
Abstract
This study investigated cosmetic surgery attitudes within the framework of objectification theory. One hundred predominantly White, British undergraduate women completed self-report measures of impression management, global self-esteem, interpersonal sexual objectification, self-surveillance, body shame, and three components of cosmetic surgery attitudes. As expected, each of the objectification theory variables predicted greater consideration of having cosmetic surgery in the future. Also, as expected, sexual objectification and body shame uniquely predicted social motives for cosmetic surgery, whereas self-surveillance uniquely predicted intrapersonal motives for cosmetic surgery. These findings suggest that women’s acceptance of cosmetic surgery as a way to manipulate physical appearance can be partially explained by the degree to which they view themselves through the lenses of sexual and self-objectification.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The central purpose of the present research was to examine women’s attitudes toward cosmetic surgery through the lens of objectification theory (Fredrickson and Roberts 1997). Extending prior research on cosmetic surgery attitudes (Brown et al. 2007; Henderson-King and Henderson-King 2005; Sarwer et al. 2005; Swami et al. 2008), the present study investigates objectification theory variables (i.e., sexual objectification, self-surveillance, body shame) as a specific set of interpersonal and intrapersonal factors that may be associated with women’s endorsement of cosmetic surgery as an acceptable means of changing their physical appearance. Specifically, this cross-sectional investigation examines the relationship between objectification theory variables and cosmetic surgery attitudes among a sample of women living in the U.K., a cultural context within which women consistently report high levels of appearance concerns, sexual and self-objectification, and interest in cosmetic surgery (Calogero 2009; Calogero et al. 2010; Calogero and Thompson 2009a; Dittmar et al. 2000; Grogan 2008; McLaren et al. 2004; Puwar 2004; Swami et al. 2009a). This research provides a new test and application of objectification theory to the understanding of women’s lived experiences in westernized societies.
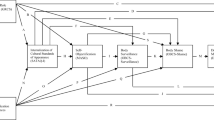
Feminist scholars have discussed how the construction of women’s bodies within particular social and cultural contexts determines the way that women’s bodies will be viewed, evaluated, and treated (Bartky 1990; Berger 1972; de Beauvoir 1952; Martin 1987). Objectification theory, proposed by Fredrickson and Roberts (1997), considers the pervasive sexual objectification of women in westernized societies as a macro-level context that produces a chain of negative micro-level consequences known to occur at a disproportionately higher rate among women. Sexual objectification occurs whenever a woman is reduced to and/or treated as a body or collection of body parts available for sexual use (Bartky 1990). According to objectification theory, sexual objectification plays out most obviously in two arenas: actual interpersonal and social encounters (e.g., cat calls, checking out or gazing at women’s bodies, sexual comments, harassment) and exposure to visual media that “spotlights” women’s bodies and body parts. From this perspective, girls and women come to place excessive emphasis on physical appearance as a result of these sexual objectification practices, ultimately adopting an external observational standpoint on their bodies such that “they treat themselves as objects to be looked at and evaluated” (p. 177, emphasis in original). Adopting this particular vantage point on the self, referred to as self-objectification, requires women to chronically ‘police’ or self-monitor their bodies in anticipation of being evaluated based on their appearance. Typically referred to as self-surveillance (McKinley and Hyde 1996; Tiggemann and Slater 2001), this engagement in chronic body monitoring is a common behavioural manifestation of self-objectification. Given the myriad social and economic rewards women earn for their physical attractiveness (Dellinger and Williams 1997; Eagly et al. 1991), and in an effort to cope with incessant external pressures to meet beauty ideals (Calogero et al. 2007; Thompson et al. 1999), many women experience objectified relationships with their own bodies in the form of self-objectification and self-surveillance.
The intended focus of objectification theory was to explicate the consequences of sexual and self-objectification for women’s lived experiences. Empirical studies have demonstrated that both interpersonal forms (Hill and Fischer 2008; Kozee and Tylka 2006; Kozee et al. 2007; Moradi et al. 2005) and media forms (Harper and Tiggemann 2008; Morry and Staska 2001) of sexual objectification contribute to self-objectification. Moreover, there is strong evidence from studies of women across North America, Australia, and the U.K. indicating that self-objectification, and the concomitant self-surveillance, exact significant costs on women’s subjective well-being (Breines et al. 2008; Fairchild and Rudman 2008) and cognitive performance (Fredrickson et al. 1998; Quinn et al. 2006b), with a greater prevalence of self-harming behavior (Harrell et al. 2006; Muehlenkamp et al. 2005) and a disproportionately higher rate of mental health risks, including depression (Grabe et al. 2007; Tiggemann and Kuring 2004), disordered eating (Calogero et al. 2005; Tylka and Hill 2004), and sexual dysfunction (Calogero and Thompson 2009b; Steer and Tiggemann 2008). In particular, researchers have identified body shame—the degree to which women feel ashamed of their bodies when they perceive them as falling short of feminine beauty ideals (McKinley and Hyde 1996)—as a key negative emotional consequence of self-objectification (Fredrickson and Roberts 1997; Moradi and Huang 2008). Body shame consistently mediates the effects of self-objectification on well-being and mental health (Noll and Fredrickson 1998; Quinn et al. 2006a; Tiggemann and Slater 2001), and thus is a critical variable in the objectification theory framework.
