
Abstract
Purpose
This study explores the use of EQ-5D-3L as a measure of population health status in a Brazilian region with significant socioeconomic, demographic, and epidemiological heterogeneity.
Methods
Data came from a study of 3363 literate individuals aged between 18 and 64 years living in urban areas of the state of Minas Gerais. Descriptive analysis and logistic and OLS regression models were performed to analyze the relationship between EQ-5D-3L (descriptive system and EQ VAS) and other health (self-assessed health status and 8 self-reported diagnosed chronic diseases), socioeconomic (educational level and economic class), and demographic (gender and age) measures. Additionally, a grade of membership (GoM) analysis was performed to identify multidimensional health profiles.
Results
A total of 76 health statuses were identified in the Brazilian population. The most prevalent one is full health (44 % of the sample). Elderly people, women, and individuals with poor health and lower socioeconomic conditions generally report more health problems in the EQ-5D-3L dimensions. The GoM analysis demonstrated that health status of older individuals is associated with the socioeconomic condition. Arthritis exhibited the strongest association with the EQ-5D-3L instrument.
Conclusions
The results indicate that EQ-5D-3L is a good measure of health status for the Brazilian population. The instrument has a good discriminatory capacity in terms of demographic, socioeconomic, and health measures. The high prevalence of individuals with full health may indicate the presence of ceiling effect. However, this prevalence is smaller than that in other countries.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The EQ-5D-3L was developed as a generic measure of health-related quality of life (HRQoL) in adults [1–4]. EQ-5D-3L defines health in terms of a five-dimensional descriptive system (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) each of which has three levels of severity (no problems, moderate problems, and extreme problems). This combination of dimensions/levels generates 243 unique health states. Health states are labeled with a five-digit numeric code representing the level of severity on each dimension. State 11111, for example, represents no problems on any dimension, whereas state 33333 represents an extreme problem on all five dimensions. EQ-5D-3L is designed for self-completion and consists of a two-page questionnaire. The first page records the self-reported level of problem on each of the five dimensions. The second page contains a vertical 20-cm visual analogue scale (EQ VAS) calibrated from 0 to 100, corresponding to the worst and best imaginable health states, respectively. The EQ-5D-3L has been officially translated into more than 120 languages including a Portuguese version validated for use in Brazil and approved by the EuroQol Group’s Translation Committee [1, 5]. EQ-5D-3L is probably the most widely used generic measure of its type with a great range of applications that includes clinical and economic evaluation, performance management and benchmarking, quality assurance and increasingly as a measure of patient-reported outcome measures (PROMs). However, EQ-5D-3L is essentially a measure of health status and has been widely incorporated in surveys of population health. Such surveys provide essential normative reference data that describe whole populations as well as important, policy-relevant subgroups. It is important to establish therefore the extent to which EQ-5D-3L has the capacity to add value to such surveys, especially given its widespread adoption by regulatory health agencies as the cornerstone of health technology assessment.
In practical terms, EQ-5D-3L has the advantage of being a simple instrument, easily applied, and with good response rates [6, 7]. However, the instrument’s brevity has two potential weaknesses. Firstly, the limited small number of response categories for each dimension reduces the capability to detect small differences in HRQoL status, and secondly, important dimensions that describe health status may be missing. Some studies have reported on the performance of EQ-5D-3L as a measure of health status in populations [8–19]. Elderly people, women, and individuals with poor health and lower socioeconomic status generally report more health problems in the EQ-5D-3L dimensions.
This study aims to evaluate the extent to which EQ-5D-3L is able to describe the HRQoL status of the Brazilian adult population. Three research questions guided our study. (1) What EQ-5D-3L health states are generated by the Brazilian adult population? (2) How are EQ-5D-3L health dimensions associated with individual characteristics and EQ VAS? (3) Who are the individuals who report the EQ-5D-3L full health? Are they really “full health” or are there omitted dimensions? It is an opportunity to analyze the performance of the EQ-5D-3L in a population with significant socioeconomic, demographic, and epidemiological heterogeneity. This context is different from that observed in most studies conducted in other countries [8–15, 18–21]. The data were obtained from a survey conducted for the state of Minas Gerais, Brazil [22]. Minas Gerais has the third largest economy in Brazil and exhibits strong socioeconomic disparities [23]. The heterogeneity observed in the state largely reflects Brazilian regional heterogeneity and therefore represents socioeconomic and epidemiological profile observed in the country. According to the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística—IBGE), in 2008, Minas Gerais GDP per capita was US$7635 compared to US$8690 in Brazil, while average years of schooling (around 7 years) and income inequality (Gini coefficient equal to 0.51) were very similar to whole country. The analysis of Human Development Index (HDI) shows evidence of how similar is the social economic disparities in Minas Gerais compared to those observed in Brazil. In 2010, HDI values for Minas Gerais ranged from 0.53 to 0.81, whereas in Brazilian states, it ranged from 0.63 to 0.78 [24].
