
Abstract
Purpose
To generate a normative profile for the EQ-5D-5L dimensions, EQ-5D-5L index, and EQ-VAS scores of the general Thai population and to examine the associations between sociodemographic characteristics and their norm-based scores.
Methods
Data from 2019 general Thai samples were employed to estimate the norm-based scores elicited using the Thai EQ-5D-5L value set. Descriptive statistics were used to estimate the norm-based scores stratified by gender and six age bands to obtain the normative profile for the general Thai population. Multivariable logistic and Tobit regression models were used to investigate the relationships between sociodemographic characteristics and EQ-5D-5L dimensions, EQ-5D-5L index, and EQ-VAS scores.
Results
The mean EQ-5D-5L index and EQ-VAS scores were 0.931 and 82.3, respectively. Approximately 88.9% of the participants reported 19 out of 3125 (3%) possible health states. The odds of having problems with mobility was greatest for the sample aged ≥ 65 years and declined with decreasing age. Women, samples with advancing age, and those with a household income of ≤ 10,000 Baht/month and fair and poor health perceptions were more likely to report a lower EQ-5D-5L index. Furthermore, advanced age and fair and poor health perception were significantly associated with lower EQ-VAS scores.
Conclusion
The EQ-5D-5L population norms were established as the benchmark for both EQ-5D-5L index and EQ-VAS scores for the general Thai population. This is expected to support the health service research and inform policymakers on the allocation of limited healthcare resources.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Plain English summary
The EQ-5D-5L is the most commonly used health preference-based instrument for health technology assessment and health-related quality of life measurement worldwide including Thailand. However, a normative profile of the EQ-5D-5L for the reference values is not available for the general Thai population. This study constructed the population norms for the EQ-5D-5L index and EQ-VAS scores stratified by age and sex, and the result indicates that the EQ-5D-5L index and EQ-VAS scores decreased when advancing age and samples with poor health perception. Moreover, variations of the EQ-5D-5L index and EQ-VAS for the ceiling effects and the associations with sociodemographic factors, which deserves further investigation. Findings from this study inspires more research on health-related quality of life measurement for health care research and policy makers.
Introduction
The EQ-5D questionnaire is a generic multi-attribute instrument developed by the EuroQoL group in the 1980s. It is designed to measure the health-related quality of life (HRQoL) levels as humanistic outcomes in a way that can be compared across different types of patients, disease areas, treatments, and in the general population [1, 2]. The EQ-5D is commonly used and applied in various fields of health sciences research such as economic analyses especially for cost-utility analysis (CUA), health population survey, and clinical study [2,3,4,5]. Moreover, this health utility index score can be used to generate a calculation of health metric outcomes in the form of quality-adjusted life-years (QALYs) for CUA as recommended by several health technology assessment guidelines [3, 6,7,8,9].
The original version of the EQ-5D is now referred to as the EQ-5D-3L. It has five dimensions with three levels of health impairments, representing no problem, some/moderate problems, and extreme problems [10]. Nevertheless, the EQ-5D-3L has certain psychometric problems including high ceiling effects and less discriminatory power that can limit its capability to capture any clinical changes in regard to HRQoL levels [11]. To eliminate those problems, a newer version (the EQ-5D-5L) was developed by expanding the number of health impairments from three to five levels for each health dimension, expressed as no problem, slight problem, moderate problem, severe problem, and extreme/unable to perform. In addition, evidence has supported the use of EQ-5D-5L because it has a lower ceiling effect and greater discriminative power than those of the EQ-5D-3L in both patient groups and the general population [12, 13].
Due to the EQ-5D-5L’s promising psychometric properties and applications in both general population and therapeutic areas, population norms have been used as a benchmark for the HRQoL levels of the general population [14]. Furthermore, the population norms for the EQ-5D-5L have been useful for determining the burden of disease by comparing the HRQoL levels of individuals/groups with specific health problems and by identifying high-risk groups with diminished HRQoL levels [14,15,16]. In general, population norms are reported through health utility index scores and the vertical visual analog scale (EQ-VAS) according to age group, gender, and sociodemographic factors (e.g., education, health conditions, and ethnicity).