In the present research, we submit that positive attitudes toward cosmetic surgery among women reflect another negative consequence stemming from the socio-cultural conditions that perpetuate the objectification of women’s bodies. Indeed, the tremendous increase in elective cosmetic procedures (surgical and minimally invasive) over the past decade or more is due primarily to the disproportionately higher number of female patients who sought these treatments. Between 1992 and 2008, total cosmetic procedures performed in the U.S. increased by 882%, with over $10 billion spent on these procedures in 2008 (American Society of Plastic Surgeons [ASPS] 2009). This extreme growth in cosmetic procedures is not limited to the U.S.: Between 2003 and 2008, the number of surgical procedures performed in the U.K. more than tripled (British Association of Aesthetic and Plastic Surgeons [BAAPS] 2009). In both of these westernized societies, 91% of these procedures are performed routinely on women, whereas 9% are performed on men (ASPS 2009). In addition to the significant depletion of women’s economic resources (Hesse-Biber et al. 2006; Tiggemann and Rothblum 1997), this high percentage of women undergoing cosmetic surgery is particularly troubling because of the numerous deleterious consequences associated with these procedures, which are well-known among cosmetic surgeons but virtually unknown among the general population, such as chronic pain, deadly infections, gangrene, nerve damage, loss of sensation, mutilated body parts, amputation, reoperation, cancer detection difficulty, suicide, and death (Haiken 1997; Jeffreys 2005; McLaughlin et al. 2004; Wolf 1991; Zones 2000).
Researchers have linked a variety of interpersonal and intrapersonal variables to people’s attitudes toward cosmetic surgery (Sarwer et al. 1998, 2003b; Swami and Furnham 2008), such as negative body image (Brown et al. 2007; Markey and Markey 2009), appearance-based self-esteem (Delinsky 2005), attachment anxiety (Davis and Vernon 2002), Big-Five personality traits (Swami et al. 2009a), previous personal or vicarious experiences with cosmetic surgery (Swami et al. 2008), intense-personal celebrity worship (Swami et al. 2009b), materialism and parental attitudes (Henderson-King and Brooks 2009), appearance-related teasing (Markey and Markey 2009; Sarwer et al. 2003a, b), internalized media appearance ideals (Sarwer et al. 2005; Sperry et al. 2009), and appearance-based rejection sensitivity (Calogero et al. 2010; Park et al. 2009, 2010).
What sets the present research apart from this impressive body of work is our reliance on a systematic theoretical framework to explain why women undergo cosmetic surgery at a disproportionately higher rate than men. Whereas many of the aforementioned intrapsychic and interpersonal factors predicting cosmetic surgery attitudes could be similarly experienced by both women and men, it is well-documented that experiences of interpersonal sexual objectification (hereafter referred to as sexual objectification), self-surveillance (the behavioural manifestation of self-objectification), and body shame are part of many women’s, but fewer men’s, day-to-day lives (Bartky 1990; Davis 1990; Fredrickson and Roberts 1997; Puwar 2004; Swim et al. 2001). Being routinely viewed and treated as an object for the pleasure of others, coming to view oneself as an object for this use, and feeling ashamed of the body when not meeting stringent appearance standards, may bring about a sort of psychic distancing between the self and the body that encourages women to support even further objectification of their bodies via elective surgical procedures.
We focus on three specific components of cosmetic surgery attitudes in the present study. First, researchers have theorized two broad motives that underpin people’s support for cosmetic surgery: intrapersonal motives and social motives (Cash and Fleming 2002; Henderson-King and Henderson-King 2005). Intrapersonal motives emphasize the use of cosmetic surgery to manage one’s self-image, alleviate feelings of inadequacy, and to feel better about oneself (Davis 1995; Didie and Sarwer 2003). From this perspective, it is acceptable to undergo cosmetic surgery to modify one’s physical appearance if the purpose is self-motivated. Given that self-surveillance represents an internally-driven view of the self as a sexual object (Fredrickson and Roberts 1997; McKinley and Hyde 1996), we expected that higher self-surveillance would be associated with intrapersonal motives, reflecting the overvaluation of physical appearance to one’s self-image. Social motives emphasize the use of cosmetic surgery to garner favourable evaluations from others (Davis 1995; Henderson-King and Henderson-King 2005), based on the notion that enhancing one’s physical attractiveness to others brings social rewards (Eagly et al. 1991; Engeln-Maddox 2006; Evans 2003). From this perspective, it is acceptable to undergo cosmetic surgery to modify physical appearance if the purpose is to gain social currency. Given that sexual objectification and body shame are more closely linked to anticipated or actual social evaluations (Fredrickson and Roberts 1997; Tangney et al. 1996), we expected that more experiences of sexual objectification and higher body shame would be associated with social motives, reflecting the overvaluation of external observer’s perspectives on one’s physical appearance. In addition to these motives, we examined the degree to which people would consider undergoing cosmetic surgery in the future. Given that each of the three objectification theory variables call attention to the evaluation and appearance of women’s bodies, we expected that all three variables would be associated with greater consideration of cosmetic surgery.
We also expected that these relationships would remain significant after controlling for global self-esteem and impression management. Global self-esteem, defined as a personal judgment of self-worth, is a well-known indicator of overall well-being (Harter 1993) and linked to women’s experiences of objectification and cosmetic surgery. Specifically, self-esteem has been negatively associated with experiences of sexual objectification (American Psychological Association Task Force on the Sexualization of Girls 2007; Tylka and Subich 2004), self-objectification and self-surveillance (Aubrey 2006; Mercurio and Landry 2008; Tolman et al. 2006), and body shame (Aubrey 2006; Lowery et al. 2005; Mercurio and Landry 2008). In other research, however, women with high self-esteem who also strongly based their self-worth on their appearance reported greater well-being when they self-objectified compared to other women, in part because they felt less unattractive when they self-objectified (Breines et al. 2008). In addition, lower trait (Swami et al. 2009) and state (Henderson-King and Henderson-King 2005) self-esteem have been associated with more positive attitudes toward cosmetic surgery. Impression management (Leary and Kowalski 1990; Paulhus 1991), or the tendency to engage in socially desirable responding to control how one appears to others, also may be relevant to women’s experiences of objectification and cosmetic surgery. For example, individuals with a stronger tendency to control how they appear to others may be more sensitive to experiences of objectification and/or hold more positive attitudes toward cosmetic surgery if they believe these procedures would garner more favourable evaluations from others. In sum, because both global self-esteem and impression management are broad motivational variables potentially implicated in women’s experiences of objectification and cosmetic surgery, we included them as covariates in our analyses.
