
Abstract
Purpose
Health-related quality of life (HRQoL) is an important patient-reported outcome in clinical and health research. The EQ-5D-Y assesses child and adolescent HRQoL by five items on mobility, self-care, usual activities, pain/discomfort, and anxiety/depression as well as a visual analogue scale (VAS) on the current health state. This study investigates predictors of self-reported HRQoL according to the EQ-5D-Y in chronically ill children and adolescents using longitudinal data.
Methods
Data from the German Kids-CAT study on children and adolescents with asthma, diabetes, and juvenile arthritis gathered over a period of six months were analyzed (n = 310; 7–17 years old; 48% female). Self-, parent-, and pediatrician-reported data were collected from June 2013 to October 2014. Generalized linear mixed models and linear mixed models served to examine effects of socio-demographic as well as disease- and health-specific predictors on the items as well as on the VAS of the EQ-5D-Y.
Results
Ceiling effects for the EQ-5D-Y indicated low burden of disease in the analyzed sample. Longitudinal analyses revealed associations between less health complaints and better HRQoL for all investigated HRQoL domains. Further, age- and gender-specific effects, and associations of better disease control, longer duration of the disease and less mental health problems with better HRQoL were found.
Conclusions
Subjective health complaints and mental health problems should be considered in the care of children and adolescents with asthma, diabetes, and juvenile arthritis. Future research should suggest administering the items of the EQ-5D-Y with five instead of three response options, and investigate HRQoL over a longer period.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The EQ-5D is a standardized, brief, easy to administer and internationally well-established instrument developed by the EuroQol group [1,2,3,4]. The measure serves to assess generic health-related quality of life (HRQoL) in adults in population-based and clinical samples, and is often used for health economic analyses [1,2,3,4]. For children and adolescents, the youth version of the EQ-5D, i.e., the EQ-5D-Y, was developed (for respondents aged 8 years onwards [5]). The EQ-5D-Y is available as self- and proxy-report, is currently offered in more than 50 language versions [6] and it includes five items on mobility, self-care, usual activities, pain/discomfort, and anxiety/depression as well as a visual analogue scale (VAS) gathering a rating of the current overall health state.
Evidence for the feasibility, reliability, and validity of the EQ-5D-Y was found in a large multinational population-based study [7], among South African high school children [8], in a Swedish general population sample [9], and among Spanish school children [10]. The EQ-5D-Y was used in different clinical populations (see Reviews including the EQ-5D-Y [11, 12]). Clinical studies reported evidence for the feasibility and validity of the EQ-5D-Y among Swedish children and adolescents with functional disabilities [9], among Swedish children with asthma [13], as well as among German children and adolescents with cystic fibrosis [14]. Moreover, Jonsson and colleagues found a better health state according to the VAS in male than female adolescents with asthma [15]. Murillo and colleagues [16] investigated effects of socio-demographic and clinical factors on the health state according to the VAS among Spanish children and adolescents with diabetes (n = 136; 8–19 years old). The authors found better health states and better HRQoL according to the KIDSCREEN-10 index [17] for younger (8–11 years old) compared to older children and adolescents (12–19 years old) in line with findings in general population samples [16]. Further, the authors detected a negative influence of mental health problems on the VAS in a multivariate model [16].
Longitudinal studies using the EQ-5D-Y are very rare. Findings based on data gathered at the beginning and at the end of an inpatient and outpatient treatment in German children and adolescents with musculoskeletal, respiratory, and metabolic diseases (n = 84; with an averaged interval between the measurements of about 4 weeks) showed that the EQ-5D-Y is a responsive measure able to capture improvements in HRQoL [18]. Further, evidence for the convergent validity and sensitivity to change of the VAS were found in children with Hodgkin disease (n = 51; data gathered at four time points over one year [19]).
Further research used other well-established self-reported HRQoL-questionnaires such as the Pediatric Quality of Life Inventory™ [20], KINDL-R [21] and KIDSCREEN [17] in clinical samples. Corresponding studies found better overall HRQoL in younger compared to older children with asthma [22] and diabetes [23]. Some studies found no gender-specific effect on overall HRQoL [22, 24], but most other studies reported better overall HRQoL for boys than girls with chronic conditions (e.g., [25, 26]). Further, a higher socio-economic status (SES) was related to better overall HRQoL in children and adolescents with diabetes [27, 28]. Among children with asthma, disease severity was negatively associated with overall HRQoL [29]. In children and adolescents with diabetes, lower overall HRQoL was related to poor glycemic control (HbA1c) [28], earlier age of disease onset [25], and the presence of at least one comorbid disease [30]. To our knowledge, no study investigated the influence of health complaints on HRQoL in corresponding clinical samples so far, but among Swedish school children more health complaints were related to lower overall HRQoL [31].
