
Abstract
Purpose
Social support does not always lead to health benefits; the outcomes depend on the match between the need and the provision of social support. Culture shapes individuals’ preference of social support types (e.g., supportive communication, social companionship, and tangible support). The present study examined how the association between social support and well-being may vary as a function of acculturation among minority cancer survivors.
Methods
One hundred and twenty-three Chinese American breast cancer survivors were invited to complete a questionnaire package.
Results
Findings showed that acculturation moderated the association of social support subtypes with psychological and physical well-being. Higher emotional/information support was associated with better quality of life and less physical symptoms among highly acculturated cancer survivors but more physical symptoms among those who were less acculturated. Tangible support was associated with more physical symptoms among highly acculturated cancer survivors but less physical symptoms among those who are less acculturated. Positive social interaction was associated with better quality of life and less physical symptoms among less acculturated cancer survivors but not associated with quality of life or physical symptoms among their highly acculturated counterparts.
Conclusion
The findings pointed to the significance of acculturation in breast cancer experience among minority women, especially its interplay with social support transactions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The health benefits of social support among cancer survivors have been broadly examined. Past studies showed that cancer survivors with adequate support from significant others reported better quality of life [1] and cancer progression [2, 3]. According to the stress-buffering hypothesis [4], social support can protect an individual from the pathogenic effects of a stressful event, which results in better physical health. This hypothesis has been well established and supported by daily diary study [5]. However, solicitation of social support often requires personal disclosure, which leads to an additional exposure to the stressors and hence emotional disturbance, especially in contexts where individuals find disclosure uncomfortable or inappropriate [6]. The optimal matching theory suggests that the outcomes of social support depend on the fit between the types of stress and the types of social support provided [7, 8]. Consistently, empirical studies found mismatched social support was associated with poor psychosocial adjustment among breast cancer survivors [9], and transactions of online emotional support were detrimental to those who were not comfortable with emotional disclosure [10].
Social support in the Asian culture
Cultural beliefs have significant influence on individuals’ attitudes toward social support. Compared with European Americans, Asian Americans tend to have more concern over the negative implications of social support on interpersonal relationships [11, 12]. Empirical studies showed that Asian American participants were relatively reluctant to seek social support to deal with their stressors [13]. Even when under extreme stressors such as cancer diagnosis, Asians tend to prioritize maintaining interpersonal harmony over gaining emotional support. Qualitative studies found Asian American breast cancer survivors seldom disclose their feelings in order to avoid causing emotional burden to their partners [14].
Notwithstanding cultural differences in the perception of social support, empirical studies showed social support was associated with better quality of life, more positive affect, and less negative affect among Asian American breast cancer survivors [15, 16]. These findings implied that these women may have better psychological outcomes when social support manifests in culturally appropriate ways [12]. Asians’ concern with utilizing social support mainly rests on its disclosing nature and consequential negative influences on interpersonal harmony [13, 17]; they may thus benefit more from social support types that do not involve disclosure or risk of disturbing relationships [12].
To discern the culturally appropriate ways of utilizing social support in the western and the Asian contexts, researchers proposed the concepts of explicit and implicit social support and distinguished them by the presence/absence of personal disclosure [18]. Explicit social support was defined as support that people can recruit from social networks through personal disclosure such as supportive communication, and implicit social support was defined as the emotional comfort people can obtain from social networks without disclosing their problems or stressors such as social companionship and behavioral manifestations of love [12]. In an experimental study, researchers found Asian Americans experienced more biological and psychological benefits from the implicit social support condition (i.e., think about a group that they were close to and then write about the significant aspects of that group) than those in the explicit social support condition (i.e., think about people to whom they were close and write a letter directly seeking advice and support for the upcoming experimental social stress tasks from one of these people) [18]. These findings were later replicated in a diary study in which Asian Americans experienced higher levels of life satisfaction when they used more implicit social support (i.e., had more people with whom they spent their time without disclosing their stressors, reminded themselves of people who love and care for them) [11].
Other than supportive communication (i.e., explicit social support) and social companionship (i.e., implicit social support), social support may manifest in other forms of behavior [19]. In Asian cultures that value relationship interdependence [20], tangible support is normative and welcomed [21]. It does not only help recipients to solve their problems but also convey affection and care [14, 21]. It is often viewed as a behavioral manifestation of emotional support. Although existing cross-cultural studies of social support were predominately conducted with college students, these findings are likely to extend to breast cancer survivors, such that Asian American breast cancer survivors would benefit more from implicit social support and tangible support than explicit social support.
