
Abstract
Economic growth is widely considered an effective instrument to combat poverty, and child malnutrition. Though there is a substantial literature on the relationship between economic growth and child malnutrition in a wide range of countries, empirical evidence on this relationship is sparse in the case of Egypt. Using repeated crosssectional data from five rounds of the National Demographic and Health Survey (DHS), we examine the association between income per-capita growth, at the governorate level, and various child malnutrition outcomes: stunting, wasting, and underweight, in Egypt during the period 1992–2008. A logistic regression model, with regional and time fixed effects applied to pooled data of the five DHS rounds, is used. The analyses control for the structure of the data, and the clustering of observations (children nested within households within clusters nested in governorates). Statistics show that 29% of the children-under-5 years were stunted, 7.2% were wasted, and 6% were underweight in 2008. We found a robust statistically significant negative association between economic growth, at the governorate level, and four indicators of child malnutrition, namely; underweight, wasting, extreme wasting, and extreme stunting. Though a negative association was also found between economic growth and stunting and extreme underweight, the odd ratios were not statistically significant but were well below unity which indicates economic significance if estimated precisely. No significant association was found between income inequality, as measured by the Gini-index, and any of the malnutrition indicators. Results also reveal that child and household-level characteristics including; child age, sex, the birth interval of a child, whether the child is a twin and father`s education, are particularly important determinants of malnutrition indicators in Egypt. The findings of the current study provide additional supportive evidence, using data from Egypt, that economic growth is an effective instrument to combat child malnutrition and improve population health outcomes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
It is widely documented that early-life nutrition has a significant impact on health and human development throughout the entire life course (Barker et al. 2002; Victora et al. 2008; Maluccio et al. 2009). The World Bank considers child malnutrition as “a major obstacle to human development and economic growth in a country, especially among the poor and the vulnerable” (Gragnolati et al. 2005). Compared to well-nourished children, malnourished children have a weaker immune system, higher risk of mortality and morbidity, reduced physical ability, and reduced ability to reach potential height. A child’s poor nutritional status has been linked to poor school performance, which in turn lowers future employment opportunities and income generation, causing an intergenerational transmission of poverty (United Nations Children’s Fund 2013).The United Nations Children’s Fund (UNICEF) estimated that tackling child malnutrition could boost poor countries’ GDP by 3% (United Nations Children’s Fund 2013). In the labor market, Case and Paxson (2006) noticed a positive association between adults’ height and earnings. They found that the height-earnings gap is mainly due to good nutrition in early childhood. Workers who received good nutrition during childhood have higher levels of cognitive function than their malnourished counterparts, which accounts for the labor market height premium (Case and Paxson 2006).
The prevalence of malnutrition is particularly high in Egypt. The country has the largest number of stunted children in the Middle East, with about 2.7 million children experiencing stunted growth (United Nations Children’s Fund 2013). The economic and social cost of child malnutrition in Egypt was estimated to be 20.3 billion Egyptian Pounds, which is equivalent to about 2% of the Egyptian GDP (Information and Decision Support Center 2013).
Economic growth has been widely considered an effective instrument for poverty alleviation and improving public health. This idea has been supported by a growing number of studies (Pritchett and Summers 1996; Smith and Haddad 2002; Vollmer et al. 2014). For example, in a cross-country study, using time series data and instrumental variables to avoid reverse causality, Pritchett and Summers (1996) found evidence that the increase in national income tends to improve population health, and that wealthier nations are healthier nations. Though there is a substantial literature on the relationship between economic growth and child malnutrition in a wide range of countries, empirical evidence on this relationship is sparse in the case of Egypt. As depicted in Fig. 1, Egypt has experienced rapid economic growth in the last two decades, where real GDP per capita has grown from $895 to $1456 between 1992 and 2008. In this paper, we aim to examine whether this rapid economic growth was associated with a reduction in child malnutrition rates. This study serves as an initial attempt to evaluate the association between economic growth and child nutritional outcomes preceding the popular uprising in Egypt which called for social justice and better economic conditions in the 2011 revolution.

Economic growth in Egypt: 1992–2008. Source: World Development Indicators, World Bank (2014)
In Egypt, to date, no study empirically examined the association between economic growth and child malnutrition. Two earlier studies, El-Laithy et al. (2003), and Kheir-El-Din and El-Laithy (2008) assessed the effect of economic growth on poverty alleviation in Egypt. They found evidence that economic growth, which took place between 1990 and 2005, has reduced poverty rates. The current study goes beyond poverty, by examining the association between economic growth and other measures of human deprivation, i.e., child nutrition outcomes. We develop a unique repeated cross-sectional dataset to examine the association between income per capita growth, at the governorate level, and childhood malnutrition status in Egypt for the period between 1992 and 2008.
The paper is organized as follows: Sect. 2 presents a review of the theoretical and empirical literature on the link between economic growth and child malnutrition. The data and empirical methodology are described in Sect. 3. Section 4 presents the empirical results which are then discussed in Sect. 5. Section 6 concludes the paper.
2 Literature Review
2.1 The Economic Growth—Malnutrition Linkage: A Theoretical Framework
Theoretically, the relationship between economic growth and child malnutrition could be bi-directional. While poverty and food insecurity could lead to malnutrition, child malnutrition may, in turn, have intergenerational consequences, which could slow down economic growth. Inadequate dietary intake and diseases are the direct causes of child malnutrition. This could arise as a result of households’ food insecurity, inadequate feeding practices, unhealthy household environments and inadequate health services, all of which are directly related to economic growth.