The present study provides a secondary analysis of longitudinal data gathered in the German Kids-CAT study on health and HRQoL in children and adolescents with asthma, diabetes, and juvenile arthritis. Based on baseline data of the Kids-CAT study, a former study already reported good HRQoL according to the EQ-5D-Y and disease-group-specific differences, but no differences in HRQoL were found compared to a general population sample [32]. In the present study, we explore effects of socio-demographic as well as disease- and health-specific predictors on self-reported HRQoL according to the items and the VAS of the EQ-5D-Y based on data gathered over a period of six months. We expected to find better HRQoL associated with male gender, younger age, higher SES, no migration background, a less severe disease, a shorter duration of the disease, no severe comorbid disease as well as with less health complaints and less mental health problems.
Methods
Study
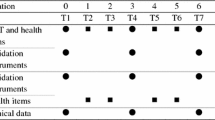
The primary goals of the Kids-CAT study were to develop, implement, and validate the first German-speaking computer-adaptive test for HRQoL in healthy and chronically ill children and adolescents (i.e., the Kids-CAT; see [33,34,35]). The observational Kids-CAT study investigated n = 312 children and adolescents aged 7–17 years diagnosed with bronchial asthma (J45), diabetes mellitus (E10−11) or juvenile arthritis (M08) according to the International Classification of Diseases-10 (ICD-10). Study participants were consecutively recruited at specialist outpatient departments of the University Medical Center Schleswig–Holstein in Kiel and Luebeck (northern Germany). Each participant was enrolled together with a parent; data were collected from June 2013 to October 2014. Self-reported information was gathered using an online survey, parent-reports were collected by a paper–pencil questionnaire, and specialized pediatricians documented disease-specific clinical data on participants using a short paper–pencil questionnaire. Ethical approval was received from the ethics committees of the Universities Kiel and Luebeck, and from the Chamber of Psychotherapists in Hamburg. More details on the Kids-CAT study are published [35].
Sample
We analyzed data from the first three major measurement points of the Kids-CAT study, i.e., baseline (t1), 3-month follow-up (t2) and 6-month follow-up (t3). Cases were included in subsequent analyses, if valid EQ-5D-Y data were given for at least one of the three measurement points (n = 310).
Measures
Generic health-related quality of life
The EQ-5D-Y was administered in its self-reported German version at each measurement point. Its five items on mobility (“walking about”), self-care (“looking after myself”), usual activities (“doing usual activities”), pain/discomfort (“having pain or discomfort”), and anxiety/depression (“feeling unhappy, sad or worried”) are administered with three response options representing different levels of problems (i.e., 0 = “no problems,” 1 = “some problems,” and 2 = “a lot of problems”). Further, the VAS gathers a self-rating of the current overall health state on a scale ranging from 0 (representing the worst health state, the respondent can imagine) to 100 (the best health state). Value sets (representing country-specific preference scores of the general public) were not used in this study (those scores are not provided so far).
Socio-demographic factors
The SES was assessed by parent-reports using an SES index [36, 37] including seven items on education, occupation, and income (index scores range from 3 to 21); higher index scores indicate better SES. For sample description, we used cutoffs determined based on data from a German general population sample to categorize participants into groups with low (first quintile of the reference population), medium (second to fourth quintile), and high SES (fifth quintile) [37]. Further, we determined a potential migration background based on Schenk and colleagues [38]. A participant was considered to have a migration background, if (i) both parents were born in a country other than Germany or if (ii) the participant and at least one parent were born in a country other than Germany, or if (iii) the native language of the participant was not German.
Disease- and health-specific factors
For each participant, the center (0 = “Luebeck”, 1 = “Kiel”) was documented. Based on physician-reported information, we allocated participants to disease groups (i.e., asthma, diabetes, and juvenile arthritis), calculated the duration of the disease (in years, at baseline) and created a binary variable indicating, if participants had a severe comorbid disease (0 = “none”, 1 = “at least one”).
Disease control was determined at each measurement point based on physician-reported data. Short sets of disease-specific items were developed by pediatric sub-specialists using clinical disease-specific guidelines to collect information on the current level of disease control (e.g., on symptoms at day and at night for asthma, hyper- and hypoglycaemic episodes including HbA1c measurements for diabetes, and ophthalmologic complications for juvenile arthritis). We created a binary variable for each measurement point differentiating participants with partly or completely uncontrolled diseases (0) from those with good disease control (1).
