
Abstract
Purpose
The purpose of this study was to assess the psychometric properties of the Satisfaction with Life Scale (SWLS), evaluate the measurement invariance with respect to sex, age, and tumor location, as well as analyze associations between life satisfaction and socio-demographic and clinical variables among individuals with resected, non-advanced cancer.
Methods
A confirmatory factor analysis was conducted to explore the dimensionality of the scale and test invariance across gender, age, and tumor localization in a prospective, multicenter cohort of 713 patients who completed the following scales: SWLS, Health-related Quality of Life Questionnaire (EORTC QLQ-C30), Brief Symptom Inventory (BSI-18).
Results
Confirmatory factor analysis results indicated that the SWLS is an essentially unidimensional instrument, providing accurate scores: both McDonald’s omega and Cronbach’s alpha estimates were 0.91. Strong measurement invariance was found to hold across gender, age, and tumor localization. Low satisfaction with life was associated with psychological symptoms (anxiety, depression, and somatization), and decreased quality of life (malfunction, symptoms, poor global QoL).
Conclusion
The SWLS is a reliable, valid satisfaction with life measurement among people with cancer and should be recommended as an indicator of psychological adjustment in oncological patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cancer is a complex, multifarious disease, the incidence of which continues to grow in developed countries, reaching 1.3 million new cases each year in Europe [1]. Treatments have improved over the last decade, leading to a noticeable increase in cancer survivors [2]. Intensive therapies are responsible for these advances, albeit at the expense of formidable side effects (e.g., infertility, heart problems, endocrine dysfunction, post-traumatic stress, or neuropsychological deficits) [3, 4]. Physical and psychological changes, and the decline observed in patients owing to the direct effects of the cancer itself, comorbidities, and treatments result in the need to understand the biopsychosocial impact of the disease and its long-term treatment [2].
The Satisfaction with Life Scale (SWLS) is extensively used to quantify the cognitive component of subjective well-being [5], examining a person’s expectations against their achievements [6]. A recent conceptual paper considered that satisfaction with life is a type of evaluative well-being that, together with hedonic well-being and eudemonic well-being, constitutes a measure of subjective well-being [7].
In studies conducted in the general population, satisfaction with life has been found to be independent of gender [8, 9], level of education, employment status, and social support [10]. Low satisfaction with life has been correlated with having physical (fatigue, physical complaints, insomnia, and low quality of life) and psychological (anxiety and pessimism) problems in the general population [8] and in patients with colorectal cancer [11]. Likewise, it has been linked to socio-demographic factors (not having a partner, low income, and unemployment) both in the general population [8] and in individuals with prostate cancer [12]. Among breast cancer patients, satisfaction with life has been related to having children, being employed, having social and emotional support, and being in good physical and psychological condition [13], as well as actively engaged in shared decision-making [14].
Thus, life satisfaction in individuals with cancer is a relevant quality-of-life indicator [15] and has been used both as an outcome measure, as it relates to recovery from disease, and as an indicator of adaptation to new life conditions [13]. Furthermore, people with cancer display lower levels of satisfaction with life versus those suffering from chronic illness (diabetes, osteoporosis, respiratory failure) [15]. Dissatisfaction with life is related to psychological distress in oncology patients [16] and lower quality of life [17]. Women who had undergone mastectomy and/or breast reconstructive surgery had lower levels of satisfaction and lower quality of life, compared to those who had undergone breast-conserving surgery [17, 18]. A longitudinal study with nearly 2000 colorectal cancer survivors found that less optimism and a higher use of threat appraisals were associated with poorer life satisfaction [11].
We must analyze patients’ satisfaction with life if we are to understand the domains in which they feel a discrepancy between their expectations and achievements and their current health status, as well as the areas in which they may need support. The SWLS, a multi-item questionnaire developed in the United States in 1985, widely used and validated in numerous countries [9, 19,20,21] enables us to do just that. Internal consistency reliability coefficients range from 0.79 to 0.91 [6, 21]. The SWLS has good divergent validity for constructs such as depression, anxiety, and psychological distress [6], and convergent validity with other measures of subjective well-being [22]. The scale’s factorial invariance has aroused interest in recent studies and it is important to be able to compare results across different genders and age groups, amongst others [19, 23,24,25]. Nevertheless, so far as we know, the scale’s psychometric properties and its invariance across oncological patients’ gender, age, tumor type, socio-demographic, and clinical factors have yet to be evaluated.
The aim of this study is to examine the SWLS’s psychometric properties and assess the effect of gender, age, and tumor type, as well as the relation between satisfaction with life and variables of clinical relevance and socio-demographic factors in a sample of individuals with cancer initiating adjuvant chemotherapy. A high or moderate correlation between the SWLS and Europe QoL, and psychological scales of BSI is expected for the convergent validity.
