
Abstract
The present paper examines the relationship between child mortality and fertility at the micro level. We use individual data collected quarterly within the health and demographic surveillance system of the rural community of Niakhar (Fatick, Senegal). Birth histories of 2,884 women born between 1932 and 1961 are analyzed. The determinants of completed fertility are investigated using a standard Poisson Regression Model. The global effect of child mortality on total and net fertility is found to be positive. To our knowledge, this is the first paper to provide evidence for the child survival hypothesis—an effect of child mortality on net fertility—at the micro level. We further identify an inverted-U shaped relationship between child mortality and net fertility. The implication is that health policies aiming at reducing child mortality have indirect effects on desired fertility; yet only a steep decrease in child mortality would be likely to trigger fertility declines.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Sub-Saharan Africa (SSA) has long been trapped in a crisis characterized by high mortality and fertility rates. However, mortality rates are continuously decreasing in a significant number of SSA countries since the 1950s, and life expectancy is projected to increase (United Nations 2012). Concurrently, fertility rates remain markedly high: 39 out of the 55 African countries exhibit high current fertility, namely five children or more per woman (United Nations 2011). This results in a growing demographic pressure. Demographic transition theories usually postulate that fertility is likely to follow the decrease in child mortality after some lag. Concerns are raised about the validity of these theories for the sub-Saharan African context, as they apparently fail to explain contemporary demographic patterns. Everything happens as if most countries in SSA were still at the early stage of the transition (Bongaarts and Casterline 2013). The availability of family planning services is crucial for the fertility transition to occur. In developing countries, knowledge of contraception is now quite widespread. However, Cleland et al. (2011) report that attitudinal resistance remains a severe barrier in SSA, so that progress towards adoption of contraception has been dramatically slow. Studies reveal that even though some components of fertility arise from an unmet need for family planning, its largest share is actually desired by households (Bongaarts 2011). Acknowledging the statistical regularities previously reported, we will consider fertility as a choice variable. Households are expected to alter their fertility behavior according to the surrounding socio-economic and epidemiological context, which can change incentives for childbearing.
Addressing the extent to which households adjust their behavior in a context of low child survival probability is a decisive research question. Aside from direct health outcomes, health policies aiming at improving child survival could have indirect demographic effects via changes in household fertility behavior.Footnote 1 There is as yet no clear consensus in the economic and demographic literature as regards the relationship between child mortality and fertility in developing countries. A distinction is made between total fertility (the number of births per woman), and net fertility (the number of surviving children). The replacement hypothesis posits that households have additional children to replace the ones that they lose, involving a targeted number of children chosen by parents. Replacement behavior would then generate a positive relationship between child mortality and total fertility, leaving net fertility unchanged. However, it is worth noticing that among micro studies which attempt to empirically test the replacement hypothesis, estimates of direct replacement rates are systematically smaller than 0.5, as pointed out in Kalemli-Ozcan (2003). This means that a replacement strategy cannot be fully realized, as one-to-one replacement is never achieved, due for instance to physiological limits such as birth spacing, breastfeeding period or limited fecundity. In practice, replacement behavior is thus likely to generate a positive (negative) relationship between child mortality and total (net) fertility. The child survival hypothesis (also known as the hoarding motive) postulates a positive effect of child mortality on the number of surviving children. When uncertainty about child survival is high, households would generate a precautionary demand for children in order to ensure a sufficiently large family size. This theory predicts that improvements in child survival will lead to decreasing total and net fertility rates.
Clearly, replacement behavior alone is inconsistent with the observation of past and present patterns of demographic transition, during which both total and net fertility follow the decrease in child mortality. Within the endogenous fertility framework, several theoretical models have been developed to reveal the underlying factors behind the demographic transition. Research on the topic dates back to the seminal works of Becker et al. (1973, 1976, 1988), in which parents are assumed to have a dynastic utility function depending on their own consumption as well as on the number and consumption of descendants in all generations. In this framework, an increase in income, by affecting the cost of surviving children, should lead to a trade-off between child quantity and child quality. A permanent decline in the level of child mortality would, however, not directly affect the demand for surviving children (Becker and Barro 1988).Footnote 2 An increase in the survival probability has nonetheless the effect of lengthening the period during which returns to investment in children’s human capital (quality) are realized. Parents may thus substitute child quality for child quantity following an exogenous mortality decline, which will lead to a decrease in net fertility, as pointed out in O’Hara (1975). Another factor that has been shown to play a central role in the demographic transition is the uncertainty about child survival. Sah (1991) predicts a positive impact of child mortality on fertility in the first attempt to incorporate uncertainty in a model of endogenous fertility choice. Also allowing for uncertainty about the number of surviving children, Kalemli-Ozcan (2003) builds a quantity-quality model of children and provides support for the hoarding motive, so that child mortality has a positive effect on both total and net fertility. There is a lack of micro-level studies that quantitatively test the actual realization of a fertility strategy (replacement versus child survival hypothesis) at the end of the reproductive life span, partly due to the lack of data availability. The demographic and epidemiological monitoring of the population of Niakhar (Fatick, Senegal) allows us to empirically investigate this research question.
