
Abstract
As one of the most destructive natural disasters, earthquakes affect the health of survivors. The devastating earthquakes that hit Sichuan, China have aroused the concern of domestic and international scholars. The health-related quality of life (HRQOL) of survivors also requires substantial research. Studies on impact factors, such as gender, age, monthly income, and education, have become controversial. The subjects in this study are the people of five hard-hit disaster counties in Sichuan Province, namely, Wenchuan, Qingchuan, Mianzhu, Lushan, and Dujiangyan. A preliminary survey was conducted in May and June 2013 in areas badly hit by the earthquake in Sichuan, China. A total of 2000 questionnaires were distributed, and 1672 of which were received, yielding a recovery rate of 83.6 %. To further complement and corroborate the conclusions, a follow-up survey was conducted in October and November 2013, where 1526 effective questionnaires were received. The analysis in this paper is mainly based on the first survey, and the collected data from the follow-up survey were used to perform a supplementary analysis. By analyzing data from five hard-hit areas in Sichuan and by establishing models, we drew the following conclusions: The results of analysis of variance and Tukey’s honestly significant difference tests revealed the following results. First, the results of two investigations indicate the HRQOL of earthquake survivors is relatively poor, especially in terms of general health (GH), mental health (MH), social functioning (SF), etc. However, results of the second survey indicate that the scores of all domains (except GH) have increased significantly, with the SF having the most significant increase. Second, the HRQOL scores of men are higher than those of women. Individuals with higher education or monthly income have higher HRQOL scores than those with lower education or income. Moreover, younger survivors have higher HRQOL scores than older survivors. Third, a positive correlation exists among the HRQOL domains of all survivors. Among all domains, the PF, RP, GH, MH, and VT of survivors have a very strong correlation. In addition, SF, BP, MH, and VT have a strong correlation. Other variables have a relatively weak correlation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
The lives and health of people affected by natural disasters are often vulnerable and disadvantaged. In recent years, severe natural disasters have occurred frequently worldwide. These disasters have significantly affected the health of survivors, which aroused the concern of many scholars. As the largest developing country in the world, China also suffered from the damaging impacts of natural disasters, especially earthquakes. Since the Wenchuan earthquake in 2008, several devastating earthquakes, such as the Yushu earthquake and Lushan earthquake, hit Mainland China and caused severe casualties. Sichuan Province, one of the western provinces with large population, has suffered from the most frequent and destructive earthquakes. The residents of Sichuan Province are facing earthquake threats. The health of the people in this province is the concern of domestic and international scholars. Thus, studying the health of survivors during reconstruction is indispensable. Figures 1, 2 show the affected houses in the rural communities of Guangyuan and Ya’an after the 2013 Lushan earthquake.Footnote 1

Affected houses in Guangyuan

Ya’an rural community
Since the devastating 2008 Sichuan earthquake, the health of survivors in the affected districts has been an important issue. Many studies determined whether or not the survivors have developed post-traumatic stress disorder (PTSD). Some scholars have studied the reactions of survivors with different demographics to PTSD (Wang et al. 2012; Dell’Osso et al. 2011; Goenjian et al. 2011; Jia et al. 2010). Age and gender are strongly related to the health of survivors. A three-year follow-up investigation on the survivors of the Chi–Chi earthquake has shown that the public health system has a significant effect on the initial period of PTSD. The impact of PTSD on the pressure toward survivors has significantly decreased (Su et al. 2010). Evidently, these studies have limitations. These studies did not determine the overall health of survivors because they only used PTSD as basis to assess the mental health of survivors. Moreover, only a few studies have examined the health of survivors based on health-related quality of life (HRQOL).
People have become more concerned about the overall physical and mental health since 1980. HRQOL refers to the health status of individuals affected by diseases, injuries, medical interventions, aging, and social environment. HRQOL also represents the subjective satisfaction linked to economic, cultural background, and individual values (Sprangers and Schwartz 1999; Burckhardt and Anderson 2003). HRQOL describes the functional status of individuals in terms of physical, psychological, and social aspects. HRQOL covers physical health and MH and can clearly determine the health status indexes of individuals (Cummins et al. 2004; Tan et al. 2013). As an important indicator of the quality of life of people in terms of physical health and mental health, HRQOL has also become an important means to evaluate and monitor the health status of people (Ashing-Giwa 2005). HRQOL can reduce the boundaries between various disciplines and can be widely applied to social, psychological, and medical services (Herdman et al. 1998; Desouky et al. 2013; Nesterko et al. 2013). HRQOL also has a significant effect on the health of people (Quinn et al. 2013; O’ Neil et al. 2013; Gothwal et al. 2013).
