
Abstract
This study explores country differences in late-life loneliness in Europe among men and women and establishes the role of micro-level differences in socioeconomic status, health, and social variables in these patterns. We use cross-sectional, nationally representative data from the Generations and Gender Survey. The analysis comprises 33,832 Europeans aged 60–80 from 11 countries. A six-item short version of the de Jong-Gierveld Scale is used to measure loneliness, yet we employ a different method of calculating loneliness scores than in prior work. Findings show considerable between-country heterogeneity in late-life loneliness, especially among women. The rate of a quite severe level of loneliness is 30–55 % among men and women in Eastern Europe, compared with 10–20 % among their peers in Western and Northern Europe. Loneliness is strongly associated with lower socioeconomic status, poorer health, and not having a partner. More than half of the country variance in loneliness is mediated by health, partnership status, and socioeconomic disparities across countries. Differences in societal wealth and welfare and cultural norms may account for some of the unexplained country variance in loneliness.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Loneliness is widely perceived as a problem of old age, as part of “normal” aging. In a U.S. survey, 55 % of those aged under 65 and 33 % of those aged over 65 believe that loneliness is a serious problem “for most people over 65” (Abramson and Silverstein 2006). Similarly, 86 % of Swedes (aged 18–75) believe that “almost half of retirees often feel lonely” (Tornstam 2007). Loneliness can be considered the outcome of the subjective and negative evaluation of the gap between an individual’s desired and actual quantity and quality of social relationships (de Jong-Gierveld et al. 2006). The belief that loneliness is common in old age has validity as aging often involves events and conditions associated with a higher risk of loneliness, including retirement, bereavement, somatic illness, and low socioeconomic status (Yang and Victor 2011). Research shows, however, that only 5–15 % of adults aged 60–80 report frequent feelings of loneliness (Dykstra 2009; Pinquart and Sörensen 2001; Victor et al. 2000). Yet this literature is based primarily on data from richer, Western countries with advanced welfare systems. Age-related increases in loneliness may be stronger and occur earlier in countries with poorer living conditions and welfare provision.
There is wide variation across European countries in the distribution of risk factors for late-life social isolation and loneliness. Socioeconomic deprivation, for example, is far more prevalent among elders in Eastern than in Western European countries (see “Appendix” for a table of selected demographic and economic data for the countries in this study). Since the end of the communist regimes, an increasing number of Eastern European retirees face severe financial strain due to rising inflation and decreasing value of pensions (Botev 2012). The lowest old-age poverty rates are found in the Nordic countries, reflecting a generous and universal welfare system (Hvinden 2010). The increased risk of loneliness with low socioeconomic resources is attributed to less opportunity for social participation and a smaller and less supportive social network (Pinquart and Sörensen 2001). The different health status of older Europeans also warrants concern. Health and mobility are central for social participation, and self-reported health is in general much poorer among elders in Eastern than in Western European countries (Deaton 2007, see also Table 1). The recent decrease in life expectancy and self-reported health among older Eastern Europeans reflects a combination of unhealthy lifestyle and poor healthcare services as well as financial difficulties that prevent elderly people from accessing medical services (Lipsitz 2005). European elders also face different social risks for loneliness. Because of relatively low life expectancy among men, the proportion of widows is much higher among Eastern than Western older European women (Botev 2012; Goodwin 2006). The social network of older Eastern Europeans may also suffer due to decreasing fertility and increasing out-migration of younger adults (OECD 2012a). Many older adults thus lack children and grandchildren to care for them, and when government provision falls short, they may lack resources to help them combat loneliness.
Cultural differences may counteract—or exacerbate—country differences in the risk of late-life loneliness. Southern and Eastern European countries are generally characterized by a more familistic and collectivistic orientation than the more individualistic Northern and Western European countries (Reher 1998; Saraceno and Keck 2010). In familistic cultures, people tend to emphasize and expect strong ties within the family and community. Such cultures may prevent loneliness by promoting social integration. However, as others have noted (Johnson and Mullins 1987; Jylha and Jokela 1990), the high expectations of strong ties may increase feelings of loneliness if these expectations are not met. Placing a high value on close family ties may thus make matters worse for seniors in countries with high rates of widowhood, decreasing fertility rates, and increasing out-migration (see “Appendix”).
Understanding national differences in loneliness may provide valuable insights into macro-level influences on late-life well-being (Ploubidis and Grundy 2009). Comparative findings may help to enhance our understanding of possible variations between European countries in the well-being of older people and inform the debate about public health policy relevant to life quality in older age groups. Yet cross-national data and findings on loneliness are still sparse. There is much data from Western Europe but comparatively little data on Scandinavia, Central Europe or, especially, Eastern Europe (Dykstra 2009; Yang and Victor 2011).
A large body of Western cross-sectional and longitudinal studies have explored associations between age and loneliness (for reviews, see Dykstra 2009; Pinquart and Sörensen 2001; Victor et al. 2009; Yang and Victor 2011). Loneliness is shown to be quite stable between age 25 and 80 but to increase rapidly above age 80. In young old age (age 60–80), the percentage that reports frequently feeling lonely is 5–10 %, while an additional 20–40 % report occasional feelings of loneliness. In advanced old age (80+), about 40–50 % often feel lonely (Dykstra 2009; Yang and Victor 2011).