Figure 2 shows that economic growth could help in reducing child malnutrition through three channels. Firstly, economic growth increases the employment opportunities, income levels, and wealth which offer poor household food security, better nutrition, and health care, and improved maternal education. Secondly, economic growth widens the tax base and increases public revenues, which enable higher public spending on health and social protection, such as expenditure on food ration cards. Thirdly, economic growth could benefit individuals indirectly through higher public expenditure on infrastructures, such as roads, schools, and hospitals. We believe that possible reverse causality, i.e. healthier individual being more productive and hence leading to higher economic growth, is not a concern here, as we exclusively focus on short and medium term outcomes of children.

Economic growth and children nutritional status linkage. Source: Adopted from Subramanyam et al. (2011)
2.2 Empirical Literature
A growing number of empirical studies have emerged to examine the effect of economic growth on childhood malnutrition with mixed findings (see for example Smith and Haddad 2002; Subramanyam et al. 2011; Harttgen et al. 2012; Vollmer et al. 2014). Existing empirical studies differ in their methodologies, as far as sample covered, and the level of analysis. On the one hand, some have performed a cross-country analysis, using macro-level data. On the other, other studies use data at the household level. Hence, the results of these studies are not directly comparable.
For example, using panel data on 63 developing countries, over the period 1970–1996, Smith and Haddad (2002) found a strong negative effect on economic growth on child malnutrition. They hypothesized that the global economic growth which took place between 1970 and 1996 is responsible for half of the reduction in the prevalence of child malnutrition, through promoting investments in women’s education and health, environment quality and food affordability. In another cross-country study, Harttgen et al. (2012) examined the association between GDP per capita growth, and the reduction of child malnutrition in 15 Sub-Saharan African countries, using both a macro and a micro model. In the macro model, they estimated the overall levels of malnutrition across countries from the Demographic and Health Surveys (DHS) which were regressed on GDP per capita using a fixed effect model. The fixed effect macro model failed to detect a significant relationship between income growth and the level of child malnutrition. In the micro model, all the DHS surveys from Sub-Saharan African countries were pooled together into one single large dataset, and results showed that GDP per capita growth has a mild effect on child malnutrition. The authors concluded that economic growth did not trickle down to the poor and that individual level variables, such as mother’s education, socioeconomic status, and mother’s nutritional status are more critical to children’s growth than national development indicators.
Using data from 121 surveys in 36 low-income and middle-income countries, Vollmer et al. (2014) utilized logistic regression models to estimate the association between changes in per-capita GDP, and changes in child under-nutrition outcomes. They found evidence that macroeconomic growth has a null, to quantitatively very weak, contribution to the reductions in early childhood stunting, underweight, and wasting. Using country-level data from the World Bank’s World Development Indictors, Heltberg (2009) analyzed spells of malnutrition over time, and found a significant, but small, negative association between economic growth and chronic child malnutrition, where periods of economic growth are often associated with reduced child malnutrition. The author also found that the association between economic growth and chronic child malnutrition is much lower than the effect of growth on poverty. The elasticity of stunting with respect to growth in per-capita gross national income was about −0.2 in a country with 30% stunting rate and that halving stunting from a level of 30% through economic growth alone would require an annual growth of real per capita income by 3.7% for 25 years.
In addition to cross-country studies, several country-specific studies have investigated the association between economic growth and child malnutrition, in a wide range of countries. For example, Alderman et al. (2006) found, using panel data from Tanzania, evidence that a combination of income growth and nutrition interventions are effective in reducing malnutrition. In another study, Subramanyam et al. (2011) focused on India; the country with the largest number of children under 5 years old who are stunted in the world. The unique contribution of their study to the literature is in the use of income growth at the state level rather than at the country level. They pooled three nationally representative surveys of India for years 1992, 1998 and 2005, and regressed a binary variable for child malnourishment on individual and state-level variables. No or at best a weak association was found between economic growth at the state level and the different types of child malnutrition. They concluded that the strong economic growth that took place in India was not sufficient to reduce child malnutrition.
At the micro level, several studies have examined the relationship between household income and the health status of children (see for example Case et al. 2009). The premise is that households with high levels of income are better able to invest in their children’s health and education, and that would lead to better health and nutritional status. However, it ‘s hard to reach causal inferences in these studies, as health affect household income and household income influence the health of the household’s members (Currie and Madrian 1999; Frijters et al. 2005).
3 Data and Methods
3.1 Data
This paper uses data on children’s nutritional status for a nationally representative sample of 45,600 households from five rounds (1992, 2000, 2003, 2005, and 2008) of the Egyptian Demographic and Health Survey (EDHS). The DHS is an international survey, which is conducted in 85 developing countries and is sponsored by the U.S. Agency for International Development. It is the main source of information on child health in developing countries. EDHS interviews women between age 15 and 49 (reproductive age), collects information on infant and child mortality and is conducted every 5 years.