Data
This study uses data from a Brazilian population survey that measured societal preferences for health states using time trade-off method [22]. A total of 3363 literate individual residents of the urban areas of Minas Gerais aged between 18 and 64 years were interviewed between October and December 2011. Individuals aged over 64 were excluded due to the high level of illiteracy and cognitive problems. Besides, as life expectancy in Brazil is around 74, the time horizon of 10 years used in MVH protocol may be implausible for individuals over 65. The sample is probabilistic (margin of error of 3 %) and stratified by gender and age, representative for adult population living in Minas Gerais. Only one individual in each household was selected, and economic incentives were not offered to the interviewees.
Statistical methods
Three methods were used besides a descriptive analysis including analysis of variance (ANOVA) to compare means of health conditions among population subgroups. Ordinary least square (OLS) models were estimated using the individuals score in the EQ VAS as the dependent variable. The goal of these models was to understand how the EQ-5D-3L dimensions explain the EQ VAS score. The estimation sequentially included explanatory variables. In order to know better the characteristics of individuals with full health in the EQ-5D-3L, a logistic regression model was estimated. The dependent variable assumes a value equal to 1 if an individual reported having no problem in the five dimensions. Finally, a cluster analysis based on the grade of membership (GoM) method was estimated. This method identifies multidimensional health profiles associating EQ-5D health dimensions to individual characteristics.
GoM is a mathematical method of clustering based on fuzzy sets theory. Considering a system of closed and well-defined sets, individuals can have partial membership in multiple groups. Based on the distribution of individual characteristics, the method defines extreme profiles and estimates the GoM of each individual to each extreme profile using the method of maximum likelihood [25]. For each individual, J categorical variables are observed, where the j-th variable has L j response levels. Consider K as the number of extreme profiles. The probability that the l-th response to the j-th variable is associated with the k-th extreme profile is represented by λ kji , whereas the GoM score for each K profile for the i-th individual is represented by g ik [26]. The g ik values add 1 to each individual, and as the individual approaches an extreme profile, his/her GoM for this profile increases while the GoM for other profiles decreases. At the limit, an individual having all characteristics for a K extreme profile has GoM equal to 1 for that profile and 0 for the others. Individuals who have this characteristic are called pure types [27].
The number of profiles was chosen based on the Akaike information criterion (AIC) [28] and on the substantive significance analysis [29], which evaluates the theoretical interpretation of the profiles. The characteristics of each profile were obtained using the Lambda-Marginal Frequency Ratio (LMFR). The cutoff value was set at 1.20 except for the following binary variables: no problem with respect to mobility, self-care, or usual activities. For these characteristics, the cutoff value was 1.02 because the percentage of individuals without problems in these dimensions reaches 98 %. To consider a characteristic as a profile identifier, the estimated probability of a response occurring among the pure types of the profile must be at least 20 % higher than the mean observed probability of the sample set [30]. In the case of the dimensions mentioned in the EQ-5D-3L, this probability should be at least 2 % higher. The cluster criteria according to the relative preponderance defined the membership of each individual in extreme profiles. According to this criterion, each individual belongs to a profile if his/her GoM for that profile is greater than the sum of the grades for the remaining profiles.
Variables
Two groups of explanatory variables were used. The first group refers to health variables: EQ-5D-3L dimensions, presence of chronic diseases, and self-assessed health. Categorical variables for each EQ-5D-3L dimension were created according to the severity level. The presence of diseases was measured according to the self-reported diagnosis of chronic conditions that are more prevalent in Brazilian adult population: hypertension, arthritis or rheumatism, diabetes, heart problem, respiratory or lung problems, depression, chronic kidney disease, and chronic back problems [31]. A total of eight dummy variables corresponding to each of these chronic diseases were created. Self-assessed health is a categorical variable with five response options: very good, good, fair, poor, and very poor. Due to the low prevalence of individuals with very poor health status, this category was grouped with the “poor” category.