The available cross-national European literature shows wide variation in the prevalence of late-life loneliness. Two studies use data from up to 15 countries based on the SHARE survey, which covers countries from Northern Europe to the Mediterranean region (Fokkema et al. 2012; Sundstrom et al. 2009). Findings show that older adults in Southern and Central European countries are generally lonelier than their peers in Northwest Europe. This pattern is confirmed in a study of 25 European countries (age 60–101) from the European Social Survey (ESS) (Yang and Victor 2011). The ESS study, in addition to two studies of up to six European countries from the GGS (age 60–79) (de Jong-Gierveld and van Tilburg 2010; de Jong-Gierveld et al. 2012), include some Eastern European countries. Findings show that rates of loneliness in these countries are the highest in Europe.
The comparative findings have several limitations. First, none of the above studies separate results by gender. Doing so is important as the different life course trajectories of men and women may lead to different risks of social isolation and loneliness in old age. Reviews of Western findings show that older women generally report a slightly higher level of loneliness than older men, and that this gap increases with higher age (Pinquart and Sörensen 2001; Nicolaisen and Thorsen 2014). Gender differences in loneliness are completely or largely explained by differences in health, living arrangements, and socioeconomic status (ibid.). The heightened risk of women may be more pronounced in Southeastern European countries given the higher prevalence of financial difficulties, widowhood, and health problems among older women in many of these countries than in Western European countries (Petrov 2007, see also Table 1).
Second, few studies examine the role of socioeconomic disparities in cross-national patterns of late-life loneliness (Yang and Victor 2011). Low socioeconomic status (as indicated by education or income) is consistently associated with higher rates of loneliness (Pinquart and Sörensen 2001). Socioeconomic status may be considered an “upstream” or distal factor affecting the more proximate or predisposing conditions for social contact and loneliness. For example, socioeconomic status may relate to self-esteem and social skills, making people more confident and uninhibited in social interactions and more attractive to others. Greater educational attainment also enables persons to demonstrate greater competence and mastery over their lives, which in turn allows individuals to shape behavior in a way that increases social integration, promotes healthy psychological states, and reduces risk of loneliness in old age (Mirowsky and Ross 2007). High socioeconomic status is also associated with a more diverse social network, more friendship ties, and more friendship support (Pinquart and Sörensen 2001). Different indicators of socioeconomic status may have different associations with loneliness, however. For example, low levels of income and difficulty in making ends meet in households have been associated with chronic stressful situations and fewer opportunities to engage in joyful activities (Hawkley et al. 2008). A higher educational level has been shown to reduce late-life loneliness through its role in decreasing neuroticism and stress and increasing social support (Bishop 2007).
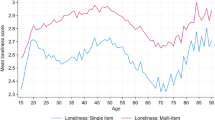
Third, most analyses are based on single-item measures of loneliness. Single items demonstrate less reliability and validity than multi-item scales (see Hansen 2010). Importantly, single item loneliness measures are more prone to social desirability bias because people may be unwilling to admit to feeling “lonely” (Dykstra 2009). The above-reviewed prevalences of loneliness, all based on single-item measures, may thus be under-representations of the true levels of loneliness. Furthermore, the stigma of admitting to loneliness may vary across social groups. It is likely, for example, that different nationalities and age cohorts vary in the extent to which they openly express negative subjective experiences, with country and age differences in loneliness as a result. There is thus a general preference for loneliness scales, with questions that probe loneliness more indirectly—avoiding the words “lonely” or “loneliness”—and also cover different aspects of loneliness.
Fourth, a different methodological issue concerns the choice of cutoff on the short de Jong-Gierveld scale. We argue that the cutoff recommended by the scale developers is rather low and lumps together mild and more severe levels of loneliness (see below under Methods). Research on loneliness is usually motivated, at least in part, by the fact that loneliness predicts later negative development in a range of physical and mental health outcomes (Hawkley et al. 2008). These effects may be stronger, or only observed, at higher levels of loneliness. Researchers may thus want to concentrate on moderate to severe levels of loneliness.
This study explores the prevalence of a quite serious level of loneliness for men and women across 11 countries that represent different regions of Europe. We first report the country-specific prevalence of loneliness in different age groups between 18 and 80, to obtain an overall picture of how age relates differently to loneliness across countries. Next, as our primary concern is with older people, we focus on the 60–80 age group and explore patterns and mediators of cross-national differences in loneliness. We pay specific attention to the role of socioeconomic status, social network variables, and physical health as mediating factors. We use an established and cross-culturally validated multi-item scale to measure loneliness.
2 Methods
2.1 Data
We use data from the Generations and Gender Survey (GGS). The survey forms part of the Generations and Gender Programme (GGP). The GGP is a system of national GGS surveys and contextual databases based on a number of European and some non-European countries. The GGP aims to improve the understanding of demographic and social developments and the factors that influence these developments. The GGS fieldwork guidelines, developed by a consortium of demographic institutes, statistical offices, and universities, specify random sampling of the non-institutionalized population aged 18–79. The GGS aims to ensure cross-national comparability of data also by using standard instruments.
We first use the whole age range (18–80) (n = 132,319), and later restrict our analysis to the ages 60–80 (n = 33,832). We use data from the 11 countries that implemented the loneliness measurement and the independent variables. We use a listwise deletion procedure. Data were collected between 2004 and 2011, using face-to-face interviews. Year of data collection is unrelated to loneliness, net the effect of country (not shown). It is worth noting that the Norwegian GGS posed questions about loneliness in a postal questionnaire. Average response rate in GGS is 67.5 %, ranging from 42 (Belgium) to 97 % (Romania) (Fokkema et al. 2014).