Acculturation as a moderator
The majority of cross-cultural social support research emphasized the differences among ethnic groups, but few have examined within-group heterogeneity. Acculturation is the socialization process by which foreign-born individuals adopt the values, customs, norms, attitudes, and behaviors of the mainstream culture [22, 23]. Immigrants from the same heritage culture may have very diverse acculturation experience because of different degrees of contact with, and engagement in, the host culture [24]. For example, a Chinese American breast cancer survivor who recently emigrated from the mainland China and a Chinese American breast cancer survivor who immigrated to the USA in her early childhood are likely to have different degrees of acculturation.
With theoretical and empirical support of cultural differences in perceiving different types of social support, it is likely that these associations between social support types and well-being among Chinese American breast cancer survivors may vary across their levels of acculturation to the American society. Research showed European Americans tended to have higher levels of emotional expression and benefit more from explicit social support than Asian Americans [11, 18]. Consistently, more acculturated Chinese American immigrants reported higher levels of emotional expressivity than less acculturated counterparts [25], which might in turn increase their preference of explicit social support. On the other hand, the American culture places great value on autonomy and independence [20], and tangible support may sometimes be interpreted as intrusive acts, which implies the recipients as codependent or inefficacious in dealing with stressors [21]. In the same vein, highly acculturated Chinese American cancer survivors may also find tangible support intrusive. However, studies that examine the role of acculturation in the association between social support types and well-being among Asian American cancer survivors have been lacking.
Aims of the present study
The present study aimed to examine the associations of social support types (i.e., explicit social support, implicit social support, and tangible support) with psychological and physical well-being (i.e., quality of life and physical symptoms) and test the moderating role of acculturation in these associations. It was expected that implicit social support and tangible support would be positively associated with psychological and physical well-being among Chinese American breast cancer survivors. In addition, an interaction effect between acculturation and social support types on well-being was also expected, with the positive effect of explicit social support (i.e., emotional/informational support) more salient among highly acculturated breast cancer survivors, compared with implicit social support (i.e., positive social interaction, affectionate support) and tangible support.
Methods
Participants
One hundred and twenty-three Chinese breast cancer survivors were recruited. Their age ranged between 31 and 83 years old (M = 54.50, SD = 8.67). Among them, 55.3 % received college education or above, 72.1 % were married, 87.6 % were diagnosed with breast cancer at stage I–III, and the mean time since diagnosis was 21.35 months (SD = 12.51 months).
Procedure
The study procedure was approved by the institutional review board. The entire study was conducted in participants’ native language (i.e., Chinese). Participants were recruited from local Chinese American community organizations in California. This study was the baseline of a larger intervention study, and inclusion criteria included: (1) being diagnosed with breast cancer at stage 0–III within 5 years and (2) self-identified to be comfortable speaking, reading, and writing in Chinese. With indication of initial interest in the study, potential participants were contacted by community research to screen for eligibility over the phone. Upon informed consent, questionnaire packages were mailed to eligible individuals who agreed to participate in the study. Upon completion and return of the questionnaires (by mail), participants received monetary compensation (US$20).
Measures
Except for Functional Assessment of Cancer Therapy Breast which has an available Chinese version, all measures were translated into Chinese by a bilingual research team using the backward translation method and procedure [26]. One member translated the English items into Chinese, a second member back-translated the Chinese items into English, and a third member compared the back-translated English items with the original English items and made suggestions for item revision. The procedure was repeated until all Chinese items achieved equivalent meaning with the English items.
Social support
The 19-item Chinese version of the Medical Outcomes Study Social Support Survey [27, 28] was used to assess individuals’ levels of perceived availability of social support. Sample items are “someone to confide in or talk to about yourself or your problems (emotional/informational support, representing explicit social support and supportive communication in the this study),” “someone to have a good time with (positive social interaction, representing implicit social support and social companionship in this study),” “someone who hugs you (affectionate support, representing implicit social support and behavioral manifestations of love in this study),” and “someone to help with daily chores if you were sick (tangible support).” Participants rated on a five-point scale from (1) none of the time to (5) all of the time. In the present study, Cronbach’s alphas of the emotional/informational support, positive social interaction, affectionate support, and tangible support subscales are .95, .89, .88, and .92, respectively.