Methods
Study populations
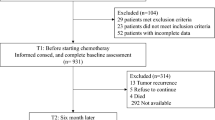
The Neocoping project is a national, multicenter (15 centers), cross-sectional, prospective study of the Continuous Care Group of the Spanish Society of Medical Oncology (SEOM). The protocol was approved by the Ethics committee of each hospital, and by the Spanish Agency for Medicines and Medical Devices (AEMPS); all participants signed informed consent forms prior to inclusion. The population consisted of patients with histologically confirmed, non-advanced cancer treated with surgery for which international clinical guidelines considered that adjuvant treatment could be an option. Subjects were excluded if they were under 18 years of age, had been treated with preoperative radio- or chemotherapy, only hormonal therapy, or adjuvant radiotherapy without chemotherapy, and if they had any serious mental illness that prevented them from understanding the study. Self-report scales were completed by the participants at the beginning of adjuvant treatment. Each questionnaire contained written instructions and specified that participation was voluntary and anonymous. Of the 803 patients screened, 90 were not eligible (17 did not meet inclusion criteria, 33 met exclusion criteria, and 40 had incomplete data).
Instruments
The Satisfaction with Life Scale (SWLS) is a 5-item scale that assesses an individual’s global judgment regarding their life satisfaction [5]. Individuals were asked to indicate their level of agreement with the statements on a seven-point Likert-type scale. Raw scores ranged from 5 to 35, with higher scores indicating greater life satisfaction. We used the Spanish version of the SWLS [19]. The unidimensional structure of the scale has been confirmed in different studies conducted in Spanish populations [9, 10].
The Brief Symptom Inventory (BSI-18) includes 18 symptoms to appraise distress on a five-point scale ranging from ‘not at all’ (0) to ‘extremely (4)’ [26]. The scale provides three groups of symptoms (somatization, depression, and anxiety) and a total score, known as the Global Severity Index (GSI), which compiles the interviewee’s psychological distress. Cronbach’s alpha ranged from 0.81 to 0.90 [26].
The European Organization for Research, and Treatment of Cancer Quality of Life Questionnaire(EORTC QLQ-C30) is widely used in Europe to assess quality of life, and its validity has been well established [27]. Response choices range from 1 (not at all) to 4 (very much), with the exception of the global QoL scale, where responses range from 1 (very poor) to 7 (excellent). All scale scores are linearly transformed to a 0–100 scale. Higher scores on the functioning scales and global QoL scale represent a higher level of functioning or QoL. For the symptom scales, the higher the score, the greater the symptom burden.
Demographic and clinical variables consisted of age, gender, marital status (married/partnered, not partnered), five age groups (≤ 49, 50–59, 60–69, ≥ 70 years), employment status (inactive, active), tumor (colon, breast, others), cancer treatment (chemotherapy, chemotherapy, and radiotherapy), and tumor stage (I–II, III).
Data analysis
Data analysis was performed using a 3-stage approach. First, basic sample and item descriptive statistics were obtained by using SPSS v23, then, confirmatory factor analyses (CFA’s) were performed in two steps. In the preliminary step, the unidimensional FA model assumed for the SWLS items was fitted to the entire patient sample. The second step consisted of evaluating measurement invariance in groups defined by gender, age, and tumor localization. All FA models were fitted using robust maximum likelihood (RML) estimation with second-order (mean and variance) corrections as implemented in Mplus (see [28], Appendix 4). Model fit and appropriateness were assessed with three groups of measures. First, model residuals and relative fit were appraised with the SRMR and RMSEA statistics. Second, relative comparative fit was evaluated with the CFI index (as a relative measure of fit with respect to the null independence model). Finally, in the overall analysis, additional indices of appropriateness to examine the strength and replicability of the solution (H index), as well as closeness to unidimensionality (ECV index), were also obtained by using the FACTOR program [29, 30]. As for reference values, CFI values ≥ 0.95 are indicative of good model fit [31], whereas SRMR values ≤ 0.08 and RMSEA values ≤ 0.06 indicate satisfactory fit [32, 33].
In the factor-analytic framework, the property of measurement invariance (MI) means that, in all the groups to be compared, the instrument which is assessed measures the same dimensions with the same factorial structure (see [34]). In our case, MI would imply that the SWL items (a) conform to the unidimensional model in all the groups to be compared and (b) have the same quality and measurement properties across the groups. Within this general framework, and, as discussed below, there are different levels of MI that can be considered or attained.
