
Abstract
Purpose
To investigate the validity of direct and indirect health state utility (HSU) and subjective well-being measures in psoriasis vulgaris patients.
Methods
A convenience sampling framework was used to successively recruit patients with psoriasis vulgaris from the outpatient clinics of a tertiary hospital in Changsha, Central South China. Participants completed time trade-off (TTO), standard gamble (SG), the five-level EQ-5D (EQ-5D-5L), the WHO-5 well-being index, and the psoriasis disability index (PDI). The concurrent and known-groups validity of HSUs and well-being index in psoriasis patients were firstly studied. The agreements among HSUs and the relationship between HSU and well-being measures were further explored.
Results
A valid sample of 343 patients was analyzed. Mean HSU and well-being scores elicited from the EQ-5D-5L/TTO/SG and WHO-5 were 0.90/0.85/0.88 and 13.69, respectively. The Spearman correlation (concurrent validity) was the strongest between PDI and WHO-5 (r = 0.45), followed by with EQ-5D-5L (0.38), SG (r = 0.20), and the TTO (r = 0.18). The pairwise intraclass correlation coefficients among the three HSU measures were < 0.30. The known-groups validity was evident in all measures except for the SG. Exploratory factor analysis further suggests a complementary relationship between the EQ-5D-5L and WHO-5.
Conclusions
There is a poor agreement between direct and indirect methods on measuring HSU with psoriasis vulgaris. Results from this study recommend that the EQ-5D-5L is the most preferred method to elicit HSU from psoriasis vulgaris patients in mainland China. It is important to further analyze the subjective well-being in addition to the HSU to fully understand the impact of psoriasis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Psoriasis is a chronic, immune-mediated inflammatory skin disease. The prevalence of psoriasis in adults ranges from 0.91% (United States) to 8.5% (Norway) in Western countries [1]. In China, the prevalence of psoriasis is 0.47% [2], showing an upward trend from 0.12% in 1984 [3]. Affecting 85–90% of patients, the most prevalence form of psoriasis (psoriasis vulgaris) results in the occurrence of raised plaques with silvery scales that can present on any part of the skin, but are most commonly found on the scalp, back, and extensor surfaces (elbows and knees) [4]. Psoriasis has a profound impact on the patient’s everyday life. For instance, 59.8% of Chinese psoriatic people experience negative influences on quality of life (QoL) [2]. The burden of the disease extends beyond painful, debilitating, highly visible physical symptoms; psoriasis is associated with substantial psychological impairments, such as embarrassment, lack of self-esteem, anxiety, or helplessness [5, 6].
Health-related QoL (HRQoL), especially preference-based health-related QoL, has become an increasingly important outcome measure in a particular form of economic evaluation—cost-utility analysis (CUA) [7]. In CUA, the benefit measure commonly used is quality-adjusted life-years (QALYs), which accounts for both the length and quality of life. The quality is measured by using health state utility (HSU) scores, which lies on a (0–1) scale where 1 and 0 represent best health and death, respectively [8].
The HSU scores can be either measured directly or indirectly [7]. The direct approaches mainly include the standard gamble (SG) and the time trade-off (TTO). The SG method is generally considered to have the strongest theoretical foundation of choice-based valuation methods, as it can be traced to theory of rational decision-making under uncertainty set out by von Neumann and Morgenstern [9]. The TTO method was developed by Torrance et al. [10] as a simple alternative to the SG method and with health state valuation specifically in mind; in particular, the TTO task asks respondents to make a choice between two alternatives of certainty. There is no scientific consensus on the optimal specification of the TTO task [11]. The indirect approach mainly refers to using multi-attribute utility (MAU) instruments (which consist of a descriptive system and a value set usually derived from the general population in a particular country) [12]. Currently, the EQ-5D is the most widely used MAU instruments in the world [13, 14]. Although both direct and indirect approach can be used to elicit HSU scores, evidence suggests that they usually yield different utility scores; in particular, it has been commonly reported that the indirect approach produces lower HSU scores than the direct approach [15]. Identifying the optimal approach to elicit HSU scores from patients is crucial for prioritizing resource allocation within health sector.