Our specific hypotheses are as follows:
-
H1:
Sexual objectification, self-surveillance, and body shame should positively correlate with intrapersonal motives, social motives, and consideration of cosmetic surgery.
-
H2:
Self-surveillance, but not sexual objectification or body shame, should positively predict intrapersonal motives for cosmetic surgery, and this relationship should remain significant after controlling for impression management and global self-esteem.
-
H3:
Sexual objectification and body shame, but not self-surveillance, should positively predict social motives for cosmetic surgery, and these relationships should remain significant after controlling for impression management and global self-esteem.
-
H4:
Sexual objectification, self-surveillance, and body shame should positively predict consideration of cosmetic surgery in the future, and these relationships should remain significant after controlling for impression management and global self-esteem.
Method
Participants and Procedure
A total of 100 college women attending a southeastern British university received psychology course credit for their participation. The mean age was 23.37 years (SD = 6.35), ranging from 18 to 49, with 86% of the women below the age of 30. The ethnic composition of the sample was 79% White, 9% Black African, 7% Asian, and 5% Other/Mixed Race. Participants were predominantly British (78%) and there was little variability in the reported sexual orientation of participants: 91% heterosexual, 6% bisexual, 1% homosexual, and 4% unspecified. A female experimenter announced the study at the end of a psychology lecture. After reading a brief description of the research, consenting participants completed the self-report measures described below in counterbalanced order, and provided demographic information (i.e., age, ethnicity, sexual orientation) before returning the packet of measures in a sealable envelope. The experimenter provided a full debriefing immediately following completion of the study.
Measure
Impression Management
The Impression Management (IM) subscale of the Balanced Inventory of Desirable Responding (Paulhus 1991) was used to measure the tendency to control how one appears to others, with a focus on presenting oneself in a socially desirable way. Participants rated 20 items on a scale from 1 (not true) to 7 (very true), such as “I have done things that I don’t tell other people about.” In the present study, the items were summed to create scale scores (α = .75), using a continuous scoring method (e.g., Pauls and Crost 2004). Scores ranged from 20 to 140, with higher scores indicating a greater tendency to engage in impression management. Previous research on the IM subscale has shown stable 5-week test-retest reliability and internal reliability, with alphas ranging from .75 to .86 (Paulhus 1991), and good convergent and discriminant validity (Lanyon and Carle 2007; Paulhus 1991).
Global Self-esteem
The Rosenberg Self-Esteem Scale (RSE; Rosenberg 1965) was used to measure trait-based global self-esteem. Participants rated items, such as ‘On the whole, I am satisfied with myself,’ on a scale from 1 (strongly disagree) to 6 (strongly agree), with higher scores indicating higher global self-esteem. In the present study, items were averaged to create scale scores (10 items, α = .85). Previous research has shown that the RSE has high internal reliability, with alphas ranging from .72 to .88, and good convergent and discriminant validity (Blascovich and Tomaka 1991; Wylie 1989).
Interpersonal Sexual Objectification
The Interpersonal Sexual Objectification Scale (ISOS; Kozee et al. 2007) was used to measure the extent to which women have experienced interpersonal forms of sexual objectification (i.e., body evaluation and unwanted explicit sexual advances) throughout their lifetime. Participants rated 15 items on a scale from 1 (never) to 5 (almost always), such as “How often have you noticed someone staring at your breasts when you are talking to them?” In the present study, items were averaged to create scale scores (α = .94). Scores ranged from 1 to 5, with higher scores indicating more frequent experiences of interpersonal sexual objectification. Previous research on the ISOS has shown stable 3-week test-retest reliability and internal reliability, with alphas ranging from .91 to .95, and good convergent, discriminant, and incremental validity (Kozee et al. 2007).
Self-surveillance
The Surveillance subscale of the Objectified Body Consciousness Scale (McKinley and Hyde 1996) was used to measure the degree to which individuals habitually monitor their bodies from an external observational standpoint, thus focusing more on how their bodies look than on how their bodies feel. Participants were asked to rate 8 items from 1 (strongly disagree) to 7 (strongly agree), such as “During the day, I think about how I look many times.” In the present study, items were averaged to create scale scores. Scores ranged from 1 to 7, with higher scores indicating more frequent monitoring and thinking about how one looks (α = .83). Previous research on this subscale has demonstrated stable 2-week test-retest reliability and moderate to high internal reliability, with alphas ranging from .76 to .89), and good convergent and discriminant validity (McKinley and Hyde 1996).
Body Shame
The Body Shame subscale of the Objectified Body Consciousness Scale (McKinley and Hyde 1996) was used to measure the degree to which individuals feel shame about their bodies when they perceive themselves as falling short of meeting cultural appearance standards. Participants rated 8 items from 1 (strongly disagree) to 7 (strongly agree), such as “When I’m not the size I think I should be, I feel ashamed.” In the present study, items were averaged to create scale scores (α = .89). Scores ranged from 1 to 7, with higher scores indicating more frequent monitoring and thinking about how one looks. Previous research on this subscale has demonstrated stable 2-week test-retest reliability and moderate to high internal reliability, with alphas ranging from .70 to .75, and good convergent and discriminant validity (McKinley and Hyde 1996).