Tools such as the sickness impact profile (SIP), the Nottingham health profile (NHP), the EuroQol questionnaire (EQ-5D), the medical outcomes study short form 12 (SF-12), the medical outcome study short form 36 (SF-36), and the WHO quality of life–best available technique reference (WHOQOL-BREF) can be used to measure HRQOL. SIP can be applied to any health status evaluation of any diseases. NHP is used to measure the health status of large populations and is a self-reported scale composed of 45 items, six health domains, and seven living domains. Among the aforementioned tools, EQ-5D is the simplest for measuring the health status of people. EQ-5D is divided into five domains and a visual scale. SF-36 is one of the most commonly used scales worldwide. SF-36 includes 36 items and eight domains, namely, physical functioning (PF), role physical (RP), role emotional (RE), social functioning (SF), body pain (BP), general health (GH), vitality (VT), and mental health (MH). SF-12 is the simplified version of SF-36. (Guyatt et al. 1993) cleared the concept and measuring methods of HRQOL; their study served as the reference of using scales to measure HRQOL. WHOQOL-BREF consists of 26 items and six domains, namely, physical health, psychological heath, independence, social relationship, environment, and spirituality. These scales are important for evaluating the health status of individuals. Compared with clinical diagnoses, these scales can help better characterize the physical, psychological, and functional states of individuals. In this study, we employed SF-36 to measure HRQOL. SF-36 is a versatile short scale that consists of a physical component summary (PCS) and a mental component summary (MCS) based on eight small domains. More than 5,000 published studies worldwide have used SF-36, which has been proven to be a global tool for measuring HRQOL. SF-36 is suitable for HRQOL measurement because it can be applied under different conditions (Ware Jr and Gandek 1998; Ware Ware 2000).
Only a few studies have focused on the HRQOL of survivors. Previous studies have investigated the HRQOL of survivors from different angles (Zhang et al. 2009; Chen 2011; Wang et al. 2012; Ke et al. 2010). For example (Zhang et al. 2012) used SF-36 to measure the HRQOL of fracture survivors in an affected area while considering physiologic factors. Other studies focused on psychological health and ignored the overall health of survivors (Zhang et al. 2010; Kiliç et al. 2003; Zhang et al. 2011). A study conducted in Taiwan indicated that elders, divorced or widowed, and low-educated people have poor scores in psychiatric examinations (Chou et al. 2004). Thus, improving the HRQOL of survivors and finding the key factors affecting HRQOL have become urgent issues. However, only a few studies have measured the HRQOL of survivors via PCS and MCS domains. Accordingly, the present study aims to examine Chinese earthquake survivors in terms of both PCS and MCS.
In addition, our research used SF-36 to measure HRQOL because this tool has been deemed suitable to evaluate quality of life (Fuh et al. 2000). Many studies have shown that SF-36 is appropriate for analyzing the situation of Mainland China. The reliability and validity of SF-36 have also been proven. For example, a previous study employed SF-12 to measure the HRQOL of the Chinese population. SF-12, the simplified version of SF-36, is valid to assess the Chinese population (Lam et al. 2005). In addition, previous research evaluated the HRQOL of Chinese urban construction workers and found that the reliability and validity of SF-36 are suitable for studying this vulnerable group (Qu et al. 2009; Zhu et al. 2012). Another research compared the Chinese version of SF-36 with the original version and revealed that both versions have excellent validity. The difference in internal consistencies between the two versions is negligible (Yu et al. 2003). SF-36 was also used to explore whether or not the life model affects the HRQOL of rural residents by comparing the scores of eight domains of urban residents (Liu et al. 2010).
The present study used the Chinese version of SF-36 to investigate the HRQOL and health of survivors. This study promotes social concern for the survivors and improves their HRQOL.
To date, the HRQOL of earthquake survivors remains unclear. Previous studies showed that survivors suffer from serious health problems. Some of these survivors suffered physical and mental problems after losing their families and homes. The survivors also experienced terrible health problems. But after a long time of rest, has their health improved? These are what we want to learn. Thus, we propose the first hypothesis.
Hypothesis 1
The scores of all HRQOL domains of the survivors are low. But they are improving.
Sichuan earthquakes, including the Wenchuan earthquake, have destroyed the lives and homes of thousands of people. The Chinese culture may also contribute to the effects of earthquake. Thus, we propose the second hypothesis.
Hypothesis 2
The scores of the survivors for each HRQOL domain are affected by different genders, ages, educational levels, and monthly incomes.
In this study, we employed SF-36, which includes MCS and PCS, to measure the HRQOL of survivors. Many studies indicated that all eight SF-36 domains are related to one another (Gandhi et al. 2013; Touma et al. 2011). Thus, we propose the third hypothesis.
Hypothesis 3
Positive correlations exist among the eight HRQOL domains.
As one of the most destructive natural disasters, earthquakes affect the health of survivors. The health of survivors has been an important research issue. However, the factors affecting the HRQOL of survivors remain unknown. This study aims to recognize and promote the HRQOL of survivors. We divided the survivors into different ages, genders, monthly income, and educational level to explore the structural differences among various demographics. We also investigated the MCS and PCS of the survivors. The eight SF-36 domains, namely, PF, RP, BP, GH, VT, SF, RE, and MH, were included. We appeal that health services should be provided to increase the HRQOL of survivors.