Nutritional anthropometry assesses the past and current nutritional and health status of children. Staff trained in taking anthropometric measures have collected the weight and height of the sampled children. The collected weight and height have been used in the construction of three anthropometric indicators (height-for-age, weight-for-age, and weight-for-height). Each indicator provides a unique viewpoint on the nutritional status of children. Low height-for-age (stunting) results from an inadequate nutrition for an extended period while low weight-for-height (wasting) reflects acute nutrition problems, and a low weight-for-age (underweight) reveals general nutritional and health problems. Each of the three indicators is represented by deviations (z-score) from the median value of the reference population for the same sex and age. The z-score (standard deviation score) is calculated as \(- score = \frac{A - M}{\sigma }\), where A is the child anthropometric measure, M is the median of the reference population, and σ is the standard deviation in the reference population.
A child with a z-score less than negative two standard deviations i.e.\((\frac{A - M}{\sigma } < - 2\sigma )\), is considered to be moderately malnourished, while a child with a z-score less than three standard deviation i.e.\((\frac{A - M}{\sigma } < - 3\sigma )\), is considered to be severely malnourished. The World Health Organization’s (WHO) reference population has been used as the reference population in this study.
The EDHS has a complex design which involves stratification based on the level of urbanization, and region. It involves clustering, where the selected villages are the clusters for rural areas, while the selected districts/towns are the clusters for urban areas. The complex survey design has been taken into account in all stages of the analyses in this study. The EDHS collects information on all born children. However, children who are dead by the time of the interview, and children with missing data on height or age, have been excluded from the analyses.
There are 26 governorates in Egypt, four are urban, and the rest are a mixture of urban and rural regions. Data on GDP per capita and the Gini index, at the governorate level, are developed by the Egyptian Institute of National Planning and are collected from the Egyptian Human Development Reports. In this study, all analyses and statistics are population weighted using the sampling weights in the EDHS survey.
3.2 Econometric Methodology
The purpose of this study is to examine the association between economic growth, at the governorate level, and six outcomes of malnutrition: stunting, severe stunting, wasting, severe wasting, underweight, and severe underweight. These associations are examined within a multivariate framework, after controlling for other covariates that are widely used in the literature (see for example Subramanyam et al. 2011 and Vollmer et al. 2014). A logistic regression model, with regional and time fixed effects applied to pooled data of the five DHS rounds, is used. We control for the structure of the data and the clustering of observations (children nested within households within clusters nested in governorates). We model the odds of malnutrition for child i in household j, nested in governorate k at the survey year t, using the logistic model in Eq. (1).
In Eq. (1), \(M_{ijkt}\) is an indicator variable of malnutrition (stunting, wasting, underweight) of child i in household j, nested in governorate k at the survey period t. \(Y_{kt}\) is the log real GDP per capita of governorate k for the survey year t. \(X_{ijkt}\) is a vector of child characteristics such as child age, sex, birth order of the child. \(H_{ijkt}\) is a vector of parental and household-level factors. \(G_{kt}\) is a vector of governorate fixed effects, \(S_{t}\) are the year fixed-effects, and \(\varepsilon_{ijkt}\) is the clustered error term that is clustered at the household and governorate levels.
The key predictor of interest is the log GDP per capita at the governorate level. Also, the multivariate analyses control for other explanatory variables that are closely related to the child’s nutritional status. The control variables can be grouped into three categories: variables that are related to the household socioeconomic status and food security; variables that reflect the degree of access to medical care and the quality of the health environment; and factors that indicate women and child characteristics. Household socioeconomic status is measured by the household wealth index, mother’s nutritional status and parents’ education. The household’s economic status, captured by the wealth index, is represented by five categories: poorest (reference category), poorer, middle, richer, and richest. The wealth index is widely used as a living standard measure. The EDHS team has developed the wealth index using a statistical method known as principal components analysis. The value of the wealth index depends on household’s possession of chosen assets such as cars, floor type, access to water and sanitation, and materials used for housing construction. This index was used to stratify the interviewed households into five wealth quintiles. For a detailed discussion on how the wealth index is constructed in the DHS, see Rutstein and Johnson (2004). Household socioeconomic status is considered a strong predictor of child nutritional status because it indicates whether a household has sufficient resources to obtain appropriate food for a nutritious diet.
A mother’s nutritional status is not only a proxy of economic deprivation, but it also affects child nutritional status directly during pregnancy and breastfeeding periods. Malnourished mothers are likely to deliver underweight babies and are less effective in breastfeeding. We control for women’s nutritional status by using the body mass index (BMI). For a systematic literature review on the impact of a women’s nutritional status, before and during early pregnancy, on maternal and infant outcomes see Ramakrishnan et al. (2012).
An adequate maternity care reduces the health risks of pregnancy and involves monitoring women’s nutritional status. In addition, it provides mothers with the opportunity to gain information on appropriate feeding practices. By using a dummy variable, we control for regular access to antenatal care. Concerning the quality of the health environment, access to clean water and adequate sanitation are included to control for drinking water quality and safe sanitation using dummy variables. Unsanitary living conditions and inadequate clean drinking-water are leading causes of infectious diseases. Access to safe drinking-water, sanitation, and hygiene services have been consistently linked to better nutrition outcomes (UNICEF and World Health Organization 2015).