Cosmetic Surgery Attitudes
The Acceptance of Cosmetic Surgery Scale (ACSS; Henderson-King and Henderson-King 2005) was used to measure the degree to which people hold favourable attitudes toward using cosmetic surgical procedures as a means for changing one’s physical appearance. It consists of three subscales: The Intrapersonal subscale includes five items that represent the endorsement of self-oriented reasons for deciding to have cosmetic surgery, such as “Cosmetic surgery can be a big benefit to people’s self-image.” The Social subscale includes five items that represent the endorsement of social motivations for deciding to have cosmetic surgery, such as “I would seriously consider having cosmetic surgery if my partner thought it was a good idea.” The Consider subscale includes five items that represent the likelihood of deciding to have cosmetic surgery, such as “In the future, I could end up having some kind of cosmetic surgery.” Participants rated each of the items from 1 (strongly disagree) to 7 (strongly agree). In the present study, items were averaged to create scale scores (α = .89, α = .87, α = .92, respectively). Scores ranged from 1 to 7, with higher scores indicating more positive attitudes toward cosmetic surgery.
Previous research has shown that each subscale of the ACSS has stable 3-week test-retest reliability, convergent and discriminant validity, and high internal consistency, with alphas ranging from .84 to .92 (Henderson-King and Henderson-King 2005). Furthermore, several studies have examined the subscales as distinct constructs when examining attitudes toward cosmetic surgery (e.g., Henderson-King and Henderson-King 2005; Swami et al. 2008).
Results
We handled the few missing data points by substituting participants’ mean scale scores for the missing value, and then examined the normality of the data. The skewness (−.53 to +.50) and kurtosis (−.65 to +.56) values for the scale scores indicated normally distributed observations that fell within the acceptable range for testing hierarchical regression models (skewness <3 and kurtosis <10; Kline 2005). In addition, we computed Shapiro-Wilk tests (W) to confirm that the scale scores represented normal distributions in this small sample (Shapiro et al. 1968). A significant W-test statistic indicates a non-normal distribution. The W-statistics for the scale scores were not significant, indicating that the sample of observations came from normally distributed populations of observations (ps = .12 to .50).
Means, standard deviations, and correlations are presented in Table 1. In support of our first hypothesis, cosmetic surgery attitudes were positively correlated with each of the predictor variables, such that more frequent experiences of sexual objectification, greater self-surveillance, and higher body shame were each associated with greater acceptance of intrapersonal and social motives for cosmetic surgery and greater consideration of cosmetic surgery. Next, hierarchical regression analyses tested the role of the objectification theory variables in women’s attitudes toward cosmetic surgery. This approach is appropriate considering the sizeable amount of shared variance observed among objectification variables in prior research (Calogero 2010; Moradi and Huang 2008). As order of entry in hierarchical regression is critical, the predictor variables were entered based on their temporal position derived from objectification theory (Fredrickson and Roberts 1997), such that shared variance would not contribute to any increment in R 2 when subsequent predictors were entered into the model. Specifically, impression management and global self-esteem were entered first to control for these effects at each step. Then, sexual objectification was entered in the second step, self-surveillance in the third step, and body shame in the final step.
We first examined the Tolerance and VIF values to determine the degree of multicollinearity among the predictors. Both of these values were very close to 1 for all predictors (Tolerance = .90 to .99; VIF = 1.01 to 1.11), indicating that multicollinearity was not a problem in these analyses. The results of the hierarchical regression analyses revealed support for the remaining three hypotheses (see Table 2). That is, after controlling for impression management, global self-esteem, and shared variance among the predictors, unique associations were found between the set of objectification theory variables and each of the cosmetic surgery attitudes. As expected (H2), only self-surveillance significantly predicted intrapersonal motives, accounting for the most unique variance of the objectification theory variables: sexual objectification (sr 2 = .03), self-surveillance (sr 2 = .11), and body shame (sr 2 = .03). Also, as expected (H3), only sexual objectification and body shame significantly predicted social motives, accounting for more unique variance than self-surveillance: sexual objectification (sr 2 = .06), self-surveillance (sr 2 = .01), and body shame (sr 2 = .05). Finally, as predicted (H4), all of the objectification theory variables significantly and uniquely predicted the extent to which women would consider having cosmetic surgery in the future: sexual objectification (sr 2 = .06), self-surveillance (sr 2 = .05), and body shame (sr 2 = .08).
Discussion
Experiences of sexual and self-objectification have been associated with various health risks and self-harming behaviors among women (Kozee et al. 2007; Moradi and Huang 2008; Wolf 1991). Drawing from and extending objectification theory (Fredrickson and Roberts 1997), we investigated the possibility that women’s experiences of sexual objectification, self-surveillance, and body shame would predict more positive attitudes toward cosmetic surgery as a way of manipulating how their bodies look. The results of this cross-sectional, correlational study provide preliminary evidence that this set of objectification theory variables predicts the degree to which women accept cosmetic surgery as a means of body modification and appearance control.
The significant associations observed between specific objectification variables and specific motives for cosmetic surgery also shed light on the different psychological processes that may inform women’s attitudes toward cosmetic surgery. For example, prior research has shown that intrapersonal reasons for cosmetic surgery are related to body shame, but not self-surveillance (Henderson-King and Henderson-King 2005). However, these findings were based on zero-order correlations that did not control for competing influences, whereas the present study found that self-surveillance was a unique predictor of intrapersonal reasons even after accounting for more general concerns related to self-presentation and self-esteem, sexual objectification experiences, and body shame. The items that comprise the intrapersonal reasons subscale focus on the use of cosmetic procedures to enhance one’s self-image and to feel better about oneself overall. Women who engage in more habitual body monitoring are more self-focused, and therefore would be more likely to endorse strategies that could potentially improve how they view their appearance.