As in most clinical studies, the main relevance of MI is that it is a prerequisite for validly interpreting and comparing scores obtained from the instrument under study. Thus, if MI holds, this means that the scores of two individuals belonging to different groups can be validly compared, because eventual differences in these scores univocally reflect ‘true’ differences on the trait that is measured. And the same occurs when mean differences are observed among groups. On the contrary, when MI cannot be demonstrated, valid interpretation of score differences is not warranted. In this case, the observed differences might reflect that the individuals of the different groups interpret the item questions differentially (see [34]) or, even worse, that the instrument measures different dimensions in the different groups.
There is considerable debate surrounding the appropriate level of MI to be recommended for a measurement instrument. The most complete form implies invariance in the item thresholds, loadings, and error variances, and is known in the literature as strict factorial invariance [35]. Strict invariance, however, represents an often unattainable ideal in applied research and is not strictly necessary for the present purposes; moreover, when forced in a solution, it can lead to biased parameter estimates (e.g., [36]). We therefore considered strong or scalar invariance [35] to be a reasonable aim for the SWLS items. Strong invariance implies that both item intercepts and loadings are invariant, and if attained, that any systematic group differences in means and covariances are due to common factors. Furthermore, when measuring individuals from different groups, the measurement scale can be considered to be the same and trait estimates comparable (see [37]). Figure 1 depicts the measurement invariance diagram for the SWL items in the two-group case. Note that in both groups, the same factor (i.e., satisfaction with life) is measured with the same regression parameters (note that the intercepts µ and loadings λ have the same common subscripts in both groups) and only the residual terms or errors are allowed to have different magnitudes in each group (these terms have additional group subscripts).

Satisfaction with Life Scale (SWLS) mean score by marital status and age group
Provided that strong invariance was obtained, the mean differences in groups defined by gender, age, and tumor site were assessed in this second, CFA stage. The reliabilities of the scores derived from the factorial solution were also examined at the end of this stage using Cronbach’s alpha and MacDonald’s Omega.
In the third stage, validity relations were assessed via product-moment correlations between SWLS and EORTC (functional scale, symptom scale, global QoL), and BSI (psychological distress).
Results
Sample characteristics
The study included 713 patients with cancer (57.8% females and 42.2% males), aged 18–75 years (M = 59.3, SD = 12.2), consecutively referred to the Department of Medical Oncology at each hospital, predominantly married or partnered (75.9%), and unemployed (58.2%). The most common tumor site was colon (43.8%) and breast (31.6%), stage I–II (55.5%); all patients received adjuvant chemotherapy and 33.2% also received radiotherapy; see Table 1.
The lowest life satisfaction scores were observed for patients who were unmarried, widowed, or divorced (M = 24.6), who presented marginally lower values than those who were married or partnered (M = 27.8; F = 39.458 p < 0.001; η2 = 0.05), and for young people (F = 3.999, p = 0.008; η2 = 0.02). The lowest satisfaction scores were found for people aged < 49 years (M = 25.9) compared to those aged 60–69 years (I–J = − 1.70, p = 0.036), and ≥ 70 years (I–J = − 1.92, p = 0.019); see Table 1.
Descriptive statistics for SWLS items
Descriptive statistics of the five items of the SWLS are presented in Table 2. The mean score obtained was 27.1 (SD = 5.9) and all five items exhibited very similar means, 5.10–5.78 on the 1–7 scale. SWLS item score distributions were unimodal and asymmetrical (negatively skewed), thereby indicating that most of the values were concentrated at the highest end of the response scale. All the corrected item-total correlations surpassed 0.66. Provided that the scale behaves unidimensionally, this last result indicates that the items have adequate discriminating power and are strongly related to the construct they measure.
Confirmatory factor analysis and measurement invariance
Because (a) response variables are ordered-categorical, (b) item distributions are negatively skewed, and (c) item discriminating power is relatively high, the most ‘a priori’ appropriate factor analysis procedure for the SWLS items is the underlying-variables approach (UVA), fitting the FA model to the inter-item polychoric correlation matrix (more details in [38]). However, the number of scale response points is relatively high and we found that the results of fitting the UVA-based model and the standard linear FA model were virtually the same. Given this result, plus the fact that applying the linear model considerably simplifies assessment of the measurement invariance, we opted to use the linear approach in all the FA analyses that follow.