2.2 Dependent variable
Loneliness is measured by the six-item version of the de Jong-Gierveld Loneliness Scale (de Jong-Gierveld et al. 2006; de Jong-Gierveld and van Tilburg 2010). The reliability, validity, and structural characteristics of the scale are of high quality, and the instrument has proven cross-national equivalence, thus allowing for intercultural comparison (Van Tilburg and De Leeuw 1991; de Jong-Gierveld and Van Tilburg 2010). For example, the scale has been tested for seven GGP countries (France, Germany, the Netherlands, Russia, Bulgaria, Georgia, and Japan) and found reliable and valid for each of the countries under investigation (de Jong-Gierveld and van Tilburg 2010).
The scale encompasses three positively formulated items (There are plenty of people that I can lean on in case of trouble; There are many people that I can count on completely; There are enough people that I feel close to) and three negatively formulated items (I experience a general sense of emptiness; I miss having people around; Often, I feel rejected). None of the items refer directly to loneliness. The items have three response categories: “no” (0), “more or less” (1), and “yes” (2). After reversing positively formulated items, a simple additive score index (0–12) was created (α = 0.75, range 0.62–0.79 across countries) in which higher scores indicate higher levels of loneliness. Our method of calculation uses the full breadth of responses, consistent with modal calculations of index scores for other psychological constructs (e.g. life satisfaction, depression, self-esteem) and for use of the UCLA Loneliness Scale (e.g. Lasgaard 2007).
Instead of the additive score, researchers typically calculate a loneliness index by applying a count score. The method of the scale developers (de Jong-Gierveld and van Tilburg 1999), since adopted by others, is to create an index score that counts the number of items on which the respondent reports “more or less” or “higher” (“no” on positively formulated items, “yes” on negatively formulated items) loneliness. This procedure ignores the difference between “more or less” and higher scores. According to the developers, the reasoning was that, because of the taboo of expressing loneliness, “more or less” could have the same meaning as higher scores (personal communication). The count score approach thus ignores the rank order of the responses and leads to a loss of information. This index ranges from 0 to 6 (intensely lonely). Individuals’ score as reported by the count score (0–6) and current (0–12) approach in our dataset correlates at 0.92.
The different dichotomization of index scores may have more important implications. It has been common in the traditional approach to dichotomize the count score (0–6) and let scores ≥2 indicate “lonely” (de Jong-Gierveld 2006; de Jong-Gierveld et al. 2012). Hence, being classified as lonely only requires two “more or less” responses. This level of loneliness can be viewed as “mild” or even “normal”. Not surprisingly, this cutoff yields very high rates of loneliness: in 6 of the 11 countries used in the current study, more than two-thirds (69–87 %) of the respondents aged 60–80 are “lonely”.
We have dichotomized the additive score (0–12) and let scores ≥6 indicate “lonely”. Hence, we use a much higher or stricter cutoff, whereby “lonely” refers to those reporting on average “more or less” on all items (note that this result may also be the outcome when half of the items indicate low loneliness and half indicate high loneliness). We chose this cutoff because we are interested in a more serious and problematic level of loneliness, which may have substantial consequences for physical and mental health. In the ages 60–80, 21 % are classified as lonely in the aggregate analytical sample.
Loneliness can be conceptualized as comprising two dimensions: emotional and social loneliness (Weiss 1973). The former arises out of the loss or absence of a close emotional attachment, the latter out of the absence of an engaging social network. We use a loneliness measure that allows distinguishing between the two dimensions. However, because results are rather uniform for the two dimensions (ancillary analysis, not shown), we present analyses for one general loneliness dimension.
2.3 Independent variables
We control for several country-variant factors associated with loneliness (Pinquart and Sörensen 2001). The respondents’ age is included as loneliness is generally associated with older age. Living arrangement measures co-residency with partner and others, in four categories: lives alone, lives with partner, lives with partner and others, and lives with others (not partner). We include the number of (biological) children as children may represent an important source of social contact and support. In the multivariate analyses, numbers above 3 are coded as 3. Health refers to subjective health status, ranging from very poor (1) to very good (5). We also include a measure of disability (chronic health problem or limiting longstanding illness: no/yes), which captures the respondent’s functional health. Three socioeconomic variables are included. Educational level is classified into the following categories: low (ISCED 0–2), medium (ISCED 3–4), and high (ISCED 5–6). Employed (no/yes) is included as employment may reduce loneliness by fostering supportive network ties and access to support. Financial situation (perceived difficulties in making ends meet) ranges from 1 (great difficulties) to 5 (very comfortable).
2.4 Analytical strategy
We used X 2 tests and F tests to compare the proportions and means of loneliness between groups. All multivariate analyses use ordinary least squares (OLS) regressions. We use OLS regression for reasons of familiarity and ease of interpretation. Using OLS regression when the dependent variable is ordinal may be problematic since it violates the assumption of interval level data. We thus performed all the analyses using an ordinal-probit model (ancillary analyses) and the results were almost identical to those using OLS regression. Ferrer-i-Carbonell and Frijters (2004) have shown that the choice of methodology (OLS regression, ordinal-probit, or ordinal-logit techniques) in this context makes little difference to the empirical results. Analyses are run separately for men and women.
