
Abstract
Purpose
The aim of this study was to examine the impact of demographic and cultural factors on health preferences among Chinese general population.
Methods
The Chinese EQ-5D-5L valuation study was conducted between December 2012 and January 2013. A total of 1296 participants were recruited from the general public at Beijing, Chengdu, Guiyang, Nanjing, and Shenyang. Each participant was interviewed to measure preferences for ten EQ-5D-5L health states using composite time trade-off and seven pairs of states using discrete choice experiment (data were not included in this study). At the end of the interview, each participant was also asked to provide their demographic information and answers to two questions about their attitudes towards whether bad living is better than good death (LBD) and whether they believe in an afterlife. Generalized linear model and random effects logistic models were used to examine the impact of demographic and cultural factors on health preferences.
Results
Participants who had serious illness experience received college or higher education, or agree with LBD were more likely to value health states positively and have a narrower score range. Participants at Beijing were more likely to be non-traders, value health states positively, less likely to reach the lowest possible score, and have narrower score range compared with all other four cities after controlling for all other demographic and culture factors.
Conclusions
Health state preference is significantly affected by factors beyond demographics. These factors should be considered in achieving a representative sample in valuation studies in China.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
“Preference refers to the set of assumptions related to ordering some alternatives, based on the degree of satisfaction, enjoyment or utility they provide, a process which results in a real or imagined optimal choice [1]”. Health preference is the preference towards a particular health state or outcome. Values and utilities are types of measurements of the preference for a specific health state or health outcome, which are measured under certainty and uncertainty, respectively [2]. As the results of assessment of health outcome, preference-based health utilities or values are used to calculate quality-adjusted life years (QALY) in economic evaluation which generates a compelling evidence for health policy decision-making.
Factors affecting health preferences have been extensively studied and reported in the literature. The majority of studies explored differences in health preferences by demographic factors including sex, age, ethnicity, race, and religion [3–8]. A recent study showed that compared with mainland Chinese, Singaporean Chinese were more likely to value extremely poor EuroQol Five-Dimension Five-Level Questionnaire (EQ-5D-5L) health states as worse than death [3]. Another study showed that Chinese, Malays, and Indians in Singapore had similar preferences for Health Utilities Index Mark 3 health states [9]. A study found that older adults or Hispanics preferred to reduce lifespan over depression, anxiety, and fatigue compared with younger adults or non-Hispanics, respectively [4], while Asians were found to be more likely to have higher preferences than the Whites for same health states among the US population [6]. However, little is known about factors affecting health preferences in China.
View on life and death has been an important part of the Chinese culture since ancient times. There’s a famous old Chinese saying, “bad living is better than a good death (LBD)”, which reflects the Chinese people’s desire for survival and endurance for suffering. Here the “bad living” not only includes the poor health status, but also includes the bad environment and social relation [10]. Living means hope, and death means nothing. However, influenced by the Buddhism and Taoism, a lot of Chinese people also believe in afterlife (AL) for thousands of years. More recently, “good death” has been discussed in related to euthanasia and end of life care [11]. An American study showed that patient’s attitudes towards the “bad living” and “good death” had a significant correlation with their preferences for the severe side effects of treatment for melanoma [12]. No study on the relationship between LBD and AL and time trade-off (TTO) values has been studied. Therefore, we were interested in how participants’ view on life and death distributed, and how their view impacted their health state preference in China.
The primary objective of the present study was to identify demographic and cultural factors that affect health preferences in China.
Methods
The instrument
The EuroQol Five-Dimension Questionnaire (EQ-5D) is widely used as an indirect measure of health utilities. It measures health status in five dimensions, including mobility, self-care, usual activities, pain/discomfort, and anxiety/depression with three-level response options for no, some, and extreme problems. A new version which keeps the same five dimensions but with five-level response options to reflect no, slight, moderate, severe, and extreme problems was recently developed (called the EQ-5D-5L) [13, 14]. We used selected health states defined by the EQ-5D-5L.
