
Abstract
Female sexual dysfunctions are common in the general population and remain a multifaceted problem that continues to be under recognized and under treated. This article reports a descriptive analytic study to assess prevalence of female sexual dysfunction and related factors for under treatment. In this cross sectional study, 1054 married women age 18–59 years were randomly selected from rural and urban health centers of Bushehr province. Data was collected by a questionnaire for demographic characteristic and Female Sexual Function Index for assessment of sexual dysfunction. For data analysis descriptive analytic tests were used. A total of 71.1% of subjects reported desire disorder. Prevalence of arousal, lubricating, orgasmic and pain disorders were 66.4, 38, 34.8 and 38.4%, respectively. Desire and arousal disorder were significantly interrelated with age, educational level, economic and marital status, smoking behavior of subjects and age, educational level, occupation and marital status of their husbands. Lubricating disorder was interrelated with age, educational level, occupation, smoking behavior and economic status of subjects and age, educational level, occupation of their husbands. Orgasmic disorder was significantly interrelated with age, educational level, occupation, economic status and smoking behavior of subjects and age, educational level and occupation of their husbands. There was a significant relationship between pain disorder with age, smoking, economic status of subjects and age, educational level and occupation of their husbands. 47.1 percent of subjects agreed that they had a problem. Only 9.2% of them reported going for treatment. Most of participants reported that they were ashamed of talking about these problems. Female sexual dysfunction is prevalent in Bushehr province but treatment rate is very low. Screening for sexual disorder, initiating dialogue by professionals and establishing a counseling plan may provide the opportunity to improve their sexual health.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sexual dysfunction is defined as disturbance in sexual desire and in the psycho-physiological changes that characterize the sexual response cycle and which cause marked distress and interpersonal difficulty [1]. Sexual disorders are very common in public population. These disorders can be classified in four groups: desire, arousal, orgasm and sexual pain disorders [2]. According to sexual function index, two extra cases can be added to the mentioned groups which include disorder in vaginal lubrication during intercourse and satisfaction of sexual relationship. According to Safarinejad’s research of 2626 Iranian women, the prevalence of sexual disorder was 31.5%. The prevalence increased with age, from 26% in women aged 20–39 years to 39% in those >50 years old. 37% reported orgasmic disorders, 35% desire disorders and 30% arousal disorders, all of which increased significantly with age. Pain disorder was reported by 26.7%, occurring most frequently in women aged 20–29 years. In this study the educational level and marriage age (<18 years) were inversely correlated with the risk of orgasmic, desire and arousal disorders. No significant differences were detected in smoking history, the presence of previous pelvic surgery, and contraception methods used [3]. Another research which is done in Quazvin city of Iran showed that 89% of subjects suffered from sexual disorders. Commonest problem (41.1) was desire disorder [4]. Study of Bahrainian et al. [5] showed sexual desire, arousal, orgasm and pain disorder 27, 28, 40 and 39%, respectively. A study conducted on 179 Turkish women of ages 18–69 years old showed that 46.9 of subjects were suffering from sexual disorders. The prevalence of sexual dysfunction for each domain also increased with age. Sexual dysfunction was observed as significantly higher in the presence of older age, lower educational level, unemployment status, chronic disease, multi parity and menopause status [6]. Another study conducted in 1998 on English, German, French and Italian women showed that disorder in sexual desire differed from 11% in 20–29 years-old to 35% in 60–70 years-old women [7].
In a study by Ponholzer et al. on 703 Austrian women who aged between 15 and 43, sexual desire, arousal and orgasm disorder were 22, 35 and 39%. All problems were related to age. Disorder in sexual desire, and arousal were related to exercise and orgasm disorder was related to psychological stress [8]. Two studies in California and Egypt showed prevalence of sexual disorder was 33 and 68.9%, respectively [9, 10].
The etiology of sexual dysfunction is frequently multifactor as it relates to general physical and mental well-being, quality of relationship, past sexual functioning, social class, education, employment, life stressors, personality factors, the presence of a sexual partner, and partner’s age and health, Culture, social customs of the community, and religion [11, 12]. Studies showed that despite prevalent sexual disorders, many women may find it difficult to talk to their physicians about sexual concerns and few had sought medical care for these problems. On the other hand, many physicians are uncomfortable discussing sexual issues with their patients [10, 13, 14]. Obstacles to discussing sexual health included limited time and training, embarrassment, believing that the problem is not serious, not being bothered by the problem, difficulties regarding access to or affordability of medical care, and/or a lack of awareness of available treatments [15, 16]. In Wendt’s research, 92% of women considered it appropriate to be asked about sexuality in general. However, 76–99% had never been asked such questions [17].