Acculturation
Five items with top factor loadings on “dominant society immersion” factor were extracted from the Stephenson Multigroup Acculturation Scale (SMAS; [29]) to measure individuals’ levels of acculturation to the dominant American society. Participants rated on a 4-point scale from (0) false to (3) true. The items were “I attend social functions with (Anglo) American people,” “I have many (Anglo) American acquaintances,” “I speak English at home,” “I think in English,” and “I know how to prepare American food.” In the present study, Cronbach’s alpha was .87.
Quality of life
Four subscales of the Chinese version of the Functional Assessment of Cancer Therapy Breast (FACT-B; [30]) were used to measure breast cancer survivors’ different facets of quality of life, including physical (e.g., “I have a lack of energy”), emotional (e.g., “I am losing hope in the fight against my illness), and functional well-being (e.g., “I am able to work”), as well as their other concerns about breast cancer (e.g., “One or both of my arms are swollen or tender,” reverse scored, and higher values refer to less concerns). Participants rated on a 5-point scale from (0) not at all to (4) extremely. In the present study, Cronbach’s alpha of the FACT-B subscales ranged from .71 to .90.
Physical symptoms
A modified version of the ten-item Physical Symptoms Checklist was used to measure the number of days during the last 30 days in which individuals have experienced symptoms of acute illness such as headache, chest pain, stiff/sore muscles, faintness/dizziness, and difficulty in breathing [31, 32]. It has been used among breast cancer survivors [33] and Asian college students [34] and was found to correlate with the number of medical appointments for cancer-related morbidities in a trial of expressive writing in breast cancer survivors [33]. In the present study, Cronbach’s alpha was .85.
Demographic information
Participants provided information about their demographic and medical characteristics such as age, education, annual household income, marital status, stage of breast cancer, and time since diagnosis (see Table 1).
Data analytic plan
Descriptive statistics and correlation analyses were conducted among variables of major interests (i.e., social support types, acculturation, quality of life, and physical symptoms). Associations between dependent variables (i.e., quality of life and physical symptoms) and demographic variables were also examined to identify potential covariate(s) to be controlled for in later analysis. For hypothesis testing, hierarchical linear regressions were conducted to examine the moderating effect of acculturation in the association between social support types and well-being (i.e., quality of life and physical symptoms).
Results
Descriptive statistics and correlations
Descriptive statistics and correlations among all of the examined variables were examined. Given the scores of physical symptoms were positively skewed (skewness = 1.59), as a common practice, log transformation was applied to the scores, and the transformed scores were used in analyses [34]. Correlation results showed that quality of life was significantly associated with all social support subtypes (rs ranged from .39 to .55, ps < .01), while physical symptoms were significantly associated with positive social interaction only (r = − .35, p < .01 see Table 2). Positive social interaction tended to have stronger associations with quality of life and physical symptoms (rs of ranged from −.16 to .39) than emotional/informational support (rs ranged from −.29 to .45, ps < .01).
Correlations and Chi-square tests were also conducted to examine the association of dependent variables with demographic and medical variables. The demographic and medical variables were not significantly associated with quality of life or physical symptoms (ps > .05) except for education level and stage of breast cancer (ps < .01). These two variables were used as covariates in the later regression analyses.
Regression analysis
To examine the moderating effect of acculturation in the association between social support types and well-being (i.e., quality of life and physical symptoms), regression analysis was carried out based on the procedures recommend by Aiken and West [35]. The predictor (i.e., social support types) and moderator (i.e., acculturation) variables were centered before computing the interaction terms. In the regression model, covariates (i.e., education level, stage of breast cancer) were entered as the first step, followed by independent variables (i.e., social support types and acculturation) as the second step, and the interaction terms as the final step. The predictor, moderator, and interaction variables in regression analysis were checked for multicollinearity, and none showed a variance inflation factor (VIF) of ten or greater.