This paper conducts an in-depth quantitative analysis of the determinants of completed fertility in order to provide a better understanding of the relationship between child mortality and fertility in a rural sub-Saharan African context. Empirical analysis of both gross and net effects of child mortality on fertility is carried out. We use a large longitudinal data set to analyze the birth histories of 2,884 women born between 1932 and 1961. The determinants of completed fertility are investigated using a standard Poisson Regression Model. Different model specifications are estimated to emphasize the potential heterogeneous effects of child mortality. The global impact of child mortality on total and net fertility is found to be positive. To our knowledge, this is the first paper providing evidence for the child survival hypothesis at the micro level. However, the effect on net fertility, even though positive and significant, is fairly small. We further show that the relationship is of non-linear nature, as the amplitude and the direction of the effect of child mortality vary with the number of child losses. More specifically, an inverted-U shaped relationship between child mortality and net fertility is exhibited. Finally, we find that the effect of child mortality is the highest for women belonging to older cohorts and for women who start childbearing earlier.
Although infant and child mortality rates are declining continuously since the 1950s, progress have been slower in the past two decades (United Nations 2012).Footnote 3 In line with this empirical observation, we show that the highest fertility rates are essentially associated with relatively low values of child mortality. The implication is that, along with family planning policies which only affect unwanted fertility, health policies aiming at reducing child mortality have indirect effects on desired fertility. However, the decrease in child mortality should be steeper than the one experienced in SSA so far in order to trigger fertility declines.
2 Background and existing studies
The determinants of completed fertility are clearly identified in the demographic and economic literature. We thus understand completed fertility to be primarily influenced by economic conditions, educational and occupational status, religion, access to family planning services, child mortality, marital status, ethnicity, and social norms.Footnote 4 Accumulating evidence has shown that child mortality and fertility are inextricably linked (Montgomery and Cohen 1998). A large number of studies document a positive association between gross fertility and child mortality (Taylor et al. 1976; Balakrishnan 1978; Olsen 1980; Olsen and Wolpin 1983; Rosenzweig and Schultz 1983; Eckstein et al. 1999; Handa 2000; Hossain et al. 2007). Empirical studies providing evidence of a net effect of child mortality on fertility are much scarcer. To our knowledge, only three studies document both effects of child mortality on total and net fertility (Schultz 1997; Angeles 2010; McCord et al. 2010), and solely at the macro level. Using calorie availability per capita as an instrument for child mortality, Schultz (1997) finds that improvements in child health are associated with slower population growth during the period 1972–1988 in a panel of 80 developing countries. Angeles (2010) employs dynamic panel GMM techniques to account for the potential endogeneity of fertility and shows that both gross and net fertility are negatively affected by reductions in child mortality for a panel of 118 countries over the period 1960–2000. McCord et al. (2010) instrument child mortality with an ecologically-based spatial index of the stability of malaria transmission across countries and find that child mortality declines are likely to account for over half of the fertility decline during the demographic transition. The lack of micro data collected over a sufficiently long time-span, in particular in low-income countries, makes it difficult to quantify the net effect of child mortality on fertility at the individual level. Hence, microeconometric estimates of the effect of child mortality on fertility in developing countries usually rely on dynamic models and are based on data covering relatively short time periods.
Other attempts have been made to estimate the determinants of fertility using count data models of fertility, which are suitable for the analysis of birth histories.Footnote 5 However, these studies are mainly based on household composition data, and not on completed fertility. The effect of child mortality on fertility is investigated in some of these empirical papers. Nguyen-Dinh (1997) documents a small and positive effect of community-level child mortality on fertility in Vietnam.Footnote 6 In his analyses of fertility in four Arab countries, Al-Qudsi (1998a, b) finds that infant mortality exerts a positive impact on fertility for replacement purposes. Finally, Atella and Rosati (2000) stress the importance of the uncertainty about child survival in determining fertility choices. Using data from India, the authors show that the negative fertility response to a decrease in child mortality may be dampened if it is also associated with a reduction of its variance. Such studies are typically designed to test the direct replacement effect of child mortality on fertility (birth spacing and timing) during the observation period. They provide a better understanding of the short-term aspect of the child mortality-fertility relationship, yet they do not bring any information about the actual realization of a strategy at the end of a woman’s reproductive life.