3 Results
To obtain an overall picture of how age relates differently to loneliness across countries, we report first the country-specific prevalence of loneliness in age groups 18–80. Figure 1 shows the prevalence of loneliness by age and country among men. The positive association between age and loneliness is stronger in Eastern European than in Northwestern European countries. As a result, cross-national disparities in loneliness increase with older age. In Norway, France, Belgium, Poland, and Germany, the rates of loneliness are very low (5–9 %) in the age cohort 18–30 and almost twice as high (10–13 % per country) in the age cohort 71–80. The latter rates are still much lower that the rates found among older adults in the other countries. In Russia, the Czech Republic, Romania, and Lithuania, rates range from 9 to 15 % in the youngest group, and from 25 to 32 % in the oldest group. The largest age differences are found in Bulgaria (from 16 to 38 %) and Georgia (from 14 to 43 %).

Prevalence of loneliness by age and country. Men. Note: Percentages by age and country are available by the authors on request
Figure 2 shows that cross-national differences in the patterning of loneliness with age are even more pronounced for women. In Norway, Belgium, Germany, France, and Poland, rates of loneliness are low in the youngest age group (4–12 %) and moderate (11–17 %) in the oldest age group. In the Czech Republic, Russia, Lithuania, and Romania, the rates are moderate (11–20 %) in the youngest group, but relatively high (28–38 %) in the oldest group. Bulgaria (from 20 to 52 %) and Georgia (from 13 to 53 %) show the strongest age-related increases in loneliness. With some exceptions, rates of loneliness in the oldest age cohorts of men and women are between double and triple the rates in the youngest age cohorts.

Prevalence of loneliness by age and country. Women. Note: Percentages by age and country are available by the authors on request
Next, we focus on the ages 60–80 and explore patterns and mediators of cross-national differences in mean levels of loneliness. Table 1 presents the descriptive statistics of the variables used in the analyses per country. Mean age is quite similar across countries. The living arrangements of older adults vary considerably between countries, especially among women. Older adults in the Northern and Western European countries, compared with their peers in other parts of Europe, more often live with a partner (especially women) and more often have a large number of children, but less often live with others beside a partner (usually children). Rates of solitary living is generally higher among women in the Eastern European than in the Northern and Western European countries. This rate is notably lower in Georgia, Bulgaria, and Romania than in the other Eastern European countries. Furthermore, older adults in the Northern and Western countries are relatively more financially satisfied and more often employed and highly educated. The differences in financial satisfaction are noteworthy: Western Europeans on average score around four (“…able to make ends meet…fairly easily”) and Eastern Europeans around two (“…with difficulty”). In the Western countries, only 1–4 % report to have “great difficulties” in making ends meet—far fewer than in countries like Romania (20 %), Russia (32 %), Bulgaria (43 %), and Georgia (43 %) (not shown). Older Western Europeans also report better health status and fewer of them have disabilities than older adults in the Eastern European countries. Finally, older adults in Northwest Europe report a lower prevalence and mean level of loneliness than other older adults. The prevalence of loneliness in the age group 60–80 varies for men from 8.4 % (Norway) to 38.1 % (Georgia), and for women from 8.1 % (Norway) to 46.8 % (Georgia). Generally, country prevalence differences larger than 3 % are significant at the 0.05 level (not shown).
In Table 2, country and controls are regressed on loneliness separately for men and women aged 60–80. Unless otherwise noted, associations are similar for men and women (gender differences explored in ancillary analyses). The first model shows the bivariate country-level mean differences in loneliness. Older Norwegian men and women report significantly lower levels of loneliness than their peers in the other GGP countries.
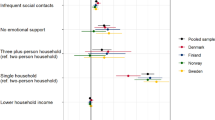
The second model takes into account age, living arrangement, children, employment status, and education. These factors partially or fully mediate differences in loneliness among the Western European countries, but only mediate a small portion of the association between loneliness and Eastern Europe. The model also shows that higher age is associated with greater loneliness among men and women, yet the association is significantly stronger among women (p < 0.01). We have explored the quadratic effects (age2) in ancillary analysis, but the results were not significant. With regard to living arrangement, the largest difference in loneliness is found between those with and those without a partner in the household. Having a partner is significantly more strongly related to men’s than women’s loneliness (p < 0.01). Also, loneliness is inversely related to educational level and the number of children, and more strongly so for women than men (p < 0.01). We also note that, in the 60–80 age group, loneliness is unrelated to employment status.
In the third model, differences in financial satisfaction are taken into consideration. Financial satisfaction relates to lower loneliness for both genders and mediates part of the effect of education. Financial satisfaction mediates only a small portion of the effect of living arrangement. Moreover, because of the above-discussed prevalence of financial difficulties in Eastern European countries, including financial satisfaction in the model strongly attenuates the relatively high level of loneliness in Eastern European countries. Once financial satisfaction is held constant, there also are no significant differences in loneliness between the Western European countries.
In the final model, differences in health (subjective health and disability) are taken into consideration. Health status is more closely linked with women’s than men’s loneliness. Subjective health is strongly related to loneliness for both genders, but more strongly for women (p < 0.01). Similarly, disability is significantly associated with women’s but not men’s loneliness.