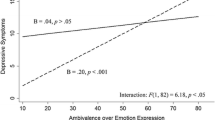
In accordance with the hypothesis, significant interaction effects were found between social support types and acculturation on different facets of quality of life (i.e., physical well-being, emotional well-being, and other concerns about breast cancer) and physical symptoms (see Table 3; Fig. 1). Unexpectedly, the interaction effect between all social support types and acculturation was not significant on functional well-being. Also, the main effect of affectionate support and its interaction effect with acculturation on different facets of quality of life and physical symptoms were not significant (see Table 3).

Interaction between social support subtypes and acculturation on physical symptoms and different facets of quality of life. Note EIS—emotional/informational support, PSI—positive social interaction, TS—tangible support
As recommended by Aiken and West [35], simple slope tests were conducted to follow up the significant interaction effects. The dependent variables were regressed on the predictors (i.e., social support types) at specific values of the moderator (high vs. low acculturation: 1 SD above vs. below the mean). The standardized coefficients (β) of predictors are presented as follows: Higher emotional/information support was associated with better physical well-being (β = .84, p < .05) and less physical symptoms (β = −1.49, p < .001) among those highly acculturated but worse physical well-being (β = −.53, p = .05) and more physical symptoms (β = 1.14, p < .001) among less acculturated cancer survivors. Also, higher emotional/information support was associated with better emotional well-being (β = .85, p < .05) and less other concerns about breast cancer (β = 1.06, p < .01) among those highly acculturated, but not among those who were less acculturated (emotional well-being: β = −.01, p = .97; other concerns: β = −.42, p = .11).
Opposite pattern appeared for positive social interaction and tangible support. Positive social interaction was significantly associated with better physical well-being (β = .82, p < .001), better emotional well-being (β = .90, p < .001), less other concerns about breast cancer (β = .60, p < .01) and less physical symptoms (β = −.70, p < .05) among less acculturated cancer survivors, but not among those who were highly acculturated (physical well-being: β = .09, p = .78; emotional well-being: β = −.41, p = .22; other concerns: β = .06, p = .84; physical symptoms: β = .25, p = .52). Similarly, tangible support was associated with less physical symptoms among those who were less acculturated (β = −.50, p < .05) but more physical symptoms among highly acculturated counterparts (β = .57, p < .05).
Discussion
The present study is one of the first attempts to examine how the relationships between social support types and well-being among Chinese American breast cancer survivors and how these associations may vary as a function of individuals’ levels of acculturation. Social support is perceived differently across cultures, and it is most effective when it manifests in a way that is consistent with the cultural expectation [36]. The findings are consistent with previous literature on the cultural differences in social support among healthy young adults that Asians/Asian American participants tended to favor implicit social support over explicit social support [11, 18]. In the present study, we found that positive social interaction (representing implicit social support and social companionship) tended to have stronger associations with physical symptoms and quality of life than emotional/informational support among Chinese American breast cancer survivors.
In addition, results showed the differences in the associations between social support types and well-being between highly acculturated and less acculturated Chinese American breast cancer survivors resemble the cultural differences found between Asians/Asian Americans and European Americans. Specifically, among highly acculturated Chinese American breast cancer survivors, emotional/informational support (representing explicit social support) was positively associated with well-being, while tangible support was associated with worse well-being. Highly acculturated Chinese American breast cancer survivors, similar to many European American counterparts, may place significance on self-expression and independence. Supportive communication that allows people to freely express their thoughts and feelings may be more preferred, over tangible support which may encroach upon recipients’ sense of personal agency [21].
Conversely, non-verbal, indirect behavioral manifestations of social support, such as providing social companionship or tangible assistance [18, 21], are more adaptive in Asian cultures. Less acculturated Chinese American breast cancer survivors are likely to endorse Chinese values of emotional suppression and relationship interdependence [37]. They may have concern that utilizing explicit social support would burden others and disrupt interpersonal harmony. Considering the cost of emotional disclosure may outweigh its benefits [38, 39], they may appreciate and benefit more from positive social interaction and tangible support, over explicit social support.
Our hypotheses regarding the moderation effect of acculturation in the associations between social support types and well-being were largely confirmed, with the exception of affective support. Affectionate support was not significantly related to physical or psychological well-being, regardless of cancer survivors’ levels of acculturation. The null association may be attributed to cultural irrelevance of the affectionate support measure, which focuses on direct expression of affection, e.g., shows you love and affection, loves and makes you feel wanted, and hugs you. These supportive actions may be considered as foreign and too explicit for Chinese Americans who are emotionally restrained [40].