The determinants of completed fertility appear to have been investigated in only a few empirical papers. Since these studies are based on data from developed countries, where child mortality is low, none of them examines the effect of child mortality on fertility. The present paper aims at filling this gap by determining the quantitative contribution of child mortality on completed fertility in a fairly representative rural West African setting.
3 Data: the Niakhar Health and Demographic Surveillance System
The rural community of Niakhar is located in the Fatick region of Senegal, 135 km east from Dakar. A Health and Demographic Surveillance System (HDSS) has been set up in 8 villages since 1962, and has been extended to 22 more villages in 1983.Footnote 7 Since 1983, the geographical boundaries of the study zone comprehends a total area of 203 km\(^{2}\) and encompasses 30 villages. Niakhar is Africa’s oldest and still operational statistical observatory, and world’s second-oldest (after Matlab, Bangladesh). This is a fairly representative rural West African setting, and the study population is relatively homogeneous in terms of socio-economic characteristics. The Serer ethnic group comprises 96.5 % of the population. Islam and Christianity are the main religions, representing respectively 76 and 21 % of the population. The major cause of migration is seasonal migration to Dakar, the closest major urban center, for economic motives. Agriculture is the main source of livelihood, and formal education is very low. Villages are subdivided into hamlets, which are themselves subdivided into compounds. Compounds are constituted of one or more ‘kitchens’ (households) which bring together members of the extended patrilineal family. The average household size is approximately 13 persons. Further information on the study area can be found in Delaunay et al. (2002). There are large variations between households regarding both fertility and child mortality rates. Hence, it is a convenient setting to analyze the relationship between these two variables.
At the onset of the HDSS, major life events such as birth histories were collected retrospectively among the residents of the area to serve as a baseline for the follow-up. The HDSS consists in conducting quarterly exhaustive surveys within the study area. Thoroughly reliable data on all demographic events are systematically recorded. These events include pregnancies, deaths, marriages, migrations (inside or outside the study area), as well as changes in social characteristics. Such events are also being retrospectively and then systematically collected among the immigrants as they enter the study area. Accounting of pregnancies is practically comprehensive as a result of the quarterly follow-up. Although likely limited, the possibility of underreporting of pregnancies is still possible, especially those ending in induced abortion. Data on mortality events are reported via verbal autopsy, and causes of death follow World Health Organization’s ICD-9 classification. Altogether, this results in an exhaustive and systematic monitoring of the study population.
Alongside the systematic collection of data, several cross-sectional surveys were conducted for specific purposes. This study uses a cross-sectional survey conducted in 2003 to derive economic characteristics of households which remained supposedly path-dependent until the mid 2000s. In this survey, non-monetary data on living and economic conditions were collected in an exhaustive manner, which allows us to estimate measures of multidimensional poverty. More specifically, we estimate an index of deprivation in living standards. The dimensions taken into consideration are: access to electricity, type of sanitation facilities, source of drinking water, type of cooking fuel, possession of certain assets, and flooring material of housing. This index has been calculated following the methodology outlined in Alkire and Santos (2010), which is one of the international standards for the measurement of multidimensional poverty with non-monetary data.
The long time period of data collection (from 1962 to 2010 given our last data extraction) allows us to conduct an individual analysis on completed fertility. We analyze the complete birth histories of 2,884 women born between 1932 and 1961. The sample is left censored because of data availability, and is right censored as the fecund period is usually assumed to last from 15 to 49 years old (following United Nations standards). The analysis does not include women who died before the end of their reproductive years. Furthermore, the study is zero-truncated, as it excludes nulligravidas (women who have never been pregnant), but not necessarily nulliparas (women who never gave birth). The drivers of fertility are obviously not the same as the factors determining infertility. Moreover, infertility and voluntary childlessness are very rare in the study area (Ronsmans et al. 2001). The long time-span of the data also allows us to distinguish between six different birth cohorts of five-year intervals (1932–1936 for the earliest cohort, and 1957–1961 for the latest).
For the sake of simplicity, we will denominate total fertility (TF) the number of times a woman has been pregnant (her obstetrical history, that is, gravidity) and net fertility (NF) the number of her children who survived to age 5. TF and NF will be the two dependent variables used in the different model specifications. The occupation variable has been defined as the occupation held by a woman for the longest period of time during her reproductive life. Descriptive statistics of the variables used in the analyses are given in Table 1. The methodology employed in the study to explore the link between child mortality and fertility is presented in the next section.