2 Methods
2.1 Objects
In 2013, a preliminary survey and a follow-up survey were conducted in five hard-hit areas in Sichuan. The data analysis in this paper is mainly based on the first survey, and the collected data from the follow-up survey were used to perform a supplementary analysis. Two surveys have been conducted in Sichuan, China within half a year.The first survey was in May and June 2013, distributing 2000 questionnaires and received 1672, yielding a recovery rate of 83.6 %. To further complement and corroborate the conclusions, a follow-up survey was conducted in October and November 2013, where 1526 effective questionnaires were received.
Earthquake damages in Sichuan varied with location. Five cities (Aba, Guangyuan, Deyang, Ya’an, and Chengdu) were first selected randomly from 39 hard-hit areas, followed by five counties (Wenchuan, Qingchuan, Mianzhu, Lushan, and Dujiangyan) being selected from each city, using the same random sampling method. 400 survivors were randomly picked from each county using the quota sampling method. Note that vigorous and professional training were conducted to the survey workers. The questionnaires were distributed in community and relief centers. Questionnaires were completed by each respondent under guidance from the survey workers. In the first survey conducted half a year ago, the respondents were asked to leave their contact details such as telephone and family address. For the second survey conducted half a year later, the respondents were telephoned them to answer the questionnaires again. Should the phone call fail, the respondents were visited from their homes according to the family address.
2.2 Methods
2.2.1 Analysis of Variance (ANOVA) Analysis
ANOVA or F test, which was designed by R.A. Fisher, is a significance test regarding the difference of the mean values of two or more samples. The research data are fluctuating because of the influence of various factors. The causes of these fluctuations that affected the results of studies may be divided into two categories, namely, uncontrollable random factors and controllable factors.
We used ANOVA to check whether or not significant differences exist between the scores of all domains under different control variables. For values with significant differences, we used Tukey’s honestly significant difference (HSD) test to determine which groups are significant.
ANOVA and Tukey’s HSD are proven effective measurement tools. (Yoon et al. 2012) designed the questionnaire and used ANOVA and Tukey’s tests to analyze the efficacy of an herbal plant. The aged Maggi experimental product was found to be better than the fresh Maggi product. In addition, the minty STW5 is different from the herbal products (Lim et al. 2012) used ANOVA and Tukey’s tests to determine whether or not subclinical atherosclerosis in elderly is worse than in that in young people. Siegrist et al. (2010) explored the influence of three healthcare systems on work-related pressure. They used ANOVA and Tukey’s tests to analyze the differences among groups. Brock et al. (2010) studied the requirements of pathogen testing and equipment in the disaster. ANOVA and Tukey’s multiple comparison tests were used to compare the rating questionnaires. Lee et al. (2010) used ANOVA and Tukey’s multiple comparison tests to compare the different effects of three external fluorides on surface micro hardness, fluoride uptake, and fluorescence lesion area in enamel.
In the present study, we explored whether or not significant differences exist between the scores of each domain under different control variables. We used Tukey’s HSD multiple comparison test to compare the differences of scores under each control variable.
2.2.2 Reliability Evaluation
An ideal questionnaire should not only accurately reflect the properties of the object of study but also obtain all the required information with the smallest measurement error under certain conditions. Thus, testing the quality of the scales is necessary. Reliability analysis can test the consistency, stability, and reliability of questionnaires. If research unit properties and the measurement results are unchanged, then this measure is credible. Currently, several reliability assessment methods, including repeat test, staggered method, binary method, and internal consistency, can be used.
In the current study, we assessed the internal consistency of SF-36 using the statistical software of Stata. Cronbach’s alpha coefficient was used to represent the internal consistency of the scale. In general, an alpha coefficient that exceeds 0.7 indicates that the questionnaire is credible.
2.2.3 SEM-Based Model
The structural equation modeling-based model (SEM-based model) starts from the concept model, fits with the observation data and concept models, and tests the support degree of the observation data to the concept model. This model can test whether or not the fit of the concept model is reasonable. The SEM-based model can also explore the relationship between observations and potential variables within the model. We will use this model to evaluate and discuss all HRQOL domains of survivors.
3 Results
3.1 SF-36 Basic Statistics
Table 1 presents the SF-36 scale results from two surveys, each comprising eight domains. From the scores of eight domains, the HRQOL and health improvement the survivors after half a year can be determined.
The scores in all domains are lower than 50 for the first survey (Table 1). The scores of PF, BP, and RE are higher than those of GH, SF, and MH. The second survey shows that with the exception of domains with scores higher than 50, the mean values of all domains are not ideal. However, the scores are better compared that of first survey; for instance, the mean value of SF increased by 53.87 %.
ANOVA was used to further determine any significant differences between the survey results. All domains except GH have passed the significance test, and the scores have increased significantly, with the SF having the most significant increase.
3.2 ANOVA Analysis
Differences between the HRQOL of the survivors were determined based on gender, age range, educational attainment, and previous monthly income. The HRQOL of the survivors has been improved after half a year (i.e., the second survey). We chose the data collected from the first survey, which was closer to the disaster occurrence, to further explore the effect of different control variables on the HRQOL.