Although the HSU, especially through using the MAU instruments such as the EQ-5D, has been widely used to facilitate resource allocation across different diseases in the health sector, the subjective well-being (SWB) (an alternative broader construct) has gained increasing attention in the policy debate [7, 16]. The SWB, which is commonly referred to as happiness, goes beyond health. Studying the SWB of psoriasis patients is particularly relevant since psoriasis can lead to substantial psychological stress for the patient. The classification system of the classical MAU instruments such as the EQ-5D mainly covers physical health dimensions [14, 17]. As such purely using the EQ-5D may underestimate the disease impact on overall QoL.
The primary aim of this study was to investigate the validity of three HSU (EQ-5D-5L, TTO, and SG) measures and one SWB instrument for use with psoriasis vulgaris patients. The secondary aim of this study was to explore the degree of agreement among three HSU measures, and to what extent the HSU (especially the EQ-5D-5L) and SWB measures align with each other.
Methods
Study population
Psoriasis vulgaris patients were recruited successively from the dermatological outpatient clinics of Xiangya Hospital Central South University, China, between May 2014 and February 2015. Patients were excluded if they were younger than 16 years at the time of the survey, unwilling to give an informed consent or unable to understand the questionnaires. All interviews were performed face-to-face by the two investigators (YZ and JLZ). Clinical information was collected from the hospital information system. Informed consent was obtained from all respondents prior to the interviews. The study was approved by the Ethics Review Board of the School of Medicine, Shandong University (Reference No. LL-201401044), and the research adhered to the tenets of the Declaration of Helsinki.
Instruments
The questionnaire consists of three sections. Section 1 includes socio-demographic characteristics of respondents, e.g., age, gender, and educational level. Section 2 includes clinical characteristics of the respondents, e.g., disease duration, the psoriasis area, and severity index (PASI). Section 3 includes two direct approaches to elicit HSU (the SG and TTO) through an interview-based method (without using a visual aid tool), one self-assessed MAU instrument (Chinese version EQ-5D-5L) [18], a disease-specific QoL instrument (Psoriasis Disability Index, PDI), and the WHO-Five Well-Being Index (WHO-5). For all QoL and SWB instruments, the official Chinese versions were used.
Standard gamble
Participants were asked to imagine a technology that would restore them to perfect health. However, since this imaginary technology could fail, what would be the highest risk of death that (s)he would be willing to accept. SG utility value was calculated as the amount of risk (in percentage) of death that a participant was willing to take for the hypothetical technology that could restore perfect health, i.e.,
Time trade-off
The TTO method measures the number of years the patient is willing to sacrifice for a new technology that restores perfect health. Participants were asked to predict their expected life expectancy and the maximum number of remaining years of life they would be willing to give up if (s)he could receive an imaginary technology and have perfect health for the rest of their lives. TTO utility score was calculated based on the time traded in years over the expected number of years of the respondent’s remaining life that (s)he is willing to give up for a hypothetical technology to restore perfect health, i.e.,
EQ-5D-5L
The 3-level EQ-5D questionnaire (EQ-5D-3L) was introduced in 1990s and it is the most widely used generic preference-based HRQoL instrument internationally. To improve the instrument’s sensitivity and to reduce ceiling effects, the five-level EQ-5D questionnaire (EQ-5D-5L) was developed in 2011. The EQ-5D-5L adopts the same five dimensions as EQ-5D-3L (mobility, self-care, usual activities, pain/discomfort, anxiety/depression). Each dimension has five levels: no problems, slight problems, moderate problems, severe problems, and unable to/extreme problems [19].
The Chinese version of the EQ-5D-5L descriptive system and Chinese-specific scoring algorithm of EQ-5D-5L were adopted [18, 20]. The Chinese-specific valuation study followed a standard research protocol (EQ-VT v1.0) developed by the EuroQol Group. A total of 86 health states were valued by using a composite TTO technique from a total of 1271 urban residents. The final tariff which generates all 3125 EQ-5D-5L health state was derived from 86 health states using regression technique. The Chinese-specific EQ-5D-5L utility scores ranged from − 0.391 to 1.