As described above, the unidimensional FA model was first fitted in the entire sample of 713 respondents. As expected from previous studies, the fit of the unidimensional model was quite acceptable (χ2 = 15.79, df = 5; CFI = 0.99, RMSEA = 0.056, and SRMR = 0.02). The ECV estimate was 0.947, meaning that 94.7% of the common variance of the item scores can be accounted for by the single factor. Finally, the replicability H index was 0.953, indicating not only that the solution is essentially unidimensional, but also that the single factor is strong and replicable [29]. The estimated intercepts obtained by fitting the FA model were essentially the same as the item means given in Table 2. Standardized factor loadings for the five SWLS items are illustrated in Fig. 2.

Standardized estimates of confirmatory factor analysis of the five SWLS items in the entire sample
As for invariance, similar to previous studies [9, 19, 21, 23, 24], strong measurement invariance was attained for both gender and age. Table 3 presents the results of the strong invariance model for gender and age, as well as mean group estimates. As discussed above, the attainment of this MI level allows us to assume that the same construct is measured in the different gender and age groups and that the regression parameters of the SWL items are the same (i.e., invariant) in these groups. Therefore, group mean score differences can be validly interpreted as reflecting ‘true’ group differences in the construct that is measured. With regards to this interpretation, note that the mean satisfaction estimate is lower in Women with a statistically significant difference, given that the fixed 0 estimate in Men falls outside the 95% confidence interval around the Women mean. However, the upper limit of the confidence interval is almost zero and the effect size for mean differences (Cohen’s d) is a mere 0.17. In short, these results suggest that there is a significant difference in satisfaction with life in the direction that said scores are lower in the Women. However, statistical significance is probably due to the power of the test with the large samples employed and the practical significance is likely negligible. This result is consistent with the less powerful raw score-based mean comparisons shown in Table 1, in which statistical significance was still not attained.
As regards age comparisons, the results shown in Table 3 reveal that group 1 (< 49) has significantly lower satisfaction-with-life levels than the remaining groups; again, in line with the raw score-based results shown in Table 1.
The results for groups defined by tumor location are new; consequently, they will be discussed in greater detail. Table 4 provides the sequential assessment results for the nested sub-models going from configural invariance to strong invariance. Given that a second-order correction was used in the robust ML estimation, difference testing was conducted using DIFFTEST [39]. Mean group estimates are provided at the bottom of the table.
Results shown in Table 4 can be summarized as follows. First, the strong invariance submodel has quite an acceptable fit, and, in relative terms (i.e., RMSEA), the fit is better than that of the less restricted configural model. Second, goodness-of-fit does not appear to worsen substantially when going from the configural to the strong model. Strictly speaking, the Chi-square difference test when passing from the weak to the strong model is statistically significant. However, the difference in CFI terms is < 0.01 and < 0.015 in RMSEA terms. Overall, the hypothesis that strong measurement invariance is achieved when grouping by tumor site is quite tenable, which implies that the same valid comparisons that were made for gender and age can be also made here.
Group differences are quite clear: the 0 fixed mean is contained in both confidence intervals and these intervals, in turn, widely overlap. Thus, no significant group mean differences in satisfaction with life emerge.
At the end of this second step, and because the unidimensional structure for the SWLS items was found to be reasonable, the reliability of the scores derived from this structure was assessed. Both reliability estimates (McDonald’s omega and Standardized Cronbach’s alpha) were 0.91.
Convergent validity of the SWLS scores
Low satisfaction with life was associated with anxiety (r = − 0.33), depression (r = − 0.42), somatization (r = − 0.26), functional scale (r = − 0.29), symptom scale (r = 0.25), and decreased global quality of life (r = − 0.32); see Table 5.
Discussion
This is the first study with a large sample of adults with non-metastatic, resected cancer with curative intent to analyze the psychometric properties of the SWLS. In line with other published studies, the scale exhibits high internal consistency, a well-defined, strong unifactorial structure, and achieves strong invariance in terms of gender, age, and tumor location.
The mean SWLS score was 27.1 in this study, slightly above the means obtained in studies in our setting with representative samples of German M = 26.4 [8], Norwegian M = 26.2 2 [21], and Spanish M = 24.1 adult populations [10, 15]. In this last study, half of the participants presented physical and psychological problems, which might account for the lower scores on the scale in comparison with the other studies. Insofar as patients with cancer are concerned, satisfaction with life was also slightly higher in our sample than in people with colorectal cancer who had recently undergone surgery, many of whom received adjuvant therapy, M = 26.4 [40], and well above that of women of child-bearing age with cancer (leukemia, Hodgkin and non-Hodgkin lymphoma, breast cancer, and gastrointestinal cancer), M = 20.0 [41], and women with breast cancer receiving treatment adjuvant, M = 18.4 [42]. We believe that our sample’s age and characteristics might explain these differences. In the last two studies, the mean age was between 40 and 49 years, which coincides with the age range in which our patients also exhibited lower satisfaction with life scores. Our series had a higher mean age, which could be associated with greater satisfaction. As for our group’s clinical status, they had undergone surgery with curative intent for an early-stage cancer. This, despite the fear surrounding the potential risk of recurrence, may have influenced the high score on the Satisfaction with Life Scale. The participants may feel that life has given them a “second chance.”