3.2.1 Gender-SF36
According to the data of each domain for different genders, we established eight ANOVA models to determine whether or not significant differences exist among the scores of all domains under different genders. The judging criteria for the single-factor ANOVA are based on the F value. In general, significant differences are considered to occur when the P value that corresponds to the F value is lower than 0.05. The results are shown in Table 2.
The results of single-factor ANOVA indicate that the F test of the scores for each domain under different genders is highly significant (P < 0.0001). Therefore, differences in the scores of each domain exist between males and females. As shown in Table 3 and Fig. 3, the differences in the scores of each domain between males and females are significant. The scores of women are obviously lower than those of men among the eight domains. According to the results of Tukey’s HSD test, the mean value of the eight domains of females is 20 points lower than those of males. All eight domains pass the significance test (P < 0.001). Figure 3 shows that the mean values of males for PF, RP, BP, VT, SF, RE, and MH are above 50. However, their mean score for GH is approximately 40. Among these domains, the mean values of males for PF, BP, VT, and RE are relatively high. The mean values of females for each domain are lower than 40. Moreover, the mean values for RP, GH, SF, and MH are approximately 20, which is relatively low.

Box diagrams of scores of different genders

Box diagrams of scores under different age ranges
3.2.2 Age-SF36
Considering that the age range of the correspondents of the survey was [18, 70], we divided the subjects into three groups according to the WHO age criteria (Table 4).
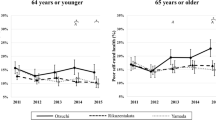
Single-factor ANOVA was then conducted to determine the HRQOL of the survivors according to the three age groups (Table 5). The results of ANOVA for the eight domains in different age ranges indicate that all the F test results of each domain under different age ranges are highly significant (P < 0.0001). These results suggest that significant differences exist among the scores of the eights domains under different genders. The differences between the scores can be observed in Table 6 and Fig. 4. The mean values of all domains of the survivors under Age 1 are higher than those under the two groups. No significant differences exist between Age 2 and Age 3. Significant differences exist between Age 1 and the other two groups (P < 0.001, Table 6). The mean value of Age 1 is also 30 points higher than those of Age 2 and Age 3.
The scores of each domain tend to decline as age increases. For example, the mean SF score of the first age range is above 60; whereas that of the last age range is lower than 40.
The scores of the three ages exhibit a “tiered” phenomenon. The first age range has the highest mean value of each domain, whereas the second and third age ranges have the lowest mean value of each domain. For example, the mean MH score of the first age range is 60, whereas that of the second and third age ranges is approximately 20.
3.2.3 Education-SF36
We divided the education of the respondents into five levels: illiterate, elementary, middle, high school, and college and above. We then determined whether or not differences in HRQOL exist among the survivors with different levels of education.
Table 7 shows that the F test scores of each domain under different educational levels are highly significant (P < 0.001). Therefore, differences exist in the scores of each domain under different educational levels. Furthermore, the box diagram shows that the differences in the scores of each domain are significant (Fig. 5).

Box diagrams of scores under different levels of education. The abscissas edu1, edu2, edu3, edu4, and edu5 in the figure indicate the educational levels illiterate, elementary, middle, high school, and college and above, respectively
As shown in Table 8, no significant differences exist between some groups. Significant differences in the mean scores of the domains other than PF, BP, and GH are noted in the Edu2–Edu1 group. No significant differences in the mean BP score of the Edu5–Edu4 group exist (Table 9).
-
1.
Tukey’s HSD test shows that not all levels of education have significant differences. However, the scores of each domain generally increase with the level of education. The box diagrams show similar results.
-
2.
The HRQOL of the survivors whose education is below high school (high school excluded) is relatively poor. As shown in Fig. 5, the HRQOL of the survivors whose educational level is illiterate, elementary or middle school differs significantly from that of the survivors whose education is high school and above.
3.2.4 Monthly Income-SF36
We divided the monthly income of respondents into six levels: below RMB 1000, RMB 1000–1500, RMB 1500–2000, RMB 2000–3000, RMB 3000–4000, and above RMB 4000. Afterward, we analyzed whether or not differences in HRQOL exist among the survivors with different levels of monthly income.
Table 10 shows that all the F test scores of each domain under different levels of monthly income are highly significant (P < 0.0001). Therefore, differences in the scores of each domain exist among the survivors with different levels of monthly income. Furthermore, the box diagram shows that the differences in the scores of each domain are significant (see Fig. 6).

Box diagrams of scores under different levels of monthly income. The abscissas inc1, inc2, inc3, inc4, inc5, and inc6 indicate the monthly income levels of below RMB 1000, RMB 1000–1500, RMB 1500–2000, RMB 2000–3000, RMB 3000–4000, and above RMB 4000, respectively
As shown in Table 10, no significant differences exist between some groups. The mean scores of the domains, except for RE, show significant differences in the Inc6–Inc5 group. In addition, no significant differences exist in the scores of the VT, RP, and SF domains in the Inc2–Inc1 group; RP, BP, and GH domains in the Inc5–Inc4 group; and BP and GH domains in the Inc6–Inc4 group.
-
1.