In supplementary analyses using a mixed model with random country intercepts, we find that the control variables account for 57 % of the country-variation in loneliness for men (age 60–80), and similarly 69 % of the variation for women (not shown). Only 5 and 9 % of the country-variation in loneliness for men and women, respectively, are accounted for by the control variables in model two. Hence, the bulk of the explained country variation is explained by financial satisfaction and subjective health.
After controlling for compositional differences, loneliness is actually higher in Norway than in some of the other Western European countries and Poland. Yet, the relatively high level of loneliness in the Eastern European countries (except Poland) is not fully accounted for: Net of other variables, older Eastern European men and women have levels of loneliness that far exceed those of their peers in Western European countries.
Controlling for compositional differences may not solve problems concerning the comparability of age groups from countries with different life expectancies. To compare age-groups that are likely to reflect similar life stages, we analyze individuals aged up to 10 years younger than the average (gender-specific) life expectancy of their country (see Table 4 in the “Appendix”). For example, for Belgium, where life-expectancy for men is 77.6, we use data from men aged between 68 and 78. If the average life-expectancy exceeds age 80 (see Table 3 in the “Appendix”), we use ages 70–80. For example, for Norway, where life-expectancy for women is 82.7, we use data from women aged 70–80. The findings show large country differences in loneliness (also after controls), although the differences are smaller than when using the ages 60–80 (Table 2).
4 Discussion
The current study corroborates and extends previous research showing considerable between-country heterogeneity in late-life loneliness across European countries and regions. We use a loneliness instrument with better psychometric properties than the single-item measures typically used in the literature, thus enhancing the reliability of the findings. Compared with prior work, we also broaden the representation of Eastern European countries and we measure a more serious level of loneliness. In harmonized nationally representative data from 11 countries, we verify the existence of a North-West versus Central-East divide in late-life loneliness in Europe. Loneliness is up to five times more prevalent among older men and women in Central and Eastern Europe (30–55 %) than among their peers in Northwestern Europe (10–20 %). Poland is an exception among the former socialist countries, with loneliness levels akin to that of Western European countries. Norway has the lowest prevalence of loneliness, a fact that may be underestimated because Norway decreased the influence of social desirability biases by posing questions about loneliness in a more anonymous way (questionnaire) than the other GGP countries (personal interviews). We further extend the literature by exploring gender differences in cross-national patterns of late-life loneliness. Findings show that in the former socialist countries but not in Northwestern European countries, rates of loneliness among older adults are generally 5–15 % higher for women than for men.
Although gerontologists have for some time debunked the myth that loneliness is inherent to old age, researchers may have gone too far in arguing that loneliness is generally stable until very old age (e.g., Dykstra 2009; Victor et al. 2009). A pattern of relative stability only holds for Western countries, where rates of intense loneliness in old age (age 70–80) are actually comparable to those among young adults. In many former socialist countries, however, between a third and half of the older population is lonely, many more than the 10–20 % who are lonely among young adults in these countries. Our strict operationalization of loneliness highlights the significance of these results: “Lonely” individuals report a quite serious level of loneliness.
Why are older Eastern Europeans particularly vulnerable to loneliness? Part of the answer lies in their socioeconomic status, health, and social networks and thus their opportunities for social participation and for experiencing rewarding social relationships. A large part—almost two-thirds—of the country variation in late-life loneliness is explained by inequalities in socioeconomic resources, health, and marital status. Similarly, the pronounced risk of loneliness faced by Eastern European women can be attributed to the fact that a relatively high number of these women are aging without a partner and with health problems and financial concerns.
The micro-level risks must be interpreted in the context of societal factors. Individuals are embedded in larger material and societal contexts that shape the quality of living conditions and create opportunities for social integration (de Jong-Gierveld and Tesch-Romer 2012). Central to this discussion is the role and scope of the welfare state.
Two contradictory perspectives can be put forward on the role of the welfare state in shaping social integration and loneliness. One emphasizes that generous welfare states may promote better conditions for social integration and self-reliance and thus enable and stimulate social participation, in particular among individuals with health limitations or low socioeconomic resources (Hvinden 2010). The other perspective, the crowding-out hypothesis, warns that strong welfare states may decrease civic engagement by taking over tasks traditionally carried out by families, local communities, and social networks (Saltkjel et al. 2013; van Oorschot and Arts 2005).
Empirical evidence generally supports the first perspective. Both current and prior research associates a higher national level of welfare generosity with less loneliness among older people (e.g., Fokkema et al. 2012; Sundstrom et al. 2009). Similarly, the findings presented and reviewed by Saltkjel et al. (2013) show that a comprehensive welfare state is positively associated with social participation (both formally and informally). It appears that in countries with generous social security schemes, where per capita public expenditure on health and welfare services is among the highest in Europe, people enjoy better social and psychological well-being than in countries where the state provides less. In many of the former socialist countries, formal support structures are largely absent (Iecovich et al. 2004). Hence, older people in Eastern Europe may be particularly prone to loneliness because of inequalities in health, social integration, and socioeconomic resources, which in turn may be driven by macro-level socioeconomic inequalities and different levels of welfare provision.