The second group refers to socio-demographic indicators: gender, age, educational level, and socioeconomic class. Gender is binary with value “1” for men. Age is modeled by considering five groups: 18–25, 26–35, 36–45, 46–55, and 56–64 years. Educational level is defined by a variable with five categories representing the completed education level achieved by the interviewee: less than 4 years of education; 4–7; 8–10; 11–14 years; and 15 or more years. Socioeconomic class is a categorical variable defined by the Brazilian Association of Research Companies (Associação Brasileira de Empresas de Pesquisa-ABEP) [32]. This criterion classifies the population according to the possession of household goods, number of domestic employees, and the highest educational level in the household. A wealth index was built for each household, ranging from 0 to 46. Households were classified into four socioeconomic classes: A, B, C, and D/E.
Other variables, that may be associated with health status, were also included: marital status, place of residence, occupational status, religious belief, four-point scale self-assessed happiness status, smoking behavior, having children, private health insurance coverage, history of being caregiver, and death of a close friend/relative.
Results
What EQ-5D-3L health states are generated by the Brazilian adult population?
A total of 76 health states were identified among the 243 defined by EQ-5D-3L descriptive system. Figure 1 presents the prevalence of the 10 most frequent health states. Full health (11111) was the most common health status (44 %). The ten most frequent health states comprised 90 % of the sample. Among them, only one had an extreme severity level in one of the dimensions (anxiety/depression).

Prevalence of the 10 most frequent EQ-5D health states in the sample
Figure 2 presents the distribution of individuals by severity level for each EQ-5D-3L dimension. The majority of the interviewees had no problems in each dimension. Pain/discomfort and anxiety/depression were the dimensions with the highest prevalence of individuals reporting moderate or severe problems, while self-care presents the lowest prevalence of problems. Prevalence of extreme problems was less than 0.5 % for mobility, self-care, and usual activities.

Percentage of individuals by severity level for each EQ-5D dimension
How are EQ-5D-3L health dimensions associated with individual characteristics and EQ VAS?
Women tended to have more problems than men did in all EQ-5D-3L dimensions except for self-care. Due to the low prevalence of individuals with extreme problems, the category “some problem” was created to include individuals with moderate and severe problems. This difference was more evident for the pain/discomfort and anxiety/depression dimensions. Although women reported more health problems, the EQ VAS score was not significantly different between men and women (Fig. 3).

Percentage of individuals with some problem in each EQ-5D dimension and the mean EQ VAS score by gender
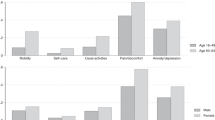
In general, the youngest group had a significantly lower prevalence of problems than the oldest group. This difference was not significant only for the self-care dimension. The mean EQ VAS score reinforced this result, demonstrating a monotonically decreasing relationship with age (Fig. 4).

Percentage of individuals with some problem in each EQ-5D dimension and the mean EQ VAS score by age group
There was a negative relationship between socioeconomic status and the prevalence of health problems, suggesting a health inequality favoring wealthy. The dimension with the greatest differences among socioeconomic subgroups was pain/discomfort. Again, there were no significant differences for self-care (Fig. 5).

Percentage of individuals with some problem in each EQ-5D dimension and the mean EQ VAS score by socioeconomic indicator
Among chronic diseases, arthritis exhibited the strongest association with the EQ-5D-3L. Individuals with arthritis were more likely to have problems in all dimensions and lower EQ VAS scores. In contrast, hypertension and lung problems were the diseases least associated with the EQ-5D-3L, with a lower prevalence of individuals with problems in all dimensions (Fig. 6).

Percentage of individuals with some problem in each EQ-5D dimension and the mean EQ VAS score according to the presence of chronic disease
Figure 7 presents boxplots for the EQ VAS score according to the number of dimensions in which the interviewees have some problem. The median EQ VAS score decreased as the number of problems increased. The median was 90 for people without problems and 50 for those with problems in all five dimensions. The fact that individuals who report having no problem on any of the EQ-5D-3L dimensions and who do not rate their own health on EQ VAS close to 100 suggests there could be health dimensions that are missing from the existing classification system. There are also some outliers, mainly among individuals who reported having problems in up to two dimensions, which are represented by the points in the figure. These findings suggest that the EQ-5D-3L descriptive system does not address health aspects that are important for some individuals.