Tukey’s HSD test shows that not all levels of last monthly income show significant differences. However, the scores of each domain generally increase with the level of monthly income. The box diagrams show similar results.
-
2.
The HRQOL of the survivors whose monthly income is below RMB 2000 is relatively poor. As shown in Fig. 6, the scores of each domain under monthly income levels of below RMB 1000, RMB 1000–1500, and RMB 1500–2000 are below 50, whereas those of each domain under monthly income levels of RMB 2000–3000, RMB 3000–4000, and above RMB 4000 are above 50. Significant differences exist in the HRQOL of the survivors whose monthly income is approximately RMB 2000.
3.3 Correlation Test
For factor analysis, the original variables should exhibit a strong correlation. Thus, raw data must be correlated before the factors are analyzed. The factor analysis for the original variables is statistically significant only when most of the correlation coefficients in the matrix are above 0.3. If most of these coefficients are lower than 0.3, then the original variables are suitable for factor analysis. Correlation analysis was then conducted using the raw data from the questionnaires (Table 11).
3.4 Tests of the SF-36 Scale
3.4.1 Reliability Analysis of the SF-36 Scale
The reliability of analysis to the survey results was determined. The total Cronbach’s alpha coefficient of the SF-36 scale in the first and second surveys are 0.913 (Table 12) and 0.921 (Table 13). The reliability of scales is greater than 0.50. The questionnaire is reliable and has strong internal consistency when the coefficient is above 0.70. Subsequently, we calculated the total Cronbach’s alpha coefficient when a domain is removed. After removing any domain, the corresponding Cronbach’s alpha coefficient value generally declines, which makes the scale highly stable.
3.4.2 SEM-Based Model
In this section, the relationship among the eight SF-36 scale domains is studied using SEM (Fig. 7). We fit the concept model first and then evaluated the model-fitting results. Evaluating the CFA model is widely considered a comprehensive problem. Different fit indexes have different emphases. Thus, multiple indexes must be considered comprehensively to determine whether or not the model supports the observation data. We chose six model fit indexes, including Chi square (χ2), Chi square/degrees of freedom (\(\chi^{2} /df\)), comparative fit index (CFI), increasing fit index (IFI), and goodness-of-fit index (GFI).

SEM of SF-36 scale
The model fits better with the observations when the \(\chi^{2} /df\) is less than 3. This result suggests that the model is good. Sample size influences \(\chi^{2} /df\). Thus, certain other indexes were utilized, such as CFI, IFI, and root mean square error of approximation (RMSEA). The fit of the model is good when both CFI and IFI are over 0.9 and when RMSEA is between 0 and 0.05. The SEM result of the first survey conducted half a year ago shows that \(\chi^{2} /df = 1.41\), CFI = 0.987(> 0.9), and IFI = 0.987(> 0.9). Moreover, the estimated value of RMSEA is 0.016, which is within the precise fitting range. While in the model of the investigation conducted half a year later shows, \(\chi^{2} /df = 2.80,\) CFI = 0.914(> 0.9), and IFI = 0.914(> 0.9).Overall, the model fit are good.
In addition, the path coefficients of the eight domains are positive and pass the significance test. CR value is a Z statistic that consists of the ratio of the parameter estimates and their standard deviations. CR value can evaluate whether or not the estimated path coefficient is statistically significant. CR value corresponds to the P value. When the P value is less than 0.05, each path coefficient passes the significance test. Furthermore, the P value proves that all domains exhibit a certain degree of correlation. The domains are not completely independent and have common potential confounders.
The degree of correlation between each domain is not similar. Table 14, 15 show that the path coefficients of each domain are not similar. Greater path coefficient results in stronger degree of differences between the corresponding variables. For example, SF, BP, MH, and VT of survivors have a very strong correlation with each other.
4 Conclusion and Discussion
4.1 Conclusion
Sichuan Province, one of the central provinces with a large population in China, has suffered from destructive earthquakes. The Wenchuan and Lushan earthquakes have caused severe casualties and posed threats to the health of the survivors. Thus, the HRQOL of the survivors must be investigated.
The data analysis in this paper is mainly based on the first survey, and the collected data from the follow-up survey were used to perform a supplementary analysis. By analyzing data from five hard-hit areas in Sichuan and by establishing models, we drew the following conclusions:
-
1.
The HRQOL of earthquake survivors is relatively poor, especially in the GH, MH, SF, VT,. And so on. We used SF-36 to measure the HRQOL domains of the survivors. The scores of each domain are relatively low, indicating that the HRQOL of the survivors is low, especially in the GH, MH, and SF domains.SF of survivors has been improved greatly at second survey.
-
2.
ANOVA results show that all domains (except GH) have improved significantly, including the SF cores, wherein the mean value increased by 53.87 % compared with that of the first survey (half a year ago).
-
3.
There are several features of survivors’ health. Gender, education, monthly income, and age significantly affect the HRQOL of the survivors. In general, the HRQOL scores of men are higher than those of women. Higher education or monthly income results in higher HRQOL scores. Moreover, younger survivors tend to have higher HRQOL scores. We present a detailed analysis based on four aspects.