Health complaints were measured at each measurement point using the self-reported German version of the Health Behavior in School-aged Children Symptom Checklist (HBSC-SCL) [39]. The HBSC-SCL includes eight items assessing the frequency of complaints (e.g., headache, sleeping difficulties) using a five-point response scale (from 0=“most days” to 4=“seldom or never”). All items were recoded and gathered in a sum score with higher scores indicating more frequent health complaints. For sample description, we identified those with recurrent health complaints (i.e., at least two complaints occurred at least once a week [40]).
Mental health problems in children and adolescents were measured at each measurement point using the parent-reported German version of the Strengths and Difficulties Questionnaire (SDQ) [41]. The SDQ covers emotional symptoms, peer-related problems, conduct problems, and hyperactivity/inattention with five items per domain. SDQ items refer to the past six months and are offered with three response options (0 = “not true” to 2 = “certainly true”). The total difficulties score over the four problem scales was calculated with higher scores indicating more problems. For sample description, we categorized participants into two groups (“normal” vs. “borderline/abnormal”) using the recommended cut-off [42].
Data analysis
First analyses served to describe the analyzed sample and examine distributions of EQ-5D-Y data.
Predictors of self-reported HRQoL according to the EQ-5D-Y
We investigated effects of socio-demographic as well as disease- and health-specific predictors on self-reported HRQoL using individual growth modeling. To analyze EQ-5D-Y items, generalized linear mixed models (GLMMs) were calculated using a binominal distribution and a logit link-function for mobility (Model A1), usual activities (Model B1), pain/discomfort (Model C1), and anxiety/depression (Model D1). The item on self-care was excluded from the analyses due to very severe ceiling effects (see Results). Further, a linear mixed model (LMM) was used for the VAS (Model E1). In each analyzed model, the same predictors were included. We examined effects of predictors measured over time (level-1-predictors) and influences of predictors measured only at baseline (level-2-predictors). Level-1-predictors included a time variable (representing individual information on the intervals between measurement points in months with a value of zero indicating baseline), as well as variables on disease control, health complaints and mental health problems. Level-2-predictors included age, gender, SES, migration background, the center, the disease, duration of the disease, and comorbidity.
Following a stepwise approach, we started calculating the null-model for each outcome to estimate the intracluster correlation (ICC) [43]. Subsequently, we added (i) level-1-predictors, (ii) level-2-predictors, and (iii) interaction terms (time × gender, time × age, gender × age, and time × gender × age) to each model. To strengthen the power of estimations, we finally excluded those interaction terms from our models, which had not been significant in any model. Predictors were included as fixed effects; only the time variable was additionally included as random effect (i.e., random slope). Moreover, we included intercepts as fixed and random effects in each model. As a fixed effect, the intercept represents an average score for the outcome, if scores in all predictors are fixed to zero (in a GLMM the corresponding log odd for the outcome is calculated). The random intercept was used to account for varying outcome scores across participants at baseline [43].
Prior to model calculations, we centered metric predictors (grand mean) and created dummy-coded variables indicating disease-groups asthma and diabetes using juvenile arthritis as reference category. Moreover, we replaced missing data using the Expectation–Maximization (EM)-algorithm (missing data rates for level-1-predictors ranged from 5.6% for mental health problems to 18.1% for disease control; data were complete for gender, age, disease groups, and the center, in remaining level-2-predictors missing data rates ranged from 0.3% for comorbidity to 19.4% for SES). Mechanisms of handling missing data differed for GLMMs compared to LMMs in the used software IBM SPSS 22 (due to different levels of measurement of the outcomes and modeling approaches [43, 44]). For running our Models A1 to D1 (GLMMs), we thus used our data set with replaced missing values in each variable; further, we conducted sensitivity analyses by rerunning each model over 15 data sets generated by multiple imputation (MI). For analyzing the metric VAS (Model E1), we used an LMM with full-information maximum-likelihood (FIML) estimation and a data set with replaced missing data only in level-2-predictors. Analyses were conducted using IBM SPSS 22. Prior to longitudinal analyses, we calculated corresponding logistic and linear regression analyses based only on baseline data.
Results
In the analyzed sample (n = 310), about half of the participants were female, and the majority of the participants had a medium SES (see Table 1).
Preliminary analyses
Distributions of EQ-5D-Y items (Table 2) indicated severe ceiling effects (compare [32]), which were most obvious for the item on self-care. Almost all participants reported no problems in self-care at baseline (98%). For remaining items, corresponding rates were lower (ranging from 69 to 90%); however, hardly any of the investigated children and adolescents (2% or less) chose the response option “a lot of problems” for any item. Item distributions based on follow-up data showed similar results. For subsequent analyses, we thus excluded the item on self-care and collapsed the highest response option for each remaining EQ-5D-Y item (0 = “no problems”; 1 = “some/a lot of problems”).