The reliability (internal consistency) estimates (McDonald ω and Cronbach α = 0.91) were similar to those of other studies: 0.89 [8], 0.91 [21], and 0.88 [10], and there is no item that when eliminated increases the scale’s consistency. Nevertheless, item no. 5 presents less saturation and the item-total correlation is the lowest, similar to other investigations [10, 19]. The results of the invariance study indicate that there is no differential functioning in any of SWLS items and, therefore, that the test’s structure is equivalent in men and women. These results are comparable to those reported by several groups [9, 19, 21], although they contrast with those published regarding a sample of Spanish and Portuguese adolescents, and another sample of Serbian adolescents that found incomplete scaler invariance with the intercept for item 5 [19, 20]. Because the strong invariance hypothesis was found to be plausible, the mean groups could be meaningfully compared. Results indicated a statistically significant difference in the direction that satisfaction with life was lower in women. However, the effect size was very small and the practical significance was probably negligible, although this effect is somewhat greater than those found in other populational studies [8, 21].
Strong invariance was also found to be tenable in the age-defined groups. Our finding is compatible with previous reports [43, 44], although others [9, 45, 46] found that life satisfaction does not have the same meaning across the life span. Multigroup-based comparisons suggested differences between group 1 and the remaining groups (older people reporting higher levels of life satisfaction). Given that satisfaction with life is a judgment between what we expect to obtain and what we have actually achieved [5], older individuals can be expected to score higher, since seniors have been able to satisfy some of their life goals, whereas younger people, by virtue of their age, may still be building their careers, families, and have greater economic responsibilities and can perceive cancer as something outside the usual age- and health-related expectations [11].
As far as tumor site is concerned, strong invariance was also found to be reasonable, this being the first study that analyzes invariance on the basis of tumor. No significant differences were detected between mean levels of satisfaction in the three groups: colon, breast, and others. Along these same lines, Dunn et al. found that half of all patients with cancer reported high levels of satisfaction with life and that the experience of having cancer did not bring them to judge their lives as impaired or less than ideal [11]. This speaks of patients’ ability to maintain a stable sense of satisfaction with life despite their illness [6, 42].
Insofar as patients’ socio-demographic and clinical variables are concerned, results based on direct test scores are as follows. Marital status appears to intervene in the reported levels of satisfaction. Married people or those living with a partner reported greater satisfaction with life than single, divorced, or widowed individuals. Furthermore, the latter were the group exhibiting the lowest score on the scale. Recent studies suggest that positive marital relationships contribute in the process of coping with cancer [47, 48].
As for construct validity, the closest correlations were observed in the negative emotional component of the BSI (anxiety, depression, and somatization). Associations were also found with quality-of-life indicators (functional status, symptoms, and global QoL), although slightly lower than in the emotional component. Many health studies have used the SWLS to gage quality of life in people undergoing medical procedures and/or rehabilitative therapies [8, 11, 13].
The findings of this study have several clinical implications. The SWLS can complement other measures that appraise negative states in oncological patients. As for satisfaction with life, psychosocial interventions that help the patient maintain and enhance their sense of meaning and purpose in life, despite their disease, can aid in their recovery and improve their quality of life, particularly in those who are struggling. It would be interesting in future studies to analyze the relationship between satisfaction and risk of recurrence and their ability to recover, as well as to examine if satisfaction with life remains stable throughout treatment.
Among the study’s limitations, we must point that since the study was designed to include a single satisfaction with life assessment, information regarding causality cannot be examined, nor can we offer an explanation about how satisfaction evolves over time. Second, though we have a large sample, it is possible that those who did not want to participate because they were tired, anguished, or in worse health (n = 66) might have caused the results to vary. Third, specific factors that might account for satisfaction with life such as resilience were not assessed; this is an area for future research. Finally, the possibility exists that the results of our study might not be susceptible to extrapolation to individuals with advanced tumors, whose clinical situation and prognosis differ appreciably.
The strengths of this study include its prospective design, the use of widely validated and reliable measures, the utilization of different scales, and a sizable sample of subjects with non-advanced, resected cancer from different hospitals of all over Spain.