The China EQ-5D-5L valuation study
Overview
The China EQ-5D-5L valuation study was to develop a value set based on the societal preference for China. The main preference elicitation techniques were the composite time trade-off (cTTO) and discrete choice experiment (DCE). This study was conducted from November 2012 to January 2013 and was carried out in five cities of the mainland China including Beijing, Chengdu, Guangzhou, Nanjing, and Shenyang [15]. Data were collected through face-to-face interviews facilitated by a computerized survey software, the EuroQol Group’s Valuation Technology (EQ-VT) developed by the EuroQol Group [16].
This present study only used the cTTO data and demographic information from the China EQ-5D-5L valuation study. The development of EQ-5D-5L value set among Chinese population is still ongoing.
Sampling
Participants were randomly recruited from the streets and general public places in the five cities using quota sampling in terms of age, sex, and educational level according to the Sixth National Population Census [17]. Within each city, respondents were recruited from at least five different administrative districts. The recruitment sites included: (1) library, hospital, university, and other institutions; (2) community and park; and (3) shopping street (or mall) and restaurant.
Participant inclusion criteria were as follows: (1) age of 16 years old or older; (2) without any cognitive impairment and not currently experiencing serious illness; (3) able to read and communicate in mandarin; and (4) without serious vision and hearing problems. No more than one person per household was interviewed.
The sample size was determined according to a multi-country pilot study conducted by the EuroQol group followed the international EQ-5D-5L valuation protocol [16].
Health state selection
Health states were selected for cTTO section and DCE section, based on the results from the multi-country pilot study [16, 18]. A total of 86 health states were selected for the cTTO section. These health states were blocked into ten groups with each having ten states. One of the five very mild states with only one dimension at level 2 (i.e. 21111, 12111, 11211, 11121, 11112) and the worst state with all the five dimensions at level 5 (i.e. 55555) were included in every group. For DCE section, 196 pairs of EQ-5D-5L health states were randomly assigned into 28 blocks with seven pairs within each block. Each participant was randomly assigned a block number, and the health states/pairs within each block were presented in a random order.
Preference elicitation techniques
The cTTO uses the traditional TTO for states better than dead and the lead time TTO (LT-TTO) for states worse than dead. The cTTO starts with 10 years in full health and then die (Life A) or 10 years in the state being valued and then die (Life B). For health states better than dead, participants are asked to trade-off time in Life A in order to avoid living in Life B until they consider there is no difference between Life A and Life B. For severe health states, participants may trade-off all 10 years in Life A and still prefer Life A. If this was the case, the participant was presented the LT-TTO with 10-year lead time in full health and then die (Life A) or 10-year lead time in full health followed by 10 years in the state being valued and then die (Life B). Then, participants can keep on trading off time in Life A until they consider Life A and Life B are about the same. Health utility is calculated using (X − 10)/10 where X is the number of years in Life A at which participants considered the two options are about the same. The cTTO-derived health utilities ranged from −1 to 1.
DCE presented two EQ-5D-5L health states to participants at a time, and let participants to image living in each of the two states and choose the better one. This paper reports the findings using the cTTO data only.
The interview process
Through face-to-face interview, each participant was explained the purpose of the study. Participants were firstly asked to evaluate their current health status using the EQ-5D-5L. In order to help participants understand the procedure of cTTO, a wheelchair example was first demonstrated followed by valuation of ten hypothetical EQ-5D-5L health states. After the cTTO task completed, participants were asked whether they agree that it is easy to understand the cTTO questions, decide the indifferent point, and tell the difference between EQ-5D-5L health states. A supplemental questionnaire was designed to collect demographic and cultural information at the end of the interview. We asked two cultural-related questions: whether agree with LBD and whether believe in AL. Participants can choose from “strongly agree”, “somewhat agree”, “somewhat disagree”, and “strongly disagree” for LBD question. Four options were provided for the AL question, “there will be a happy afterlife”, “there will be an afterlife, but not sure whether happy or not”, “I don’t know if there will be an afterlife or not”, and “nobody will have an afterlife”.
Training and quality control
A total of 31 interviewers attended an eight-hour training session which covered introduction of the EQ-5D-5L and the cTTO and DCE, explanations for possible questions, as well as mock interviews conducted between interviewers. After training, each interviewer was asked to finish at least two interviews with strangers to practice the interview skills as a pilot test. Throughout the data collection, two study coordinators downloaded the interview data sheet and analysed it on a daily basis. Interviews ended before completing the TTO session were considered incomplete.