WHO-five well-being index
The WHO-5 is one of the most widely used generic questionnaires assessing subjective psychological well-being. It contains five positively phrased items, related to positive mood (good spirits, relaxation), vitality (being active and waking up fresh and rested), and general interests (being interested in things). Since its first publication in 1998, the WHO-5 has been applied successfully across a wide range of diseases or conditions [21, 22].
Psoriasis disability index
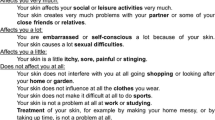
The PDI focuses on the functional lifestyle disabilities caused by psoriasis [23]. It includes five subscales: daily activities (five-item), work or school (three-item), leisure (four-item), personal relationships (two-item), and treatment (one-item). The Tick-Box method was used in this study, so that each item was answered with four options (not at all, a little, a lot, very much). A summary score (ranged between 0 and 45) was calculated by adding raw responses of all 15 items; the higher the score, the worse the quality of life [24]. The Chinese version PDI has been shown to have good reliability and validity [25].
Psoriasis area and severity index (physician-assessed)
The PASI is the standard objective measure of psoriasis severity. It combines the intensity of the three main signs of psoriasis (redness, scaliness, and thickness) weighted by the coverage of the affected body part (legs, body, arms, and head) [26]. PASI results in a score ranging from 0 to 72, and it is usually re-grouped into three categories implying three severity levels of psoriasis: PASI < 7 (mild severity), PASI 7–12 (moderate severity), and PASI > 12 (severe severity) [27].
Statistical analysis
The means, standard deviation (SD), 95% confidence interval (CI), and medians of HSU and SWB scores were calculated. The null hypothesis of normal distribution of HSU and SWB scores was rejected by the Shapiro–Wilk W test. The agreement between the three HSU measurements was studied using the intraclass correlation coefficients (ICCs) (with an ICC > 0.7 indicating a strong agreement [28]) and the Bland–Altman plots [29].
To explore the optimal measure for eliciting HSU, as well as the potential of the SWB measure in psoriasis vulgaris patients, concurrent validation and known-groups validation analyses were conducted. Firstly, the Spearman correlation coefficient between the HSU/SWB measure and psoriasis-specific PDI scores was calculated to investigate the concurrent validity of the generic outcome measures. Secondly, regression analyses were conducted to investigate the known-groups validity. It is hypothesized that psoriasis patients in a more severe stage (according to the PASI score) should have a significantly larger decrement in utility/well-being score. For three HSU measures, Tobit models were used as the ceiling issue (i.e., a large proportion of patients were classified as full health and with a utility score of 1.0) is evident in the utility data [30]. On the other hand, the classical ordinary least squares model was used when the dependent variable was the well-being data.
The relationship between HSU and SWB was also studied by firstly calculating the Spearman correlation coefficients. Further analyses were conducted between the EQ-5D-5L and the WHO-5 using both exploratory factor analysis and a regression analysis (reported in the supplementary document).
All P values reported are two-sided and considered statistically significant when the values are below 0.05. With the exception of the Bland–Altman plot, which was performed using MedCalc version 16.8 (MedCalc Software, Ostend, Belgium), all other statistical analyses were performed using Stata version 14.1 (StataCorp LP, College Station, TX).
Results
Patient characteristics
A total of 362 patients were invited to the interview and among them four patients refused to participate. Further, eight patients who initially agreed to participate withdrew from the survey after completing the socio-demographic information. Of the left 350 psoriasis vulgaris patients who were interviewed, seven were excluded due to incomplete answers to SG and/or TTO questions. A valid sample of 343 patients who completed all HSU and SWB questionnaires was analyzed.
Socio-demographic and clinical characteristics of the 343 participants are presented in Table 1. The mean age was 39.4 ± 12.9 years (range 16–80 years). Of the respondents, one-third (34.4%) had completed secondary school education, 69.4% were male, most of them (74.1%) had been married, 59.8% lived in rural area, and 20.1 and 26.8% were company employee and freelancers, respectively. The mean duration of psoriasis vulgaris was 8.4 ± 9.3 years (range 0.1–48 years). Apart from 12 respondents who did not complete the PASI questionnaire in the valid sample, the psoriasis vulgaris conditions of 139 (42.0%) respondents were of moderate or severe severity.