As for the child characteristics, we control for the child sex, age, whether the child had a risky birth interval (defined as a birth-to-birth interval of less than 24 months), and whether the child is a twin. For a review of the literature on the impact of birth spacing on maternal and child nutritional status and health see Dewey and Cohen (2007) and Conde-Agudelo et al. (2012). Gender inequality could play a fundamental role in exacerbating the nutritional status of young girls, and this is particularly evident in Arab societies. Thus, the child sex variable controls for gender bias and norms in nutritional practices. Twin children are likely to increase the nutritional burden on the mother and the budget of low-income families. Twins are found to be more often malnourished than single children (Bijlmakers et al. 1998). Likewise, short birth intervals, mother’s current pregnancy status, and the number of children in the household adversely affect child nutritional status, as it increases the sociological and financial pressure on the household. The age of the mother could play a major role in the birth outcome. Childbearing by teenagers and older mothers adversely affect child health (Chen et al. 2007).
Governorates in Egypt differ in their geographical location, climate, natural resources, income inequality, and the degree of economic problems. Thus, we also included governorate fixed-effects, which account for governorate-specific factors affecting malnutrition that are constant over time. Recent research shows that public health is not only affected by the level of income, but also by the degree of inequality in the distribution of income within the society. Pickett and Wilkinson (2007) studied the impact of income inequality on child well-being in the US and found that all indicators of child well-being were significantly worse in states with inequitable income distribution. To control for income inequality, we use the Gini index, which measures the degree of fairness of income distribution within a governorate, where a high Gini coefficient indicates a high level of income inequality. The logistic model also controls for survey year fixed-effects to capture general developments that affected all the Egyptian governorates.
4 Results
Table 1 presents summary statistics of the variables used in the analyses. The table shows an increase in the fraction of mothers and fathers with higher and secondary education over the study period. Based on the wealth index, the fractions of the poorest and poorer households have slightly increased. There is also an increase in the rate of access to clean water and a private toilet as proxies for living in a healthy environment. The rate of receiving regular antenatal care during pregnancy has also increased significantly from 23.8% in 1992 to 65% in 2008. The prevalence of risky birth interval has grown from 76% in 1992 to 86% in 2008.
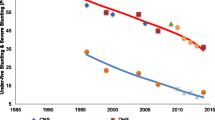
Figure 3 depicts the level of stunting, wasting and underweight in Egypt based on data from EDHS, during the period 1992 to 2008. The WHO classifies the degree of child malnutrition within a country into four levels: “low,” “medium,” “high,” and “very high.” Based on the WHO’s classification, the overall prevalence of stunting in Egypt is classified as high, while the degree of underweight and wasting is low. This pattern is becoming an increasingly global phenomenon. For instance, the number of stunted children in developing countries is about 200 million, while the number of wasted children is about 52 million. There are also other countries such as Albania, Egypt, Iraq, Mongolia, Zambia, Peru and Swaziland in which underweight and wasting prevalence is low but stunting rates are extremely high (UNICEF 2013). A possible explanation for the low levels of underweight and wasting versus the high prevalence of stunting is that stunted children face a markedly increased risk of becoming overweight and obese. Some children in Egypt are experiencing a double burden of malnutrition, having excess weight to height, and being too short for their age. This is coupled with the global shift toward junk food with high level of starch, fats, and sugar that affects malnutrition indicators that involve weight measurements severely in comparison to stunting indicators that involve only height measurements (De Haen et al. 2011).

Percentage of children under 5 years classified as malnourished according to anthropometric indices in Egypt. Source: Authors’ calculations based on data from several rounds of the EDHS
As shown in Fig. 3, in 2008, 29% of the children under-5-years were stunted, 7.2% were wasted, and 6% were underweight. Though the prevalence of stunting dropped in the beginning of the new millennium to 19.8% in 2003, compared to 25% in 1992, the declining trend for stunting prevalence was reversed after the 2006 avian influenza outbreak, which resulted in culling of millions of chickens and other poultry disrupting a key animal source of food that is critical for child growth and increasing the prices of other protein substitutes, mainly beef and fish (Kavle et al. 2014). Stunting rates then started to grow once again reaching 29% in 2008.
Table 2 presents the results of the logistic regression models for the different indicators of malnutrition (stunting, wasting, and underweight). Controlling for household economic status may remove a major channel through which economic growth could affect child nutritional status, and hence may underestimate the impact of economic growth. To account for this, and to check the robustness of the results, we estimated different model specifications that did not include household economic status. In particular, we started with estimating a model without controlling for the household economic situation by just regressing the likelihood of malnutrition on the governorate GDP per capita, and the time and governorate fixed effects. We then controlled for the household and individual characteristics in following specifications. We followed the same procedure in Table 3 which shows the results for extreme malnutrition.
The regression coefficients of logistic regression are quite difficult to interpret; thus, the reported coefficients in Tables 2 and 3 are odds ratios (ORs) that are easier to interpret. For example, if the odds ratio for stunting is less than one, it would mean \(\left[ {\left( {\frac{1}{OR} - 1} \right) \times 100} \right]\) percent lower odds of being stunted, while if the odds ratio is larger than one, we would have \(\left[ {\left( {OR - 1} \right) \times 100} \right]\) increase in the odds of being stunted. Since we are mainly interested in the impact of economic growth on malnutrition, we use log GDP per capita as the key explanatory variable. A one unit increase in log GDP per capita would be interpreted as approximately 72% increase in GDP per-capita \(\left( {e - 1} \right) = 1.72\), where e is the base of the natural logarithm. Consequently, the odds ratios would correspond to 72% increase in GDP per capita. For simplicity, we divide \(\left[ {\left( {\frac{1}{OR} - 1} \right) \times 100} \right]\) by 7.2 then the coefficients for GDP would refer to a 10% increase in GDP per-capita instead of 72%.