In conclusion, these results add to the growing body of knowledge about the adequate reliability and validity properties of the SWLS and the strong gender, age, and tumor location invariance. These findings are pertinent, as they prove that the SWLS can be used as a complementary measure to evaluate psychological adjustment in individuals with cancer.
References
Ferlay, J., Steliarova-Foucher, E., Lortet-Tieulent, J., Rosso, S., Coebergh, J. W. W., Comber, H., … Bray, F. (2013). Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. European Journal of Cancer, 49(6), 1374–1403. https://doi.org/10.1016/j.ejca.2012.12.027.
Kvale, E. A., Huang, C.-H. S., Meneses, K. M., Demark-Wahnefried, W., Bae, S., Azuero, C. B., … Ritchie, C. S. (2016). Patient-centered support in the survivorship care transition: Outcomes from the patient-owned survivorship care plan intervention. Cancer, 122(20), 3232–3242. https://doi.org/10.1002/cncr.30136.
Ramchand, S. K., Lim, E., & Grossmann, M. (2016). Adjuvant endocrine therapy in women with oestrogen-receptor-positive breast cancer: how should the skeletal and vascular side effects be assessed and managed? Clinical Endocrinology, 85(5), 689–693. https://doi.org/10.1111/cen.13172.
Pendergrass, J. C., Targum, S. D., & Harrison, J. E. (2018). Cognitive impairment associated with cancer: A brief review. Innovations in clinical neuroscience, 15(1–2), 36–44.
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The Satisfaction With Life Scale. Journal of Personality Assessment, 49(1), 71–75. https://doi.org/10.1207/s15327752jpa4901_13.
Pavot, W., & Diener, E. (2008). The Satisfaction With Life Scale and the emerging construct of life satisfaction. The Journal of Positive Psychology, 3(2), 137–152. https://doi.org/10.1080/17439760701756946.
Steptoe, A., Deaton, A., & Stone, A. A. (2015). Subjective wellbeing, health, and ageing. The Lancet, 385(9968), 640–648. https://doi.org/10.1016/S0140-6736(13)61489-0.
Hinz, A., Conrad, I., Schroeter, M. L., Glaesmer, H., Brähler, E., Zenger, M., … Herzberg, P. Y. (2018). Psychometric properties of the Satisfaction with Life Scale (SWLS), derived from a large German community sample. Quality of Life Research, 0(0), 0. https://doi.org/10.1007/s11136-018-1844-1.
Esnaola, I., Benito, M., Antonio-Agirre, I., Freeman, J., & Sarasa, M. (2017). Measurement invariance of the Satisfaction With Life Scale (SWLS) by country, gender and age. Psicothema, 29(4), 596–601. https://doi.org/10.7334/psicothema2016.394.
Vázquez, C., Duque, A., & Hervás, G. (2013). Satisfaction with Life Scale in a representative sample of Spanish adults: Validation and normative data. The Spanish Journal of Psychology, 16, E82. https://doi.org/10.1017/sjp.2013.82.
Dunn, J., Ng, S. K., Breitbart, W., Aitken, J., Youl, P., Baade, P. D., & Chambers, S. K. (2013). Health-related quality of life and life satisfaction in colorectal cancer survivors: Trajectories of adjustment. Health Qual Life Outcomes, 11, 46.
Chambers, S. K., Ng, S. K., Baade, P., Aitken, J. F., Hyde, M. K., Wittert, G., … Dunn, J. (2017). Trajectories of quality of life, life satisfaction, and psychological adjustment after prostate cancer. Psycho-Oncology, 26(10), 1576–1585. https://doi.org/10.1002/pon.4342.
Olsson, M., Nilsson, M., Fugl-Meyer, K., Petersson, L.-M., Wennman-Larsen, A., Kjeldgård, L., & Alexanderson, K. (2017). Life satisfaction of women of working age shortly after breast cancer surgery. Quality of Life Research, 26(3), 673–684. https://doi.org/10.1007/s11136-016-1479-z.
Ashraf, A. A., Colakoglu, S., Nguyen, J. T., Anastasopulos, A. J., Ibrahim, A. M. S., Yueh, J. H., … Lee, B. T. (2013). Patient involvement in the decision-making process improves satisfaction and quality of life in postmastectomy breast reconstruction. Journal of Surgical Research, 184(1), 665–670. https://doi.org/10.1016/j.jss.2013.04.057.
Vázquez, C., Rahona, J. J., Gómez, D., Caballero, F. F., & Hervás, G. (2015). A national representative study of the relative impact of physical and psychological problems on life satisfaction. Journal of Happiness Studies, 16(1), 135–148.