Data on prevalence, risk factor for sexual disorder and quality management of these disorders are rare in Iran especially in some areas. This study was conducted to detect the prevalence and risk factors of female sexual dysfunction and related factors to non treatment in Bushehrian women.
Method and Material
This is a cross-sectional study to assess the prevalence and associated risk factors of sexual dysfunction and the reasons for not consulting in Bushehrian women referred to urban and rural health centers in Bushehr province. Sample size was 1058 with calculating the confidence interval as 95%, prevalence of sexual dysfunction as 20% and precision as 0.04%. All women were married and aged between 18 and 59 years old. Cluster sampling was done on the basis of age and covered population of each center. In each cluster, the sampling was done in a random way. Exclusive criteria included, chronic disease such as high blood pressure, heart or pulmonary disease, diabetes, known psychotic diseases and the absence of subjects’ husbands during the 4 weeks before completing the questionnaire. These diseases were diagnosed on the basis of the participants’ speech, and the inaccessibility of participants’ medical files was the limitation of this research.
Data gathering tools consisted of a demographic questionnaire and the female sexual function index. Demographic characteristic questionnaire include age, marriage of subjects and narcotic and psychotic drugs use of subjects’ husbands. Sexual dysfunction was evaluated by female sexual function index. This standardized questionnaire evaluates six domain of female sexual function during 4 week (Desire, arousal, lubrication, orgasm, satisfaction and pain during intercourse). Sexual function index included 19 questions. Sexual desire was assessed as frequency and desire level with 2 questions. Arousal was as frequency, level, confidence and satisfaction with 4 questions. Lubrication was assessed as frequency, difficulty, frequency of maintaining and difficulty in maintaining with 4 questions. Orgasm was assessed as frequency, difficulty and satisfaction with 3 questions. Satisfaction of sexual relationship was assessed as the amount of closeness with partner, sexual relationship and overall sex life with 3 questions. Pain was assessed as pain frequency during vaginal penetration and pain frequency following vaginal penetration with 3 questions. Ranges for questions 3–14 and 17–19 were 0–5, and for items 1, 2, 15 and 16 were 1–5. The score for desire questions was 0.6, for question related arousal and lubrication 0.3 and 0.4 for orgasm, satisfaction and pain disorder questions. In each domain, the scores under 3.9 were considered as sexual dysfunction (score <3.9 was <65% of maximum achievable score in each domain). The 6 domains together showed overall sexual disorder, so that the score above or equal to 23 was considered as normal, 18–23 as mild sexual disorder, 11–17 as moderate and score 10 or lower than that as sever sexual disorder. This index previously has been used in Iran by Safarinejad with mentioned score [3]. The Index was translated to Persian and then translated again to English, and some questions about reasons of not consulting the doctor for treating sexual disorders were added to it. The validity of this questionnaire was confirmed by using the correctors’ verdict and its reliability by pilot study and Alpha (Cronbach) method and the coefficient of 0.85.
The procedure for data collection was such that at first, the researchers presented a letter of introduction from the research department to health care centers and with supervisors’ permission selected research subjects. The purpose of this research was explained for all participants. All participants’ contribution was voluntarily. The study complies with declaration of Helsinki and was approved by the institutional ethics committee of Bushehr University of medical sciences and gave written informed consent.
Data gathering was also done through face to face interview. After gathering, data were coded and put into a computer. Then, data was analyzed by analytic-descriptive, statistic tests such as T test, ANOVA and Pearson’s correlation coefficient. All statistic tests, under 0.05 were assumed as significant.