4 Model specifications
The use of an inappropriate model to estimate fertility outcomes can lead to serious drawbacks (Caudill and Mixon 1995; Winkelmann 2008). However, suitable models appear to be used only in a few empirical applications. We need a model that allows us to capture the discrete and non-negative nature of our two dependent variables (TF and NF). Obstetric and birth histories are typical count data, which call for the use of count data models. Winkelmann and Zimmermann (1994) indicate that the mean-variance equality of the standard Poisson Regression Model is often violated due to the recurrent presence of underdispersion in fertility data. Yet, this is most likely to occur when infertility is taken into consideration, which is not the case for our study. The outcome of zero counts in fertility data is mostly driven by physiological issues rather than by a choice process. For that reason, Santos Silva and Covas (2000) argue that the underdispersion problem that characterizes completed fertility data cannot be solved by replacing the Poisson distribution by a model with a flexible mean to variance ratio. Instead, the authors build a modified hurdle model which takes into account the fact that zeros and positive counts are generated by different mechanisms. Such a model has some desirable features for fertility studies, yet its application is heavily constrained by data availability. For example, in their application to Portuguese data, Santos Silva and Covas (2000) cannot interpret the results of the model for zero counts, as only 37 out of 1,093 observations correspond to childless couples. We thus estimate a standard Poisson Regression Model for the determinants of completed fertility. Other count data models have also been employed, namely Generalized Poisson Regression Models and Hurdle Models. However, predicted probabilities for the two dependent variables were less accurately estimated compared with the standard Poisson Regression Model.
Let the count outcome \(y _{i}\)—alternatively the TF and NF of a woman \(i\), be a Poisson random variable. Hence:
\(X_i\) is the vector of covariates of woman \(i\). TF is taken to be the dependent variable in a first set of model specifications, and NF in a second set. Recall that \(y=0\) is only possible for NF. The explanatory variables include all individual-level determinants of fertility identified in the demographic and economic literature. Yet the lack of data on knowledge and use of contraception makes it impossible to decompose fertility into desired and undesired components. We include measures of educational attainment and women’s employment in the same regressions as we expect both variables to have a specific impact on fertility rates.
Different model specifications are estimated to account for the potential heterogeneous effects of child mortality on both TF and NF.Footnote 8 Model 1 aims to capture the global effect of child mortality on the two dependent variables. For that purpose, child mortality is included as a binary variable for having experienced a child death. The level effect of child mortality is analyzed in Model 2 and Model 3. In Model 2, the child mortality variable stratifies the sample into four mutually exclusive groups according to the total number of child deaths per woman during her reproductive life (namely, 0, 1, 2 and 3 or more). Model 3 attempts to improve the estimation of the effect of child mortality by using fractional polynomial transformations of the variable in levels. Several models are fitted and compared using a set of fractional polynomial terms. The model with the lowest deviance, defined as twice the negative log likelihood, is finally chosen (see Royston and Sauerbrei 2008, for further methodological information). This allows us to capture the potential non-linear nature of the relationship between fertility and child mortality. More specifically, the marginal effects on fertility of an increase in child mortality levels will be allowed to vary across the distribution of child mortality. As already mentioned in the second section of this paper, there are only few studies examining the effect of child mortality on fertility that use count data models. Moreover, fertility is generally specified as a linear function of child mortality among these studies. Such linear restriction is likely to lead to a misspecification of the underlying relationship, especially when there is a priori no reason to expect a linear relationship. Loken et al. (2012) provide methodological support for the necessity of relaxing the linearity assumption when one wants to thoroughly investigate a certain relationship. Finally, Model 4 and Model 5 investigate the rate effect of child mortality, calculated at the individual level (namely, the number of child losses divided by the dependent variable). When child mortality is expressed in levels, an offset is likely to occur due to the mechanical link between the number of child losses and the number of pregnancies. In turn, estimates of regression coefficients may be artificially inflated. This potential issue is avoided here by using the rate of child mortality. Such a formulation allows us to properly establish the behavioral link between child mortality and fertility, and thus to capture the net effect of child mortality. The variable is categorical in Model 4, with four categories: women with a child mortality rate equals to 0, between 0 and 0.2, 0.2 and 0.3, and higher than 0.3. Fractional polynomial transformations of child mortality rate are used in Model 5. All other explanatory variables remain unmodified across all specifications.
5 Results
Regression results are presented in Table 2. Coefficients are to be interpreted as incidence rate ratios (IRR). Figure 1 shows that both TF and NF are well predicted by the model, as the difference between observed and predicted probabilities lies in a small interval (−0.5; 0.5). The goodness-of-fit of the model is also assessed in view of the deviance statistics at the bottom of Table 2. Figure 2 focuses on the relationship between child mortality and fertility and shows that average predicted counts given all values of child mortality are accurately estimated.