Statistical analysis
This study aimed to investigate the participants’ behaviour in responding to health preference questions and what factors might affect their responses. Specifically, we used four indicators: (a) whether or not a health state is valued at 1 which indicates that participants are not willing to trade-off life to avoid living in an impaired state (i.e. non-trader, model 1); (b) whether a health state is valued positively or negatively (model 2); (c) whether or not a health state is valued at −1 which is the lowest possible cTTO value that can be observed using the cTTO (model 3); and (d) the difference between the highest and lowest cTTO scores valued by each participants (i.e. the cTTO score range, model 4). We did not use actual utility values as these are primarily determined by the severity of the health states.
The factors included as explanatory variables were demographics such as age, gender, education, employment, residence, health insurance, and serious diseases experience as well as the responses to LBD and AL questions. There was no specific definition or explanation of “serious disease”. If participants asked for the definition, the standard answer was “please answer the question according to your own understanding”.
Since distribution of cTTO score range was non-normal, and the residues did not meet the basic assumption of homogeneity of variance, generalized linear regression model (GLM) with identity link function was used to examine the impact of the factors on the score range. Since each participant valued ten health states, random effects (RE) logistic regression models were used to assess the impact of the factors on health state preference (i.e. non-trading, positively, or reaching the lowest possible score). All statistical analyses were conducted with two-tailed test at significance level of 5 % in STATA 12.0 (StataCorp LP, Texas, USA).
Results
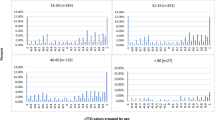
A total of 1328 participants were recruited and interviewed in the valuation study with a response rate of 68.4 % (1942 individuals were approached). Among all the recruited participants, 32 did not complete the interview and were excluded from the analysis. For the 1296 completed interviews (without any missing value), the mean interview time was 31.9 min (range 17.0–68.6 min). The mean (standard deviation) age was 42.3 (16.2) years, with 49.85 % female, 65.05 % urban residents, and 29.48 % full-time employed. The demographics and responses to LBD and AL questions are shown in Table 1. There were significant differences in proportions of participants living in urban areas, with high school or lower education, full-time employed, and covered by national health insurances between the five cities (Table 1). Compared to the Chinese general population, the study sample had higher proportions of people with college or higher education, unemployed, and living in urban area [17, 19]. Figures 1, 2, and 3 show the histograms of all cTTO scores grouped by cities, attitudes towards LBD and AL. Participants from Beijing or who agreed with LBD had less health states valued as −1 than participants from other four cities or disagreed with LBD.

Distribution of cTTO values grouped by city

Distribution of cTTO values grouped by belief in LBD. LBD bad living is better than good death

Distribution of cTTO values grouped by belief in AL. AL afterlife. a Belief in AL, b don’t know if there’s an AL or not, c nobody will have an AL
Table 2 shows the GLM and RE logistic regression results. Participants with college or higher education were more likely to be non-traders, value states positively, and have narrower score range. Participants experienced serious diseases (either by themselves or through taking care of others who had serious diseases) were also more likely to value health states positively. Compared with the other four cities, the participants from Beijing were more likely to be non-traders, value health states positively, and less likely to reach the lowest possible score, and their cTTO score range was narrower after controlling for all other factors considered in the model.
Participants who either strongly or somewhat agreed with LBD were more likely to be non-trader, value health states positively, and less likely to reach the bottom of the score scale compared with those who disagreed with LBD. Also, the difference between the highest and lowest values was also significantly smaller among those who agreed with LBD. Compared with those who believed “nobody will have an AL”, participants who believed AL (whether the AL will be happy or not) were more likely to value health states positively. The effects from the belief in LBD and AL remained significant even after controlling for all other variables in a single model.
Discussion
This study investigated the impact of demographic and cultural factors on health state preferences. We found that participants who receive college or higher education or live in Beijing exhibited more positive attitude in health state preference. It is also interesting to reveal that participants’ view on life and death has a significant impact on their health state preference after controlling for demographic factors. These factors that are associated with more positive state preference are also associated with significantly narrower score range which implies the larger incremental cost-effectiveness ratio in economic evaluation, everything else equal.