The fact that wide country heterogeneity in loneliness remains after controlling for various living conditions prompts the adoption of a cultural perspective to understand this variation. The north of Europe is characterized by weak family and community ties and the Mediterranean and Eastern European countries by strong such ties (Reher 1998; Viazzo 2010). In “weak family” areas, individualistic values tend to dominate, whereas collectivistic values predominate in “strong family” contexts. Individualistic contexts are also characterized by increasing proportions of people living alone, increasing divorce rates, and declining fertility and size of kinship networks. Unsurprisingly, therefore, stereotypes tend to equate the individualism and de-familialism of Northern Europe with high levels of social isolation and loneliness (Dykstra 2009). It is thus a paradox that older people are less lonely in more individualistic and less familistic cultures.
Several authors point to the importance of considering people’s frames of reference and normative orientations in the cultural context of countries under investigation (Jylha and Jokela 1990; Johnson and Mullins 1987). Loneliness occurs when the quality of one’s social relationships falls short of the expected or desired quality of social relationships. Johnson and Mullins (1987) introduced the term “loneliness threshold” to refer to the level at which loneliness arises. Southern and Eastern Europeans, because of high expectations of strong family and community ties, may have a lower loneliness threshold than other Europeans. A low loneliness threshold may make matters worse for seniors in countries with high rates of widowhood, decreasing fertility rates, and increasing out-migration. Moreover, it may be that political upheavals, economic insecurity, and greater socioeconomic inequalities have eroded feelings of trust and social integration, which in turn increased the risk of loneliness among older adults in Eastern Europe (Rokach et al. 2001). In sum, the combination of a low loneliness threshold and negative changes in social integration may help to explain high levels of loneliness in former socialist countries.
Several other hypotheses have been advanced to account for country variations in late-life loneliness. Rokach (2007) proposes that many older Eastern Europeans, because they have lived under communist rule when citizens’ needs were generally cared for by the state, may feel more doubtful about their personal abilities and coping resources. In a similar vein, Dykstra (2009) asks whether older members in former socialist countries are lonelier because they are unaccustomed to fending for themselves and their lesser self-reliance makes them more vulnerable to the relationship losses that accompany old age. Pietilä and Rytkönen (2008) ask whether people in former communist countries report higher levels of loneliness because a “litany of suffering” is a way of articulating the hopelessness and insecurities they have incurred in the transition to capitalism. Another issue concerns the comparability of age groups from countries with different life expectancies. Theoretically, loneliness might generally be “stable until very old age” (e.g., Dykstra 2009), but that aging and the onset of “very old age” occur earlier in countries with lower life expectancy. We are not fully able to account for this possibility by controlling for self-rated health and the presence of disability alone. Ideally, we need to control for other aspects of biological (objective health, sensory problems), psychological (cognition, memory, sense of control), and social aging (network and support deficits). This possibility may explain some country differences but not the fact that loneliness is higher even among younger Eastern Europeans than among older Western Europeans (see Figs. 1, 2). Similarly, marked country differences in loneliness are also indicated when we compare country-specific age-groups that are likely to reflect similar life stages (see Table 4 in the “Appendix”).
5 Limitations and Future Research
Several limitations in this study highlight areas for future research. First, our study lacks a solid basis for explaining country differences in late-life loneliness. For example, it would be interesting to explore the role of values, standards, and attitudes concerning social contact and integration. Also, we lacked information about important aspects of older adults’ social network, such as social contact and access to, or receipt of, social support. Measures of “objective loneliness” (actual contact with family, friends, etc.) would have provided an opportunity for assessing the existence and importance of differences in “loneliness threshold” for variations in self-reported loneliness between nations. We would also have liked to investigate the oldest old (age 80+), for whom rates of loneliness are likely higher and country differences possibly even more pronounced. Another direction for future research concerns the role of welfare state spending. To what extent and by what mechanisms can welfare state spending affect loneliness? Can country indicators of welfare explain cross-national differences in loneliness over and above individual-level factors? To answer such questions we need more countries to analyze and to adopt a multilevel analytical framework.
We are also limited in several ways by the fact that we are analyzing only one time point. For example, we do not know whether some of the cross-national differences in late-life loneliness stretch back to earlier times. Furthermore, because of the inevitable selection biases in larger surveys of healthier, non-frail, and non-institutionalized adults, the presented prevalences of loneliness are likely underestimates. This problem is compounded by the fact that sensitive questions about loneliness were posed in personal interviews (except in Norway), thus increasing social desirability issues in these measurements. Also, because in all countries investigated lower educated people are underrepresented (Fokkema et al. 2014), and low education is tied to more loneliness, rates of loneliness may be underestimated, perhaps especially in countries with low response rates.
Moreover, cross-national comparative research on psychological outcomes has some methodological challenges. Notably, different age groups from different cultures and languages may demonstrate unique understanding of questions or may be differently inclined to admit to feelings of loneliness. Further, there is likely important between-country variation, especially among the Eastern European countries, that we have not addressed.
6 Conclusion
Gerontologists have long since debunked the myth that loneliness is an inherent characteristic of old age. However, in some Eastern European countries, so far under-researched in the literature on loneliness, between a third and a half of the older population report a rather serious level of loneliness. Loneliness is particularly high among older women in this region. Loneliness is a comparatively rare experience in Northwestern European countries. The country differences in late-life loneliness are also generally in agreement with, although seemingly more pronounced than for, country differences in depression (Ploubidis and Grundy 2009) and life satisfaction (Deaton 2007). Country differences in the risk of late-life loneliness varies systematically with macro-level inequalities in socioeconomic status, health, and social integration. Findings attest to and reflect the unequal conditions of aging across Europe and indicate serious deficits in late-life quality of life in some European countries.