Boxplot for the EQ VAS score by the number of EQ-5D dimensions in which individuals report problems
To understand the relationship between the EQ-5D-3L descriptive system and the EQ VAS score, regression models were estimated. Dependent variable is the EQ VAS score. For mobility, self-care, and usual activities dimensions, the moderate and extreme severity levels were grouped into a single category due to the low number of observations (Table 1).
Model 1 uses only the EQ-5D-3L dimensions as explanatory variables. The EQ-5D-3L had a strong association with the EQ VAS score. This model had good explanatory power, with an adjusted R 2 of 0.273. The presence of problems in all dimensions implies significantly lower scores on the scale. The indicators associated with extreme problems have greater magnitude. On average, scores attributed by individuals with extreme problems of pain/discomfort are 16 points lower on the EQ VAS. For individuals with extreme problems of anxiety/depression, the scores attributed to their health are 10 points lower.
Chronic disease coefficients were negative and statistically significant, suggesting that these diseases cause some problems not captured by the EQ-5D-3L (Model 2). Arthritis is the only disease that was not significant, corroborating the descriptive analysis that revealed strong correlation between this disease and the EQ-5D-3L dimensions. For depression, the coefficient was significant, although this disease is present in a dimension of the descriptive system. This result is likely related to a difference in how this disease is investigated. In the EQ-5D-3L, individual responds whether he/she is anxious or depressed at the time of the interview, whereas the question regarding the presence of diseases asks whether individual has been diagnosed with some problem of depression at some point in his/her life.
Model 3 incorporates demographic indicators. On average, men tended to attribute lower scores to their health than women. With respect to age, older individuals (46–55 and 56–64 years) attributed significantly lower scores to their health status than younger individuals. With respect to socioeconomic status (Model 4), a socioeconomic gradient in the EQ VAS score was observed. On average, classes C and D/E attributed lower scores to their health status than classes A and B. Regarding educational level, only individuals with 8–10 years of education attributed significantly higher scores to their health status than those with less than 4 years. Model 5 includes other control variables. Individuals with smoking behavior and those who experienced the death of a close friend or relative tended to attribute lower scores to their health status on the EQ VAS. Happy individuals tended to score their health status 4 points higher.
Health profiles
The GoM allows the definition of multidimensional health profiles using health and socio-demographic indicators. According to the AIC and the substantive significance analysis, four health profiles were identified (Table 2). Profile 1 has the lowest prevalence in the sample (15 %) and represents individuals with moderate/extreme health limitations strongly related to socio-demographic indicators. Profile 2 (19 %) refers to older individuals with full health and better socioeconomic status. Hypertension is the only chronic disease that identifies this profile. The percentage of individuals with hypertension among the pure types of this profile is over 20 % higher than the prevalence of this disease in the total sample. This result confirms the findings that hypertension is weakly associated with the EQ-5D-3L. Profile 3 (30 %) represents younger individuals with full health and better socioeconomic status. Profile 4 (25 %) refers to individuals with good health but lower socioeconomic status. The remaining 11 % of individuals are amorphous; i.e., their GoM in the four profiles are similar.
Who are the EQ-5D-3L full health individuals? Are they really “full health” or are there omitted dimensions?
One difficulty in using the EQ-5D-3L is differentiating individuals who actually have full health from those who have some problem not captured by the descriptive system. In the population investigated, full health was the most prevalent status (44 %). Among them, only 27 % attributed the maximum score on the EQ VAS to their health.
A comparison between individuals with full health and the total sample (Table 3) indicated that individuals with full health were generally younger, well-educated, belonged to a higher social class, and male. Moreover, although approximately 50 % of individuals had some chronic disease in the total sample, while for the subgroup with full health, this value reduced to 32 %. The most common chronic diseases among individuals with full health were hypertension and respiratory or lung problems. The analysis of self-assessed health status revealed that among individuals with full health, 92 % reported their health as very good or good, compared with 77 % in the total sample.