The present study also demonstrated that more frequent experiences of sexual objectification and body shame were unique predictors of social reasons for cosmetic surgery, whereas self-surveillance was not. The items that comprise the social reasons subscale focus on the use of cosmetic procedures to enhance one’s physical attractiveness in order to reap social rewards. Given that sexual objectification and body shame are more closely tied to the experience of being socially evaluated by others based on one’s appearance, women who have experienced more sexual objectification and body shame would be more likely to endorse strategies that could potentially improve how attractive they appears to others. Not surprisingly, each of the objectification theory variables positively predicted the degree to which women would consider having cosmetic surgery in the future.
Because causal relationships cannot be established from correlational data, confirmation of these associations with experimental tests would strengthen confidence in the application of objectification theory to understanding women’s cosmetic surgery attitudes. In addition, we only tested women’s attitudes toward cosmetic surgery and not actual cosmetic surgery behavior. The degree to which objectification processes and positive attitudes toward cosmetic surgery predict whether women actually undergo cosmetic surgery requires further investigation. Moreover, whether or not cosmetic surgery changes how women experience sexual and self-objectification has not been studied. For example, a woman who undergoes a breast augmentation procedure would have larger breasts and should expect to be more (not less) sexually objectified, but would this woman experience more or less self-surveillance and body shame post-surgery? Striving to bring the body more in line with current feminine beauty ideals (e.g., larger breasts) would not necessarily alleviate body concerns. Indeed, drawing more attention to the body after cosmetic surgery may intensify views of the self as a collection of sexual body parts and lead to a greater likelihood of perceiving other physical flaws (cf. Calogero et al. 2009; Johnston-Robledo et al. 2007; Roberts 2004), potentially perpetuating a vicious cycle of self-objectification and body modification.
We did not assess body mass index or previous experiences with cosmetic surgery, both of which may account for some portion of women’s attitudes toward cosmetic surgery (Swami et al. 2008). In addition, our sample was comprised of predominantly White university students, which limits the generalizability of these findings to women across the age and ethnicity spectrum. It is noteworthy that although appearance concerns and self-objectification have been found to decrease with age (Halliwell and Dittmar 2003; McKinley 2006; Tiggemann and Lynch 2001), cosmetic surgery appears to be on the rise among older adults, primarily women (BAAPS 2009). Thus, the relationship between objectification processes and cosmetic surgery attitudes across the life span, and among non-university samples, requires further research. For example, as illustrated in Nirmal Puwar’s (2004) interviews with female members of the British parliament, women’s continued legitimacy within the legislature requires them to suffer constant sexist remarks and to chronically monitor their appearance to convey the right amount of femininity. It is possible that women who hold higher status positions, especially in traditionally male-dominated settings, might feel more pressure to undergo cosmetic surgery to enhance or maintain a feminized appearance to offset the potential backlash that comes from being perceived as violating traditional gender roles (Glick and Fiske 1999; Rudman and Glick 2001). These observations highlight that women from particular social and occupational groups may be more vulnerable to sexual and self-objectification and hold more positive attitudes toward cosmetic surgery. These understudied groups of women, such as women in effectual leadership positions, warrant further investigation with respect to their cosmetic surgery attitudes and behavior.
Overall, these findings suggest that objectification theory may have unique utility for predicting the degree to which women endorse, and potentially undergo, cosmetic surgery. Furthermore, if we agree that the objectification of women’s bodies represents a negative environmental context that encourages women to undergo cosmetic surgery, then positive environmental conditions that communicate the unconditional acceptance of women’s bodies may discourage women from endorsing cosmetic surgery. For example, drawing from Avalos and Tylka’s (2006) model of intuitive eating, environmental contexts that foster body acceptance (as opposed to body objectification) promote more intuitive eating among women because these contexts direct women’s attention more toward how their bodies feel and function instead of how their bodies look. When women focus more on how their bodies function and feel internally, rather than their external appearance, they are more likely to experience body appreciation and less likely to experience body shame (Tylka 2006). Future research is needed to investigate whether experiences of unconditional body acceptance predict less endorsement of cosmetic surgery, thereby affording some protection against an objectifying cultural milieu that encourages women to view their bodies as a collection of malleable body parts subject to surgical manipulation to alter their “looks.”
References
American Psychological Association Task Force on the Sexualization of Girls. (2007). Report of the APA Task Force on the sexualization of girls. Washington: American Psychological Association. Retrieved from http://www.apa.org/pi/wpo/sexualization_report_summary.pdf.
American Society of Plastic Surgeons (2009). 2009 report of the 2008 statistics: National clearinghouse of plastic surgery statistics. Retrieved from http://www.plasticsurgery.org/Media/stats/2008-US-cosmetic-reconstructive-plastic-surgery-minimally-invasive-statistics.pdf.
Aubrey, J. S. (2006). Exposure to sexually objectifying media and body self-perceptions among college women: An examination of the selective exposure hypothesis and the role of moderating variables. Sex Roles, 55, 159–172.
Avalos, L., & Tylka, T. L. (2006). Exploring a model of intuitive eating with college women. Journal of Counseling Psychology, 53, 486–497.
Bartky, S. (1990). Femininity and domination. New York: Routledge.
Berger, J. (1972). Ways of seeing. London: Penguin.
Blascovich, J., & Tomaka, J. (1991). Measures of social psychological attitudes. In J. P. Robinson, P. R. Shaver, & L. S. Wrightsman (Eds.), Measures of personality and social psychological attitudes (3rd ed., pp. 115–160). Ann Arbor: Institute for Social Research.
Breines, J. G., Crocker, J., & Garcia, J. A. (2008). Self-objectification and well-being in women’s daily lives. Personality and Social Psychology Bulletin, 34, 583–598.
British Association of Aesthetic and Plastic Surgeons (2009). Cosmetic rates of inflation: Male, female breast ops on the rise. Retrieved from http://www.baaps.org.uk/content/view/453/62.