Descriptive statistics
The mean health state utility and SWB scores for psoriasis vulgaris patients are shown in Table 2. Among three methods eliciting health state utilities, the indirect method, the EQ-5D-5L, had the highest mean utility (0.90, 95% CI 0.89–0.91, median 0.94), followed by the SG method (0.88, 95% CI 0.86–0.90, median 0.95) and the TTO method (0.85, 95% CI 0.83–0.87, median 0.90). The mean utility differences were significant between TTO and EQ-5D-5L/SG (P < 0.05) and insignificant between EQ-5D-5L and SG (P > 0.05). The WHO-5 well-being index had a mean score of 13.69 (95% CI 13.08–14.31, median 14). It can also be seen that substantial ceiling effects were evident in all three health state utility measures, with 29%/27%/17% respondents reported to have a full health based on the SG/EQ-5D-5L /TTO method. On the other hand, only 2% respondents reported to have a full WHO-5 well-being state. None of the four instruments have a floor effect. The HSU and the WHO-5 well-being scores of different psoriasis severities are shown in Supplementary Table 1. The distributions for three health state utility scores and the WHO-5 well-being item/overall scores are presented in Figs. 1 and 2, respectively.

Distribution of health state utility scores

Distribution of the WHO-5 well-being index
Correlations and agreements
Table 3 presents both Spearman’s correlation and ICC coefficients. The ICCs ranged from 0.15 (EQ-5D-5L & SG) to 0.27 (EQ-5D-5L & TTO), indicating poor absolute agreements between each pair of health state utility measures. Bland–Altman plots (Fig. 3) further showed that between each of the two health state utility measures the range of 95% limits of agreement (LOA) were 0.66 (EQ-5D-5L & TTO), 0.86 (EQ-5D-5L & SG), and 0.94 (TTO & SG), respectively.

Bland–Altman plots of comparison among EQ-5D-5L, SF-6D, and TTO. The 95% limits of agreement are shown with a dashed line, and the mean difference between both measurements is shown with a solid line
Concurrent validity and known-groups validity
The absolute magnitudes of Spearman’s correlation coefficient were found to be the strongest between the PDI and the WHO-5 well-being index (r = 0.45), followed by between the PDI and three health state utility instruments, the EQ-5D-5L (r = 0.38), the SG (r = 0.20), and the TTO (r = 0.18).
Table 4 reports the known-groups validity from the regression analysis. Except for the SG, all the other three measures found significant decrements in utility or well-being scores along with an increased severity of psoriasis. Compared to the mild severity patients, patients with moderate severity state on average had a decrement utility of 0.047/0.050, while patients with severe psoriasis had a decrement utility of 0.092/0.065 based on the EQ-5D-5L/TTO, respectively. On average, an additional year of disease duration was associated with a 0.002 utility or 0.075 WHO-5 well-being score increased. Other significant characteristics include (1) gender in the EQ-5D-5L equation, (2) age and education status in the TTO equation, (3) education status in the SG equation, and (4) occupation status and region in the well-being equation.
Health state utility versus subjective well-being
The exploratory factor analysis result between the EQ-5D-5L and the WHO-5 is presented in Table 5. Two factors were extracted with the first factor referring to the psycho-social dimension (including all five WHO-5 well-being and the anxiety/depression dimension from the EQ-5D-5L) and the second factor referring to the physical dimension (including the left 4 EQ-5D-5L dimensions). This result indicates that the EQ-5D-5L and the WHO-5 are complementary. Supplementary documentation Table 2 further presents the regression analysis result in which the dependent variable was the WHO-5 well-being score and the independent variables were five EQ-5D-5L dimensions (included as dummy variables). It was found that overall the EQ-5D-5L can only explain 26.8% variance of the WHO-5 well-being index. Among the five dimensions, self-care, usual activities, and pain were all insignificant. Except for the anxiety/depression dimension (which were highly significant), the second level of mobility dimension was significantly lower than the reference level.