The prevention and reduction of loneliness have ramifications beyond the social realm. Loneliness appears to hasten physiological decline and increase the use of health and care services (Hawkley and Cacioppo 2007). Alleviating loneliness is thus important for both individuals and societies. The costs of loneliness may thus exacerbate the costs of population aging, and especially so in Eastern European countries. The combination of economic and social strain and an aging population implies potentially greater harm to the well-being of large numbers of older people.
This study provides a snapshot of the current situation, and the cross-sectional design prevents causal conclusions from being drawn about age and loneliness relationships. It thus remains an open question whether the prevalent loneliness among older Eastern Europeans will persist among future cohorts of elders. As discussed, the high prevalence of loneliness among older Eastern Europeans may be tied to social and economic changes since the fall of communism and the high pressures and expectations of communality. Firstly, loneliness may decrease in this region insofar as societal conditions stabilize or improve. Furthermore, recent data suggest some important generational divides in many Eastern European countries. For example, younger cohorts are more highly educated (OECD 2012b) and report a higher sense of control and more individualistic values (Pew Research 2009). Insofar as more recent cohorts of Eastern Europeans acquire a stronger sense of personal responsibility, they may take more active step to establish and maintain social network ties and access to support than older cohorts. A higher sense of control may also help them achieve desired social goals despite structural constraints. The effect on loneliness of a possible transition away from familistic/collectivistic values toward a more individualistic orientation may be more ambiguous. On the negative side, it may imply a weakening of social network ties. On the positive side, for those who are less socially integrated, lower expectations of strong family and community ties may reduce loneliness. The dynamics of cross-national disparities in late-life loneliness thus merits investigation in future comparative studies.
References
Abramson, A., & Silverstein, M. (2006). Images of aging in America 2004. Washington: AARP and the University of Southern California.
Bishop, A. J. (2007). The indirect influence of educational attainment on loneliness among unmarried older adults. Educational Gerontology, 33(10), 897–917.
Botev, N. (2012). Population ageing in Central and Eastern Europe and its demographic and social context. European Journal of Ageing, 9(1), 69–79.
de Jong-Gierveld, J. (2006). Societal trends and lifecourse events affecting diversity in later life. In S. O. Daatland & S. Biggs (Eds.), Ageing and diversity: multiple pathways and cultural migrations (pp. 175–188). Bristol: Policy Press.
de Jong-Gierveld, J., Dykstra, P. A., & Schenk, N. (2012). Living arrangements, intergenerational support types and older adult loneliness in Eastern and Western Europe. Demographic Research, 27, 167–199.
de Jong-Gierveld, J., & Tesch-Romer, C. (2012). Loneliness in old age in Eastern and Western European societies: Theoretical perspectives. European Journal of Ageing, 9(4), 285–295.
de Jong-Gierveld, J., & van Tilburg, T. (1999). Manual of the loneliness scale. Amsterdam: Vrije Universiteit.
de Jong-Gierveld, J., & van Tilburg, T. (2010). The de Jong-Gierveld short scales for emotional and social loneliness: Tested on data from 7 countries in the UN generations and gender survey. European Journal of Ageing, 7, 121–130.
de Jong-Gierveld, J., van Tilburg, T., & Dykstra, P. A. (2006). Loneliness and social isolation. In A. Vangelisti & D. Perlman (Eds.), Cambridge handbook of personal relationships (pp. 285–500). Cambridge: University Press.
Deaton, A. (2007). Income, aging, health and wellbeing around the world: Evidence from the Gallup World Poll. Journal of Economic Perspectives, 22(2), 53–72.
Dykstra, P. A. (2009). Older adult loneliness: Myths and realities. European Journal of Ageing, 6(2), 91–100.
Ferrer-i-Carbonell, A., & Frijters, P. (2004). How important is methodology for the estimates of the determinants of happiness? Economic Journal, 114, 641–659.
Fokkema, T., de Jong-Gierveld, J., & Dykstra, P. A. (2012). Cross-national differences in older adult loneliness. Journal of Psychology, 146, 201–228.
Fokkema, T., Kveder, A., & Liefbroer, A. (2014). Report and recommentations for sample and data adjustment procedures. GGP (deliverable).
Goodwin, R. (2006). Age and social support perception in Eastern Europe: Social change and support in four rapidly changing countries. British Journal of Social Psychology, 45, 799–815.
Hansen, T. (2010). Subjective well-being in the second half of life: The influence of family and household resources. Dissertation. University of Oslo, Faculty of Medicine.
Hawkley, L. C., & Cacioppo, J. T. (2007). Aging and loneliness: Downhill quickly? Current Directions in Psychological Science, 16(4), 187–191.
Hawkley, L. C., Hughes, M. E., Waite, L. J., Masi, C. M., Thisted, R. A., & Cacioppo, J. T. (2008). From social structural factors to perceptions of relationship quality and loneliness: The Chicago Health, Aging, and Social Relations Study. Journals of Gerontology Series B-Psychological Sciences and Social Sciences, 63(6), 375–384.
Hvinden, B. (2010). The Nordic welfare model and the challenge of globalisation. In M. Böss (Ed.), The nation state in transformation: Economic globalisation, institutional mediation and political values (pp. 292–314). Århus: University Press.