As for Thailand, it is an upper middle-income country [17] with approximately 66.2 million people. Since the majority of the population is Buddhist (95.3%) [18], it naturally influences the cultures, beliefs, and lifestyles of individuals. The EQ-5D-5L has been widely used to assess health interventions in clinical practice and is strongly recommended by the Thai health technology assessment (HTA) guidelines [19]. Moreover, it is a practical, reliable, valid, and responsive instrument, which has been proven to be a better psychometric measurement than the EQ-5D-3L in both the general Thai population and Thai patients with chronic diseases [13, 20, 21]. Currently, the Thai EQ-5D-5L includes its own value set for calculating the EQ-5D-5L index [22]. However, the Thai population norms for the EQ-5D-5L are non-existent. Therefore, the purpose of this study is to present the scores for both the EQ-5D-5L index, and the EQ-VAS scores based on age group, gender, and sociodemographic factors. Additionally, it examines the relationship between the sociodemographic factors and the components of the EQ-5D-5L descriptive system, the EQ-VAS scores, and the EQ-5D-5L index scores.
Methods
Study design
This study was conducted using the dataset derived from the project of “Psychometric properties comparison between the EQ-5D-5L and EQ-5D-3L in the general Thai population [13].” A cross-sectional survey study was conducted with 1200 individuals recruited from the general Thai population. The interviews were conducted with the samples residing in five provinces across Thailand. Based on a previous general Thai population study [23], four-stage stratified random sampling was employed to select the provinces, districts, sub-districts, and villages for data collection. Each representative province was selected from each of the five Thai regions: North (Chaing-Mai), Northeast (Khon-Kaen), Central (Bangkok), East (Chonburi), and South (Nakhon Sri Thammarat). Furthermore, interviews occurred at several locations covering both city and rural areas within each province. A stratified quota-sampled in proportion to age and gender was employed to select the samples within each location according to the general Thai population structure. These interviews were conducted between July and September 2019.
Data collection
A sample of individuals aged 20–70 years living in both municipality and rural areas were recruited, after which they were asked to complete the questionnaire on their own. However, face-to-face interviews were employed in cases the respondents could not read the questions and answers due to their eyesight problems. Specifically, the interviewers were allowed to read the questions and answers without explaining their meaning to the respondents. Thus, the respondents were able to complete the questionnaire based on their understanding of the questions and answers.
Prior to each interview, the participant information sheet was given to each of the respondents, written informed consent was obtained, and all respondents were informed of their withdrawal rights. Moreover, the data were kept confidential and anonymous.
Each respondent was asked to complete the Thai EQ-5D-5L for both the descriptive system and the EQ-VAS in addition to their demographic information with the interviewers. The demographic information covered the following aspects: gender, age, education level, household income, type of health insurance, health conditions, smoking, and alcohol consumption. The respondent was also asked to rate their general health perception. The official Thai EQ-5D-5L was granted by the EuroQoL group, and ethical approval was obtained from the Burapha University Institutional Review Board (BUU-IRB; 108/2562).
Instrument
The EQ-5D-5L has two sections: a descriptive system and a visual analog scale (EQ-VAS). Its descriptive system consists of five dimensions: (1) Mobility (MO), (2) Self-care (SC), (3) Usual activities (UA), (4) Pain/discomfort (PD), and (5) Anxiety/depression (AD). The EQ-5D-5L’s descriptive responses can be converted to a single score, EQ-5D-5L index, using a national-specific value set. The national-specific value set was developed by using the stated preference data elicited from the general population to provide the weights attached to each level of health dimension, thereby converting the health descriptive responses into a single value ranging from a value ranging from 0 (the worst possible health state or dead) to 1(the best health status or full health) [24,25,26]. Regarding the EQ-VAS, it is the respondent’s self-rated health on a visual analog scale, anchored at 0 for the “worst imaginable health state” and 100 for the “best imaginable health state” to provide the EQ-VAS scores ranging from 0 to 100 [27]. Consequently, two summary scores, health utility index and EQ-VAS, were obtained from the EQ-5D-5L for each respondent.
The health utility index score was computed using the Thai EQ-5D-5L value set. It was developed from 1207 individuals from the general Thai population living in 12 provinces across Thailand using a stratified multi-stage quota sampling technique. According to the EQ-VT protocol, each sample was assigned to provide the values for a given health state using time-trade-off technique for 10 health states and discrete choice experiment (DCE) for seven pairs of health states to elicit the EQ-5D-5L index scores. Consequently, the Thai EQ-5D-5L index scores developed from Hybrid model (TTO and DCE) range from − 0.4212 to 1.00.