Implications
Social support could be detrimental if it does not match with the recipient’ expectation [9, 41] and their cultural values [11, 18, 21]. The present study demonstrated the importance of considering individuals’ levels of acculturation in social support provision. Findings of the present study may have implications on facilitating cross-generational interaction in immigrant families of cancer survivors. Due to different degrees of acculturation across generations, children and cancer survivors may have different perception toward social support. For instance, a US-born and raised daughter may think emotional expression could benefit her immigrant mother with breast cancer, and encourages her mother to talk about her cancer experience. However, the mother may find emotional disclosure uncomfortable, and she actually wants and needs social companionship or tangible assistance. This mismatch in the need and the provision of social support can lead to maladjustment in cancer survivors.
The findings may also have implications at the community level. It is generally beneficial that healthcare professionals and community workers have increased cultural sensitivity when providing services to cancer survivors with diverse ethnic backgrounds. However, if service providers neglect cancer survivors’ individual acculturation levels, the problem of incompatible expectation about social support between support providers and recipients may remain. Highly acculturated cancer survivors may perceive culturally sensitive adaptation as a stereotypical act and become reluctant to seek support from the local American network. At the same time, they may not have support from their heritage network. Not able to receive adequate social support from either the American network or the heritage network, their well-being may suffer as a result. Therefore, care providers should pay attention to cancer survivors’ levels of acculturation and have clear communication with them on the expectation and appropriateness of social support.
Limitations and future directions
The present study was subject to several limitations. Only Chinese American breast cancer survivors were included in the present study, which limits the generalizability of the findings. Future research should examine this moderation model with samples of greater diversity (e.g., ethnicity, gender, and cancer types). Also, causality of the relationships cannot be drawn because the present study was correlational. It is possible that the relations between social support and physical/psychological outcomes are bidirectional, such that people who have poorer physical health may receive more social support, which in turn influence their psychological health. Future studies may replicate the present study with a longitudinal research design to examine the direction of associations. Furthermore, the present study examined acculturation as a unidimensional continuum instead of a bidimensional process. Instead of endorsing either the American culture or the Asian culture, it is possible that some immigrant cancer survivors would endorse both cultures or endorse none of these cultures [23]. Future research should investigate how enculturation (i.e., retention or cultural socialization to one’s heritage culture) [42, 43] may interact with acculturation, and how individuals who endorse both or none of the American and/or Chinese cultures may respond differently to explicit and implicit social support.
References
Montazeri, A. (2008). Health-related quality of life in breast cancer patients: A bibliographic review of the literature from 1974 to 2007. Journal of Experimental and Clinical Cancer Research, 27(1), 27–32. doi:10.1186/1756-9966-27-32.
Cousson-Gelie, F., Bruchon-Schweitzer, M., Dilhuydy, J. M., & Jutand, M. A. (2007). Do anxiety, body image, social support and coping strategies predict survival in breast cancer? A ten-year follow-up study. Psychosomatics, 48, 211–216.
Reynolds, P., Boyd, P. T., Blacklow, R. S., Jackson, J. S., Greenberg, R. S., Austin, D. F., et al. (1994). The relationship between social ties and survival among black and white breast cancer patients. National Cancer Institute Black/White Cancer Survival Study Group. Cancer Epidemiology, Biomarkers and Prevention, 3, 253–259.
Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310–357.
Stein, R. R., & Smith, B. W. (2015). Social support attenuates the harmful effects of stress in healthy adult women. Social Science and Medicine, 146, 129–136.
Hobfoll, S. E., & London, P. (1986). The relationship of self-concept and social support to emotional distress among women during war. Journal of Social and Clinical Psychology, 4(2), 189–203. doi:10.1521/jscp.1986.4.2.189.
Cutrona, C. E. (1990). Stress and social support: In search of optimal matching. Journal of Social and Clinical Psychology, 9(1), 3–14.
Cutrona, C., & Russell, D. (1990). Type of social support and specific stress: Toward a theory of optimal matching. In B. R. Sarason, I. G. Sarason, & G. R. Pierce (Eds.), Social support: An interactional view (pp. 319–366). Oxford, England: Wiley.
Reynolds, J. S., & Perrin, N. A. (2004). Mismatches in social support and psychosocial adjustment to breast cancer. Health Psychology, 23(4), 425–430. doi:10.1037/0278-6133.23.4.425.