Discussion
By focusing on a patient sample in mainland China, this study investigated the validity and sensitivity of HSU (in particular the recently developed EQ-5D-5L) and SWB instruments in psoriasis, a common, chronic skin disease. The study also contributed to the current discussion about the relationship between HSU and SWB measures in the resource allocation within health sector.
It is firstly shown that for the whole sample the mean health state utility score based on the EQ-5D-5L (0.90) was significantly larger than those based on the SG (0.88) and TTO (0.85). This trend remains the same for the mild and moderate psoriasis patient groups. For patients with severe psoriasis, the SG produces the highest mean utility score (0.86), followed by the EQ-5D-5L (0.85) and the TTO (0.80). To the best of our knowledge, this is one of the few studies using the EQ-5D-5L to elicit health states utility scores among psoriasis vulgaris patients internationally. The sample mean EQ-5D-5L utility score from this Chinese study (overall sample 0.90, mild 0.92, moderate 0.89, and severe 0.85) was higher than both a recently published Hungarian study (overall sample 0.84) [31] and a Greek study (overall sample 0.74, mild 0.81, moderate 0.73, and high severe 0.57) [32]. With the different country-specific EQ-5D-5L tariffs been applied, the potential different compositions of psoriasis severities within the patient sample, as well as the potential different response patterns of the EQ-5D-5L questionnaire across different countries can all be the reasons behind above dissimilarities. Regarding two direct approaches, both the mean SG and TTO utility scores from this study (0.88 and 0.85) were much lower than what have previously been reported by Lundberg et al. (SG = 0.99, TTO = 0.93) based on patients in Sweden [33]. Yet, the observation that the sample mean SG utility was higher than the TTO utility is in line with above Swedish study. In addition, the correlation between two direct approaches was higher in this Chinese study as compared to the Swedish study (0.40 vs. 0.24). However, the above difference should be interpreted with caution since the direct approaches were based upon individual perspective. As such, different socio-demographic and clinical characteristics, different health systems across countries, as well as different time frames adopted in the valuation task (e.g., respondents’ own life expectation in this study vs. a 30-year time frame in the Swedish study) could all lead to different utility scores being elicited [34, 35].
In addition to the differences in absolute magnitudes of mean utility scores, the mean utility differences between different psoriasis severities also varied among three approaches. For example, compared to patients in mild severity (PASI scores < 7), patients in severe severity (PASI scores > 12) had a significantly mean utility difference of − 0.07, − 0.08, and − 0.04 based on the EQ-5D-5L, TTO, and SG, respectively.
There is also a poor agreement among HSU scores elicited from three approaches. The magnitude of ICC values between EQ-5D-5L and two direct approaches (TTO and SG) were 0.27 and 0.15, respectively, both less than 0.30. The ICC between EQ-5D-5L and TTO (0.27) is larger than that of the two direct instruments (0.24). The lack of a strong agreement between indirect and direct approaches may partly be due to the fact that in the indirect approach, the EQ-5D-5L utility score was calculated based on a pre-defined value set derived from the general population in China (i.e., it was based on a societal perspective) [20, 36]. On the other hand, both the TTO and SG task elicited HSU score directly from individual patient’s perspective. Furthermore, compared to the two direct approaches, there was a much higher correlation between EQ-5D-5L and psoriasis-specific instrument PDI. The overall poor agreements indicate that the choice of the approach will have a non-negligible effect on the HSU scores been elicited. These three approaches cannot be used interchangeably.