The Thai population norms were reported in the form of EQ-5D-5L index scores and EQ-VAS. The self-reported descriptive system was used to compute the EQ-5D-5L index scores by employing the Thai-specific value set developed based on the Hybrid model [22]. In addition, the EQ-VAS was used to report in terms of EQ-VAS scores and index-based scores wherein the EQ-VAS scores divided by 100.
Data analyses
Sociodemographic information was reported for the recruited samples using descriptive statistics, frequencies, percentage to compare with the data of general Thai population in 2019. The population norms, EQ-5D-5L index and EQ-VAS scores, were reported using the mean, standard deviation, median, and interquartile range according to stratified sociodemographic information. Both the EQ-5D-5L index and EQ-VAS scores were analyzed as continuous variables, so univariate analysis was used to analyze the differences in mean EQ-5D-5L index and EQ-VAS scores using independent t-test or ANOVA where appropriate.
Frequencies and percentages were also employed to report the distribution of the responses to each EQ-5D-5L dimension for the whole samples and stratified by the predefined age groups (< 25, 25–34, 35–44, 45–54, 55–64, ≥ 65), and the top 10 most frequently self-rated health states.
Multivariable logistic regression was used to investigate the association between the sociodemographic variables and the reported problems in each EQ-5D-5L dimension, where the responses for the EQ-5D-5L dimensions were recorded as dummy variables (0 for “no problem” and 1 for “slight,” “moderate,” “severe,” and “extreme/unable to perform”). Due to the ceiling effects of the two population norms, multivariable Tobit regression models were also employed to individually examine the association between the sociodemographic variables and the EQ-5D-5L index and EQ-VAS scores [28]. All of the data analyses were performed using IBM SPSS version 23 (IBM Corporation, Armonk, NY, USA) and STATA version 17.0 (StataCorp LLC, College Station, TX, USA), with the p < 0.05 was designated as statistical difference.
Results
Sample characteristics
Table 1 shows the sample characteristics and a comparison of the structure of the general Thai populaion. The majority of the sample was female (53.3%) and the mean age was 42.7 years (SD = 13.7). Other demographic information is presented in Table 1. Compared to the general Thai population in 2019, the sample had similar characteristic distributions, including gender, age, residence of origin, and certain medical illnesses. The sample characteristics of this study were also similar to those of a previous Thai valuation study in terms of gender and average age. However, the sample in the former had a lower education level (College/University) and higher household income than the sample in the latter. Moreover, according to age and gender, the sample in this study had a similar structure to the general Thai population, especially for the 25–34, 35–44, 45–54, and ≥ 65 age groups (Supplementary Table 1).
Responses distribution to EQ-5D-5L dimensions
Table 2 shows the most frequent self-reported EQ-5D-5L health states. Of the 3125 possible health states, 94 (3%) health states were reported by the Thai samples. Moreover, 19 health states were mainly reported by the majority of the Thai sample (88.9%), and 12 health states mainly settled around level 1 (no problem) and level 2 (slight problem), while the level 5 (extreme problem/unable to perform) of any dimensions was unrelated to these 19 health states. As shown in Table 2, the respondents reported five most health states as follows: 11111 (n = 589, 49.1%), 11121 (n = 166, 13.8%), 21121 (n = 47, 3.9%), 11112 (n = 43, 3.6%) and 11122 (n = 42, 3.5%) yielding EQ-5D-5L index scores of 1.000, 0.9436, 0.8775, 0.9419, and 0.8855, respectively. Notably, 49.1% of the samples responding to health states of 11111 were regarded as the ceiling effects of this study, while no floor effects were observed.
Table 3 also presents the responses to the EQ-5D-5L dimensions regarding the numbers and percentages across six age groups. The highest percentage of respondents reporting any problems (level 2–5) in PD (42.2%), were followed by MO (22.9%), AD (19.8%), UA (11.3%) and, with the lowest percentage, SC (2.5%) dimensions. The samples were more likely to report any problems with increasing age, and the sample group of ≥ 65 years had the highest proportions of reporting any problems for most of the EQ-5D-5L dimensions except for the UA dimension. Among the younger age groups (age < 25 and age 25–35), the youngest (age < 25) experienced greater problems in the dimensions of UA, PD, and AD than their counterparts; however, their proportions were still lower than those in the older age bands. In addition, Supplementary Table 2 shows that the females in the six age groups were more likely to report problems in the five dimensions compared to the males in the groups. This resulted in lower EQ-5D-5L index and EQ-VAS scores (Supplementary Table 3).