Observed and predicted probabilities from Model 5 for each value of the two dependent variables

Average predicted values versus average observations given all values of child mortality from Model 3 and Model 5
Covariates other than child mortality are included in the regressions in order to control for their potential influence on completed fertility; yet their analysis is not the main focus of this paper.Footnote 9 Their magnitude and significance hardly change across specifications. We now turn to the analysis of the results regarding the effect of child mortality. Model 1 reports a positive global impact of child mortality on both total and net fertility. More precisely, we find that women who have experienced at least one child death have a total fertility that is 1.39 times higher than women who have not. Such an increase is proved to be larger than the one needed to replace lost lives, as net fertility is also 1.06 times higher. Furthermore, Model 2 seems to indicate that the relationship between fertility and the level of child mortality may be of a non-linear nature. Indeed, women that have experienced three or more child deaths have a TF 1.61 times higher than women who have never lost a child, but the two groups are not significantly different in terms of NF. In order to confirm this result, we analyze the estimates of Model 3, in which fractional polynomial transformations of child mortality level are considered. A graphical analysis is required as it is not possible to interpret the coefficients directly from the regression table. Figure 3a gives the predicted values of TF and NF from Model 3 given all levels of child mortality. Although TF is continuously increasing with the level of child mortality, we clearly see that such an increase is insufficient to compensate for lost lives when child mortality levels are very high. Women exhibiting the highest NF are those who have experienced relatively low levels of child mortality (that is, one child loss). Model 4 and Model 5 are similar to Model 2 and Model 3 in all respects except that child mortality is expressed in rates (calculated at the individual level). The results remain unchanged, as shown in Fig. 3b.

Predicted values of total and net fertility given child mortality. a Model 3, b Model 5
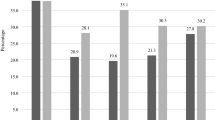
To gain more understanding about the child mortality-fertility relationship, we also investigate whether the mortality effect changes over time. Time effect is likely to capture the contextual (exogenous) development and spread of medical technology. The interaction of child mortality with the mother’s birth cohort is thus included in Model 1.Footnote 10 Figure 4 displays the average marginal effects of child mortality on total and net fertility for the different cohorts. A downward inter-cohort trend is observed, that is, the positive effect of child mortality on total fertility is decreasing for recent cohorts. The mortality effect on net fertility is even slightly negative for the 1947–1951 cohort. More specifically, mothers from the 1932–1936 cohort who experienced at least one child death have 4.13 more pregnancies (and 2.41 more survivors) than women from the same cohort who have not lost a child. For the 1957–1961 cohort, these figures fall to 1.83 more pregnancies and 0.13 more survivors. Mortality is hence likely to have a smaller impact on the fertility of more recent cohorts. With the exception of two distinct mortality peaks that occurred in 1985 and 1998–1999 due to cholera and meningitis outbreaks, infant and child mortality rates have been continuously declining in Niakhar since the 1960s (Delaunay et al. 2001). This could explain the slight rebound in the mortality effect for the last two cohorts, as only women from these cohorts were still in their childbearing years at the time of the mortality outbreaks.

Average marginal effect of child mortality by birth cohort
Finally, we also investigate interaction of child mortality with maternal age, as the effect of child mortality on total and net fertility might change depending on the mother’s entry into reproductive life. For that purpose, interaction of child mortality with the mother’s age at first birth is included in Model 1.Footnote 11 Predicted values and marginal effects are shown in Fig. 5. We see that the positive effect of child mortality on total fertility is likely to decrease with the mother’s age at first birth. Women who had their first delivery at the age of 15 years (49 years) and who experienced at least one child death have 1.90 (1.31) more pregnancies than women who have not lost a child. The positive mortality effect on net fertility—although quite small—also decreases with maternal age. Mothers who have lost a child and started childbearing at the age of 15 years (49 years) have 0.32 (0.18) more survivors than women who have not lost a child.

Effect of child mortality on total and net fertility given mother’s age at first birth
6 Discussion
Fundamentally, this study highlights the role that under five mortality plays in determining changes in households fertility behavior. Coefficient estimates for child mortality are overwhelmingly significant and robust across specifications. The positive association between total fertility and child mortality is exhibited, in line with other empirical studies in the economic and demographic literature.Footnote 12 Looking at the global effect of child mortality, this positive association holds for both total and net fertility, as women who have experienced at least one child death have a total and net fertility being, respectively, 1.39 and 1.06 times higher than women who have not. In turn, a precautionary demand for children arises, giving support for the child survival hypothesis rather than for the replacement hypothesis. Such a statement is also supported by the fact that, as mentioned earlier, one-to-one replacement has never been exhibited in dynamic models of fertility. To our knowledge, this is the first paper providing evidence for the child survival hypothesis at the micro level.