Yoo, W., Namkoong, K., Choi, M., Shah, D. V., Tsang, S., Hong, Y., et al. (2014). Giving and receiving emotional support online: Communication competence as a moderator of psychosocial benefits for women with breast cancer. Computers in Human Behavior, 30, 13–22. doi:10.1016/j/chb.2013.07.024.
Kim, H. S., & Chiu, T. Q. (2010). Cultural variation in the motivation of self-expression. In D. Dunning (Ed.), Social motivation (pp. 57–78). New York: Taylor & Francis.
Kim, H. S., Sherman, D. K., & Taylor, S. E. (2008). Culture and social support. American Psychologist, 63(6), 518–526. doi:10.1037/0003-066X.
Taylor, S. E., Sherman, D. K., Kim, H. S., Jarcho, J., Takagi, K., & Dunagan, M. S. (2004). Culture and social support: Who seeks it and why? Journal of Personality and Social Psychology, 87(3), 354–362. doi:10.1037/0022-3514.87.3.354.
Kagawa-Singer, M., & Wellisch, D. K. (2003). Breast cancer patients’ perceptions of their husbands’ support in a cross-cultural context. Psycho-Oncology, 12(1), 24–37. doi:10.1002/pon.619.
Wen, K. Y., Fang, C. Y., & Ma, G. X. (2014). Breast cancer experience and survivorship among Asian Americans: A systematic review. Journal of Cancer Survivorship, 8(1), 94–107. doi:10.1007/s11764-013-0320-8.
You, J., & Lu, Q. (2014). Sources of social support and adjustment among Chinese cancer survivors: Gender and age differences. Supportive Care in Cancer, 22(3), 697–704. doi:10.1007/s00520-013-2024-z.
Kim, H. S., Sherman, D. K., Ko, D., & Taylor, S. E. (2006). Pursuit of comfort and pursuit of harmony: Culture, relationships, and social support seeking. Personality and Social Psychology Bulletin, 32(12), 1595–1607. doi:10.1177/0146167206291991.
Taylor, S. E., Welch, W. T., Kim, H. S., & Sherman, D. K. (2007). Cultural differences in the impact of social support on psychological and biological stress responses. Psychological Sciences, 18(9), 831–837. doi:10.1111/j.1467-9280.2007.01987.x.
Kang, S., Shaver, P. R., Sue, S., Min, K., & Jing, H. (2003). Culture-specific patterns in the prediction of life satisfaction: Roles of emotion, relationship quality, and self-esteem. Personality and Social Psychology Bulletin, 29(12), 1596–1608.
Markus, H. R., & Kitayama, S. (1991). Culture and the self: Implications for cognition, emotion, and motivation. Psychological Review, 98(2), 224–253.
Chen, J. M., Kim, H. S., Mojaverian, T., & Morling, B. (2012). Culture and social support provision: Who gives what and why. Personality and Social Psychology Bulletin, 38(1), 3–13. doi:10.1177/0146167211427309.
Choi, S., Rankin, S., Stewart, A., & Oka, R. (2008). Effects of acculturation on smoking behavior in Asian Americans. Journal of Cardiovascular Nursing, 23(1), 67–73.
Yoon, E., Chang, C., Kim, S., Clawson, A., Cleary, S. E., Meghan, H., et al. (2013). A meta-analysis of acculturation/enculturation and mental health. Journal of Counseling Psychology, 60(1), 15–30.
Miller, M. J. (2007). A bilinear multidimensional measurement model of Asian American acculturation and enculturation: Implications for counseling interventions. Journal of Counseling Psychology, 54(2), 118–131. doi:10.1037/0022-0167.54.2.118.
Chen, S. J., Zhou, Q., Main, A., & Lee, E. H. (2015). Chinese American immigrant parents’ emotional expression in the family: Relations with parents’ cultural orientations and children’s emotion-related regulation. Cultural Diversity and Ethnic Minority Psychology, 21(4), 619–629. doi:10.1037/cdp0000013.
Brislin, R. W. (1970). Back translation for cross-cultural research. Journal of Cross Cultural psychology, 1(3), 185–216. doi:10.1177/135910457000100301.
