
Abstract
Purpose
The main objective of this study was to determine the relationship between quality of life, social functioning, depressive symptoms, self-efficacy, physical function, and socioeconomic status (SES) in community-dwelling older adults.
Methods
A cross-sectional design was used to examine the relationships. A sample of 193 community-dwelling older adults completed the measurements. Structural equation modeling with full information maximum likelihood in LISREL was used to evaluate the relationships between the latent variables (SES, social functioning, depressive symptoms, self-efficacy, physical function, and quality of life).
Results
The path analysis exhibited significant effects of SES on physical function, social functioning, depressive symptoms, and self-efficacy (γ = 0.42–0.73), and significant effects in regard to social functioning, depressive symptoms, and self-efficacy on quality of life (γ = 0.27–0.61). There was no direct effect of SES on the quality of life. The model fit indices demonstrated a reasonable fit (χ 2 = 98.3, df = 48, p < 0.001), matching the relative Chi-square criterion and the RMSEA criterion. The model explained 55.5 % of the variance of quality of life.
Conclusions
The path analysis indicated an indirect effect of SES on the quality of life by social functioning, depressive symptoms, and self-efficacy in community-dwelling older adults. Physical function did not have a direct effect on the quality of life. To improve the quality of life in older adults, additional focus is required on the socioeconomic psychosocial differences in the community-dwelling older population.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Due to prolonged life expectancy, retaining a good quality of life (QoL) at an older age is of increasing importance and interest. QoL is an important outcome of many studies in older adults. In these studies, a plethora of definitions is applied to specify QoL [1–4]. Conceptual and methodological ambiguity continues on how to define and measure QoL [1, 3–6]. Furthermore, there is an ongoing and challenging search to identify determinants of QoL aiming at determining indicators for improving QoL.
QoL is a subjective and multidimensional construct, which is affected in a complex manner by the person’s physical health, psychological state, level of independence, and social relationships to noticeable characteristics of the environment [7]. From this perspective, QoL transcends physical health [8, 9]. This is also applicable to older adults and superimposes with other concepts such as active, successful, and healthy aging [4, 10]. Enjoying positive social relationships, being active and capable of participating in meaningful activities, and having no functional limitations are especially beneficial for QoL at an older age [4]. Therefore, a need-satisfaction approach appears most appropriate in order to study QoL in older adults, as from this perspective, the focus is predominantly on the perceived satisfaction, expectations, and fulfillment of the needs of older adults [11, 12].
To improve QoL, gaining a comprehensive understanding of the determinants of QoL is of fundamental significance. Socioeconomic status (SES) is an important determinant of QoL [13, 14]. Both education and income were determined to be robust predictors of QoL in later life [13, 15]. In this association, several determinants may act as intermediate factors such as social and psychological factors, physical function, and SES. Psychosocial factors accounted for the majority of the changes in long-term QoL in older adults [16]. For instance, a lack of perceived social support, a small social network, and living without a partner may have a negative impact on the QoL of older persons [16, 17]. Additionally, associations of depressive symptoms and psychological resources, such as self-efficacy, with QoL were demonstrated [16, 18]. Moreover, physical function has been associated with QoL in older adults [19–22]. Increased levels of physical function such as muscular strength, agility, and aerobic endurance can contribute to the enhancement of QoL [22–24]. In addition, these determinants of QoL are also associated with SES. SES differences in self-reported physical function, social network size, feelings of loneliness, and depression are especially demonstrated [25–34]. Therefore, studies investigating the relationship between QoL and SES should incorporate the possibility of direct and indirect effects of other variables such as social functioning, depressive symptoms, global self-efficacy, and physical function. Still, only minimal information is evident regarding the latent factors SES and QoL in older adults. In regression analysis, such factors cannot be treated as being latent. For that reason, multivariate analysis techniques, such as structural equation modeling, are statistically adequate methods to examine the relationship between SES and QoL [35].
The main objective of this study is to determine the relationship between QoL, social functioning, depressive symptoms, self-efficacy, physical function, and SES in community-dwelling older adults.
Methods
Study sample and study design
In 2011 and 2012, a sample of 1,976 older inhabitants of a mid-sized city, Delfzijl, in the northern part of the Netherlands was invited for participation in the study. Participants who were recruited from both socioeconomically underprivileged and average neighborhoods were aged 65 years and older, and were not institutionalized. Candidate participants were excluded when they did not demonstrate enough mobility to move independently. All participants were informed about the goal and procedure of the study and written informed consent was obtained from the same. The research was performed in compliance with the Declaration of Helsinki. A total of 193 participants completed the measurements comprising performance-based tests and questionnaires. A cross-sectional design was employed.