The fact that HSU scores elicited from different approaches (either between or within direct and indirect approaches) are not comparable has been documented in the literature [15, 37]. Yet the findings from this study differ from the previous review [15] that the indirect approach (i.e., EQ-5D-5L) tends to elicit higher HSU scores than direct approaches in this Chinese patient sample. Though it is not the aim of this study to explore what are the reasons behind this observation, one of the potential explanations is that in general ethnic Chinese may be more likely to endure health issues than other ethnicities [38] and thus less likely to report having issues in the HRQoL questionnaire. For example, comparing the EQ-5D-3L utility scores elicited based on representative samples in a province from China and a state from Australia, it was shown that the mean utility score was much higher in adults in urban China than in Australia (0.96 vs. 0.87, respectively); in particular, the proportions of respondents who reported to have moderate or extreme problems in three EQ-5D-3L dimensions (usual activities, pain/discomfort, and anxiety/depression) were much lower in Chinese sample [30, 39]. Further qualitative study will be helpful to understand the response pattern on the HRQoL questionnaire of Chinese people.
Based on concurrent and known-group validity results, an indirect approach using the EQ-5D-5L instrument is preferable than the direct approach using TTO or SG to elicit HSU in psoriasis vulgaris patients. It should also be noted that although the new EQ-5D-5L classification system was developed to partially solve the widely reported ceiling effect issue in the EQ-5D-3L, in this study there were still 27% of patients reported to be in full health based on the EQ-5D-5L classification system, slightly lower than the SG approach (29%), but much higher than the TTO approach (17%).
This study also explored the potential benefit of using a SWB measure along with the EQ-5D-5L in psoriasis patients. Compared to the HSU instruments, it can be firstly seen that there was no ceiling effect in the WHO-5 well-being score. The WHO-5 well-being index can also significantly distinguish between different severity levels and demonstrated the known-groups validity. The correlation between WHO-5 and PDI was even stronger than between any of the three HSU measures and PDI. Further empirical evidence from exploratory factor analysis and regression analysis between WHO-5 and EQ-5D-5L suggests that these two instruments were complementary. For psoriasis patients, measuring SWB can further provide important information that may be omitted by using HSU instruments alone.
There were a couple of limitations in this study. Firstly, the study populations of psoriasis vulgaris patients were surveyed at one tertiary hospital of central China; as such it may not be representative of all psoriasis vulgaris patients in mainland China. However, the study population includes different severities of psoriasis vulgaris. Secondly, since this is the first time the Chinese-specific utility/SWB scores for psoriasis vulgaris patients have been reported, the targeting sample size was not able to be calculated prior to the data collection. However, the valid sample size of this study is similar to previous literature [31,32,33]. Thirdly, the cross-sectional nature of this study makes it impossible to investigate the responsiveness of the outcome measure in detecting changes in HSU or SWB of the psoriasis patients.
Conclusion
Both HSU measures (including the recently developed EQ-5D-5L instrument and the direct TTO approach) and the WHO-5 well-being index show known-group validity of psoriasis vulgaris patients in mainland China. There is a lack of agreement among the three approaches to elicit utility score and among them, the EQ-5D-5L is the most preferred method to elicit utility scores for psoriasis vulgaris patients in mainland China. The HSU (i.e., EQ-5D-5L) and WHO-5 SWB are complementary measures in nature and it is important to further analyze the subjective well-being in addition to the HSU to fully understand the impact of psoriasis. Although the dominant role of EQ-5D is in health resource allocation internationally, the importance of disease impact on psychological well-being may be underestimated. Along with an increasing interest to facilitate resource allocation based on a broader SWB concept, there is a need to explore and define a standard set of instruments which should be collected within clinical trials.
References
Parisi, R., Symmons, D. P., Griffiths, C. E., & Ashcroft, D. M., (2013). Global epidemiology of psoriasis: A systematic review of incidence and prevalence. Journal of Investigative Dermatology, 133(2), 377–385.
Ding, X., Wang, T., Shen, Y., Wang, X., Zhou, C., Tian, S., et al. (2012). Prevalence of psoriasis in China: A population-based study in six cities. European Journal of Dermatology, 22(5), 663–667.
Shao, C. G., Zhang, G. W., & Wang, G. C. (1987). Distribution of psoriasis in China: A nationwide screening. Proceedings of the Chinese Academy of Medical Sciences Peking Union Medical College, 2(2), 59–65.
Palfreeman, A. C., McNamee, K. E., & McCann, F. E. (2013). New developments in the management of psoriasis and psoriatic arthritis: A focus on apremilast. Drug Design, Development and Therapy, 7, 201–210.