Item-inter correlations (at baseline) indicated small to moderate associations among EQ-5D-Y items ranging from r = .23 for mobility and anxiety/depression to r = .40 for mobility and pain/discomfort. For the current health state, moderate negative relationships were found with all investigated items ranging from r = − .35 for mobility to r = − .42 for pain/discomfort.
Predictors of HRQoL according to the EQ-5D-Y
Findings of logistic and linear regression models based only on baseline data are presented in the Online Resource 1 (Supplementary Tables 1–3). Focusing on longitudinal analyses, we started by calculating the null-models. Corresponding ICCs indicated that 30.9% of the variance in mobility, 30% of the variance in usual activities, 29.9% of the variance in pain/discomfort, and 28.4% of the variance in anxiety/depression could be explained by differences between individuals.
Results for the final Model A1 (Table 3) revealed significant effects of time, gender, and the interaction time by gender on mobility. The likelihood to experience mobility problems decreased over time only for boys; at the beginning of the study, boys were more likely, but with ongoing study duration girls became more likely to experience problems in mobility. Further, participants with good disease control were less likely to experience mobility problems than those with at least partly uncontrolled diseases. Additionally, health complaints were positively associated with mobility problems. Moreover, mobility problems were less likely for participants with diabetes than for those with juvenile arthritis, and a long duration of the disease (measured at baseline) was associated with no problems in mobility. Random effects for Model A1 revealed an unexplained residual variance, differing probabilities for problems in mobility at baseline across individuals (see effect for random intercept) and higher probabilities for problems in mobility associated with shorter intervals between measurement points (interaction effect for random intercept by random slope). Concerning Model B1, results indicated a systematic decrease of problems in usual activities over time (Table 3). Further, problems in usual activities were positively associated with health complaints over time, less likely for participants with diabetes compared to those with juvenile arthritis, as well as negatively associated with the duration of the disease (measured at baseline). Concerning random effects, results for Model B1 were similar to findings for Model A1. Further, for some effects wide Confidence Intervals occurred due to small subgroups (e.g., for migration background in Model A1). Results of sensitivity analyses supported findings for Models A1 to B1.
Concerning pain/discomfort (Model C1; see Table 4), effects were found for time as well as for the interactions of time by gender and gender by age. That is, over the duration of the study, the likelihood of experiencing pain or discomfort decreased for boys, but increased for girls; further, among younger participants, boys were more likely, whereas among older participants, girls were more likely to experience pain or discomfort. Additionally, problems in pain/discomfort were positively associated with health complaints and mental health problems (measured over time). Moreover, problems in pain/discomfort were more likely for participants with low SES (at baseline), and problems in pain/discomfort were less likely for participants with diabetes compared to those with juvenile arthritis. Results of Model D1 (Table 4) showed no systematic change in anxiety/depression over time. Positive associations were found for anxiety/depression with health complaints and mental health problems (measured over time). Random effects for Models C1 and D1 pointed in the same direction compared to random effects for Models A1 and B1. Sensitivity analyses supported our findings for Models C1 to D1.
For the self-reported health state according to the VAS, a proportion of 48.6% of the variance could be explained by differences between individuals. Results for Model E1 (Table 5) indicated no systematic change of the health state over time. Further, a good health state was positively associated with good disease control as well as negatively associated with health complaints and mental health problems (all predictors measured over time). Moreover, younger compared to older participants had a better health state. Finally, random effects revealed a significant residual variance as well as significantly differing baseline scores across individuals.
Finally, we reran our models using a reduced sample excluding children aged 7 years (n = 9). Results did not differ substantially from the findings presented above. Graphs (based on raw data) demonstrating the associations of EQ-5D-Y scores with health complaints and mental health problems are depicted in the Online Resource 2 (Supplementary Figs. 1–9).
Discussion
The aims of this study were to investigate effects of socio-demographic as well as disease- and health-specific predictors on HRQoL according to the EQ-5D-Y based on longitudinal data. Longitudinal analyses revealed associations between less health complaints and better HRQoL in all investigated domains. We further found age- and gender-specific effects as well as associations of better disease control, a longer duration of the disease and less mental health problems with better HRQoL.
We detected high ceiling effects for the EQ-5D-Y in line with former studies analyzing school-based and general population samples [7,8,9,10]. To our knowledge, research findings on the EQ-5D-Y so far were based on the three-level response format as also used in the present study. Future studies should use a five-level version of the EQ-5D-Y (corresponding to the EQ-5D-5L version of the adult measure [4]), which is currently under development and may show more variability (compare [45]). The VAS on the other hand shows a rather high individual variability. Overall, future studies (especially studies on healthy or chronically ill children and adolescents; compare [46]) may wish to administer additional HRQoL measures besides the EQ-5D-Y as long as the five-level version is not available.