A logistic model was estimated to better understand the relationship between socio-demographic and health status indicators and the chance of having full health (Table 4). Results indicate health inequalities favoring richer individuals. Individuals belonging to the lower economic classes and with lower educational levels had a lower chance of having full health. Regarding health indicators, individuals with hypertension, arthritis, depression, heart, lung, and back problems had a significantly lower chance of having full health. Moreover, the chance of having full health decreased as the self-assessed health worsened. For demographic indicators, only gender was significant, indicating that men had a higher chance of having full health. Finally, individuals who took care of a sick person had a lower chance of having full health, whereas happy individuals and those living in the countryside of Minas Gerais had a greater chance.
Discussion
This study is novel in using the EQ-5D-3L instrument as a measure of the health status of the Brazilian population. Few studies have related EQ-5D-3L to other health measures by focusing on the predictive ability of the instrument. Results obtained in this study indicate that EQ-5D-3L is a good measure of the Brazilian health status which is in agreement with those presented in the literature [9–19, 21]. The main results indicate a good discriminatory capacity of the EQ-5D-3L for Brazil in terms of gender, age, socioeconomic status, and health status.
There is a direct relationship between age and the EQ-5D-3L. Older individuals exhibit higher prevalence of problems in all EQ-5D-3L dimensions and lower EQ VAS scores. The multivariate analysis from the GoM method demonstrated that health status of older individuals is strongly associated with socioeconomic class. Profiles 1 and 2 refer to individuals in the older age groups. Profile 1 identifies those with worse health and socioeconomic conditions. Profile 2 identifies individuals with full health and good socioeconomic conditions.
Regarding differences between genders, two results were observed. Women have more health problems and a lower chance of full health, whereas men tend to attribute lower EQ VAS scores to their health. Same results are observed in the OLS and logistic models. International evidence also indicates a higher prevalence of problems among women; despite in some countries, this difference is small [9, 12, 15]. For the EQ VAS score, Lubetkin et al. [13] estimate an OLS model for the American population similar to the one estimated in the present study and found that, on average, men attribute higher scores to their health. The opposite result found in the present study seems to indicate that in Brazil, men are less tolerant of health problems. Even reporting fewer problems in the EQ-5D-3L, the assessment of the general health status by the EQ VAS is lower than that observed in women. Another possible explanation is that the EQ-5D-3L descriptive system fails in capturing health problems specific to this population subgroup.
The relationship between the EQ-5D-3L and socioeconomic measures indicates the existence of health inequalities in Brazil. This result corroborates several studies on health inequalities in the country [33–35] and is in agreement with empirical evidence from other countries [9–13, 17]. Regarding health indicators, the EQ-5D-3L has a good discriminatory capacity for self-assessed health and chronic diseases. Individuals who rate their health as poor and those with chronic diseases report more problems in the EQ-5D-3L than individuals without these conditions. Arthritis is strongly associated with the EQ-5D-3L, whereas lung problems and hypertension are the less ones. Other studies had already found the same results [9, 14, 36]. For hypertension, a study conducted in Cyprus with hypertensive patients indicated a strong ceiling effect. Only 40 % of the patients reported some problem in the EQ-5D-3L dimensions, and a weak association of this disease with mobility, self-care, and usual activities dimensions was observed [37].
Despite the good discriminatory capacity of the EQ-5D-3L for the socio-demographic and health indicators, a high prevalence of individuals with full health was observed (44 %), which may indicate the presence of ceiling effect in the Brazilian population. However, population studies conducted in other countries found a higher prevalence of individuals with full health. For example, the prevalence in the UK is 58 % [10]; in Canada and USA, 47 % [19, 20]; in Catalonia, 60 % [9]; and in Argentina, 61 % [38]. A possible explanation for the lower value found in Brazil is the great socioeconomic heterogeneity observed in the country as well as the presence of strong health inequalities. This implies a lower chance of observing full health among individuals who belong to lower economic classes. Therefore, the EQ-5D-3L can be considered a good measure for health status in developing countries and countries with higher levels of social inequality, such as Brazil. For more homogenous countries, a more sensitive instrument is necessary to capture small differences in health.
References
Brooks, R. (1996). EuroQol: The current state of play. Health Policy, 37(1), 53–72.
Brazier, J., & Deverill, M. (1999). A checklist for judging preference-based measures of health related quality of life: Learning from psychometrics. Health Economics, 8, 41–51.
Williams, A. (1995). A measurement and validation of health: A chronicle. Centre for health economics discussion paper 136.