Further understanding is gained by examining more thoroughly the child mortality-fertility link. We show that the relationship is of non-linear nature, as the amplitude and the direction of the effect of child mortality vary with the number of child losses. These results are robust to changes in econometric specifications, and hold true when both level and rate effects of child mortality are accounted for. More specifically, an inverted-U shaped relationship between child mortality and net fertility is exhibited. Mothers with the largest number of survivors are those for whom the burden of child mortality has not been particularly high. An insurance mechanism is thus at work for non-zero but relatively low values of child mortality. As mothers who have lost only one child represent the largest share of mothers who have experienced child mortality, the global effect of child mortality on net fertility has been found to be positive. When child mortality further increases and reaches dramatic values, fertility do not respond anymore to compensate for child losses, so that net fertility falls under the level where any child dies at all. The explanation for this slowing may seem obvious when child mortality is expressed in levels, as there are biological limitations on the number of pregnancies a woman can experience. In order to circumvent the mechanical link between the number of child losses and the number of pregnancies, we also consider the rate of child mortality (calculated at the individual level). Then the behavioral link between child mortality and fertility is properly established. A negative child mortality–fertility relationship is documented for high child mortality rates, holding for both total and net fertility. There is a gap of two pregnancies between women who have never lost a child and those who have lost all of them, and their mean total fertility is around 4.5 and 2.5 respectively. This implies that women who have lost a large proportion of their children were less engaged in childbearing than other women.
In addition, our results provide evidence of a downward trend in the positive effect of child mortality on total and net fertility with time. This offers hope for the diffusion of the fertility transition in the region. The mortality effect also interacts with the timing of the onset of childbearing. We find that the positive effect of child mortality on total and net fertility is likely to decrease with the mother’s age at first birth. The postponement of the onset of childbearing is thus likely to have a direct negative impact on fertility, as well as an indirect negative one through the child mortality channel. This gives support to family planning policies that aim to delay the onset of childbearing in developing countries.
This study helps to explain why fertility rates in SSA are not decreasing as traditional demographic transition theories would have expected. Indeed, the decrease in child mortality rates has not been steeper enough to really influence fertility behaviors. Therefore, we argue that any policy that aims to bring about the diffusion of the fertility transition in SSA should include, along with traditional family planning programs, measures to thoroughly reduce child mortality. And it is worth noticing that rapid progress in child survival is possible, for instance through targeted interventions (Bhutta et al. 2010).
Notes
See for instance Sachs and Malaney (2002) for a review of the (potential) indirect demographic effects of malaria control policies.
Contrastingly, the decline of infant and child mortality that have preceded the demographic transition in Europe and the rest of the industrialized world has been faster and sharper on average (Corsini and Viazzo 1997).
Winkelmann (2008) provides a review of the applications of count data models in the analysis of individual fertility with an emphasis on methodological issues.
Concerns may be raised about the measurement of child mortality in Nguyen-Dinh (1997) as it is assumed that all children ever born were still alive at the time of the survey. Child mortality may thus be underreported.
Niakhar HDSS has originally been set up and is still maintained by the Institut de Recherche pour le Développement (IRD).
Although the causal link from child mortality to fertility is more tenuous, part of the correlation may be due to increased mortality due to higher fertility. Greater family size may adversely affect household constraints such as nutrition and childcare. In their systematic review of the literature on the effect of the number of births on women’s mortality, Hurt et al. (2006) do not find any negative effect of parity on mortality. And this is also true within our study area, as documented in Ronsmans et al. (2001). We argue that the direct effect of fertility on child mortality is likely to be negligible compared to the opposite effect. Endogeneity might still be a concern due to potential omitted variable bias. In addition to the inclusion of all individual-level determinants of fertility, we also include time effects in the model in order to circumvent the problem of omitted variables. Time effects are meant to capture unobserved factors common to all individuals in the sample—in particular the contextual (exogenous) development and spread of medical technology—thereby reducing the main potential source of omitted variable bias. With the impossibility to find legitimate instruments for child mortality, we nonetheless acknowledge the possibility of endogeneity bias due to omitted variables and should still remain cautious in pointing to the existence of a causal link from child mortality to fertility.
The estimated coefficients are consistent with theoretical considerations and other related empirical studies. We find that Muslim and Christian women exhibit higher fertility rates than women having a traditional religion or being atheist. Women married to the household head have a fertility rate that is roughly 1.2 times higher than that of women who are not. Women belonging to less deprived households have lower fertility rates in comparison with extremely deprived ones (that is, deprived in each and every dimension of the calculated index). Women who were maids ended their reproductive life with significantly lower fertility rates than housewives and other active women. The fact that there is no significant difference in fertility rates between housewives and other active women is certainly due to the nature of Niakhar’s economy. Indeed, women reported as housewives dedicate their time to household’s agricultural production activities. The educational achievement of the household head appears to be positively associated with fertility rates (see Diamond et al. 1999 for a review of the complex education-fertility relationship). Concerns may be raised about the use of husbands’ educational attainment—used because of data availability—to tackle the eduction-fertility relationship. However, studies which use data collected from each spouse show that their education level (Cleland and Rodriguez 1988) or fertility desire (McIntosh 1999) have equal influence on fertility decision-making. Finally, mother’s age at first birth has a negative impact on fertility rates.