EQ-5D-5L index and EQ-VAS scores for the general Thai population
Table 4 conveys the descriptive statistics of the EQ-5D-5L index and EQ-VAS scores stratified by sociodemographic variables. The mean EQ-5D-5L index, using the EQ-5D-5L Thai value set, for the general Thai population was 0.931 (SD 0.101), with values ranging from 0.2285 to 1.000. The univariate analysis showed that mean EQ-5D-5L index and EQ-VAS scores generally decreased among females and older samples (p < 0.05). In addition, both the EQ-5D-5L index and EQ-VAS scores could be affected by other sociodemographic factors, including marital status, education level, health insurance, average household income, general health perception, self-reported health conditions, smoking status, and alcohol consumption because those scores differed across subgroups of sociodemographic factors (p < 0.05).
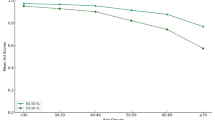
Table 5 depicts the EQ-5D-5L index and EQ-VAS scores individually estimated by gender with some additional stratifications of the six age groups and general health perceptions. Males had a higher mean EQ-5D-5L index and EQ-VAS than females across age groups, and both genders had consistently diminished mean EQ-5D-5L index and EQ-VAS scores when decreasing general health perception.
Association between sociodemographic characteristics and EQ-5D-5L descriptive system, EQ-5D-5L index, and EQ-VAS scores
Table 6 presents the results of the logistic regression models for the association between the sociodemographic characteristics and the reported problems for each EQ-5D-5L dimension. Specifically, females reported more problems in MO, PD, and AD (OR 1.811; 95% confidence interval [CI] 1.218 to 2.694, OR 1.744; 95% CI 1.264 to 2.406, and OR 1.512; 95% CI 1.028 to 2.223, respectively). Regarding the age groups, the sample aged ≥ 35 years had higher odds of MO problems (OR 8.038, 95% CI 2.739 to 22.589) than the sample aged < 25 years, whereas the highest odds were observed in the sample aged ≥ 65 years (OR 32.563, 95% CI 10.245 to 103.499). Similarly, the sample aged ≥ 55 years had higher odds of PD than the sample aged < 25 years (OR 1.852, 95% CI 1.119 to 3.066), whereas the highest odds were detected in the sample aged ≥ 65 years (OR 3.511, 95% CI 1.742 to 7.075). Furthermore, only the sample aged 55–64 years had higher odds of UA problems than the sample aged < 25 years (OR 3.195, 95% CI 1.334 to 7.654). Notably, the odds of reporting problems in SC could not be computed because there were no reporting any problems in the SC dimension for some age groups.
Compared with the “fair” and “poor” health perception groups, the lowest odds of reporting problems with UA occurred in the “excellent” health perception group (OR 0.046, 95% CI 0.006 to 0.355). Similar to UA, the odds of problems with SC for the “very good” health perception group were 0.158 (95% CI 0.031 to 0.801) times lower than those of the “fair” and “poor” health perception groups. Meanwhile, the “excellent” health perception group reported the lowest problems of AD (OR 0.019, 95% CI 0.003 to 0.147). However, the highest odds ratio was found in the “good” health perception group (OR 0.369, 95% CI 0.250 to 0.544). Notably, the odds of certain dimensions could not be computed because there were no reporting problems for some health perception groups.
Table 6 also shows the association between the selected sociodemographic characteristics and the EQ-5D-5L index and EQ-VAS scores based on the multivariable Tobit regression models. According to the results of the EQ-5D-5L dimensions, gender, age, and general health perceptions can affect the EQ-5D-5L index, after adjusting for demographic factors. Specifically, females had a lower mean EQ-5D-5L index than males (− 0.042, 95% CI − 0.063 to − 0.020). Compared with the sample aged < 25 years, the older age groups (except for the 25–34 age group) had a lower mean EQ-5D-5L index where the greatest difference was found in the oldest age group (≥ 65 years). Meanwhile, the groups that reported the “excellent,” “very good,” and “good” health perceptions had a higher mean EQ-5D-5L index (0.252, 95% CI 0.198 to 0.307; 0.195, 95% CI 0.166 to 0.225; and 0.120, 95% CI 0.095 to 0.145, respectively) than those that reported the “fair” and “poor” health perceptions. Moreover, the mean EQ-5D-5L index of the samples with a monthly household income of 10,001 to 50,000 baht was higher than that of the ≤ 10,000 baht/month group (0.019, 95% CI 0.001 to 0.038), except for the mean of the ≥ 50,001 baht/month group.