Gudex, C. (2005). The descriptive system of the EuroQol instrument. EQ-5D concepts and methods: A development history (pp. 19–28). Netherlands: Springer.
EuroQol Group. (n.d.). EuroQol. Retrieved January 6, 2014, from http://www.abep.org/new/
Holland, R., Smith, R. D., Harvey, I., Swift, L., & Lenaghan, E. (2004). Assessing quality of life in the elderly: A direct comparison of the EQ-5D and AQoL. Health Ecomonics, 13(8), 793–805.
Schulz, M. W., Chen, J., Woo, H. H., Keech, M., Watson, M. E., & Davey, P. J. (2002). A comparison of techniques for eliciting patient preferences in patients with benign prostatic hyperplasia. The Journal of Urology, 168(1), 155–159.
Essink-Bot, M. (1995). Health status as a measure of outcome of disease and treatment. Erasmus/Rotterdam: Instituut Maatschappelijke Gezondheidszorg/Universiteit Rotterdam.
Cunillera, O., Tresserras, R., Rajmil, L., Vilagut, G., Brugulat, P., Herdman, M., & Ferrer, M. (2010). Discriminative capacity of the EQ-5D, SF-6D and SF-12 as measures of health status in population health survey. Quality of Life Research, 19(6), 853–864.
Kind, P., Dolan, P., Gudex, C., & Williams, A. (1998). Variations in population health status: Results from a United Kingdom national questionnaire survey. BMJ, 316(7133), 736–741.
Macran, S., Weatherly, H., & Kind, P. (2003). Measuring population health: A comparison of three generic health status measures. Medical Care, 41(2), 218–231.
Luo, N., Johnson, J. A., Shaw, J. W., Feeny, D., & Coons, S. J. (2005). Self-reported health status of the general adult US population as assessed by the EQ-5D and Health Utilities Index. Medical Care, 43(11), 1078–1086.
Lubetkin, E. I., Jia, H., Franks, P., & Gold, M. R. (2005). Relationship among sociodemographic factors, clinical conditions, and health-related quality of life: Examining the EQ-5D in the U.S. general population. Quality of Life Research, 14(10), 2187–2196.
Saarni, S. I., Härkänen, T., Sintonen, H., Suvisaari, J., Koskinen, S., Aromaa, A., & Lönnqvist, J. (2006). The impact of 29 chronic conditions on health-related quality of life: A general population survey in Finland using 15D and EQ-5D. Quality of Life Research, 15(8), 1403–1414.
Fryback, D. G., Dunham, N. C., Palta, M., Hanmer, J., Buechner, J., Cherepanov, D., & Ganiats, T. G. (2007). US norms for six generic health-related quality-of-life indexes from the National Health Measurement study. Medical Care, 45(12), 1162–1170.
Ravens-Sieberer, U., Wille, N., Badia, X., Bonsel, G., Burström, K., Cavrini, G., & Greiner, W. (2010). Feasibility, reliability, and validity of the EQ-5D-Y: Results from a multinational study. Quality of Life Research, 19(6), 887–897.
Wang, H.-M., Patrick, D. L., Edwards, T. C., Skalicky, A. M., Zeng, H.-Y., & Gu, W.-W. (2011). Validation of the EQ-5D in general population sample in urban China. Quality of Life Research, 21(1), 155–160.
Tan, Z., Liang, Y., Liu, S., Cao, W., Tu, H., et al. (2013). Health-related quality of life as measured with EQ-5D among populations with and without specific chronic conditions: A population-based survey in Shaanxi Province, China. PLoS One, 8(7), e65958. doi:10.1371/journal.pone.0065958.
Sun, S., Chen, J., Kind, P., Xu, L., Zhang, Y., & Burström, K. (2014). Experience-based VAS values for EQ-5D-3L health states in a national general population health survey in China. Quality of Life Research,. doi:10.1007/s11136-014-0793-6.
Bharmal, M., & Thomas, J. (2006). Comparing the EQ-5D and the SF-6D descriptive systems to assess their ceiling effects in the US general population. Value in Health, 9(4), 262–271.
Johnson, J. A., & Pickard, A. S. (2000). Comparison of the EQ-5D and SF-12 health surveys in a general population survey in Alberta, Canada. Medical Care, 38(1), 115–121.