The table is not presented here but is available from the author upon request.
The table is not presented here but is available from the author upon request.
Although we attempt to address the possibility of omitted variables bias, endogeneity might still be present. We thus remain cautious in arguing for the identification of a causal link from child mortality to fertility.
References
Al-Qudsi, S. S. (1998a). Labour participation of Arab women: Estimates of the fertility to labour supply link. Applied Economics, 30(7), 931–941.
Al-Qudsi, S. S. (1998b). The demand for children in Arab countries: Evidence from panel and count data models. Journal of Population Economics, 11(3), 435–452.
Alkire, S., & Santos, M. E. (2010). Acute multidimensional poverty: A new index for developing countries. Oxford Poverty and Human Development Initiative, Working Paper 38.
Angeles, L. (2010). Demographic transitions: Analyzing the effects of mortality on fertility. Journal of Population Economics, 23(1), 99–120.
Atella, V., & Rosati, F. C. (2000). Uncertainty about children’s survival and fertility: A test using Indian microdata. Journal of Population Economics, 13(2), 263–278.
Balakrishnan, T. R. (1978). Effects of child mortality on subsequent fertility of women in some rural and semi-urban areas of certain Latin American countries. Population Studies, 32(1), 135–145.
Becker, G. S., & Barro, R. J. (1988). A reformulation of the economic theory of fertility. Quarterly Journal of Economics, 103(1), 1–25.
Becker, G. S., & Lewis, H. G. (1973). On the interaction between the quantity and quality of children. Journal of Political Economy, 81(2), S279–S288.
Becker, G. S., & Tomes, N. (1976). Child endowments and the quantity and quality of children. Journal of Political Economy, 84(4), S143–S162.
Bhutta, Z. A., Chopra, M., Axelson, H., Berman, P., Boerma, T., Bryce, J., et al. (2010). Countdown to 2015 decade report (2000–10): Taking stock of maternal, newborn, and child survival. Lancet, 375(9730), 2032–2044.
Bongaarts, J. (2011). Can family planning programs reduce high desired family size in sub-Saharan Africa? International Perspectives on Sexual and Reproductive Health, 37(4), 209–216.
Bongaarts, J., & Casterline, J. (2013). Fertility transition: Is sub-Saharan Africa different? Population and Development Review, 38(s1), 153–168.
Bongaarts, J., Frank, O., & Lesthaeghe, R. (1984). The proximate determinants of fertility in sub-Saharan Africa. Population and Development Review, 10(3), 511–537.
Boucekkine, R., Desbordes, R., & Latzer, H. (2009). How do epidemics induce behavioral changes? Journal of Economic Growth, 14(3), 233–264.
Bulatao, R. A., & Lee, R. (1983). Determinants of fertility in developing countries: A summary of knowledge. New York: Academic Press.
Caudill, S. B., & Mixon, F. G, Jr. (1995). Modeling household fertility decisions: Estimation and testing of censored regression models for count data. Empirical Economics, 20(2), 183–196.
Cleland, J., & Rodriguez, G. (1988). The effect of parental education on marital fertility in developing countries. Population Studies, 42(3), 419–442.
Cleland, J. G., Ndugwa, R. P., & Zulu, E. M. (2011). Family planning in sub-Saharan Africa: Progress or stagnation? Bulletin of the World Health Organization, 89(2), 137–143.
Corsini, C. A., & Viazzo, P. P. (1997). The decline of infant and child mortality: The European experience, 1750–1990. Dordrecht (Boston): Martinus Nijhoff Publishers.
Delaunay, V., Etard, J.-F., Préziosi, M.-P., Marra, A., & Simondon, F. (2001). Decline of infant and child mortality rates in rural Senegal over a 37-year period (1963–1999). International Journal of Epidemiology, 30(6), 1286–1293.
Delaunay, V., Marra, A., Levi, P., & Etard, J. (2002). Niakhar DSS, Senegal. In INDEPTH Network. Populations and health in developing countries, Vol. 1: Population, health and survival at INDEPTH sites (pp. 279–285). Ottawa: IDRC.
Diamond, I., Newby, M., & Varle, S. (1999). Female education and fertility: Examining the links. In: Critical perspectives on schooling and fertility in the developing world (pp. 23–45). Washington, DC: National Academy of Science Press.
Doepke, M. (2005). Child mortality and fertility decline: Does the Barro-Becker model fit the facts? Journal of Population Economics, 18(2), 337–366.