Data collection
All participants were invited to participate in the health measurements. Performance-based physical function was measured, and questionnaires were assessed. Preceding the physical function tests, the Physical Activity Readiness Questionnaire (PAR-Q) was assessed by a physiotherapist to determine any possible risk of exercising and to guarantee safety [36]. Additionally, blood pressure was measured with an electronic sphygmomanometer. When the systolic blood pressure was >150 mmHg or the diastolic pressure was >90 mmHg, participants were excluded from participation in the endurance test in order to guarantee safety. All physical function tests were individually assessed and administered by well-trained test leaders. Following the physical function tests, participants individually filled in all questionnaires under the supervision of research assistants.
Measures
Participant characteristics
Height and weight of the participants were measured to calculate the body mass index (BMI). BMI is calculated by dividing weight (in kilograms) by the square of height (in meters). Additionally, morbidity was assessed as the total number of present chronic diseases or disorders. The presence of 26 common chronic conditions was mapped [37, 38].
Quality of life
We employed the CASP-19 questionnaire to measure the broad concept of QoL based on a need-satisfaction approach. CASP-19 is an instrument that is extensively used to assess the QoL in older adults and comprises 19 items in four domains: control, autonomy, self-realization, and pleasure [39]. The CASP is developed from a need-satisfaction approach and measures the degree to which human needs are fulfilled. The range of the CASP-19 is 0–57, with the higher scores indicating a better QoL. The validity and reliability of the CASP has been previously documented in a population of older persons. In British older adults, the reliability and validity was satisfactory (α = 0.55–0.86; r = −0.58), and the CASP-19 mean (SD) score in the Office for National Statistics Omnibus Survey in 2008 for people aged 65 years and older was 41.8 (8.1) [40].
Social functioning
Partner status was measured by recording the presence of a partner (no or yes).
Loneliness was assessed with the 6-item De Jong Gierveld Scale. This 6-item Likert scale is a reliable and valid instrument for measuring overall, emotional, and social loneliness in substantial surveys of older adults (α = 0.70–0.76; congruent validity r = 0.93–0.95) [41]. All items have five response categories. The loneliness scale scores ranges from 0 (not lonely) to 6 (extremely lonely).
Social network size was assessed utilizing the 6-item Lubben Social Network Scale. This 6-item scale is a valid and reliable scale to assess perceived social support received by family and friends (α = 0.83; congruent validity r = 0.68–0.78) [42]. The scores range from 0 (very small network) to 30 (extensive network). In a large European older sample, the mean (SD) score varied from 16.1 (5.5) to 17.9 (5.3) [42].
Social support is assessed with the SSL12-I scale. This 12-item scale has satisfactory psychometric properties to assess the extent of received social support in an older population (α = 0.83) [43]. All items have four response categories. The scores range from 12 (low level of support) to 48 (high level of support). In a Dutch older population, the mean (SD) SSL12-I scale was 25.5 (5.0) [43].
Depression
Depression was measured with the Dutch version of the CES-D questionnaire. The self-report 20-item CES-D scale is valid and reliable to measure depressive symptoms and behaviors experienced during the previous week in older adults (α = 0.79–0.92; r = 0.73–0.83) [44]. The items have four response categories. CES-D scores range from 0 (no depression) to 60 (high level of depression). In an older population, the mean (SD) CES-D score was 8.33 (6.84) [45].
Self-efficacy
Self-efficacy was assessed with the Dutch version of the 16-item General Self-Efficacy Scale [46]. All items incorporate five response categories. The Dutch version of the General Self-Efficacy Scale appeared moderately reliable to measure generalized expectations of self-efficacy (α = 0.81) [47]. Scores range from 16 (very high self-efficacy) to 80 (very low self-efficacy).
Physical function
Physical function was measured with three validated and standardized performance-based tests.
Leg strength was assessed utilizing the 30-s Sit-To-Stand Test [48]. The number of complete sit-to-stands in 30 s without using arms was counted.
Aerobic endurance was assessed by using the 2-min step test [48]. During this test, the participant marched in place for 2 min while lifting the knees. The total number of times the knee was lifted was counted.
Dynamic balance was assessed employing the Timed Up-and-Go Test [49]. The time required to rise from the chair, walk to a cone, and return to the seat, all as quickly as possible, was measured. The best score from two trials was recorded.