Based on longitudinal data, we found disease-group-specific differences between children and adolescents with juvenile arthritis compared to those with diabetes in mobility, usual activities, and pain/discomfort. These disease-group-specific differences may reflect the specific symptoms of the investigated diseases. In juvenile arthritis, pain, functional limitations, and difficulties in symptom control as well as severe side-effects of the treatments may all contribute to a higher burden of the disease compared to diabetes.
Good disease control was associated with less problems in mobility and with a better overall health state corresponding to former research [29]. Further, the duration of the disease was negatively associated with mobility and usual activities. The latter finding may reflect that children and adolescents with a longer duration of their disease adapted to the chronic diseases over time, and may have adapted their evaluation of HRQoL according to their chronic disease (known as the well-being paradox [47]). Likewise, studies in clinical samples found good self-reported HRQoL even in children and adolescents with very severe chronic diseases (e.g., [48, 49]).
Health complaints were associated with each investigated domain of HRQoL and with the current health state in line with a study in a Swedish school-based sample [31]. However, some complaints as measured with the HBSC-SCL (including items on headache, stomach ache, back pain, sleeping difficulties, feeling down, irritable, nervous, and dizzy) mingle with symptoms of the investigated diseases. Moreover, mental health problems were associated with pain/discomfort and anxiety/depression as well as with the current health state in line with results of former clinical [16] and non-clinical studies [7,8,9,10]. However, bivariate analyses in non-clinical samples additionally revealed associations of mobility and usual activities with mental health problems, which we could not detect in our multivariate models. Future research may analyze these associations more detailed, but our findings may already underline the necessity to consider health complaints and mental health problems in treatments for children and adolescents with chronic diseases.
We detected a higher probability for pain/discomfort among participants with lower SES. This finding may indicate more resources and higher health literacy in more affluent compared to disadvantaged families (compare e.g., [50]). Further, we detected an interaction effect of age by gender on pain/discomfort. This result may reflect developmental changes over childhood and adolescence, which should be considered in the treatment of children and adolescents with chronic diseases.
For the VAS, our findings on age and mental health problems correspond to a study on Spanish children and adolescents with diabetes [16]. Overall, these findings underline the importance of influences of developmental changes and mental health on the health state of children and adolescents with chronic diseases.
We detected decreasing problems in usual activities over time; further, problems in mobility as well as in pain/discomfort decreased for boys, but increased for girls over time. These changes over time may partly be due to regular medical care study participants received in disease-specific consultation hours at the centers over study duration. However, the Kids-CAT study was an observational study, no systematic intervention was conducted and we did not control for treatments of participants prior to the study. Moreover, for all investigated domains of HRQoL a higher probability of problems was associated with shorter intervals between measurement points indicating that participants who were more burdened re-visited consultation hours at the centers a few days earlier than those less burdened.
This study has the following limitations. Our data only covered a period of six months. Additionally, our longitudinal data—especially parent-reports on mental health problems—may be affected by a recall bias, and we could not include further laboratory markers or control for the used medication. Future research may wish to investigate the EQ-5D-Y over a longer period, gather data consistently online, and include further (objective) medical data. Our analyses are only exploratory, we analyzed the same sample with five longitudinal models, and our data included some small subgroups and unbalanced disease groups. Future studies may confirm our findings.
To our knowledge, we present the first results on socio-demographic, disease- and health-specific predictors of HRQoL according to the items and the VAS of the EQ-5D-Y over time. Our study underlines the necessity of disease-specific treatments for children and adolescents with asthma, juvenile arthritis, and diabetes, which should consider developmental changes. Further, our results indicate that subjective health complaints and mental health problems should be considered in the care of the investigated children and adolescents. Future research should suggest administering the EQ-5D-Y with five instead of three response options, and investigating HRQoL over a longer period.
References
Rabin, R., & de Charro, F. (2001). EQ-5D: a measure of health status from the EuroQol Group. Annals of Medicine, 33(5), 337–343.
Knott, R. J., Black, N., Hollingsworth, B., & Lorgelly, P. K. (2017). Response-Scale Heterogeneity in the EQ-5D. Health Economics, 26(3), 387–394. https://doi.org/10.1002/hec.3313.
Nolan, C. M., Longworth, L., Lord, J., Canavan, J. L., Jones, S. E., Kon, S. S., et al. (2016). The EQ-5D-5L health status questionnaire in COPD: validity, responsiveness and minimum important difference. Thorax, 71(6), 493–500. https://doi.org/10.1136/thoraxjnl-2015-207782.
Devlin, N. J., & Brooks, R. (2017). EQ-5D and the EuroQol Group: Past, present and future. Applied Health Economics and Health Policy, 15(2), 127–137. https://doi.org/10.1007/s40258-017-0310-5.