Eckstein, Z., Mira, P., & Wolpin, K. I. (1999). A quantitative analysis of Swedish fertility dynamics: 1751–1990. Review of Economic Dynamics, 2(1), 137–165.
Galor, O. (2005). From stagnation to growth: Unified growth theory. In: Handbook of economic growth (pp. 171–293). Amsterdam: North Holland.
Handa, S. (2000). The impact of education, income, and mortality on fertility in Jamaica. World Development, 28(1), 173–186.
Hossain, M. B., Phillips, J. F., & LeGrand, T. K. (2007). The impact of childhood mortality on fertility in six rural thanas of Bangladesh. Demography, 44(4), 771–784.
Hurt, L. S., Ronsmans, C., & Thomas, S. L. (2006). The effect of number of births on women’s mortality: Systematic review of the evidence for women who have completed their childbearing. Population Studies, 60(1), 55–71.
Kalemli-Ozcan, S. (2003). A stochastic model of mortality, fertility, and human capital investment. Journal of Development Economics, 70(1), 103–118.
Loken, K. V., Mogstad, M., & Wiswall, M. (2012). What linear estimators miss: The effects of family income on child outcomes. American Economic Journal: Applied Economics, 4(2), 1–35.
McCord, G. C., Conley, D., & Sachs, J. D. (2010). Improving empirical estimation of demographic drivers: Fertility, child mortality & malaria ecology. Social Science Research Network Working Paper (July 2010).
McIntosh, J. (1999). An analysis of reproductive behaviour in Canada: Results from an intertemporal optimizing model. Journal of Population Economics, 12(3), 451–461.
Montgomery, M. R., & Cohen, B. (1998). From death to birth: Mortality decline and reproductive change. Washington, DC: National Academies Press.
Nguyen-Dinh, H. (1997). A socioeconomic analysis of the determinants of fertility: The case of Vietnam. Journal of Population Economics, 10(3), 251–271.
O’Hara, D. J. (1975). Microeconomic aspects of the demographic transition. Journal of Political Economy, 83(6), 1203–16.
Olsen, R. J. (1980). Estimating the effect of child mortality on the number of births. Demography, 17(4), 429–443.
Olsen, R. J., & Wolpin, K. I. (1983). The impact of exogenous child mortality on fertility: A waiting time regression with dynamic regressors. Econometrica, 51(3), 731–749.
Ronsmans, C., Khlat, M., Kodio, B., Ba, M., De Bernis, L., & Etard, J. (2001). Evidence for a ‘healthy pregnant woman effect’ in Niakhar, Senegal? International Journal of Epidemiology, 30(3), 467–473.
Rosenzweig, M. R., & Schultz, T. P. (1983). Consumer demand and household production: The relationship between fertility and child mortality. American Economic Review, 73(2), 38–42.
Royston, P., & Sauerbrei, W. (2008). Multivariable model-building: A pragmatic approach to regression anaylsis based on fractional polynomials for modelling continuous variables. New York: Wiley.
Sachs, J., & Malaney, P. (2002). The economic and social burden of malaria. Nature, 415(6872), 680–685.
Sah, R. K. (1991). The effects of child mortality changes on fertility choice and parental welfare. Journal of Political Economy, 99(3), 582–606.
Santos Silva, J., & Covas, F. (2000). A modified hurdle model for completed fertility. Journal of Population Economics, 13(2), 173–188.
Schultz, T. P. (1997). Demand for children in low income countries. In: Handbook of population and family economics (Vol. 1, pp. 393–430). Amsterdam: North-Holland.
Taylor, C. E., Newman, J. S., & Kelly, N. U. (1976). The child survival hypothesis. Population Studies, 30(2), 263–278.
United Nations. (2011). World population prospects, the 2010 revision. New York: United Nations, Department of Economic and Social Affairs, Population Division.
United Nations (2012). World mortality report, 2011. New York: United Nations, Population Division: Department of Economic and Social Affairs.
Winkelmann, R. (2008). Econometric analysis of count data (5th ed.). Berlin: Springer.
Winkelmann, R., & Zimmermann, K. F. (1994). Count data models for demographic data. Mathematical Population Studies, 4(3), 205–221.
Acknowledgments
The author would like to thank Yves Arrighi, Raouf Boucekkine, Olivier Chanel, Jean-Baptiste Combes, Valérie Delaunay, Daria Onori, Luis Sagaon Teyssier and Bruno Ventelou for helpful comments and suggestions.
Author information
Authors and Affiliations
Corresponding author
Appendix
Rights and permissions
About this article

Cite this article
Bousmah, MaQ. The effect of child mortality on fertility behaviors is non-linear: new evidence from Senegal. Rev Econ Household 15, 93–113 (2017). https://doi.org/10.1007/s11150-014-9264-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11150-014-9264-7