Sherbourne, C. D., & Stewart, A. L. (1991). The MOS social support survey. Social Science and Medicine, 32(6), 705–714. doi:10.1016/0277-9536(91)90150-B.
Yu, D. S. F., Lee, D. T. F., & Woo, J. (2004). Psychometric testing of the Chinese version of the medical outcomes study social support survey (MOS-SSS-C). Research in Nursing and Health, 27(2), 135–143. doi:10.1002/nur.20008.
Stephenson, M. (2000). Development and validation of the Stephenson Multigroup Acculturation Scale (SMAS). Psychological Assessment, 12(1), 77–88. doi:10.1037/1040-3590.12.1.77.
Wan, C., Zhang, D., Yang, Z., Tu, X., Tang, W., Feng, C., et al. (2007). Validation of the simplified Chinese version of the FACT-B for measuring quality of life for patients with breast cancer. Breast Cancer Research and Treatment, 106(3), 413–418. doi:10.1007/s10549-007-9511-1.
Pennebaker, J. W. (1982). The psychology of physical symptoms. New York: Springer.
King, L. A., & Emmons, R. A. (1990). Conflict over emotional expression: Psychological and physical correlates. Journal of Personality and Social Psychology, 58(5), 864–877.
Stanton, A. L., Danoff-Burg, S., Sworowski, L. A., Collins, C. A., Branstetter, A. D., Rodriguez-Hanley, A., et al. (2002). Randomized, controlled trial of written emotional expression and benefit finding in breast cancer patients. Journal of Clinical Oncology, 20(20), 4160–4168.
Lu, Q., & Stanton, A. L. (2010). How benefits of expressive writing vary as a function of writing instructions, ethnicity and ambivalence over emotional expression. Psychology and Health, 25(6), 669–684. doi:10.1080/08870440902883196.
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Newbury Park, CA: Sage.
Kim, H. S. (2010). Culture and self-expression. http://www.apa.org/science/about/psa/2010/06/sci-brief.aspx.
Wei, M. F., Su, J. C., Carrera, S., Lin, S. P., & Yi, F. (2013). Suppression and interpersonal harmony: A cross-cultural comparison between Chinese and European Americans. Journal of Counseling Psychology, 60(4), 625–633.
Kim, H. S., & Markus, H. R. (2002). Freedom of speech and freedom of silence: An analysis of talking as a cultural practice. In R. Shweder, M. Minow, & H. R. Markus (Eds.), Engaging cultural differences: The multicultural challenge in liberal democracies (pp. 432–452). New York: Russell Sage Foundation.
Soto, J. A., Perez, C. R., Kim, Y. H., Lee, E. A., & Minnick, M. R. (2011). Is expressive suppression always associated with poorer psychological functioning? A cross-cultural comparison between European Americans and Hong Kong Chinese. Emotion, 11(6), 1450–1455. doi:10.1037/a0023340.
Wilkins, R., & Gareis, E. (2006). Emotion expression and the locution “I love you”: A cross-cultural study. International Journal of Intercultural Relations, 30(1), 51–75. doi:10.1016/j.ijintrel.2005.07.003.
Helgeson, V. S., Cohen, S., Schulz, R., & Yasko, J. (2000). Group support interventions for women with breast cancer: Who benefits from what? Health Psychology, 19(2), 107–114. doi:10.1037/0278-6133.19.2.107.
Berry, J. W. (1994). Acculturation and psychological adaptation: An over-view. In A. Bouvy, F. J. R. Van de Vijver, P. Boski, & P. Schmitz (Eds.), Journeys into cross-cultural psychology (pp. 129–141). Berwyn, PA: Swets & Zeitlinge.
Kim, B. S. K., Atkinson, D. R., & Umemoto, D. (2001). Asian cultural values and the counseling process: Current knowledge and directions for future research. The Counseling Psychologist, 29(4), 570–603.
Funding
Dr. Qian Lu’s effort was supported by American Cancer Society MRSGT-10-011-01-CPPB (PI: Qian Lu) and National Cancer Institute R01 CA180896-01A1 (PI: Qian Lu).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Wong, C.C.Y., Lu, Q. Match between culture and social support: Acculturation moderates the relationship between social support and well-being of Chinese American breast cancer survivors. Qual Life Res 26, 73–84 (2017). https://doi.org/10.1007/s11136-016-1362-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-016-1362-y