Results
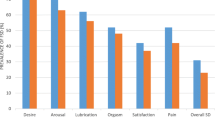
The average age of samples was 35.78 ± 11.88 and the average of marriage age was 20.38 ± 4.44. The results showed overall 37.7% prevalence of female sexual dysfunction. So that 20.4% were mild, 6.6% moderate and 8.3% severe. 71.1% of subjects reported desire disorder. Prevalence of arousal, lubricating, orgasmic, pain disorders and satisfaction of sexual relationship was 66.4, 38, 34.8, 38.4 and 24.9%. Table 1 shows general characteristics of subjects, and Tables 2 and 3 show the relationship between demographic characteristics and different type of sexual disorder. 47.1% of participants believed that they had sexual problems, but only 9.2% had consulted the doctor. The reasons for not consulting the doctor reported as follow: 54.3% of participants were ashamed of talking about their problems, 22.6% had no access to or in lack of information about service centers or no trust in treating procedures, 25% had no need for treating because regardless their husbands’ satisfaction of sexual relationship or not being allowed by them going to any health provider consultation, 3.7% had fear of revealing the secret and job or family problems and 3/4% had unsuitable economical condition. Pearson’s correlation test showed that by increasing age of subjects or their husbands’, the average score for different type of sexual disorder decreases and this relation was statistically significant (P value in all domain was lower than 0.0001). Moreover, with increasing the hours of weekly sportive activity, average score of sexual function increased in all domain, and this relation was statistically meaningful (P value was 0.002 in sexual pain and in other domain lower than 0.0001).
Discussion
The results showed an overall 37.7% prevalence of female sexual dysfunction. The study showed that disorder in all domain of sexual function is prevalent and the most prevalent type is desire disorder. Prevalence of sexual disorders and the most prevalent type of these problems are different between countries and different area of one country. Studies have shown that the disorder in sexual desire has been lower than what has been found in present study [7, 8, 10, 18]. Safarinejad showed overall a 31.5% of female sexual dysfunction in Iranian women. In studies of Safarinejad, Bahrainian, Bolourian et al. on Iranian women and Ponholzer et al. on Austrian women, the most prevalent type of sexual dysfunction was orgasmic disorder and that these studies disagree with the present study [3, 5, 8, 19]. Arman et al., Yekehfallah and Bachmann showed that desire disorder is the most prevalent of sexual disorder between all domains of sexual dysfunction and that these studies agree with the present study [4, 7, 20]. It seems that differences in the prevalence of sexual problem in different study may reflect cultural and socioeconomic factors, methodology of the studies and the demographic characteristics of the subjects. Since man-superiority is still common, and on the other side, expressing sexual desire by women is still considered as a taboo, most women hide or suppress their desires for sexual intercourse with their husbands. This situation may be a reason for increasing the disorder in sexual desire and arousal.
This research showed a meaningful statistical relationship between age increase and sexual disorder, that it agrees with other studies [3, 7, 8, 19]. Certainly, physiological changes in women which result from age increase have an important role in this relationship.
The results showed that disorder in all domain of sexual function except the pain during intercourse is related to educational level of subjects and all domains are related to educational level of their husbands. Kayan et al. reported a meaningful statistical relationship between women’s low level education and no participation in social activities and their sexual disorder [6]. The studies have also shown that sexual function is related to social class [11]. In present study, like the previous ones, illiterate women or those who have received a low level of education have got lower scores in sexual function. Also, those women whose husbands had official jobs got a higher average in sexual function. Since sexual intercourse is a reciprocal, consciously–done and training-related relationship, this can be accepted that social status, education and economical condition affect this kind of relationship. Since sexual intercourse is a physical process, unsuitable economical-social condition by creating tension in life can affect this process like the other aspects of life.
Present research showed a meaningful statistical relationship between smoking behavior in subjects and their husbands and disorder in some domains of sexual function. However, there is no conformity between these results of this research and the one which was done by Safarinejad [3]. This results confirmed study of Oksuz et al. [18]. The reason for this difference may be the research society. Smoking behavior is usually more common in women of families who are exposed to much stress and lower social status. In most parts of the Bushehr province, smoking behavior (hookah) is common in women, especially among those who have lower education. Identifying those who have this problem, supporting them socially and helping them to wean from smoking can help in decreasing sexual disorders. In this research there was no meaningful statistical relationship between drinking alcohol, using narcotics or psychotic drugs and disorder in sexual function. One reason for the absence of this relationship may be that using these factors are rarely used and rarely reported by the people. Despite attempts to make a suitable relationship with the subjects and emphasizing that the information would be kept a secret, using those materials or activities are not truly mentioned and can be considered one of the limitations of the research.