In all model specifications, economic growth has the expected negative association with child malnutrition indicators, as the odds ratios are all less than unity. Table 2 shows a statistically significant negative association between economic growth and underweight and wasting at the 1% significance level. A 10% economic growth rate is expected to reduce underweight rate by 11.3% \(\left[ {\frac{{\left( {\frac{1}{0.55} - 1} \right) \times 100}}{7.2} = 11.3} \right]\) and wasting rate by 11.8%. Though economic growth has a negative association with stunting, the odd ratio is not statistically significant at 5% significance level. However, the estimated odds ratios in the case of stunting are well below one which would indicate very large associations if estimated more precisely. This means that we fail to reject the null hypothesis of non-significance mainly due to large standard errors. Large standard errors indicate that the economic growth coefficient is not well estimated, which may be attributable to sampling error. The estimated odds ratio of log GDP per capita for the stunting model was very close to being significant at 10% significance level as the P value for the log GDP coefficient is 0.108.
As for the other covariates, results show no statistically significant association between income inequality, as measured by the Gini Index, and any of the indicators of child malnutrition, as none of the odd ratios was statistically significant. A child’s sex was significantly associated with malnutrition. Compared to a male child, a female child has lower odds of being stunted (OR 0.822; 95% CI 0.777–0.870), wasted (OR 0.837; 95% CI 0.703–0.996), and underweight (OR 0.713; 95% CI 0.624-0.816). Malnutrition has a statistically significant negative association with child’s age. In particular, when compared with an infant child (a child whose age is less than 12 month), a child who is one year old has lower odds of being underweight (OR 0.520; 95% CI 0.424–0.637), and wasted (OR 0.471; 95% CI 0.345–0.644). Similarly, a four years old child had about 63% lower odds of being underweight (OR 0.379; 95% CI 0.281–0.512) and wasted (OR 0.361; 95% CI 0.277–0.471) when compared to an infant child. On the contrary, results show higher odds of stunting among a one year old child (OR 1.419; 95% CI 1.300–1.548), a two years old child (OR 1.417; 95% CI 1.365–1.585), and a three years old child (OR 1.107; 95% CI 0.970–1.263), when compared to an infant child, while a four years old child has lower odds of being stunted (OR 0.789; 95% CI 0.672–0.925).
A twin child has higher odds of being stunted (OR 1.256; 95% CI 1.038–1.519), and underweight (OR 1.586; 95% CI 1.224–2.054) compared to a child who is not a twin. A child with a risky birth interval had higher odds of being stunted, underweight and wasted when compared to a child with no risky birth interval. Compared to children whose mothers did not receive regular health care during pregnancy, children of mothers who received regular maternal health care have lower odds of being underweight (OR 0.913; 95% CI 0.839–0.995). Compared to children from households with no private toilet, children of households who have a private toilet, as one of the indicators of a household’s economic status, have lower odds of stunting (OR 0.856; 95% CI 0.731–1.002); wasting (OR 0.764; 95% CI 0.565–1.034); and underweight (OR 0.792; 95% CI 0.635–0.988). A mother’s occupation is in general not significantly associated with child malnutrition, but for agriculture in which there is a statistically significant higher odd of stunting (OR 1.274; 95% CI 1.117–1.452) when compared to children whose mother is not employed. The composition of the GDP and the sources of economic growth could help in explaining the persistence of chronic malnutrition among children of agricultural sector workers. The service sector in Egypt accounts for more than half of the economy, and it has been the main driver of the recent economic growth between 2003 and 2008, more specifically the tourism industry, the telecommunication sector, and the transportation sector. On the other hand, the agricultural sector, on which one-fourth of the working population, and the majority of the Upper Egypt residents are depending, showed a weak economic performance. If economic growth benefits mostly the service sector workers and by-passes the agricultural sector workers, it is to be expected that income growth will likely have modest or no effect on poverty reduction and child malnutrition.
The age of the mother is not significantly associated with the child’s underweight, and wasting, as none of the odds ratios is statistically significant. However, the age of the mother was associated with lower odds of stunting; with mothers in the middle age having in general lower odds of stunted children when compared to younger mothers. Current pregnancy status of the mother was not strongly associated with any of the malnutrition indicators. Mothers’ education was in general not significantly associated with any of the child`s malnutrition indicators. However, compared to children of fathers who did not attend school, children of fathers with higher education have lower odds of stunting (OR 0.829; 95% CI 0.744–0.924). Access to clean water was not associated with lower odds of wasting, stunting, and underweight, as none of the odd ratios was statistically significant. The number of children has a positive significant association with the odds of wasting (OR 1.041; 95% CI 1.005–1.078).
Mother’s BMI has no statistically significant association with stunting, wasting, and underweight. Household economic status, as measured by the wealth index, has no significant association with wasting and underweight. Children from the richest wealth group have lower odds of being stunted (OR 0.858; 95% CI 0.731–1.008), compared to children from the poorest household. Fathers’ occupation was in general not significantly associated with any of the children nutritional indicators.