Brown, A., Furnham, A., Glanville, L., & Swami, V. (2007). Factors that affect the likelihood of undergoing cosmetic surgery. Aesthetic Surgery Journal, 27, 501–508.
Calogero, R. M. (2009). Objectification processes and disordered eating in British women and men. Journal of Health Psychology, 14, 394–402.
Calogero, R. M. (2010). Assessment of self-objectification and related processes. In R. M. Calogero, S. Tantleff-Dunn, & J. K. Thompson (Eds.), Objectification of women: Innovative directions in research and practice. Washington: American Psychological Association.
Calogero, R. M., & Thompson, J. K. (2009a). Sexual self-esteem in American and British college women: Relations with self-objectification and eating problems. Sex Roles, 60, 160–173.
Calogero, R. M., & Thompson, J. K. (2009b). Potential implications of the objectification of women’s bodies for women’s sexual satisfaction. Body Image, 6, 145–148.
Calogero, R. M., Davis, W. N., & Thompson, J. K. (2005). The role of self-objectification in the experience of women with eating disorders. Sex Roles, 52, 43–50.
Calogero, R. M., Boroughs, M., & Thompson, J. K. (2007). The impact of Western beauty ideals on the lives of women and men: A sociocultural perspective. In V. Swami & A. Furnham (Eds.), Body beautiful: Evolutionary and sociocultural perspectives (pp. 259–298). New York: Palgrave Macmillan.
Calogero, R. M., Herbozo, S., & Thompson, J. K. (2009). Complimentary weightism: The potential costs of appearance-related commentary for women’s self-objectification. Psychology of Women Quarterly, 33, 120–132.
Calogero, R. M., Park, L. E., Rahemtulla, Z. K., & Williams, K. C. D. (2010). Predicting excessive body image concerns among British university students: The unique role of appearance-based rejection sensitivity. Body Image, 7, 78–81.
Cash, T. F., & Fleming, E. C. (2002). Body image and social relations. In T. F. Cash & T. Pruzinsky (Eds.), Body image: A handbook of theory, research, and clinical practice (pp. 277–286). New York: Guilford Press.
Davis, S. (1990). Men as success objects and women as sex objects: A study of personal advertisements. Sex Roles, 23, 43–50.
Davis, K. (1995). Reshaping the female body: The dilemma of cosmetic surgery. New York: Routledge.
Davis, D., & Vernon, M. L. (2002). Sculpting the body beautiful: Attachment style, neuroticism, and use of cosmetic surgeries. Sex Roles, 47, 129–138.
de Beauvoir, S. (1952). The second sex. New York: Vintage Books.
Delinsky, S. S. (2005). Cosmetic surgery: A common and accepted form of self-improvement. Journal of Applied Psychology, 35, 2012–2028.
Dellinger, K., & Williams, C. L. (1997). Makeup at work: Negotiating appearance rules in the workplace. Gender & Society, 11, 151–177.
Didie, E. R., & Sarwer, D. B. (2003). Factors that influence the decision to undergo cosmetic breast augmentation surgery. Journal of Women’s Health, 12, 241–253.
Dittmar, H., Lloyd, B., Dugan, S., Halliwell, E., Jacobs, N., & Cramer, H. (2000). The “body beautiful”: English adolescents; images of ideal bodies. Sex Roles, 42, 887–915.
Eagly, A. H., Ashmore, R. D., Makhijani, M. G., & Longo, L. C. (1991). What is beautiful is good, but... A meta-analytic review of research on the physical attractiveness stereotype. Psychological Bulletin, 110, 109–128.
Engeln-Maddox, R. (2006). Buying a beauty standard or dreaming of a new life? Expectations associated with media ideals. Psychology of Women Quarterly, 30, 258–266.
Evans, P. C. (2003). ‘If only I were thin like her, maybe I could be happy like her’: The self-implications of associating a thin female ideal with life success. Psychology of Women Quarterly, 27, 209–214.
Fairchild, K., & Rudman, L. A. (2008). Everyday stranger harassment and women’s objectification. Social Justice Research, 21, 338–357.
Fredrickson, B. L., & Roberts, T. A. (1997). Objectification theory: Towards understanding women’s lived experience and mental health risks. Psychology of Women Quarterly, 21, 173–206.
Fredrickson, B. L., Roberts, T. A., Noll, S. M., Quinn, D. M., & Twenge, J. M. (1998). That swimsuit becomes you: Sex differences in self-objectification, restrained eating, and math performance. Journal of Personality and Social Psychology, 75, 269–284.
Glick, P., & Fiske, S. T. (1999). Sexism and other “isms”: Interdependence, status, and the ambivalent content of stereotypes. In W. B. Swann, J. H. Langlois, & L. A. Gilbert (Eds.), Sexism and stereotypes in modern society: The gender science of Janet Taylor Spence (pp. 193–221). Washington: American Psychological Association.
Grabe, S., Hyde, J. S., & Lindberg, S. M. (2007). Body objectification and depression in adolescents: The role of gender, shame, and rumination. Psychology of Women Quarterly, 31, 164–175.
Grogan, S. (2008). Body image: Understanding body dissatisfaction in men, women and children. New York: Routledge.
Haiken, E. (1997). Venus envy: A history of cosmetic surgery. Baltimore: The Johns Hopkins University Press.
Halliwell, E., & Dittmar, H. (2003). A qualitative investigation of women’s and men’s body image concerns and their attitudes toward aging. Sex Roles, 49, 675–684.
Harper, B., & Tiggemann, M. (2008). The effect of thin ideal media images on women’s self-objectification, mood, and body image. Sex Roles, 58, 649–657.
Harrell, Z. A., Fredrickson, B. L., Pomerleau, C. S., & Nolen-Hoeksema, S. (2006). The role of trait self-objectification in smoking among college women. Sex Roles, 54, 735–743.
