, C. (2017). Health expectancies. In J. P. Michel, B. L. Beattie, F. C. Martin, & J. D. Walston (Eds.), Oxford Textbook of Geriatric Medicine (3rd ed., pp. 63–68). Glasgow, UK: Oxford University Press.
Ross, C. E., & Mirowsky, J. (2010). Gender and the health benefits of education. The Sociological Quarterly, 51(1), 1–19.
Siahpush, M., Spittal, M., & Singh, G. K. (2008). Happiness and life satisfaction prospectively predict self-rated health, physical health, and the presence of limiting, long-term health conditions. American Journal of Health Promotion, 23, 18–26.
Solé-Auró, A., & Alcañiz, M. (2015). Are we living longer but less healthy? Trends in mortality and morbidity in Catalonia (Spain), 1994–2011. European Journal of Ageing, 12(1), 61–70.
Solé-Auró, A., & Alcañiz, M. (2016). Educational attainment, gender and health inequalities among older adults in Catalonia (Spain). International Journal for Equity in Health, 15, 126.
Solé-Auró, A., Beltrán-Sánchez, H., & Crimmins, E. M. (2015). Are differences in disability-free life expectancy by gender, race and Education wider at older ages? 1986–2006. Population Research and Policy Review, 34(1), 1–18.
Strine, T. W., Chapman, D. P., Balluz, L. S., Moriarty, D. G., & Mokdad, A. H. (2008). The associations between life satisfaction and health-related quality of life, chronic illness, and health behaviors among U.S. community-dwelling adults. Journal of Community Health, 33(1), 40–50.
Sullivan, D. F. (1971). A single index of mortality and morbidity. Rockville, Md: Health Services and Mental Health Administration.
Verbrugge, L. M. (1984). Longer life but worsening health? Trends in health and mortality of middle-aged and older persons. The Milbank Memorial Fund Quarterly Health and Society, 62(3), 475–519.
WHO. (2016). World Health Statistics 2016: Monitoring health for the SDGs. Global Health Observatory Data.
Yang, Y. (2008). Long and happy living: Trends and patterns of happy life expectancy in the US: 1907–2000. Social Science Research, 37(4), 1235–1252.
York, R., & Bell, S. E. (2014). Life satisfaction across nations: The effects of women’s political status and public priorities. Social Science Research, 48, 48–61.
Acknowledgements
This study belongs to the multi-country project “Care, Retirement & Wellbeing of Older People Across Different Welfare Regimes” (CREW). The authors acknowledge funding from the Spanish Ministry of Economy, Industry and Competitiveness (PCIN-2016-005) within the second Joint Programming Initiative “More Years Better Lives” and to the Socio-Demographic Consequences of the Great Recession: Altered Class and Gender Relations? (RECECON) Spanish Ministry of Economy and Competitiveness, CSO2016-80484-R. In addition, Mariona Lozano’s work was sustained by financial support from the Research Incentive program to tenure-track researchers from the Department of Political and Social Sciences at Pompeu Fabra University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Solé-Auró, A., Lozano, M. Inequalities in Longevity by Education Level in Spain: A Life Satisfaction Approach. Soc Indic Res 144, 729–744 (2019). https://doi.org/10.1007/s11205-018-02057-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-018-02057-w