Iecovich, E., Barasch, M., Mirsky, J., Kaufman, R., Avgar, A., & Kol-Fogelson, A. (2004). Social support networks and loneliness among elderly Jews in Russia and Ukraine. Journal of Marriage and Family, 66(2), 306–317.
Johnson, D., & Mullins, L. (1987). Growing old and lonely in different societies: Toward a comparative perspective. Journal of Cross-Cultural Gerontology, 2(3), 257.
Jylha, M., & Jokela, M. (1990). Individual experiences as cultural: A cross-cultural study on loneliness among the elderly. Ageing and Society, 10, 295–315.
Lasgaard, M. (2007). Reliability and validity of the Danish version of the UCLA Loneliness Scale. Personality and Individual Differences, 7, 1359–1366.
Lipsitz, L. A. (2005). The elderly people of post-soviet Ukraine: Medical, social, and economic challenges. Journal of the American Geriatrics Society, 53(12), 2216–2220.
Mirowsky, J., & Ross, C. E. (2007). Life course trajectories of perceived control and their relationship to education. American Journal of Sociology, 112(5), 1339–1382.
Nicolaisen, M., & Thorsen, K. (2014). Who are lonely? Loneliness in different age groups (18–81 years old), using two measures of loneliness. International Journal of Aging and Human Development, 78, 229–257.
OECD. (2012a). International migration outlook 2014. OECD Publishing.
OECD. (2012b). Education at a glance 2012: OECD indicators. OECD Publishing.
Petrov, I. C. (2007). The elderly in a period of transition: Health, personality, and social aspects of adaptation. Healthy Aging and Longevity, 1114, 300–309.
Pew Research. (2009). Two decades after the wall’s fall: End of communism cheered but now with more reservations. Washington, DC: Pew Research Center.
Pietilä, I., & Rytkönen, M. (2008). Coping with stress and by stress: Russian men and women talking about transition, stress and health. Social Science & Medicine, 66, 327–338.
Pinquart, M., & Sörensen, S. (2001). Influences on loneliness in older adults: A meta-analysis. Basic and Applied Social Psychology, 23(4), 245–266.
Ploubidis, G. B., & Grundy, E. (2009). Later-life mental health in Europe: A country-level comparison. Journals of Gerontology Series B-Psychological Sciences and Social Sciences, 64(5), 666–676.
Reher, D. S. (1998). Family ties in western Europe: Persistent contrasts. Population and Development Review, 24(2), 203–234.
Rokach, A. (2007). The effect of age and culture on the causes of loneliness. Social Behavior and Personality, 35(2), 169–186.
Rokach, A., Orzeck, T., Cripps, J., Lackovic-Grgin, K., & Penezic, Z. (2001). The effects of culture on the meaning of loneliness. Social Indicators Research, 53(1), 17–31.
Saltkjel, T., Dahl, E., & van der Wel, K. A. (2013). Health related social exclusion in Europe: A multilevel study of the role of welfare generosity. International Journal for Equity in Health, 12, 81–92.
Saraceno, C., & Keck, W. (2010). Can we identify intergenerational policy regimes in Europe? European Societies, 12(5), 675–696.
Sundstrom, G., Fransson, E., Malmberg, B., & Davey, A. (2009). Loneliness among older Europeans. European Journal of Ageing, 6(4), 267–275.
Tornstam, L. (2007). Stereotypes of old people persist. A Swedish, “Facts on aging quiz” in a 23-year comparative perspective. International Journal of Ageing and Later Life, 2(1), 33–59.
van Oorschot, W., & Arts, W. (2005). The social capital of European welfare states: The crowding out hypothesis revisited. Journal of European Social Policy, 15(1), 5–26.
van Tilburg, T., & De Leeuw, E. (1991). Stability of scale quality under various data collection procedures: a mode comparison of the "De Jong-Gierveld Loneliness Scale". International Journal of Public Opinion Research, 3, 69–85.
Viazzo, P. (2010). Family, kinship and welfare provision in Europe, past and present: Commonalities and divergences. Continuity and Change, 25(1), 137–159.
Victor, C., Bond, J., & Scambler, S. (2009). The social world of older people. Maidenhead: Open University Press.
Victor, C., Scambler, S., Bond, J., & Bowling, A. (2000). Being alone in later life: Loneliness, social isolation and living alone. Reviews in Clinical Gerontology, 10, 407–417.
Weiss, R. S. (1973). Loneliness: The experience of emotional and social isolation. Cambridge, MA: MIT Press.
Yang, K. M., & Victor, C. (2011). Age and loneliness in 25 European nations. Ageing and Society, 31, 1368–1388.
Acknowledgments
This research was supported by a grant from the Research Council of Norway (Grant No. 228664). The NorLAG and LOGG surveys are financed by the Research Council of Norway (Grant Nos. 149564 and 168373), Ministry of Health and Care Services, Ministry of Labour, Ministry of Children, Equality and Social Inclusion, Ministry of Local Government and Regional Development, NOVA and Statistics Norway. The LOGG and NorLAG datasets are part of the ACCESS Life Course infrastructure project funded by the National Financing Initiative for Research Infrastructure at the Research Council of Norway (Grant No. 195403) and NOVA.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hansen, T., Slagsvold, B. Late-Life Loneliness in 11 European Countries: Results from the Generations and Gender Survey. Soc Indic Res 129, 445–464 (2016). https://doi.org/10.1007/s11205-015-1111-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-015-1111-6