For these physical function tests, norm values adjusted to age and gender were calculated whereby participants were scored below average, average, or above average (according to their age and gender).
Socioeconomic status (SES)
Two indicators of SES were used: income and education. Personal monthly net income was measured with an ordinal scale consisting of the three categories: <1,100 euro, 1,100–1,600 euro, and >1,600 euro. Three education categories were distinguished: high (high school, university), medium (advanced elementary education, occupational education), and low (primary school).
Statistical analyses
Model specification
Based on a review of the literature, a model of the relationships between SES, social functioning, depressive symptoms, self-efficacy, physical function, and QoL was conceptualized. Figure 1 shows the assumed associations and directions. We hypothesized direct effects of SES on QoL [13–15], physical function [33, 34], social functioning [27–29], depressive symptoms [30, 31], and self-efficacy. Furthermore, we hypothesized direct effects of physical function on QoL [19–24], social functioning on QoL [16, 17, 50], depressive symptoms on QoL [16], and self-efficacy on QoL [18]. The variables were modeled as latent variables exploiting the indicators income and education for SES; loneliness, partner status, social network size, and social support for social functioning; and leg strength, dynamic balance, and aerobic endurance for physical function. The latent variables depression, self-efficacy, and QoL had a single indicator.
All latent variables were scaled by fixation of factor loadings of observed variables. SES was scaled on the variable education, social functioning was scaled on loneliness, and physical function was scaled on aerobic endurance. These factor loadings were set equal to 1.00 or −1.00 in such a manner that higher scores indicate greater levels of functioning. The error variance of the latent variables depression, self-efficacy, and QoL was set equal to 1.00.
Estimation method
Descriptive statistics were employed to summarize subject characteristics of the study sample. Data were processed using statistical software SPSS statistics 19 (SPSS Inc.) and LISREL 9.10 (Scientific Software International, Lincolnwood, IL). Structural equation modeling in LISREL was used to evaluate the fit of the proposed model. PRELIS was used to compute the correlation matrix for the analyses using Pearson product moment correlations between continuous variables, polychoric correlations between ordinal variables, and polyserial correlations between ordinal and continuous variables. A correlation < 0.30 was considered “low,” 0.30–0.60 “moderate,” and >0.60 “high” [51].
The data were analyzed by the full information maximum likelihood (FIML) estimation, which is recommended as a method to deal with missing data in structural equation modeling [52, 53]. In the current data, 10.9 % of education data, 7.8 % of income data, 12.4 % of depression data, 3.6 % of morbidity and social network data, 3.1 % of partner status data, 2.1 % of loneliness data, 1.6 % of self-efficacy, social support and quality-of-life data, and 0.5 % of leg strength data were missing. Age, gender, BMI, dynamic balance, and endurance data were complete.
Model testing
Structural equation modeling was used to test the relationships between six latent variables (SES, social functioning, depression, self-efficacy, physical function, and QoL). The fit of the model was evaluated on the basis of multiple criteria: (relative) Chi-square, Chi-square p value, root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), and the comparative fit index (CFI). The model fit is acceptable if the ratio of Chi-square to the degree of freedom is between 2 and 5 [54, 55]; the Chi-square p value is nonsignificant [56]; the RMSEA is <0.07 [57]; the SRMR is <0.08 [58]; and the CFI is >0.90 [59]. RMSEA or SRMR values above 0.10 indicate poor fit [58]. The statistical significance level was set to 0.05.
Power analysis
Power analysis was executed to determine required sample size to achieve adequate power to test close fit of the hypothesized structural model. Minimum sample size is determined, given the significance level (α = 0.05), the desired level of power (power = 0.80), degrees of freedom of the model (d = 48), and the hypothesized values of the RMSEA [60]. The null hypothesis specifies the hypothesized value of the RMSEA, and in our study, the model fit is acceptable if the RMSEA is <0.07 [57]. The RMSEA value under the null hypothesis was set to 0.07 and under the alternative hypothesis to 0.10. Based on the calculations specified by MacCallum et al. [60], we calculated a minimum sample size of 194 participants (ceiled).
Results
Subject characteristics
Data from 193 older adults were employed for the analyses. Table 1 shows the personal and socioeconomic characteristics of the subjects. The ages ranged from 65 to 94 years with a mean (SD) age of 71.6 (4.9) years. Most participants possessed only a low or medium education (88 %), and half of the participants (53 %) received a net month income of <1,600 euro. Highly educated persons and persons with a higher income level (>1,600 euro) were slightly older and primarily male compared with the low educated persons and persons with an income between 1,100 and 1,600 euro. Persons with an income between 1,100 and 1,600 euro reported a higher number of chronic diseases or disorders than persons with a higher income (>1,600 euro). The BMI did not vary between the education and income levels. The scores of the outcome variables physical function, social functioning, depression, self-efficacy, and quality of life are shown in Table 2.