Table 3 presents results of the logistic regression models for the extreme malnutrition outcomes (extreme stunting, extreme wasting, and extreme underweight). The results were in general similar to those presented in Table 2. In particular, the results suggest an inverse association between economic growth and extreme child wasting and extreme stunting. No statistically significant association is found between economic growth and the likelihood of being extremely underweight. However, the odds ratios for underweight, though not statistically significant, are also well below one, indicating a strong negative association between the income per capita growth and extreme underweight if estimated more precisely.
For the other covariates, household economic status, as measured by the wealth index, has a significant negative association with extreme stunting and extreme underweight, where children from the middle and the richer wealth group have lower odds of being extremely stunted and underweight compared to children from the poorest household. A child’s sex was significantly associated with extreme malnutrition. Compared to a male child, a female child has a lower odd of being extremely stunted, extremely wasted and extremely underweight. Being a twin is not a risk factor for extreme malnutrition. Higher odds of extreme stunting and underweight exist among children with risky birth intervals. Extreme malnutrition has a statistically significant negative association with child’s age, where older children have lower odds of being extremely stunted, extremely wasted, and extremely underweight when compared to an infant child. Though children, whose mothers are malnourished or currently pregnant, have higher odds of being extremely stunted, extremely wasted and extremely underweight, compared to children whose mothers are not malnourished or pregnant, none of the odds ratios were statistically significant. The number of children was also not significantly associated with any of the extreme malnutrition indicators. The father’s education has a significant negative association with extreme stunting, while the mother’s education and occupation were in general not significantly associated with any of the extreme malnutrition indicators.
5 Discussion
This study examines the association between child malnutrition in Egypt and economic growth, within a multivariate approach, using a logistic regression model applied to repeated cross-sectional data from five rounds of the Egyptian Demographic and Health Survey over the period 1992–2008. It contributes to the existing literature in several ways. To the best of our knowledge, this study is the first attempt to examine the economic growth-malnutrition linkage in the case of Egypt. Also, while most of the literature on this topic studied the effect of the country-level economic growth, an important contribution of the current study is that it directly relates the economic growth at the governorate level to the individual risk of malnutrition. We argue that by merely looking at the aggregate trends in per-capita income along with malnutrition rates in Egypt, it is difficult to reach any firm conclusion on whether or not economic growth has a negative effect on malnutrition. Instead, we suggest that linking economic growth at the smaller community level, such as governorates, would allow us to better assess the impact of economic growth on child nutritional outcomes. We also were able to link income inequality at the governorate level to child health by including governorates Gini index as an additional control variable in our regressions.
We find a statistically significant robust negative association between economic growth and four outcomes of child malnutrition (underweight, wasting, extreme wasting, and extreme stunting) in Egypt. This indicates that the rapid economic growth that took place in Egypt in the last two decades has in general helped in combating child malnutrition. While economic growth has the expected negative association with stunting and extreme underweight, the odd ratios were well below one but were not statistically significant. However, this statistical insignificance is mainly due to the very large standard errors, as the odd ratios are well below one and hence have an economic significance if estimated precisely. Results also show no statistically significant association between income inequalities as measured by the Gini index and any of the malnutrition outcomes.
We conducted a set of robustness checks by altering the model specification to check the stability of the findings. As a robustness check, though not reported but available in an online appendix, we estimated another specification by using unemployment rate per governorate as an alternative to GDP per capita. Under this specification, the level of unemployment has a statistically significant positive association with child stunting.
In addition to macroeconomic development, the literature documents other factors that are critical to child nutritional status. For instance, Kavle et al. (2014) argued that children in Egypt eat little to no animal-source foods, while junk food is a major complementary food. They suggested that junk food consumption is supported by parents and some healthcare providers, and it often replaces other nutritive foods. An additional factor that intensifies the malnutrition problem is that parents do not relate poor feeding practices to the low height for age. They commonly viewed stunting as hereditary. Jayachandran and Pande (2013) explained the fact that Indian children are shorter than Sub-Saharan African children by the parental preferences regarding higher birth order children, which is driven by culture norms of the eldest son preference. In Sub-Saharan African countries, Harttgen et al. (2012) suggested factors such as women’s education and low fertility as important to child health. In line with this evidence, findings of the current study reveal that child and household-level characteristics including; child age, sex, the birth interval of a child, and whether the child is a twin, father`s education, and household economic status are particularly important determinants of malnutrition outcomes in Egypt.
Results of the multivariate analyses show that boys are more likely to be malnourished than girls. The sex bias against boys is consistent with several previous studies (see e.g. Vella et al. 1992; Wells 2000; Van de Poel et al. 2007; Wamani et al. 2007) and is observed in many cultures, particularly in the very early ages. However, it is still poorly understood. At a previous study, Wamani et al. (2007) investigated whether there is systematic sex bias in stunting rates in children under-5 years of age in Sub-Saharan Africa, and found male children are more likely to be stunted. Sen and Sengupta (1983) noted that female children in India have better nutritional status in the first year compared to male children. They attributed the female children nutritional advantage to the phenomenon of lower neonatal mortality of girls versus boys. In line with Sen and Sengupta (1983) findings, Wells (2000) went deeper and suggested the natural selection of physiological traits that increases women survival and increase the vulnerability of boys to infection and diseases as a possible explanation for the sex difference in morbidity and mortality in early life.