It seems there is no disagreement on achieving a representative sample in deriving a population-based value set to support resource allocation decision-making. However, the challenge is what defines “representativeness”. Different jurisdictions might have to understand their local population and cultural characteristics in the context of eliciting health preference and then define the most suitable criteria for “representativeness”.
As a common practice, demographic variables such as age, sex, and education are often used to define a “representative” sample. We identified additional significant factors beyond demographics. Health preference elicited from participants at Beijing is more positive and has narrower range than that from the other cities. China is a country with great geographic spread and health and economic disparities. Beijing is the capital and one of the three “super cities” in China (the other two are Shanghai and Guangzhou) where there are better established health care, education, and economic development than the other four cities (all are provincial capitals). For example, in 2012, out of top 100 hospitals in China (including both general and specialized hospitals), 26 are located in Beijing versus only 5 in Nanjing, 3 in Chengdu, 2 in Shenyang, and none in Guiyang [20]. The per capita disposable income of urban residents in Beijing, Nanjing, Chengdu, Shenyang, and Guiyang were RMB 40,321, RMB 39,881, RMB 29,968, RMB 29,074, and RMB 23,376, respectively, in 2013 [21–25]. We speculate that disparities in health care, education, and economic developments between regions might jointly contribute to the difference in health preference. If people living in a better developed area tends to be more positive and with narrower score range, it is really important to have a valuation study sample from different regions at various levels of health care, education, and economic developments in China. Our study is obviously limited with samples only from a few large cities. More work needs to be done to understand health preference of people living in less developed or remote areas.
View on life and death is embedded deeply in Chinese culture over thousands of years. We thought the philosophy behind LBD may help explain responses to health preference tasks which has also related to life and death. Approximately half of the participants agreed with this view and this proportion was similar across the cities. Participants who agreed with this view tended to be more positive, and the distribution of their health state preference was more condensed and towards the middle of the positive side of the health utility scale. Mathematically, this implies that an intervention for patients who suffered terribly is more likely to be cost-effective for those who preferred dead to living (due to their utilities spread over the scale, thus leading to a larger increment) than for patients who preferred living to dead (due to their preferences crowd on the middle of the positive scale, thus leading to a smaller increment), everything else equal. Again, our samples came from a few large cities; it is not clear whether our result represents a true societal view on life and death. But it is important to find out what is the general public’s view on this issue by surveying people from different areas.
In addition to the limitation (only 1296 participants from five large cities) already mentioned above, we also faced a relatively low response rate. The major reason is that the recruitment on streets and public places was challenging. The most common (90 %) reason people rejected to participate in the study when interviewers contacted with them was they did not have time.
Health state preferences are significantly affected by factors beyond demographics. These factors should be considered in achieving a representative sample in valuation studies in China.
References
Arrow, K. J. (1958). Utilities, attitudes, choices: A review note. Econometrica, 26(1), 23.
Drummond, M. F., Sculpher, M. J., Torrance, G. W., et al. (2005). Methods for the economic evaluation of health care programmes (3rd ed.). Oxford: Oxford University Press.
Wang, P., Li, M., Liu, G., Thumboo, J., & Luo, N. (2014). Do Chinese have similar health-state preferences? A comparison of mainland Chinese and Singaporean Chinese. The European Journal of Health Economics. doi:10.1007/s10198-014-0635-z.
Craig, B. M., Reeve, B. B., Cella, D., et al. (2014). Demographic differences in health preferences in the United States. Medical Care, 52(4), 307–313.
Pereira, C. C., Palta, M., Mullahy, J., et al. (2011). Race and preference-based health-related quality of life measures in the United States. Quality of Life Research, 20(6), 969–978.
Gaskin, D. J., & Frick, K. D. (2008). Race and ethnic disparities in valuing health. Medical Decision Making, 28(1), 12–20.
Shaw, J. W., Johnson, J. A., Chen, S., et al. (2007). Racial/ethnic differences in preferences for the EQ-5D health states: Results from the US valuation study. Journal of Clinical Epidemiology, 60(5), 479–490.
Fu, A. Z., & Kattan, M. W. (2006). Racial and ethnic differences in preference-based health status measure. Current Medical Research and Opinion, 22(12), 2439–2448.
Luo, N., Wang, Q., Feeny, D., et al. (2007). Measuring health preferences for Health Utilities Index Mark 3 health states: A study of feasibility and preference differences among ethnic groups in Singapore. Medical Decision Making, 27(1), 61–70.