Wille, N., Badia, X., Bonsel, G., Burstrom, K., Cavrini, G., Devlin, N., et al. (2010). Development of the EQ-5D-Y: A child-friendly version of the EQ-5D. Quality of Life Research, 19(6), 875–886. https://doi.org/10.1007/s11136-010-9648-y.
EuroQolResearchFoundation (2017). Development of the EQ-5D-Y: A child-friendly version of the EQ-5D. http://www.euroqol.org/eq-5d-products/eq-5d-y-youth.html. Accessed 17 October 2017 2017.
Ravens-Sieberer, U., Wille, N., Badia, X., Bonsel, G., Burstrom, K., Cavrini, G., et al. (2010). Feasibility, reliability, and validity of the EQ-5D-Y: results from a multinational study. Quality of Life Research, 19(6), 887–897. https://doi.org/10.1007/s11136-010-9649-x.
Jelsma, J. (2010). A comparison of the performance of the EQ-5D and the EQ-5D-Y health-related quality of life instruments in South African children. International Journal of Rehabilitation Research, 33(2), 172–177. https://doi.org/10.1097/MRR.0b013e32832bb0f7.
Burstrom, K., Bartonek, A., Brostrom, E. W., Sun, S., & Egmar, A. C. (2014). EQ-5D-Y as a health-related quality of life measure in children and adolescents with functional disability in Sweden: Testing feasibility and validity. Acta Paediatrica, 103(4), 426–435. https://doi.org/10.1111/apa.12557.
Robles, N., Rajmil, L., Rodriguez-Arjona, D., Azuara, M., Codina, F., Raat, H., et al. (2015). Development of the web-based Spanish and Catalan versions of the Euroqol 5D-Y (EQ-5D-Y) and comparison of results with the paper version. Health Qual Life Outcomes, 13, 72, https://doi.org/10.1186/s12955-015-0271-z.
Noyes, J., & Edwards, R. T. (2011). EQ-5D for the assessment of health-related quality of life and resource allocation in children: a systematic methodological review. Value Health, 14(8), 1117–1129. https://doi.org/10.1016/j.jval.2011.07.011.
Janssens, A., Rogers, M., Gumm, R., Jenkinson, C., Tennant, A., Logan, S., et al. (2016). Measurement properties of multidimensional patient-reported outcome measures in neurodisability: a systematic review of evaluation studies. Developmental Medicine & Child Neurology, 58(5), 437–451. https://doi.org/10.1111/dmcn.12982.
Bergfors, S., Astrom, M., Burstrom, K., & Egmar, A. C. (2015). Measuring health-related quality of life with the EQ-5D-Y instrument in children and adolescents with asthma. Acta Paediatrica, 104(2), 167–173. https://doi.org/10.1111/apa.12863.
Eidt-Koch, D., Mittendorf, T., & Greiner, W. (2009). Cross-sectional validity of the EQ-5D-Y as a generic health outcome instrument in children and adolescents with cystic fibrosis in Germany. Bmc Pediatrics. https://doi.org/10.1186/1471-2431-9-55.
Jonsson, M., Bergstrom, A., Egmar, A. C., Hedlin, G., Lind, T., & Kull, I. (2016). Asthma during adolescence impairs health-related quality of life. The Journal of Allergy and Clinical Immunology: In Practice 4(1), 144–146. https://doi.org/10.1016/j.jaip.2015.07.020.
Murillo, M., Bel, J., Perez, J., Corripio, R., Carreras, G., Herrero, X., et al. (2017). Health-related quality of life (HRQOL) and its associated factors in children with Type 1 Diabetes Mellitus (T1DM). Bmc Pediatrics, 17(1), 16. https://doi.org/10.1186/s12887-017-0788-x.
Ravens-Sieberer, U., & Europe, T. K. G. (2006). The KIDSCREEN Questionnaires. Quality of life questionnaires for children and adolescents—Handbook. Lengerich: Papst Science Publisher.
Meyer-Moock, S., Moock, J., Morgenroth, A., & Kohlmann, T. Comparing responsiveness of the child-friendly version of the EuroQol-questionnaire (EQ-5D-Y) with population specific instruments (KINDL-R and KIDSCREEN-10) in a clinical sample of children and adolescents. 28th Scientific Plenary Meeting of the EuroQol Group, Oxford, September 2011.
Klaassen, R. J., Krahn, M., Gaboury, I., Hughes, J., Anderson, R., Grundy, P., et al. (2010). Evaluating the ability to detect change of health-related quality of life in children with Hodgkin disease. Cancer, 116(6), 1608–1614. https://doi.org/10.1002/cncr.24883.