Colombo, D., & Perego, R. (2013). Quality of life in psoriasis. In H. Lima (Ed.), Psoriasis: types, causes and medication (Chap. 07). Rijeka: InTech.
WHO (2016). Global Report on Psoriasis, http://apps.who.int/iris/bitstream/10665/204417/1/9789241565189_eng.pdf. Accessed March 21 2017.
Brazier, J., Ratcliffe, J., Salomon, J., & Tsuchiya, A. (2016). Measuring and valuing health benefits for economic evaluation (2nd edn). Oxford: Oxford University Press.
Torrance, G. W. (1986). Measurement of health state utilities for economic appraisal. Journal of Health Economics, 5(1), 1–30.
von Neumann, J., & Morgenstern, O. (1944). Theory of games and economic behavior. Princeton: Princeton University Press.
Torrance, G. W., Thomas, W. H., & Sackett, D. L. (1972). A utility maximization model for evaluation of health care programs. Health Services Research, 7(2), 118–133.
Attema, A. E., Edelaar-Peeters, Y., Versteegh, M. M., & Stolk, E. A. (2013). Time trade-off: One methodology, different methods. European Journal of Health Economics, 14(Suppl 1), S53–S64.
Gray, A. M., Clarke, P. M., Wolstenholme, J. L., & Wordsworth, S. (2010). Applied methods of cost-effectiveness analysis in healthcare. New York: Oxford University Press.
Brooks, R. (1996). EuroQol: The current state of play. Health Policy, 37(1), 53–72.
Richardson, J., Mckie, J., & Bariola, E. (2014). Multiattribute utility instruments and their use. Encyclopedia of Health Economics, 2, 341–357.
Arnold, D., Girling, A., Stevens, A., & Lilford, R. (2009). Comparison of direct and indirect methods of estimating health state utilities for resource allocation: Review and empirical analysis. BMJ, 339, b2688.
Cubi-Molla, P., de Vries, J., & Devlin, N. (2014). A study of the relationship between health and subjective well-being in Parkinson’s disease patients. Value in Health, 17(4), 372–379.
Chen, G., Ratcliffe, J., Kaambwa, B., Mccaffrey, N., & Richardson, J. (2017). Empirical comparison between capability and two health-related quality of life measures. Social Indicators Research, (1), 1–16, https://doi.org/10.1007/s11205-017-1788-9.
Luo, N., Li, M., Liu, G. G., Lloyd, A., de Charro, F., & Herdman, M. (2013). Developing the Chinese version of the new 5-level EQ-5D descriptive system: The response scaling approach. Quality of Life Research, 22(4), 885–890.
Herdman, M., Gudex, C., Lloyd, A., Janssen, M. F., Kind, P., Parkin, D., et al. (2011). Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research, 20(10), 1727–1736.
Luo, N., Liu, G., Li, M., Guan, H., Jin, X., & Rand-Hendriksen, K. (2017). Estimating an EQ-5D-5L value set for China. Value in Health, 20(4), 662–669.
Topp, C. W., Ostergaard, S. D., Sondergaard, S., & Bech, P. (2015). The WHO-5 Well-Being Index: A systematic review of the literature. Psychotherapy and Psychosomatics, 84(3), 167–176.
Bech, P., Gudex, C., & Johansen, K. S. (1996). The WHO (Ten) well-being index: Validation in diabetes. Psychotherapy & Psychosomatics, 65(4), 183–190.
Finlay, A. Y., & Kelly, S. E. (1987). Psoriasis: An index of disability. Clinical & Experimental Dermatology, 12(1), 8–11.
Finlay, A. Y., & Coles, E. C. (1995). The effect of severe psoriasis on the quality of life of 369 patients. British Journal of Dermatology, 132(2), 236–244.
He, Z., Lu, C., Ou, A., Fang, J., Wang, D., Deng, J., et al. (2012). Reliability and validity of the Chinese version of the Psoriasis Disability Index (PDI) in Chinese patients with psoriasis. Health & Quality of Life Outcomes, 10, 37.