Harter, S. (1993). Causes and consequences of low self-esteem in children and adolescents. In R. Baumeister (Ed.), Self-esteem: The puzzle of low self-regard (pp. 87–116). New York: Plenum.
Henderson-King, D., & Brooks, K. D. (2009). Materialism, sociocultural appearance messages, and paternal attitudes predict college women’s attitudes about cosmetic surgery. Psychology of Women Quarterly, 33, 133–142.
Henderson-King, D., & Henderson-King, E. (2005). Acceptance of cosmetic surgery: Scale development and validation. Body Image: An International Journal of Research, 2, 137–149.
Hesse-Biber, S., Leavy, P., Quinn, C. E., & Zoino, J. (2006). The mass marketing of disordered eating and eating disorders: The social psychology of women, thinness, and culture. Women’s Studies International Forum, 29, 208–224.
Hill, M. S., & Fischer, A. R. (2008). Examining objectification theory: Lesbian and heterosexual women’s experiences with sexual and self-objectification. The Counseling Psychologist, 36, 745–776.
Jeffreys, S. (2005). Beauty and misogyny: Harmful cultural practices in the West. New York: Routledge.
Johnston-Robledo, I., Wares, S., Fricker, J., & Pasek, L. (2007). Indecent exposure: Self-objectifcation and young women’s attitudes toward breastfeeding. Sex Roles, 56, 429–437.
Kline, R. B. (2005). Principles and practices of structural equation modeling (2nd ed.). New York: Guildford.
Kozee, H. B., & Tylka, T. L. (2006). A test of objectification theory with lesbian women. Psychology of Women Quarterly, 30, 348–357.
Kozee, H. B., Tylka, T. L., Augustus-Horvath, C. L., & Denchik, A. (2007). Development and psychometric evaluation of the interpersonal sexual objectification scale. Psychology of Women Quarterly, 31, 176–189.
Lanyon, R. I., & Carle, A. C. (2007). Internal and external validity of scores on the Balanced Inventory of Desirable Responding and the Paulhus Deception Scale. Educational and Psychological Measurement, 67, 859–876.
Leary, M. R., & Kowalski, R. M. (1990). Impression management: A literature review and two-component model. Psychological Bulletin, 107, 34–47.
Lowery, S. E., Kurpis, S. E., Befort, C., Banks, E., Sollenberger, S., Nicpon, M. F., et al. (2005). Body image, self-esteem, and health related behaviors among male and female first year college students. Journal of College Student Development, 46, 612–623.
Markey, C., & Markey, P. (2009). Correlates of young women’s interest in obtaining cosmetic surgery. Sex Roles, 61, 158–166.
Martin, E. (1987). The woman in the body: A cultural analysis of reproduction. Boston: Beacon.
McKinley, N. M. (2006). The developmental and cultural contexts of objectified body consciousness: A longitudinal analysis of two cohorts of women. Developmental Psychology, 42, 679–687.
McKinley, N. M., & Hyde, J. S. (1996). The objectified body consciousness scale. Psychology of Women Quarterly, 20, 181–215.
McLaren, L., Kuh, D., Hardy, R., & Gauvin, L. (2004). Positive and negative body-related comments and their relationship with body dissatisfaction in middle-aged women. Psychology & Health, 19, 261–272.
McLaughlin, J. K., Wise, T. N., & Lipworth, L. (2004). Increased risk of suicide among patients with breast implants: Do the epidemiologic data support psychiatric consultation? Psychosomatics, 45, 277–280.
Mercurio, A. E., & Landry, L. J. (2008). Self-objectification and well-being: The impact of self-objectification on women’s overall sense of self-worth and life satisfaction. Sex Roles, 58, 458–466.
Moradi, B., & Huang, Y.-P. (2008). Objectification theory and psychology of women: A decade of advances and future directions. Psychology of Women Quarterly, 32, 377–398.
Moradi, B., Dirks, D., & Matteson, A. (2005). Roles of sexual objectification experiences and internalization of standards of beauty in eating disorder symptomatology: A test and extension of objectification theory. Journal of Counseling Psychology, 52, 420–428.
Morry, M. M., & Staska, S. L. (2001). Magazine exposure: Internalization, self-objectification, eating attitudes and body satisfaction in male and female university students. Canadian Journal of Behavioral Sciences, 4, 269–279.
Muehlenkamp, J. J., Swanson, J. D., & Brausch, A. M. (2005). Self-objectification, risk taking, and self-harm in college women. Psychology of Women Quarterly, 29, 24–32.
Noll, S. M., & Fredrickson, B. L. (1998). A mediational model linking self-objectification, body shame, and disordered eating. Psychology of Women Quarterly, 22, 623–636.
Park, L. E., Calogero, R. M., Harwin, M. J., & DiRaddo, A. (2009). Predicting cosmetic surgery interest: Interactive effects of appearance-based rejection sensitivity and negative appearance comments. Body Image, 6, 186–193.
Park, L. E., Calogero, R. M., Young, A. F., & DiRaddo, A.-M. (2010). Appearance-based rejection sensitivity predicts body dysmorphic disorder symptoms and cosmetic surgery acceptance. Journal of Social and Clinical Psychology.
Paulhus, D. L. (1991). Measurement and control of response bias. In J. P. Robinson, P. R. Shaver, & L. S. Wrightsman (Eds.), Measures of personality and social psychological attitudes (pp. 17–59). San Diego: Academic.
Pauls, C. A., & Crost, N. W. (2004). Effects of faking on self-deception and impression management scales. Personality and Individual Differences, 37, 1137–1151.
Puwar, N. (2004). Thinking about making a difference. British Journal of Politics and International Relations, 6, 65–80.
Quinn, D. M., Kallen, R. W., & Cathey, C. (2006a). Body on my mind: The lingering effect of state self-objectification. Sex Roles, 55, 869–874.