Overall, the results indicate that age and general health perceptions were two significant factors that affected the EQ-VAS scores. Consistent with the EQ-5D-5L index, the sample aged ≥ 55 years had lower mean EQ-VAS scores than the sample aged < 25 years, except for the 25–54 age group, where the greatest difference was 3.809 (95% CI − 7.577 to − 0.041) for the sample aged ≥ 65 years. Furthermore, the groups with the “excellent,” “very good,” and “good” health perceptions had higher mean EQ-VAS scores (23.393, 95% CI 19.492 to 27.293; 16.955, 95% CI 14.476 to 19.434; and 10.555, 95% CI 8.366 to 12.744, respectively) than those with “fair” and “poor” health perceptions.
Discussion
This study revealed that the mean EQ-5D-5L index for the general Thai population was 0.931; this value is close to the mean EQ-5D-5L index for general populations of various other middle-income countries, including China (0.957) [29], Indonesia (0.911) [30], Iran (0.79) [31], and Vietnam (0.91) [32].
Approximately half of the participants (49.1%) reported “no problems” in all five dimensions of the EQ-5D-5L, known as the “ceiling effect.” This also aligns with the findings from other population norms studies in Indonesia (44.07%) [30] and China (54%) [29]. However, it contradicts a previous Thai valuation study [22] which reported a lower ceiling effect (30.32%) than that of the present study. A possible explanation could be that the previous study was conducted with a sample from wider age range (≥ 18 years) than that in the present study (20–70 years), with the majority reporting themselves as healthy (70.3%), thus resulting in higher ceiling effects.
Similar to previous population norms studies [33,34,35,36], the results showed that the highest percentage of participants reporting “no problem” for each EQ-5D-5L dimension was SC (97.5%), followed by UA (88.8%), AD (80.2%), MO (77.1%), and PD (57.8%). Unlike a previous Thai valuation study [22], it showed that the pattern was dissimilar, with a lower percentage reporting “no problem” for all five dimensions: SC (96.35%), UA (78.87%), MO (72.33%), AD (68.19%), and PD (47.31%). Again, a possible explanation is that the previous Thai valuation study was conducted with a wider age range (≥ 18 years) than that in the present study (20–70 years). Furthermore, the older participants reported more problems with AD than the younger participants, and the proportions of reporting problems declined with decreasing age. This pattern was similar to the results of previous research with the general population in Vietnam [32], whereas it was in contradiction with those of previous research in China [29]. Hence, certain sociodemographic variations seem to impose more varied health perceptions for the EQ-5D-5L dimensions across countries.
As for the regression results, they showed that the EQ-5D-5L index consistently decreased with increasing age, except for the 25–34 age group. This pattern was also found in previous population norms studies in Iran [31] and Vietnam [32], although their age groups somewhat overlapped with those in the present study. Additionally, females reported slightly diminished EQ-5D-5L index scores, compared to males, which is a common finding in previous population norms studies [30,31,32]. Similar to previous research [14, 37], there were higher EQ-5D-5L index scores for the respondents with the “excellent,” “very good,” and “good” health perceptions than those with the “poor” and “fair” health perceptions.
Furthermore, certain variations between the EQ-5D-5L index and EQ-VAS scores were found regarding the ceiling effects and the association with sociodemographic factors. Specifically, the ceiling effect of the EQ-VAS scores was only 12.6%, which was lower than that of the EQ-5D-5L index. Evidently, the participants rating 11111 for the EQ-5D-5L descriptive system achieved a mean value of 86.61 on the EQ-VAS. This aligns with the findings of research in Vietnam [32]. The multivariate analysis also suggested that the association between the EQ-VAS scores and the sociodemographic information aligned with those of the EQ-5D-5L index. The exception was gender and household income factors, which aligns with previous research [29]. Based on these findings, the EQ-VAS could have conceptually measured some aspects beyond the EQ-5D-5L descriptive system, which requires further investigation.