-
(a)
All domains of females have lower scores than those of males.
-
(b)
The HRQOL of young people is better than that of middle-aged and elder people. In addition, no significant differences in HRQOL are present between middle-aged and elder people.
-
(c)
In general, survivors with higher educational level have better HRQOL. Aside from the PF, BP, and GH domains, no significant differences exist in the HRQOL of the survivors with elementary and lower educational levels. Furthermore, no significant differences exist in the HRQOL of the survivors with high school and higher educational levels in the BP domain. Significant differences exist in the mean values of each domain under other different educational levels.
-
(d)
In general, survivors with higher monthly income have better HRQOL. No significant differences exist in the HRQOL of the survivors with monthly income levels above RMB 3000 in the RE domain. In addition, no significant differences exist in the HRQOL of the survivors with monthly income levels below RMB 1500 in the VT, RP, and SF domains; RMB 2000–4000 in the RP, BP, and GH domains; and RMB 2000–3000 and above 4000 in the BP and GH domains.
-
3.
The HRQOL domains of all survivors exhibit correlations.
-
(a)
The correlations are all positive. The domains are not completely independent and have common potential confounders.
-
(b)
The degree of correlation between each domain is not similar. The SF, BP, MH, and VT of the survivors have a very strong correlation. SF, BP, MH, and VT also have a strong correlation. Other variables have a relatively weak correlation.
-
(c)
The degree of influence varies between each domain. Here, the SF, BP, MH, and VT of the survivors strongly influence one another.
-
(a)
Based on the above analysis, several suggestions are presented.
First, the government should provide a different policy target to increase the HRQOL of the survivors. In particular, female, elder survivors with low educational and income levels require urgent social and policy support.
Second, the government should provide several aid policies, especially HRQOL-related policies, such as employment aid policy and social insurance policy. With regard to the employment aid policy, the government should ensure that one person in every family is employed and that every family has income. The government should also develop public projects for the reconstruction of affected areas that can employ jobless survivors, such as health and epidemic prevention, logistics, environmental sweeping, and police affairs assistance. Moreover, the government should encourage enterprises to hire the survivors. Regulation-insured subsidies should be given to ensure that survivors will not be affected in terms of income. With regard to the social insurance policy, the government should protect elder survivors. If the survivors have reached the statutory retirement age, they should be eligible to apply for retirement and pension. In addition, if the survivors meet the minimum living security requirements, they should be given a subsistence allowance. If the survivors meet temporary living assistance requirements, they should be given temporary living assistance.
Third, health knowledge should be disseminated. The government health department should set up regular lectures in hospitals, primary schools, and primary health units to propagate health knowledge. By doing such, survivors can be encouraged to change bad habits, which will thereby increase their health (Jorm 2000). The government should also create primary health units in resettlement sites so that public health status may be improved. In addition, the government should invite experts to propagate the importance of mental health. A database should also be established for female, elder individuals with low income and educational levels. Traced surveys to improve survivors’ HRQOL must be conducted.
Finally, the government should focus on the coordination and integration of policies. However, we should not increase their HRQOL using only one method. The process can be bidirectional. Survivors should be encouraged to participate in reconstruction work. The eight HRQOL domains are positively correlated with one another. SF, BP, MH, and VT have a strong mutual correlation. The spontaneous spirit will motivate the survivors to actively participate in the reconstruction, which can improve both MCS and PCS.
This study also has certain limitations. First, we selected only the most representative areas that suffered from destructive earthquakes. China is a country with diverse natural disasters, such as floods, landslides, and snowstorms. These disasters hit different areas every year. The health of survivors suffering from different types of natural disasters should also increase our concern. Second, this study focused on indicators of the HRQOL of earthquake survivors. In fact, many factors also affect the HRQOL of survivors. The objective environmental factor should not be ignored. Third, we attempted to improve the HRQOL of survivors and diversify the research perspective that focuses on influencing factors. Aside from the SF-36 scale, other tools that have been improved to have good reliability and validity are available. Future research may attempt to employ these tools to explore the HRQOL of survivors.
Notes
The two photos below were taken in Guangyuan and Ya’an, two of the sites where the questionnaires were distributed.
Abbreviations
- HRQOL:
-
Health-related quality of life
- SF-36:
-
Medical outcome study short form 36
- PCS:
-
Physical component summary
- MCS:
-
Mental component summary
- CFA:
-
Confirmatory factor analysis
- ANOVA:
-
Analysis of variance
- 1st Qu:
-
One fourth quartile
- 3rd Qu:
-
Three quarter quartile
- PF:
-
Physical functioning
- RP:
-
Role physical
- RE:
-
Role emotional
- SF:
-
Social functioning
- BP:
-
Body pain
- GH:
-
General health
- VT:
-
Vitality
- MH:
-
Mental health
References
Ashing-Giwa, K. T. (2005). The contextual model of HRQoL: A paradigm for expanding the HRQoL framework. Quality of Life Research, 14(2), 297–307.
Brock, T. K., Mecozzi, D. M., Sumner, S., & Kost, G. J. (2010). Evidence-based point-of-care tests and device designs for disaster preparedness. American journal of disaster medicine, 5(5), 285.