Quinn, D. M., Kallen, R. W., Twenge, J. M., & Fredrickson, B. L. (2006b). The disruptive effect of self-objectification on performance. Psychology of Women Quarterly, 30, 59–64.
Roberts, T.-A. (2004). “Female trouble”: The menstrual self-evaluation scale and women’s self-objectification. Psychology of Women Quarterly, 28, 22–26.
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton: Princeton University Press.
Rudman, L. A., & Glick, P. (2001). Prescriptive gender stereotypes and backlash toward agentic women. Journal of Social Issues, 57, 743–762.
Sarwer, D. B., Wadden, T. A., Pertschuk, M. J., & Whitaker, L. A. (1998). The psychology of cosmetic surgery: A review and conceptualization. Clinical Psychology Review, 18, 1–22.
Sarwer, D. B., LaRossa, D., Bartlett, S. P., Low, D. W., Bucky, L. P., & Whitaker, L. A. (2003a). Body image concerns of breast augmentation patients. Plastic and Reconstructive Surgery, 112, 83–90.
Sarwer, D. B., Magee, L., & Clark, V. (2003b). Physical appearance and cosmetic medical treatments: Physiological and socio-cultural influences. Journal of Cosmetic Dermatology, 2, 29–39.
Sarwer, D. B., Cash, T. F., Magee, L., Williams, E. F., Thompson, J. K., Roehrig, M., et al. (2005). Female college students and cosmetic surgery: An investigation of experiences, attitudes, and body image. Plastic and Reconstructive Surgery, 115, 931–938.
Shapiro, S. S., Wilk, M. B., & Chen, H. J. (1968). A comparative study of various tests for normality. Journal of the American Statistical Association, 63, 1341–1372.
Sperry, S., Thompson, J. K., Sarwer, D. B., & Cash, T. F. (2009). Cosmetic surgery reality TV viewership: Relations with cosmetic surgery attitudes, body image, and disordered eating. Annals of Plastic Surgery, 62, 7–11.
Steer, A., & Tiggemann, M. (2008). The role of self-objectification in women’s sexual functioning. Journal of Social and Clinical Psychology, 27, 205–225.
Swami, V., & Furnham, A. (2008). The psychology of physical attraction. London: Routledge.
Swami, V., Arteche, A., Chamorro-Premuzic, T., Furnham, A., Stieger, S., Haubner, T., et al. (2008). Looking good: Factors affecting the likelihood of having cosmetic surgery. European Journal of Plastic Surgery, 30, 211–218.
Swami, V., Chamorro-Premuzic, T., Bridges, S., & Furnham, A. (2009a). Acceptance of cosmetic surgery: Personality and individual difference predictors. Body Image, 6, 7–13.
Swami, V., Taylor, R., & Carvalho, C. (2009b). Acceptance of cosmetic surgery and celebrity worship: Evidence of associations among female undergraduates. Personality and Individual Differences, 47, 869–872.
Swim, J. K., Hyers, L. L., Cohen, L. L., & Ferguson, M. J. (2001). Everyday sexism: Evidence for its incidence, nature, and psychological impact from three daily diary studies. Journal of Social Issues, 57, 31–53.
Tangney, J. P., Miller, R. S., Flicker, L., & Barlow, D. H. (1996). Are shame, guilt, and embarrassment distinct emotions? Journal of Personality and Social Psychology, 70, 1256–1269.
Thompson, J. K., Heinberg, L. J., Altabe, M. N., & Tantleff-Dunn, S. (1999). Exacting beauty: Theory, assessment, and treatment of body image disturbance. Washington: American Psychological Association.
Tiggemann, M., & Kuring, J. K. (2004). The role of body objectification in disordered eating and depressed mood. British Journal of Clinical Psychology, 43, 299–311.
Tiggemann, M., & Lynch, J. E. (2001). Body image across the life span in adult women: The role of self-objectification. Developmental Psychology, 37, 243–253.
Tiggemann, M., & Rothblum, E. D. (1997). Gender differences in internal beliefs about weight and negative attitudes towards self and others. Psychology of Women Quarterly, 21, 581–593.
Tiggemann, M., & Slater, A. (2001). A test of objectification theory in former dancers and non-dancers. Psychology of Women Quarterly, 25, 57–64.
Tolman, D. L., Impett, E. A., Tracy, A. J., & Michael, A. (2006). Looking good, sounding good: Femininity ideology and adolescent girls’ mental health. Psychology of Women Quarterly, 30, 85–95.
Tylka, T. L. (2006). Development and psychometric evaluation of a measure of intuitive eating. Journal of Counseling Psychology, 53, 226–240.
Tylka, T. L., & Hill, M. S. (2004). Objectification theory as it relates to disordered eating among college women. Sex Roles, 51, 719–730.
Tylka, T. L., & Subich, L. M. (2004). Examining a multidimensional model of eating disorder symptomatology among college women. Journal of Counseling Psychology, 51, 314–328.
Wolf, N. (1991). The beauty myth. New York: Morrow.
Wylie, R. C. (1989). Measures of self-concept. Lincoln: University of Nebraska Press.
Zones, J. S. (2000). Beauty myths and realities and their impacts on women’s health. In M. B. Zinn, P. Hondagneu-Sotelo, & M. Messner (Eds.), Gender through the prism of difference (2nd ed., pp. 87–103). Boston: Allyn and Bacon.
Acknowledgement
This research was supported by an ESRC postdoctoral fellowship to Rachel Calogero.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Calogero, R.M., Pina, A., Park, L.E. et al. Objectification Theory Predicts College Women’s Attitudes Toward Cosmetic Surgery. Sex Roles 63, 32–41 (2010). https://doi.org/10.1007/s11199-010-9759-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11199-010-9759-5