This study includes several limitations that should be noted. First, sampling bias was possible because the participants were selected in proportion to age and gender by the local village leaders. Second, the samples aged < 20 and > 70 years were excluded because this study was part of a psychometric testing project between the EQ-5D-3L and EQ-5D-5L in the general Thai population. Since there was a sensitive question in relation to sexual behaviors from the WHOQOL-BREF, the ethical committee was aware of obtaining the invalidated information from these age groups. Consequently, EQ-5D-5L population norms should be further investigated with a wider sample to better represent the general Thai population. Third, since this study recruited mostly healthy individuals, the EQ-5D-5L index and EQ-VAS scores might be underestimated for those with severe health problems/conditions. Fourth, since the individuals were selected based on age and gender from the general Thai population, other characteristics might be over or under proportioned. Moreover, in terms of age and gender, the sample in this study was similar to the general Thai sample for some age groups. Thus, future population norms studies should recruit a wider sample of individuals to better represent the general Thai population. Fifth, this study was conducted with only 1200 individuals, which is a relatively small sample size, compared to the majority of population norms studies. This was due to the limited budget from the funding agency. Therefore, future research should be conducted with a larger sample size to better represent the general Thai population. Finally, this study selected the samples based on their ability to quickly facilitate the data collection process which could lead to recruit more healthy samples.
Conclusion
The first general Thai population norms for the EQ-5D-5L index elicited from the Thai-specific EQ-5D-5L value set was established. Despite disparities between the EQ-5D-5L index and EQ-VAS scores across sociodemographic factors, age, and general health perceptions significantly affected both scores. Therefore, this study provides the EQ-5D-5L index and EQ-VAS norms for the general Thai population as the benchmark to support health service research and inform policymakers on better allocation of the limited health care resources to those with diminished population norm-based scores.
Data availability
The data analyzed and reported in this manuscript is not available for public sharing because all raw data should be kept it with researcher for privacy in order to comply with the ethical standard.
References
Brooks, R. (1996). EuroQol: The current state of play. Health Policy, 37(1), 53–72.
Devlin, N., Parkin, D., & Janssen, B. (2020). An introduction to EQ-5D instruments and their applications. In N. Devlin, D. Parkin, & B. Janssen (Eds.), Methods for analysing and reporting EQ-5D Data (pp. 1–22). Springer.
Kennedy-Martin, M., Slaap, B., Herdman, M., van Reenen, M., Kennedy-Martin, T., Greiner, W., et al. (2020). Which multi-attribute utility instruments are recommended for use in cost-utility analysis? A review of national health technology assessment (HTA) guidelines. The European Journal of Health Economics, 2, 8. https://doi.org/10.1007/s10198-020-01195-8
Nordlund, A., Ekberg, K., & Kristenson, M. (2005). EQ-5D in a general population survey—A description of the most commonly reported EQ-5D health states using the SF-36. Quality of Life Research, 14(4), 1099–1109. https://doi.org/10.1007/s11136-11004-13062-11132
Martí-Pastor, M., Pont, A., Ávila, M., Garin, O., Vilagut, G., Forero, C. G., et al. (2018). Head-to-head comparison between the EQ-5D-5L and the EQ-5D-3L in general population health surveys. Population Health Metrics, 16(1), 14. https://doi.org/10.1186/s12963-018-0170-8
Sassi, F. (2006). Calculating QALYs, comparing QALY and DALY calculations. Health Policy and Planning, 21(5), 402–408. https://doi.org/10.1093/heapol/czl018
Rawlins, M. D., & Culyer, A. J. (2004). National Institute for Clinical Excellence and its value judgments. BMJ, 329(7459), 224–227. https://doi.org/10.1136/bmj.1329.7459.1224
Weinstein, M. C., Siegel, J. E., Gold, M. R., Kamlet, M. S., & Russell, L. B. (1996). Recommendations of the panel on cost-effectiveness in health and medicine. JAMA, 276(15), 1253–1258.