Burckhardt, C. S., & Anderson, K. L. (2003). The quality of life scale (QOLS): Reliability, validity, and utilization. Health and quality of life outcomes, 1(1), 60.
Chen, J. (2011). Internal migration and health: Re-examining the healthy migrant phenomenon in China. Social Science and Medicine, 72(8), 1294–1301.
Chou, F. C., Chou, P., Lin, C., Su, T. T. P., Ou-Yang, W. C., Chien, I. C., et al. (2004). The relationship between quality of life and psychiatric impairment for a Taiwanese community post-earthquake. Quality of Life Research, 13(6), 1089–1097.
Cummins, R. A., Lau, A. L., & Stokes, M. (2004). HRQOL and subjective well-being: Noncomplementary forms of outcome measurement. Expert Review of Pharmacoeconomics and Outcomes Research, 4(4), 413–420.
Dell’Osso, L., Carmassi, C., Massimetti, G., Daneluzzo, E., Di Tommaso, S., & Rossi, A. (2011). Full and partial PTSD among young adult survivors 10 months after the L’Aquila 2009 earthquake: Gender differences. Journal of Affective Disorders, 131(1), 79–83.
Desouky, T. F., Mora, P. A., & Howell, E. A. (2013). Measurement invariance of the SF-12 across European-American, Latina, and African-American postpartum women. Quality of Life Research, 1–10.
Fuh, J. L., Wang, S. J., Lu, S. R., Juang, K. D., & Lee, S. J. (2000). Psychometric evaluation of a Chinese (Taiwanese) version of the SF-36 health survey amongst middle-aged women from a rural community. Quality of Life Research, 9(6), 675–683.
Gandhi, P. K., Ried, L. D., Huang, I. C., Kimberlin, C. L., & Kauf, T. L. (2013). Assessment of response shift using two structural equation modeling techniques. Quality of Life Research, 1–11.
Goenjian, A. K., Roussos, A., Steinberg, A. M., Sotiropoulou, C., Walling, D., Kakaki, M., et al. (2011). Longitudinal study of PTSD, depression, and quality of life among adolescents after the Parnitha earthquake. Journal of Affective Disorders, 133(3), 509–515.
Gothwal, V. K., Srinivas, M., & Rao, G. N. (2013). A new look at the WHOQOL as health-related quality of life instrument among visually impaired people using Rasch analysis. Quality of Life Research, 1–13.
Guyatt, G. H., Feeny, D. H., & Patrick, D. L. (1993). Measuring health-related quality of life. Annals of Internal Medicine, 118(8), 622–629.
Herdman, M., Fox-Rushby, J., & Badia, X. (1998). A model of equivalence in the cultural adaptation of HRQOL instruments: The Universalist approach. Quality of Life Research, 7(4), 323–335.
Jia, Z., Tian, W., He, X., Liu, W., Jin, C., & Ding, H. (2010). Mental health and quality of life survey among child survivors of the 2008 Sichuan earthquake. Quality of Life Research, 19(9), 1381–1391.
Jorm, A. F. (2000). Mental health literacy public knowledge and beliefs about mental disorders. The British Journal of Psychiatry, 177(5), 396–401.
Ke, X., Liu, C., & Li, N. (2010). Social support and quality of life: A cross-sectional study on survivors eight months after the 2008 Wenchuan earthquake. BMC Public Health, 10(1), 573.
Kiliç, E. Z., Özgüven, H. D., & Sayil, I. (2003). The psychological effects of parental mental health on children experiencing disaster: The experience of Bolu earthquake in Turkey. Family Process, 42(4), 485–495.
Lam, C. L., Eileen, Y. Y., & Gandek, B. (2005). Is the standard SF-12 health survey valid and equivalent for a Chinese population? Quality of Life Research, 14(2), 539–547.
Lee, Y. E., Baek, H. J., Choi, Y. H., Jeong, S. H., Park, Y. D., & Song, K. B. (2010). Comparison of remineralization effect of three topical fluoride regimens on enamel initial carious lesions. Journal of Dentistry, 38(2), 166–171.
Lim, S., Choi, H. J., Shin, H., Khang, A. R., Kang, S. M., Yoon, J. W., et al. (2012). Subclinical atherosclerosis in a community-based elderly cohort: The Korean longitudinal study on health and aging. International journal of cardiology, 155(1), 126–133.
Liu, C., Li, N., Ren, X., & Liu, D. (2010). Is traditional rural lifestyle a barrier for quality of life assessment? A case study using the Short Form 36 in a rural Chinese population. Quality of Life Research, 19(1), 31–36.
Nesterko, Y., Braehler, E., Grande, G., & Glaesmer, H. (2013). Life satisfaction and health-related quality of life in immigrants and native-born Germans: The role of immigration-related factors. Quality of Life Research, 1–9.
O’ Neil, A., Stevenson, C. E., Williams, E. D., Mortimer, D., Oldenburg, B., & Sanderson, K. (2013). The health-related quality of life burden of co-morbid cardiovascular disease and major depressive disorder in Australia: Findings from a population-based, cross-sectional study. Quality of life research, 22(1), 37–44.