In the current study, the fathers’ education is found to be more important for the children’s nutritional outcomes than mother’s education. While this is not in line with the considerable evidence in the literature about the important role of mother’s education in child health, similar findings have been observed in other areas of child development in Egypt. For example, Namoro and Roushdy (2009) found a stronger effect of fathers’ education than mother’s education on children’s years of schooling. Male domination and the limited women’s roles in household decision making in Egypt and particularly in rural areas relating to health, household purchases, limited control over household earning and restrict women’s mobility outside of the home may explain the differential effect of men and women’s education on child nutritional status.
The current study is not free from limitations. One limitation is its cross-sectional design, which limits reaching causal inferences. The availability of longitudinal data in the future could help overcome this limitation. Another limitation is that there could be other confounding factors that are associated with child malnutrition, but we did not control for due to data limitation, such as differences in geographical access to healthcare facilities, variations in the quality of health care services across regions, and cultural norms. However, we believe that the governorates fixed effects would capture at least part of these effects and hence reduce any omitted variables bias. Further research would be needed to examine the impact of these factors such as cultural norms, behavioral change due to income growth and regional variations in the quality of health care services on under-nutrition in Egypt. There is a concern that malnourished children are frequently sick, which hinders mother’s ability to work outside the house, and hence reduce economic growth. This endogeneity problem, if exists, is likely to have a minor impact, especially in our sample, where the number of working mothers outside the house is quite small in Egypt.
Another limitation is that child nutritional outcomes may reflect not only current exposure but also cumulative exposures to economic growth. One way to control for this cumulative exposure is to add the lagged value for per capita GDP as an extra control variable. However, this was not feasible due to data limitation, as data on income per capita at the governorate level are not published on an annual basis in Egypt. Though not reported but available upon request, as an attempt to account for this limitation, we estimated a specification with the lagged GDP of the previous round of the DHS as a control variable. This lead to a loss of one round of the DHS and the results, in general, did not change. We believe that adding the lag of the previous round of the DHS may not be accurate in capturing the cumulative exposure of the nutritional outcomes because the time gap between the rounds of the DHS are not uniform and the time gap between two of the rounds was about eight years.
6 Conclusion
We found a robust statistically significant negative association between economic growth, at the governorate level, and four outcomes of child malnutrition, namely; underweight, wasting, extreme wasting, and extreme stunting in Egypt over the period 1992–2008. Though a negative association was also found between economic growth and stunting and extreme underweight, the odd ratios were not statistically significant but were well below unity which indicates economic significance if precisely estimated.
Our results also reveal that child and household-level characteristics including child age, sex, birth interval, and whether the child is a twin, father`s education, and household economic status are particularly important determinants of malnutrition outcomes in Egypt. Unlike some evidence from the recent literature, the current study based on data from Egypt found supportive evidence that economic growth remains an effective instrument to combat child malnutrition and improves population health outcomes.
References
Alderman, H., Hoogeveen, H., & Rossi, M. (2006). Reducing child malnutrition in Tanzania: Combined effects of income growth and program interventions. Economics & Human Biology, 4(1), 1–23.
Barker, D. J., Eriksson, J. G., Forsén, T., & Osmond, C. (2002). Fetal origins of adult disease: Strength of effects and biological basis. International Journal of Epidemiology, 31(6), 1235–1239.
Bijlmakers, L. A., Bassett, M. T., & Sanders, D. (1998). Socioeconomic stress, health and child nutritional status in Zimbabwe at a time of economic structural adjustment: A three year longitudinal study (vol. 105). Nordic Africa Institute.
Case, A., &Paxson, C. (2006). Stature and status: Height, ability, and labor market outcomes (No. w12466). National Bureau of Economic Research.
Case, A., Paxson, C., & Islam, M. (2009). Making sense of the labor market height premium: Evidence from the British Household Panel Survey. Economics Letters, 102(3), 174–176.
Chen, X. K., Wen, S. W., Fleming, N., Demissie, K., Rhoads, G. G., & Walker, M. (2007). Teenage pregnancy and adverse birth outcomes: A large population based retrospective cohort study. International Journal of Epidemiology, 36(2), 368–373.
Conde-Agudelo, A., Rosas-Bermudez, A., Castaño, F., & Norton, M. H. (2012). Effects of birth spacing on maternal, perinatal, infant, and child health: A systematic review of causal mechanisms. Studies in Family Planning, 43(2), 93–114.
Currie, J., & Madrian, B. C. (1999). Health, health insurance and the labor market. Handbook of Labor Economics, 3, 3309–3416.
De Haen, H., Klasen, S., & Qaim, M. (2011). What do we really know? Metrics for food insecurity and undernutrition. Food Policy, 36(6), 760–769.
Dewey, K. G., & Cohen, R. J. (2007). Does birth spacing affect maternal or child nutritional status? A systematic literature review. Maternal & Child Nutrition, 3(3), 151–173.
El-Laithy, H., Lokshin, M., &Banerji, A. (2003). Poverty and economic growth in Egypt, 1995–2000. World Bank Policy Research Working Paper, (3068).
Frijters, P., Haisken-DeNew, J. P., & Shields, M. A. (2005). The causal effect of income on health: Evidence from German reunification. Journal of Health Economics, 24(5), 997–1017.
Gragnolati, M., Shekar, M., Gupta, M. D., Bredenkamp, C., & Lee, Y. K. (2005). India's undernourished children: a call for reform and action. Washington, DC: World Bank.