The results showed that sexual disorder is less in those women who have more physical activity and allocate more hours to sportive activity through a week. This result is just like what was found in Safarinejad’s research in Iran [3]. Wang et al. observed a meaningful statistical relationship between sexual function and less stress and also, more daily physical activities [21] Certainly, brain activities and neurotransmitter which are exuded during doing physical activities can result in stress deduction; decreasing daily tensions can also cause improving one’s function in different aspects of life such as sexual cycle.
In spite of the high prevalence of sexual problems, most women had not consulted the physician about these problems. Most subjects expressed shame, had no information of or access to medical centers as the reasons for not consulting the doctor. In Moreira’s research 37% of women reported lack of sexual pleasure but 2% of men and women had talked to a medical doctor about their sexual problems. He also said that this is largely due to believing that the problem is not serious, not being bothered by the problem, difficulties regarding access to or affordability of medical care, and/or a lack of awareness of available treatments [15]. In Bachmann’s study obstacles to discussing sexual health included limited time and training, embarrassment, and absence of effective treatment options. He believes that if the health expert and health provider begin to talk about this problem, this can be a key to stimulate the help seekers to express their problem [16].
Cause of differences between reasons of not consultation for sexual problems in different studies may be cultural factors, attitude of population about sexuality, data gathering tools and quantity and quality of questions about this issue.
In many societies, sexual function and problem are of those difficulties about which few people talk clearly. The information about these issues is mostly received secretly from those friends and relatives who may not have scientific and true information. Unknowingness and untrue information can increase sexual disorders. On the other hand, considering these problems as a taboo cause the remedy not to be done or be delayed and this can make the problem more acute. Training classes can help in recognizing and treating the patient and eventually decreasing the prevalence of sexual disorders. Topics for these classes could include talking about the quality of sexual function in marriage and ways to access information and treatment.
In many societies discussion about sexual issues are often not volunteered. Initiating dialogue by women’s health providers about this issue, of course respecting the clients’ sense of privacy and in the frame of professionalism can help in identifying sexual dysfunction.
The other matter is that most health providers do not have enough information on sexual function and disorders related to it, or do not like to talk about this issue or do not know the way they can provide treatment. Training classes for health care providers about sexuality and sexual dysfunction would also help them to recognize sexual problems in patients and can be a step toward decreasing sexual problems and improving sexual relationship in women.
Conclusion
Female sexual dysfunction is frequent in research population, but very few individuals seek medical help for these disorders. Most of participants reported that they were ashamed of talking about these problems. Training classes for clients and health care providers about sexuality and sexual dysfunction, screening for sexual disorder, and initiating dialogue by professionals can help in recognizing, treating and eventually decreasing the prevalence of sexual disorders and suffering. More research in different areas of the country is essential to further understand the prevalence of female sexual dysfunction and quality of recognizing, help seeking and treatment for these disorders.
Limitation of the Research
One of the limitations of this research was the inaccessibility of the sample’s medical file in order to find out if there had been any symptoms of such diseases or dysfunction previously. Information was recorded on the basis of what was reported. Although the researcher tried to emphasize that the information would be kept as a secret, another limitation was the person’s sense of privacy or lack of privacy during research inquiry.