Varni, J. W., Burwinkle, T. M., Rapoff, M. A., Kamps, J. L., & Olson, N. (2004). The PedsQL™ in pediatric asthma: Reliability and validity of the Pediatric Quality of Life Inventory™ generic core scales and asthma module. Journal of Behavioral Medicine, 27(3), 297–318.
Ravens-Sieberer, U., & Bullinger, M. (1998). Assessing health-related quality of life in chronically ill children with the German KINDL: first psychometric and content analytical results. Quality of Life Research, 7, 399–407.
Varni, J. W., Limbers, C. A., & Burwinkle, T. M. (2007). Impaired health-related quality of life in children and adolescents with chronic conditions: a comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the PedsQL™ 4.0 Generic Core Scales. Health Qual Life Outcomes, 5(1), 43.
Wagner, V. M., Müller–Godeffroy, E., von Sengbusch, S., Häger, S., & Thyen, U. (2005). Age, metabolic control and type of insulin regime influences health-related quality of life in children and adolescents with type 1 diabetes mellitus. European Journal of Pediatrics, 164(8), 491–496.
Lundberg, V., Lindh, V., Eriksson, C., Petersen, S., & Eurenius, E. (2012). Health-related quality of life in girls and boys with juvenile idiopathic arthritis: self-and parental reports in a cross-sectional study. Pediatric Rheumatology, 10(1), 1.
Kalyva, E., Malakonaki, E., Eiser, C., & Mamoulakis, D. (2011). Health-related quality of life (HRQoL) of children with type 1 diabetes mellitus (T1DM): self and parental perceptions. Pediatric Diabetes, 12(1), 34–40.
Lawrence, J. M., Joyce, P., Black, M. H., Anderson, A., Hood, K., Imperatore, G., et al. (2012). Demographic and clinical correlates of diabetes-related quality of life among youth with type 1 diabetes. The Journal of Pediatrics, 161(2), 201–207. e202.
Hassan, K., Loar, R., Anderson, B. J., & Heptulla, R. A. (2006). The role of socioeconomic status, depression, quality of life, and glycemic control in type 1 diabetes mellitus. The Journal of Pediatrics, 149(4), 526–531.
Stahl-Pehe, A., Straßburger, K., Castillo, K., Bächle, C., Holl, R. W., Lange, K., et al. (2014). Quality of life in intensively treated youths with early-onset type 1 diabetes: a population-based survey. Pediatric Diabetes, 15(6), 436–443.
Everhart, R. S., & Fiese, B. H. (2009). Asthma severity and child quality of life in pediatric asthma: a systematic review. Patient Education and Counseling, 75(2), 162–168.
Naughton, M. J., Ruggiero, A. M., Lawrence, J. M., Imperatore, G., Klingensmith, G. J., Waitzfelder, B., et al. (2008). Health-related quality of life of children and adolescents with type 1 or type 2 diabetes mellitus: SEARCH for Diabetes in Youth Study. Archives of Pediatrics & Adolescent Medicine, 162(7), 649–657.
Svedberg, P., Eriksson, M., & Boman, E. (2013). Associations between scores of psychosomatic health symptoms and health-related quality of life in children and adolescents. Health and Quality of Life Outcomes, 11(1), 176.
Fischer, K., Barthel, D., Otto, C., Thyen, U., Klein, M., Walter, O., et al. Application of the EQ-5D-Y in a clinical study: How children and adolescents with chronic conditions value HRQoL. 22nd Annual Conference—International Society for Quality of Life Research, Vancouver, BC, October 2015.
Devine, J., Otto, C., Rose, M., Barthel, D., Fischer, F., Mülhan, H., et al. (2015). A new computerized adaptive test advancing the measurement of health-related quality of life (HRQoL) in children: the Kids-CAT. Quality of Life Research, 24(4), 871–884.
Barthel, D., Fischer, K. I., Nolte, S., Otto, C., Meyrose, A. K., Reisinger, S., et al. (2016). Implementation of the Kids-CAT in clinical settings: a newly developed computer-adaptive test to facilitate the assessment of patient-reported outcomes of children and adolescents in clinical practice in Germany. Quality of Life Research, 25(3), 585–594.
Barthel, D., Otto, C., Nolte, S., Meyrose, A.-K., Fischer, F., Devine, J., et al. (2017). The validation of a computer-adaptive test (CAT) for assessing health-related quality of life in children and adolescents in a clinical sample: study design, methods and first results of the Kids-CAT study. Quality of Life Research, 26, 1105–1117.
Lampert, T., Kroll, L. E., Müters, S., & Stolzenberg, H. (2013). Messung des sozioökonomischen Status in der Studie “Gesundheit in Deutschland aktuell” (GEDA). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz, 56(1), 131–143.