Harttgen, K., Klasen, S., & Vollmer, S. (2012). Economic growth and child undernutrition in Africa (No. 14). Global Food Discussion Papers.
Heltberg, R. (2009). Malnutrition, poverty, and economic growth. Health Economics, 18(S1), S77–S88.
Jayachandran, S., & Pande, R. (2013). Why are Indian Children Shorter than African Children? Department of Economics, Northwestern University, Mimeo.
Kavle, J., Mehanna, S., Saleh, G., Foaud, M., Ramzy, M., Hamed, D. et al. (2014). Examining factors associated with stunting in Lower Egypt in comparison to Upper Egypt. Bridging the gap between cultural beliefs and feasible feeding practices through Trials for Improved Practices, Washington DC.
Kheir-El-Din, H., & El-Laithy, H. (2008). An assessment of growth, distribution, and poverty in Egypt: 1990/91-2004/05. The Egyptian Economy: Current Challenges and Future Prospects, Cairo, pp. 13–52.
Maluccio, J. A., Hoddinott, J., Behrman, J. R., Martorell, R., Quisumbing, A. R., & Stein, A. D. (2009). The impact of improving nutrition during early childhood on education among Guatemalan adults. The Economic Journal, 119(537), 734–763.
Namoro, S., & Roushdy, R. (2009). Intrahousehold resource allocation in Egypt: Women empowerment and investment in children. Middle East Development Journal, 1(01), 105–121.
Pickett, K. E., & Wilkinson, R. G. (2007). Child wellbeing and income inequality in rich societies: Ecological cross sectional study. BMJ, 335(7629), 1080.
Pritchett, L., & Summers, L. H. (1996). Wealthier is healthier. Journal of Human Resources, 31(4), 841–868.
Ramakrishnan, U., Grant, F., Goldenberg, T., Zongrone, A., & Martorell, R. (2012). Effect of women’s nutrition before and during early pregnancy on maternal and infant outcomes: A systematic review. Paediatric and Perinatal Epidemiology, 26(s1), 285–301.
Rutstein, S. O., & Johnson, K. (2004). The DHS wealth index. DHS comparative reports no. 6. Calverton: ORC Macro.
Sen, A., & Sengupta, S. (1983). Malnutrition of rural children and the sex bias. Economic and Political Weekly, 18(19/21), 855–864.
Smith, L. C., & Haddad, L. (2002). How potent is economic growth in reducing undernutrition? What are the pathways of impact? New cross-country evidence*. Economic Development and Cultural Change, 51(1), 55–76.
Subramanyam, M. A., Kawachi, I., Berkman, L. F., & Subramanian, S. V. (2011). Is economic growth associated with reduction in child undernutrition in India? PLoS Medicine, 8(3), 448.
The Egyptian Cabinet Information and Decision Support Center (IDSC). (2013). The cost of hunger in Egypt implications of child undernutrition on the social and economic development of Egypt. Cairo: IDSC.
UNICEF. (2013). Improving child nutrition: The achievable imperatives for global progress. New York: UNICEF.
UNICEF, & World Health Organization. (2015). Improving nutrition outcomes with better water, sanitation and hygiene: practical solutions for policies and programmes.
United Nations Children’s Fund. (2013). Improving child nutrition: The achievable imperative for global progress. New York, USA: UNICEF.
Van de Poel, E., Hosseinpoor, A. R., Jehu-Appiah, C., Vega, J., & Speybroeck, N. (2007). Malnutrition and the disproportional burden on the poor: The case of Ghana. International journal for equity in health, 6(1), 21.
Vella, V., Tomkins, A., Borghesi, A., Migliori, G. B., Adriko, B. C., & Crevatin, E. (1992). Determinants of child nutrition and mortality in north-west Uganda. Bulletin of the World Health Organization, 70(5), 637.
Victora, C. G., Adair, L., Fall, C., Hallal, P. C., Martorell, R., Richter, L., et al. (2008). Maternal and child under nutrition: Consequences for adult health and human capital. The Lancet, 371(9609), 340–357.
Vollmer, S., Harttgen, K., Subramanyam, M. A., Finlay, J., Klasen, S., & Subramanian, S. V. (2014). Association between economic growth and early childhood under nutrition: Evidence from 121 Demographic and Health Surveys from 36 low-income and middle-income countries. The Lancet, Global Health, 2(4), e225–e234.
Wamani, H., Åstrøm, A., Peterson, S., Tumwine, J. K., & Tylleskär, T. (2007). Boys are more stunted than girls in sub-Saharan Africa: A meta-analysis of 16 demographic and health surveys. BMC Pediatrics, 7(1), 1.
Wells, J. C. (2000). Natural selection and sex differences in morbidity and mortality in early life. Journal of Theoretical Biology, 202(1), 65–76.
World Bank. (2014). International Economics Dept. Development data group. World Development Indicators. World Bank.
Acknowledgements
We would like to thank the anonymous reviewers, and the academic editor of this journal for the invaluable comments and suggestions that substantially improved the manuscript. We would also like to thank Stephan Klasen, Jurgen Maurer, Samer Atallah, and Doaa Omran for useful comments on an earlier version of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Rashad, A.S., Sharaf, M.F. Economic Growth and Child Malnutrition in Egypt: New Evidence from National Demographic and Health Survey. Soc Indic Res 135, 769–795 (2018). https://doi.org/10.1007/s11205-016-1515-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-016-1515-y