Rencz, F., Gulácsi, L., Drummond, M., Golicki, D., Prevolnik Rupel, V., Simon, J., et al. (2016). EQ-5D in Central and Eastern Europe: 2000–2015. Quality of Life Research, 25(11), 2693–2710. https://doi.org/10.1007/s11136-016-1375-6
Devlin, N. J., & Brooks, R. (2017). EQ-5D and the EuroQol group: Past, present and future. Applied Health Economics and Health Policy, 15(2), 127–137. https://doi.org/10.1007/s40258-017-0310-5
Herdman, M., Gudex, C., Lloyd, A., Janssen, M. F., Kind, P., Parkin, D., et al. (2011). Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research, 20(10), 1727–1736. https://doi.org/10.1007/s11136-011-9903-x
Buchholz, I., Janssen, M. F., Kohlmann, T., & Feng, Y. S. (2018). A systematic review of studies comparing the measurement properties of the three-level and five-level versions of the EQ-5D. PharmacoEconomics, 36(6), 645–661. https://doi.org/10.1007/s40273-40018-40642-40275
Kangwanrattanakul, K., & Parmontree, P. (2020). Psychometric properties comparison between EQ-5D-5L and EQ-5D-3L in the general Thai population. Quality of Life Research, 29(12), 3407–3417. https://doi.org/10.1007/s11136-020-02595-2
Jiang, R., Janssen, M. F. B., & Pickard, A. S. (2021). US population norms for the EQ-5D-5L and comparison of norms from face-to-face and online samples. Quality of Life Research, 30(3), 803–816. https://doi.org/10.1007/s11136-020-02650-y
Garratt, A. M., Hansen, T. M., Augestad, L. A., Rand, K., & Stavem, K. (2022). Norwegian population norms for the EQ-5D-5L: Results from a general population survey. Quality of Life Research, 31(2), 517–526. https://doi.org/10.1007/s11136-021-02938-7
Jensen, M. B., Jensen, C. E., Gudex, C., Pedersen, K. M., Sørensen, S. S., & Ehlers, L. H. (2021). Danish population health measured by the EQ-5D-5L. Scandinavian Journal of Public Health. https://doi.org/10.1177/14034948211058060
The World Bank. (2021). GNI per capita, Atlas method (current US$). Retrieved March 14, 2023, from https://data.worldbank.org/indicator/NY.GNP.PCAP.CD.
National Statistical Office. (2021). Retrieved November 30, 2022, from http://statbbi.nso.go.th/staticreport/page/sector/en/index.aspx. 2022.
Tavorncharoensap, M., & Sakthong, P. (2019). Health utility. In S. Pannarunothai, S. Pilasant, W. Saengsri, & P. Kingkaew (Eds.), The guideline of health technology assessment in Thailand (pp. 77–94). Health Systems Research Institute.
Pattanaphesaj, J., & Thavorncharoensap, M. (2015). Measurement properties of the EQ-5D-5L compared to EQ-5D-3L in the Thai diabetes patients. Health and Quality of Life Outcomes, 13, 14. https://doi.org/10.1186/s12955-014-0203-3
Sakthong, P., Sonsa-Ardjit, N., Sukarnjanaset, P., & Munpan, W. (2015). Psychometric properties of the EQ-5D-5L in Thai patients with chronic diseases. Quality of Life Research, 24(12), 3015–3022. https://doi.org/10.1007/s11136-11015-11038-z
Pattanaphesaj, J., Thavorncharoensap, M., Ramos-Goni, J. M., Tongsiri, S., Ingsrisawang, L., & Teerawattananon, Y. (2018). The EQ-5D-5L valuation study in Thailand. Expert Review of Pharmacoeconomics & Outcomes Research, 18(5), 551–558. https://doi.org/10.1080/14737167.14732018.11494574
Kangwanrattanakul, K., Gross, C. R., Sunantiwat, M., & Thavorncharoensap, M. (2019). Exploration of a cultural-adaptation of the EQ-5D for Thai population: A “bolt-on” experiment. Quality of Life Research, 28(5), 1207–1215. https://doi.org/10.1007/s11136-018-2072-4
Sakthong, P. (2008). Measurement of clinical-effect: Utility. Journal of the Medical Association of Thailand, 91(Suppl 2), S43-52.
Thavorncharoensap, M. (2014). Measurement of utility. Journal of the Medical Association of Thailand, 97(Suppl 5), S43-49.
Devlin, N., Parkin, D., & Janssen, B. (2020). Analysis of EQ-5D values. In N. Devlin, D. Parkin, & B. Janssen (Eds.), Methods for analysing and reporting EQ-5D data (pp. 61–86). Springer.
Oemar, M., & Janssen, B. (2013). EQ-5D-5L User Guide Basic information on how to use the EQ-5D-5L instrument. EuroQol group.