References
Marthol, H., Hilz, M.J.: Female sexual dysfunction: a systematic overview of classification, pathophysiology, diagnosis and treatment. Fortschr. Neurol. Psychiatr. 72(3), 121–135 (2004)
David, A.B., Rosemary, B.: Sexuality and sexual dysfunction. In: Jonathan, S.B. (eds) Berek and Novak’s Gynecology, 14th edition, pp. 324–325. Lippincott Williams & Wilkins publisher, USA (2007)
Safarinejad, M.R.: Female sexual dysfunction in a population-based study in Iran: prevalence and associated risk factors. Int. J. Impot. Res. 18(4), 382–395 (2006)
Yekehfallah, L., Goodarzi, M.: Prevalence of sexual dysfunction and related factors among married couples in Qazvi. J. Huazhong Univ. Sci. Technol. Med. Sci. 1(13), 49–55 (2009). (Full text in Persian)
Bahrainian, S., Saki, K.: Sexual dysfunction in married women attending primary care centers in Khoram Abad; Iran. Int. J. Clin. Endocrinol. Metab. 1(4), 294–298 (2000). (Full text in Persian)
Cayan, S., Akbay, E., Bozlu, M., Canpolat, B., Acar, D., Ulusoy, E.: The prevalence of female sexual dysfunction and potential risk factors that may impair sexual function in Turkish women. Urol. Int. 72(1), 52–57 (2004)
Hayes, R.D., Dennerstein, L., Bennett, C.M., Sidat, M., Gurrin, L.C., Fairley, C.K.: Risk factors for female sexual dysfunction in the general population: exploring factors associated with low sexual function and sexual distress. J. Sex. Med. 5(7), 1681–1693 (2008)
Ponholzer, A., Roehlich, M., Racz, U., Temml, C., Madersbacher, S.: Female sexual dysfunction in a healthy Austrian cohort: prevalence and risk factors. Eur. Urol. 47(3), 366–374 (2005)
Addis, I.B., Van, Den., Eeden, S.K., Wassel-Fyr, C.L., Vittinghoff, E., Brown, J.S., Thom, D.H.: Sexual activity and function in middle-aged and older women. Obstet. Gynecol. 107(4), 755–764 (2006)
Elnashar, A.M., El-Dien, I.M., El-Desoky, M.M., Ali, OM., El-Sayd, Mohamed, Hassan, M.: Female sexual dysfunction in Lower Egypt. BJOG. 114(2), 201–206 (2007)
Aslan, E., Fynes, M.: Female sexual dysfunction. Int. Urogynecol. J. Pelvic. Floor Dysfunct. 19(2), 293–305 (2008)
Fourcroy, J.L.: Customs, culture, and tradition–what role do they play in a woman’s sexuality? J. Sex. Med. 3(6), 954–959 (2006)
Nicolosi, A., Laumann, E.O., Glasser, D.B., Moreira Jr., E.D., Paik, A., Gingell, C.: Global study of sexual attitudes and behaviors investigators’ group. Sexual behavior and sexual dysfunctions after age 40: the global study of sexual attitudes and behaviors. Urology. 64(5), 991–997 (2004)
Ho, T.M., Fernández, M.: Patient’s sexual health: do we care enough? J. Ren. Care. 32(4), 183–186 (2006)
Moreira Jr., E.D., Kim, S.C., Glasser, D., Gingell, C.: Sexual activity, prevalence of sexual problems, and associated help-seeking patterns in men and women aged 40–80 years in Korea: data from the global study of sexual attitudes and behaviors (GSSAB). J. Sex. Med. 3(2), 201–211 (2006)
Bachmann, G.: Female sexuality and sexual dysfunction: are we stuck on the learning curve? J. Sex. Med. 3(4), 639–645 (2006)
Wendt, E., Hildingh, C., Lidell, E., Westerståhl, A., Baigi, A., Marklund, B.: Young women’s sexual health and their views on dialogue with health professionals. Acta. Obstet. Gynecol. Scand. 86(5), 590–595 (2007)
Ergun, oksuz., Smitten, Malhan.: Prevalence and risk factors for female sexual dysfunction in Turkish women. J. Urol. 175(2), 654–658 (2006)
Bolourian, Z., Ganjloo, J.: Evaluating sexual dysfunction and some related factors in women attending Sabzevar Health Care Centers. Med. J. Reprod. InFertil. 2(8), 163–170 (2007). (Full text in Persian)
Arman, S., Fahami, F., Hassanzahraei, R.: A comparative study on women’s sexual functioning disorders before and after menopause. Rahavard Danesh. J. Arak Uni. Med.Sci. 32(8), 1–7 (2008). (Full text in Persian)
Wang, T.F., Lu, C.H., Chen, I.J., Yu, S.: Sexual knowledge, attitudes and activity of older people in Taipei, Taiwan. J. Clin. Nurs. 17(4), 443–450 (2008)
Acknowledgments
The authors would like to acknowledge the assistance of personal in urban and rural health care of Bushehr province.
Funding
This study was funded by a grant from Bushehr University of Medical Sciences.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bagherzadeh, R., Zahmatkeshan, N., Gharibi, T. et al. Prevalence of Female Sexual Dysfunction and Related Factors for Under Treatment in Bushehrian Women of Iran. Sex Disabil 28, 39–49 (2010). https://doi.org/10.1007/s11195-010-9149-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11195-010-9149-5