Fredriksson, T., & Pettersson, U. (1978). Severe psoriasis–oral therapy with a new retinoid. Dermatologica, 157(4), 238–244.
Schmitt, J., & Wozel, G. (2005). The psoriasis area and severity index is the adequate criterion to define severity in chronic plaque-type psoriasis. Dermatology, 210(3), 194–199.
Fayers, P., & Machin, D. (2013). Quality of life: The assessment, analysis and interpretation of patient-reported outcomes: Wiley.
Bland, J. M., & Altman, D. G. (1986). Statistical methods for assessing agreement between two methods of clinical measurement. Lancet, 1(8476), 307–310.
Zhou, Z., Fang, Y., Zhou, Z., Li, D., Wang, D., Li, Y., et al. (2017). Assessing income-related health inequality and horizontal inequity in China. Social Indicators Research, 132(1), 241–256.
Poor, A. K., Rencz, F., Brodszky, V., Gulacsi, L., Beretzky, Z., Hidvegi, B., et al. (2017). Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L in psoriasis patients. Quality of Life Research, 26(12), 3409–3419.
Yfantopoulos, J., Chantzaras, A., & Kontodimas, S. (2017). Assessment of the psychometric properties of the EQ-5D-3L and EQ-5D-5L instruments in psoriasis. Archives of Dermatological Research, 309(5), 357–370.
Lundberg, L., Johannesson, M., Silverdahl, M., Hermansson, C., & Lindberg, M. (1999). Quality of life, health-state utilities and willingness to pay in patients with psoriasis and atopic eczema. British Journal of Dermatology, 141(6), 1067–1075.
Boye, K. S., Matza, L. S., Feeny, D. H., Johnston, J. A., Bowman, L., & Jordan, J. B. (2014). Challenges to time trade-off utility assessment methods: When should you consider alternative approaches? Expert Review of Pharmacoeconomics & Outcomes Research, 14(3), 437–450.
Matza, L. S., Boye, K. S., Feeny, D. H., Bowman, L., Johnston, J. A., Stewart, K. D., et al. (2015). The time horizon matters: Results of an exploratory study varying the timeframe in time trade-off and standard gamble utility elicitation. European Journal of Health Economics Hepac Health Economics in Prevention & Care, 17(8), 1–12.
Devlin, N. J., Shah, K. K., Feng, Y., Mulhern, B., & van Hout, B. (2017). Valuing health-related quality of life: An EQ-5D-5L value set for England. Health Economics, 27(1), 7–22.
Gamst-Klaussen, T., Chen, G., Lamu, A. N., & Olsen, J. A. (2016). Health state utility instruments compared: Inquiring into nonlinearity across EQ-5D-5L, SF-6D, HUI-3 and 15D. Quality of Life Research, 25(7), 1667–1678.
Wang, Y., Tan, N. C., Tay, E. G., Thumboo, J., & Luo, N. (2015). Cross-cultural measurement equivalence of the 5-level EQ-5D (EQ-5D-5L) in patients with type 2 diabetes mellitus in Singapore. Health & Quality of Life Outcomes, 13(1), 103.
Clemens, S., Begum, N., Harper, C., Whitty, J. A., & Scuffham, P. A. (2014). A comparison of EQ-5D-3L population norms in Queensland, Australia, estimated using utility value sets from Australia, the UK and USA. Quality of Life Research, 23(8), 2375–2381.
Acknowledgements
The authors thank all the participants for their time and effort. Responsibility for any remaining errors lies solely with the authors.
Funding
The project was sponsored by the Scientific Research Foundation for the Returned Overseas Chinese Scholars, State Education Ministry (No. [2015]311).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the Ethics Review Board of the School of Medicine, Shandong University (Reference No. LL-201401044), and the research adhered to the tenets of the Declaration of Helsinki.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Liu, L., Li, S., Zhao, Y. et al. Health state utilities and subjective well-being among psoriasis vulgaris patients in mainland China. Qual Life Res 27, 1323–1333 (2018). https://doi.org/10.1007/s11136-018-1819-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-018-1819-2