Austin, P. C., Escobar, M., & Kopec, J. A. (2000). The use of the Tobit model for analyzing measures of health status. Quality of Life Research, 9(8), 901–910. https://doi.org/10.1023/a:1008938326604
Yang, Z., Busschbach, J., Liu, G., & Luo, N. (2018). EQ-5D-5L norms for the urban Chinese population in China. Health and Quality of Life Outcomes, 16(1), 210. https://doi.org/10.1186/s12955-018-1036-2
Purba, F. D., Hunfeld, J. A. M., Iskandarsyah, A., Fitriana, T. S., Sadarjoen, S. S., Passchier, J., et al. (2018). Quality of life of the Indonesian general population: Test-retest reliability and population norms of the EQ-5D-5L and WHOQOL-BREF. PLoS ONE, 13(5), e0197098. https://doi.org/10.1371/journal.pone.0197098
Emrani, Z., Akbari Sari, A., Zeraati, H., Olyaeemanesh, A., & Daroudi, R. (2020). Health-related quality of life measured using the EQ-5D-5 L: Population norms for the capital of Iran. Health and Quality of Life Outcomes, 18(1), 108. https://doi.org/10.1186/s12955-020-01365-5
Nguyen, L. H., Tran, B. X., Le, Q. N. H., Tran, T. T., & Latkin, C. A. (2017). Quality of life profile of general Vietnamese population using EQ-5D-5L. Health and Quality of Life Outcomes, 15(1), 199. https://doi.org/10.1186/s12955-017-0771-0
McCaffrey, N., Kaambwa, B., Currow, D. C., & Ratcliffe, J. (2016). Health-related quality of life measured using the EQ-5D-5L: South Australian population norms. Health and Quality of Life Outcomes, 14(1), 133. https://doi.org/10.1186/s12955-016-0537-0
Wong, E. L., Cheung, A. W., Wong, A. Y., Xu, R. H., Ramos-Goñi, J. M., & Rivero-Arias, O. (2019). Normative profile of health-related quality of life for Hong Kong general population using preference-based instrument EQ-5D-5L. Value Health, 22(8), 916–924. https://doi.org/10.1016/j.jval.2019.02.014
Grochtdreis, T., Dams, J., König, H. H., & Konnopka, A. (2019). Health-related quality of life measured with the EQ-5D-5L: Estimation of normative index values based on a representative German population sample and value set. The European Journal of Health Economics, 20(6), 933–944. https://doi.org/10.1007/s10198-019-01054-1
Bailey, H., Janssen, M. F., La Foucade, A., & Kind, P. (2019). EQ-5D-5L population norms and health inequalities for Trinidad and Tobago. PLoS ONE, 14(4), e0214283. https://doi.org/10.1371/journal.pone.0214283
Poder, T. G., Carrier, N., & Kouakou, C. R. C. (2020). Quebec health-related quality-of-life population norms using the EQ-5D-5L: Decomposition by sociodemographic data and health problems. Value Health, 23(2), 251–259. https://doi.org/10.1016/j.jval.2019.08.008
Acknowledgements
The author expresses sincere gratitude to the EuroQoL group for their permission to use the EQ-5D-5L questionnaire in this study, and also thanks all local village leaders and participants from the provinces of Nakhon-Srithammarat, Khon-Kaen, Chonburi, Chaing-Mai, and Bangkok in Thailand who facilitated or participated in the data collection process. Special thanks to all interviewers for their assistance with the data collection process.
Funding
This work was supported by Grants Rx2/2562 from the Burapha University through the National Research Council of Thailand. However, the funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
KK was the only one involved in study conception and design, data collection, data analyses, interpretation, drafting, and final approval of this manuscript.
Corresponding author
Ethics declarations
Competing interests
The author has no relevant financial or non-financial to disclose.
Ethical approval
This work was approved by the Burapha University Institutional Review Board (BUU-IRB): 108/2562 before the study commenced.
Consent to participate
The written consent form was obtained from each study subject before the study commenced; however, they were informed to be able to withdraw from this study at any time if they felt uncomfortable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kangwanrattanakul, K. Normative profile of the EQ-5D-5L dimensions, EQ-5D-5L index and EQ-VAS scores for the general Thai population. Qual Life Res 32, 2489–2502 (2023). https://doi.org/10.1007/s11136-023-03420-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-023-03420-2