Cipora, E., Konieczny, M., Karwat, I., Roczniak, W., & Babuśka-Roczniak, M. (2018). Satisfaction with life among women with breast cancer: Selected demographic and social factors. Annals of Agricultural and Environmental Medicine. https://doi.org/10.26444/aaem/82622.
He, Z.-Y., Tong, Q., Wu, S.-G., Li, F.-Y., Lin, H.-X., & Guan, X.-X. (2012). A comparison of quality of life and satisfaction of women with early-stage breast cancer treated with breast conserving therapy vs. mastectomy in southern China. Supportive Care in Cancer, 20(10), 2441–2449.
Han, J., Grothuesmann, D., Neises, M., Hille, U., & Hillemanns, P. (2010). Quality of life and satisfaction after breast cancer operation. Archives of Gynecology and Obstetrics, 282(1), 75–82. https://doi.org/10.1007/s00404-009-1302-y.
Atienza, F. L., Balaguer, I., Corte-Real, N., & Fonseca, A. M. (2016). Factorial invariance of the Satisfaction with Life Scale in adolescents from Spain and Portugal. Psicothema, 28(3), 353–358. https://doi.org/10.7334/psicothema2016.1.
Jovanović, V. (2016). The validity of the Satisfaction with Life Scale in adolescents and a comparison with single-item life satisfaction measures: a preliminary study. Quality of Life Research, 25(12), 3173–3180. https://doi.org/10.1007/s11136-016-1331-5.
Clench-Aas, J., Nes, R. B., Dalgard, O. S., & Aarø, L. E. (2011). Dimensionality and measurement invariance in the Satisfaction with Life Scale in Norway. Quality of Life Research, 20(8), 1307–1317. https://doi.org/10.1007/s11136-011-9859-x.
Pavot, W., & Diener, E. (2009). Review of the satisfaction with life scale. In N. Diener (Ed.), Assessing well-being (pp. 101–117). New York: Springer.
Emerson, S. D., Guhn, M., & Gadermann, A. M. (2017). Measurement invariance of the Satisfaction with Life Scale: reviewing three decades of research. Quality of Life Research, 26(9), 2251–2264. https://doi.org/10.1007/s11136-017-1552-2.
Bagherzadeh, M., Loewe, N., Mouawad, R. G., Batista-Foguet, J. M., Araya-Castillo, L., & Thieme, C. (2018). Spanish version of the Satisfaction with Life Scale: Validation and factorial invariance analysis in Chile. Spanish Journal of Psychology, 21, 1–17. https://doi.org/10.1017/sjp.2018.2.
Whisman, M. A., Judd, C. M., Whisman, M. A., & Judd, C. M. (2015). A Cross-National analysis of measurement invariance of the Satisfaction With Life Scale. Psychological Assessment, 28(2), 239–244.
Derogatis, L. R. (2001). BSI 18, Brief symptom inventory 18: Administration, scoring and procedures manual. Minneapolis: NCS Pearson, Inc.
Aaronson, N. K., Ahmedzai, S., Bergman, B., Bullinger, M., Cull, A., Duez, N. J., … de Haes, J. C. (1993). The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. Journal of the National Cancer Institute, 85(5), 365–376.
Muthén, L. K., & Muthén, B. O. (2004). Mplus user’s guide: Statistical analysis with latent variables: User’ss guide. Los Angeles: Muthén & Muthén.
Ferrando, P. J., & Lorenzo-Seva, U. (2017). Assessing the quality and appropriateness of factor solutions and factor score estimates in exploratory item factor analysis. Educational and Psychological Measurement. https://doi.org/10.1177/0013164417719308.
Lorenzo-Seva, U., & Ferrando, P. J. (2013). FACTOR 9.2: A comprehensive program for fitting exploratory and semiconfirmatory factor analysis and IRT Models. Applied Psychological Measurement, 37(6), 497–498. https://doi.org/10.1177/0146621613487794.
Schermelleh-Engel, K., Moosbrugger, H., & Müller, H. (2003). Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods of Psychological Research Online, (2), 23–74.
Hair, J. F., Black, W. C., & Babin, B. J. (2010). RE Anderson multivariate data analysis: A global perspective. New Jersey: Pearson Prentice Hall.
Schermelleh-Engel, K., Kerwer, M., & Klein, A. G. (2014). Evaluation of model fit in nonlinear multilevel structural equation modeling. Frontiers in Psychology, 5, 181. https://doi.org/10.3389/fpsyg.2014.00181.
Van de Schoot, R., Lugtig, P., & Hox, J. (2012). A checklist for testing measurement invariance. European Journal of Developmental Psychology, 9(4), 486–492.