Mu, G. (1994). About “Bad living is better than good death”. Chinese Journal of Sociology, 7(1), 18–21.
Vig, E., Davenport, N., & Pearlman, R. (2002). Good deaths, bad deaths, and preferences for the end of life: A qualitative study of geriatric outpatients. Journal of the American Geriatrics Society, 50(9), 1541–1548.
Kilbridge, K. L., Weeks, J. C., et al. (2001). Patient preferences for adjuvant interferon alfa-2b treatment. Journal of Clinical Oncology, 19(3), 812–823.
Luo, N., Li, M., Liu, G. G., et al. (2012). Developing the Chinese version of the new 5-level EQ-5D descriptive system: The response scaling approach. Quality of Life Research, 22(4), 885–890.
EuroQol Group. About EQ-5D. EuroQol group. http://www.euroqol.org/about-eq-5d.html. Accessed 02 Jan 2015.
Luo, N., Liu, G. G., & Li, M. (2014). Estimating the time trade-off values of the EQ-5D-5L health states in urban China. Value in Health, 17(3), A192.
Oppe, M., Devlin, N. J., van Hout, B., et al. (2014). A program of methodological research to arrive at the new international EQ-5D-5L valuation protocol. Value in Health, 17(4), 445–453.
National Bureau of Statistics of the People’s Republic of China. (2011). Tabulation on the 2010 population census of the People’s Republic of China. National Bureau of Statistics. http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm. Accessed 01 Nov 2012.
Krabbe, P. F., Devlin, N. J., Stolk, E. A., et al. (2014). Multinational evidence of the applicability and robustness of discrete choice modeling for deriving EQ-5D-5L health-state values. Medical Care, 52(11), 935–943.
Ministry of Education of People’s Republic of China. (2011). National education statistics 2010. Beijing: People’s Education Press.
Hospital Management Institute, Fudan University. (2013). China hospital rankings 2012 top 100. Fudan University. http://www.fudanmed.com/institute/news2012-2.aspx#. Accessed 04 Nov 2014.
Beijing Municipal Statistics Bureau. (2014). The per capita disposable income of Beijing’s urban residents in 2013. Beijing Municipal Statistics Bureau. http://www.bjstats.gov.cn/tjzn/mcjs/201303/t20130318_245551.htm. Accessed 02 Jan 2015.
Statistics Bureau of Nanjing. (2014). Nanjing 2013 statistical bulletin for national economic and social development. Statistics Bureau of Nanjing. http://www.njtj.gov.cn/47448/47488/47491/. Accessed 02 Jan 2015.
Chengdu Bureau of Statistics. (2014). Chengdu 2013 statistical bulletin for national economic and social development. Chengdu Bureau of Statistics. http://www.cdstats.chengdu.gov.cn/detail.asp?ID=82250&ClassID=020705. Accessed 02 Jan 2015.
Statistics Bureau of Shenyang. (2014). Shenyang 2013 statistical bulletin for national economic and social development. Statistics Bureau of Shenyang. http://www.sysinet.gov.cn/news.aspx?id=8562. Accessed 02 Jan 2015.
Statistical Bureau of Guiyang. (2014). Guiyang main economic indicators 2013. Statistical Bureau of Guiyang. http://tjj.gygov.gov.cn/gystjj/2452212196126490624/20140224/372433.html. Accessed 02 Jan 2015.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The Chinese EQ-5D-5L valuation study was funded by the EuroQol Research Foundation and China Centre for Health Economic Research, Peking University. Nan Luo and Feng Xie are members of the EuroQol Group. The authors declare that they have no conflict of interest.
Human and animal rights statement
All procedures performed in this research involving human participants were in accordance with the ethical standards of Peking University and have been performed in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. A waiver of the informed consent was approved as this study did not provide any intervention to participants. Participants can withdraw at any time without any consequences.
Rights and permissions
About this article

Cite this article
Jin, X., Liu, G.G., Luo, N. et al. Is bad living better than good death? Impact of demographic and cultural factors on health state preference. Qual Life Res 25, 979–986 (2016). https://doi.org/10.1007/s11136-015-1129-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-015-1129-x