Andrade, M. V., Noronha, K., Kind, P., Maia, A. C., Menezes, R. M., Reis, C. B., & Lins, C. (2013). Societal preferences for EQ-5D health states from a Brazilian population survey. Value in Health Regional Issues, 2(3), 405–412.
Instituto Brasileiro de Geografia e Estatística. (IBGE). secccpmae@ime.usp.br. http://www.ibge.com.br/home/estatistica/economia/contasregionais/2010/default_xls_2002_2010_zip.shtm
Programa das Nações Unidas para o Desenvolvimento (PNUD). (2013). Atlas do Desenvolvimento Humano no Brasil 2013. Retrieved from http://www.atlasbrasil.org.br/2013/
Melo, F. L. B. (2006). Trajetórias no mercado de trabalho: perfis socioocupacionais de indivíduos e casais da Grande São Paulo. Centro de Desenvolvimento e Planejamento Regional, Universidade Federal de Minas Gerais, Belo Horizonte
Manton, K. G., Woodbury, M. A., & Tolley, H. D. (1994). Statistical applications using fuzzy sets (1st ed.). New York: Wiley.
Siviero, P. C. L. (2012). Causas múltiplas de morte associadas à insuficiência renal crônica no Brasil, 2000–2004. Belo Horizonte: Universidade Federal de Minas Gerais.
Akaike, H. (1974). A new look at the statistical model identification. IEEE Transactions on Automatic Control, 19(6), 716–723.
Pereira, C. C. A., Machado, C. J., & Rodrigues, R. N. (2007). Profiles of multiple causes of death related to HIV/AIDS in the cities of São Paulo and Santos, Brazil, 2001. Cadernos de Saúde Pública, 23(3), 645–655.
Sawyer, D. O., Leite, I. C., & Alexandrino, R. (2002). Perfis de utilização de serviços de saúde no Brasil. Ciência e Saúde Coletiva, 7(4), 757–776.
PESQUISA nacional por amostra de domicílios—PNAD 2008. (2008). Rio de Janeiro: IBGE. Microdados em CD-Rom.
Critério de classificação econômica Brasil. (n.d.). Portal ABEP. Retrieved from http://www.abep.org/new/
Almeida, G., Sarti, F. M., Ferreira, F. F., Diaz, M. D. M., & Campino, A. C. (2013). Analysis of the evolution and determinants of income-related inequalities in the Brazilian health system, 1998–2008. Revista Panamericana de Salud Publica, 33(2), 90–97.
Andrade, M. V., Noronha, K., Menezes, R. M., Souza, M. N., Reis, C. B., Martinss, D., & Gomes, L. (2013). Desigualdade socioeconômica no acesso aos serviços de saúde no Brasil: um estudo comparativo entre as regiões brasileiras em 1998 e 2008. Economia Aplicada, 17(4), 623–645.
Macinko, J., & Lima-Costa, M. F. (2012). Horizontal equity in health care utilization in Brazil, 1998–2008. International Journal for Equity in Health, 11(33), 1–8.
Harper, R., Brazier, J. E., Waterhouse, J. C., Walters, S. J., Jones, N. M., & Howard, P. (1997). Comparison of outcome measures for patients with chronic obstructive pulmonary disease (COPD) in an outpatient setting. Thorax, 52(10), 879–887.
Theodorou, M., Kaitelidou, D., Galanis, P., & Middleton, N. (2011). Quality of life measurement in patients with hypertension in Cyprus. Hellenic Journal of Cardiology, 52(5), 407–415.
Augustovski, F., Rey Ares, L., & Gibbons, L. (2013). Self-reported health status and EQ-5D-3L values of the Argentine population: Comparing 2005 versus 2009 national risk factor surveys. Value in Health, 16, A671.
Acknowledgments
This research was supported by Minas Gerais State Research Foundation (Fundação de Apoio a Pesquisa do Estado de Minas Gerais—FAPEMIG), Belo Horizonte, Minas Gerais, Brazil, and by National Council for Scientific and Technological Development—CNPQ. Partial financial support was also provided by Universidade Federal de Minas Gerais. Authors are grateful to Gilvan Guedes for his comments on grade of membership analysis.
Conflict of interest
There are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Menezes, R.M., Andrade, M.V., Noronha, K.V.M.S. et al. EQ-5D-3L as a health measure of Brazilian adult population. Qual Life Res 24, 2761–2776 (2015). https://doi.org/10.1007/s11136-015-0994-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-015-0994-7