Millsap, R. E., & Meredith, W. (2007). Factorial invariance: Historical perspectives and new problems. In R. Cudeck & R. C. MacCallum (Eds.), Factor analysis at 100 (pp. 131–152). Mahwah: LEA.
Little, T. D. (1997). Mean and covariance structures (MACS) analyses of cross-cultural data: Practical and theoretical issues. Multivariate Behavioral Research, 32(1), 53–76. https://doi.org/10.1207/s15327906mbr3201_3.
Ferrando, P. J. (1996). Calibration of invariant item parameters in a continuous item response model using the extended Lisrel measurement submodel. Multivariate Behavioral Research, 31(4), 419–439. https://doi.org/10.1207/s15327906mbr3104_2.
Ferrando, P. J., & Lorenzo-Seva, U. (2013). Unrestricted item factor analysis and some relations with item response theory. Retrieved from http://psico.fcep.urv.es/utilitats/factor.
Asparouhov, T. (2006). General multi-level modeling with sampling weights. Communications in Statistics - Theory and Methods, 35(3), 439–460. https://doi.org/10.1080/03610920500476598.
Courneya, K. S., Friedenreich, C. M., Quinney, H. A., Fields, A. L. A., Jones, L. W., & Fairey, A. S. (2003). A randomized trial of exercise and quality of life in colorectal cancer survivors. European Journal of Cancer Care, 12(4), 347–357. https://doi.org/10.1046/j.1365-2354.2003.00437.x.
Letourneau, J. M., Ebbel, E. E., Katz, P. P., Katz, A., Ai, W. Z., Chien, A. J., … Rosen, M. P. (2012). Pretreatment fertility counseling and fertility preservation improve quality of life in reproductive age women with cancer. Cancer, 118(6), 1710–1717. https://doi.org/10.1002/cncr.26459.
Campbell, A., Mutrie, N., White, F., McGuire, F., & Kearney, N. (2005). A pilot study of a supervised group exercise programme as a rehabilitation treatment for women with breast cancer receiving adjuvant treatment. European Journal of Oncology Nursing, 9(1), 56–63. https://doi.org/10.1016/j.ejon.2004.03.007.
Bai, X., Wu, C., Zheng, R., & Ren, X. (2011). The psychometric evaluation of the Satisfaction with Life Scale using a nationally representative sample of China. Journal of Happiness Studies, 12(2), 183–197. https://doi.org/10.1007/s10902-010-9186-x.
Gouveia, V. V., Milfont, T. L., da Fonseca, P. N., & de Coelho, J. A. P. M (2009). Life satisfaction in Brazil: Testing the psychometric properties of the Satisfaction With Life Scale (SWLS) in five Brazilian samples. Social Indicators Research, 90(2), 267–277. https://doi.org/10.1007/s11205-008-9257-0.
Hultell, D., & Petter Gustavsson, J. (2008). A psychometric evaluation of the Satisfaction with Life Scale in a Swedish nationwide sample of university students. Personality and Individual Differences, 44(5), 1070–1079. https://doi.org/10.1016/j.paid.2007.10.030.
Pons, D., Atienza, F. L., Balaguer, I., & García-Merita, M. L. (2000). Satisfaction with Life Scale: Analysis of factorial invariance for adolescents and elderly persons. Perceptual and Motor Skills, 91(1), 62–68. https://doi.org/10.2466/pms.2000.91.1.62.
Merluzzi, T., & Martinez Sanchez, M. (2018). Husbands’ perceptions of their wives’ breast cancer coping efficacy: Testing congruence models of adjustment. Cancer Management and Research, 10, 297–304.
Kayser, K., Acquati, C., Reese, J. B., Mark, K., Wittmann, D., & Karam, E. (2018). A systematic review of dyadic studies examining relationship quality in couples facing colorectal cancer together. Psycho-Oncology, 27(1), 13–21. https://doi.org/10.1002/pon.4339.
Acknowledgements
The authors would like to thank the investigators of the Neocoping study (coping, shared decision-making, and quality of life in patients with early-stage cancer treated with adjuvant chemotherapy) and the Supportive Care Working Group of the Spanish Society of Medical Oncology (SEOM).
Funding
This work was funded by the Spanish Society of Medical Oncology (SEOM) in 2015. The sponsor of this research has not participated in data collection, analysis, or interpretation, in writing the report, or in the decision to submit the article for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lorenzo-Seva, U., Calderon, C., Ferrando, P.J. et al. Psychometric properties and factorial analysis of invariance of the Satisfaction with Life Scale (SWLS) in cancer patients. Qual Life Res 28, 1255–1264 (2019). https://doi.org/10.1007/s11136-019-02106-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-019-02106-y