Qu, B., Guo, HQ., Liu, J., Zhang, Y., & Sun, G,. (2009). Reliability and validity testing of the SF-36 questionnaire for the evaluation of the quality of life of Chinese Urban construction workers. Journal of International Medical Research, 37(4), 1184–1190.
Quinn, G. P., Huang, I. C., Murphy, D., Zidonik-Eddelton, K., & Krull, K. R. (2013). Missing content from health-related quality of life instruments: Interviews with young adult survivors of childhood cancer. Quality of Life Research, 22(1), 111–118.
Siegrist, J., Shackelton, R., Link, C., Marceau, L., von dem Knesebeck, O., & McKinlay, J. (2010). Work stress of primary care physicians in the US, UK and German health care systems. Social Science and Medicine, 71(2), 298–304.
Sprangers, M. A., & Schwartz, C. E. (1999). Integrating response shift into health-related quality of life research: a theoretical model. Social Science and Medicine, 48(11), 1507–1515.
Su, C. Y., Tsai, K. Y., Chou, F. H. C., Ho, W. W., Liu, R., & Lin, W. K. (2010). A three-year follow-up study of the psychosocial predictors of delayed and unresolved post-traumatic stress disorder in Taiwan Chi–Chi earthquake survivors. Psychiatry and Clinical Neurosciences, 64(3), 239–248.
Tan, M. L., Wee, H. L., Lee, J., Ma, S., Heng, D., Tai, E. S., et al. (2013) Association of anthropometric measures with SF-36v2 PCS and MCS in a multi-ethnic Asian population. Quality of Life Research, 1–10.
Touma, Z., Gladman, D. D., Ibañez, D., & Urowitz, M. B. (2011). Is there an advantage over SF-36 with a quality of life measure that is specific to systemic lupus erythematosus? The Journal of rheumatology, 38(9), 1898–1905.
Wang, L., Cao, C., Wang, R., Zhang, J., & Li, Z. (2012). The dimensionality of PTSD symptoms and their relationship to health-related quality of life in Chinese earthquake survivors. Journal of Anxiety Disorders, 26(7), 711–718.
Ware, J. E, Jr. (2000). SF-36 health survey update. Spine, 25(24), 3130–3139.
Ware Jr, J. E., & Gandek, B. (1998) Overview of the SF-36 health survey and the international quality of life assessment (IQOLA) project. Journal of clinical epidemiology, 51(11), 903–912.
Yoon, S. L., Grundmann, O., Keane, D., Urbano, T., & Moshiree, B. (2012). Clinical evaluation of liquid placebos for an herbal supplement, STW5, in healthy volunteers. Complementary Therapies in Medicine, 20(5), 267–274.
Yu, J., Coons, S. J., Draugalis, J. R., Ren, X. S., & Hays, R. D. (2003). Equivalence of Chinese and US-english versions of the SF-36 health survey. Quality of Life Research, 12(4), 449–457.
Zhang, J., Li, X., Fang, X., & Xiong, Q. (2009). Discrimination experience and quality of life among rural-to-urban migrants in China: The mediation effect of expectation–reality discrepancy. Quality of Life Research, 18(3), 291–300.
Zhang, Y., Kong, F., Wang, L., Chen, H., Gao, X., Tan, X., et al. (2010). Mental health and coping styles of children and adolescent survivors one year after the 2008 Chinese earthquake. Children and Youth Services Review, 32(10), 1403–1409.
Zhang, Z., Shi, Z., Wang, L., & Liu, M. (2011). One year later: Mental health problems among survivors in hard-hit areas of the Wenchuan earthquake. Public health, 125(5), 293–300.
Zhang, X., Hu, X. R., Reinhardt, J. D., Zhu, H. J., Gosney, J. E., Liu, S. G., et al. (2012). Functional outcomes and health-related quality of life in fracture victims 27 months after the Sichuan earthquake. Journal of Rehabilitation Medicine, 44(3), 206–209.
Zhu, C. Y., Wang, J. J., Fu, X. H., Zhou, Z. H., Zhao, J., & Wang, C. X. (2012). Correlates of quality of life in China rural–urban female migrate workers. Quality of Life Research, 21(3), 495–503.
Acknowledgments
This paper is supported by the General Program of National Natural Science Foundation of China (71173099) and the Program for New Century Excellent Talents in University (NCET-11-0228). The authors would also like to thank Peiyi Lu (School of Communication and Design of Sun Yat-sen University) for her contributions to this study and Shu Zhang (School of Humanities and Social Sciences of Nanjing University of Science & Technology) for her contributions to the survey.
Conflict of interests
The authors declare that they have no conflict interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liang, Y., Chu, P. & Wang, X. Health-Related Quality of Life of Chinese Earthquake Survivors: A Case Study of Five Hard-Hit Disaster Counties in Sichuan. Soc Indic Res 119, 943–966 (2014). https://doi.org/10.1007/s11205-013-0525-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-013-0525-2