Lampert, T., Müters, S., Stolzenberg, H., Kroll, L. E., & Group, K. S. (2014). Messung des sozioökonomischen Status in der KiGGS-Studie. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz, 57(7), 762–770.
Schenk, L., Bau, A.-M., Borde, T., Butler, J., Lampert, T., Neuhauser, H., et al. (2006). Mindestindikatorensatz zur Erfassung des Migrationsstatus. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz, 49(9), 853–860.
Haugland, S., Wold, B., Stevenson, J., Aaroe, L. E., & Woynarowska, B. (2001). Subjective health complaints in adolescence: A cross-national comparison of prevalence and dimensionality. The European Journal of Public Health, 11(1), 4–10.
Ravens-Sieberer, U., Ottova, V., Hintzpeter, B., Hillebrandt, D., Saier, U., Moeller, N., et al. (2012). Gesundheitsverhalten von Kindern und Jugendlichen: Die WHO-Jugendgesundheitsstudie für Hamburg. [Health behaviour of children and adolescents: The WHO-youth health study for Hamburg (Germany)]. Lengerich: Pabst Verlag.
Goodman, R. (1997). The Strengths and Difficulties Questionnaire: a research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586.
Woerner, W., Becker, A., Friedrich, C., Klasen, H., Goodman, R., & Rothenberger, A. (2002). Normierung und Evaluation der deutschen Elternversion des Strengths and Difficulties Questionnaire (SDQ): Ergebnisse einer repräsentativen Felderhebung. [Normal values and evaluation of the German parents’ version of Strengths and Difficulties Questionnaire (SDQ): Results of a representative field study]. Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 30, 105–112.
Heck, R. H., Thomas, S. L., & Tabata, L. N. (2012). Multilevel modeling of categorical outcomes using IBM SPSS. New York: Routledge.
Heck, R. H., Thomas, S. L., & Tabata, L. N. (2014). Multilevel and longitudinal modeling with IBM SPSS (2nd edn.). New York: Routledge.
Chen, G., Flynn, T., Stevens, K., Brazier, J., Huynh, E., Sawyer, M., et al. (2015). Assessing the health-related quality of life of australian adolescents: An empirical comparison of the child health utility 9D and EQ-5D-Y instruments. Value in Health, 18(4), 432–438. https://doi.org/10.1016/j.jval.2015.02.014.
Scott, D., Ferguson, G. D., & Jelsma, J. (2017). The use of the EQ-5D-Y health related quality of life outcome measure in children in the Western Cape, South Africa: psychometric properties, feasibility and usefulness—a longitudinal, analytical study. Health Qual Life Outcomes. https://doi.org/10.1186/s12955-017-0590-3.
Ravens-Sieberer, U., Erhart, M., Wille, N., Wetzel, R., Nickel, J., & Bullinger, M. (2006). Generic health-related quality-of-life assessment in children and adolescents: methodological considerations. Pharmacoeconomics, 24(12), 1199–1220.
Landfeldt, E., Lindgren, P., Bell, C. F., Guglieri, M., Straub, V., Lochmuller, H., et al. (2016). Health-related quality of life in patients with Duchenne muscular dystrophy: a multinational, cross-sectional study. Developmental Medicine and Child Neurology, 58(5), 508–515. https://doi.org/10.1111/dmcn.12938.
Eiser, C., & Morse, R. (2001). Quality-of-life measures in chronic diseases of childhood. Health Technology Assessment, 5(4), 1–157.
Sanders, L. M., Shaw, J. S., Guez, G., Baur, C., & Rudd, R. (2009). Health literacy and child health promotion: implications for research, clinical care, and public policy. Pediatrics, 124 Suppl 3, S306–S314, https://doi.org/10.1542/peds.2009-1162G.
Acknowledgements
We thank all children, adolescents and their parents, who participated in the Kids-CAT study. Further, we thank the study nurses Anja Bünte and Andrea Knaak, as well as all involved pediatricians for their valuable contributions to the Kids-CAT project. Moreover, we thank Dr. Claus Barkmann for statistical advice, as well as all student assistants and interns for their support. The work on the present publication was financially supported by the EuroQol Foundation, but the views expressed by the authors in the present publication do not necessarily reflect the views of the EuroQol Group.
Funding
This Kids-CAT study was funded by the German Federal Ministry of Education and Research (Grant No. 0010-01GY1111). The present manuscript was funded by the EuroQol Research Foundation (EQ Project 2016270).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Otto, C., Barthel, D., Klasen, F. et al. Predictors of self-reported health-related quality of life according to the EQ-5D-Y in chronically ill children and adolescents with asthma, diabetes, and juvenile arthritis: longitudinal results. Qual Life Res 27, 879–890 (2018). https://doi.org/10.1007/s11136-017-1753-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-017-1753-8