Associations between QoL and the determinants
Pearson product moment, polyserial, and polychoric correlations between all pairs of variables are shown in Table 3. As expected, SES indicators were moderately correlated (r = 0.36) just as with the physical function components (r = 0.23–0.46). Within social functioning indicators, most indicators were also significantly correlated (r = −0.35 to 0.16); only partner status and social support were not significantly correlated. Education and income correlated low with all other variables (r = 0.01–0.28). QoL was minimally correlated with SES indicators (r = 0.09–0.19); physical function components (r = 0.07–0.22); social network size (r = 0.27); partner status (r = 0.23); and social support (r = 0.27). QoL was moderately correlated with loneliness (r = −0.47), depression (r = −0.58), and self-efficacy (r = −0.43). Additionally, loneliness and partner status were moderately correlated with depression (resp. r = 0.50; r = −0.31); aerobic endurance was moderately correlated with self-efficacy (r = −0.30); and depression was moderately correlated with self-efficacy (r = 0.44).
Structural equation model
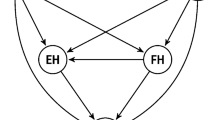
Based on the literature, we hypothesized that SES has a direct and indirect effect on QoL by physical function, social functioning, and psychological functioning (depressive symptoms and self-efficacy). The path diagram of the model, including standardized regression coefficients, is shown in Fig. 1. The model fit indices demonstrated a reasonable fit (χ 2 = 98.3, df = 48, p < 0.001), matching the relative Chi-square criterion (χ 2/df < 5) and the RMSEA criterion (RMSEA ≤ 0.07). The SRMR value was 0.083, indicating mediocre fit (a value between 0.08 and 0.10). The CFI value was lower than the conventional criteria of 0.90, indicating minimal acceptable fit. The Chi-square p value criterion was not met. Overall, the model explained 55.5 % of the variance of QoL.

Path diagram of the hypothesized model illustrating the relationship between socioeconomic status and quality of life. Presented are the standardized coefficients. Nonsignificant path coefficients are displayed in gray
The model indicates significant effects of SES on physical function (γ = 0.42, p = 0.001), social functioning (γ = 0.73, p < 0.001), depression (γ = −0.70, p < 0.001), and self-efficacy (γ = 0.63, p < 0.001). Furthermore, social functioning, depression, and self-efficacy have a significant direct effect on QoL (resp. β = 0.61, p = 0.02; β = −0.51, p = 0.001; β = 0.27, p = 0.03), whereas the effect of physical function on QoL was not significant (β = 0.05, p = 0.57). There was no direct effect of SES on QoL (β = −0.53, p = 0.24).
The standardized direct, indirect, and total effect of SES, physical function, social functioning, depression, and self-efficacy on QoL are presented in Table 4. The results demonstrated that SES, social functioning, depression, and self-efficacy had substantial total effects on QoL and that physical function had only a minimal total effect on QoL.
An alternative theory driven model was tested as a sensitivity analysis. Inspired by social cognitive theory and earlier research, effects of self-efficacy and social functioning on physical function were added and estimated in the model. This alternative model did not reveal any new significant indirect effects. The overall fit of this model was sufficient, but weaker than the hypothesized model (χ 2 = 95.4, df = 46, p < 0.001; RMSEA = 0.08). Besides, basic regression analysis was performed to check if the results were consistent with those from path analysis. The results of these analyses were similar.
Discussion
In the present study, a path analysis indicates an indirect effect of SES on QoL by social functioning, depressive symptoms, and self-efficacy in community-dwelling older adults. Persons with a more moderate SES reported poorer social functioning, more frequent depressive symptoms, lower self-efficacy, and, as a consequence, a less fulfilled QoL. Surprisingly, physical function had neither a direct or indirect effect on QoL. The model has a reasonable overall fit and explained 55.5 % of the QoL variance.
An association between SES and QoL is often presupposed; however, it has not been intensively studied whether the relationship is direct or indirect. The majority of previous studies examined separate bivariate relationships between indicators of SES, such as income or education, and measures of QoL [4, 14, 15]. The current multivariate analysis afforded the opportunity to evaluate both direct and indirect relationships utilizing path analysis. Our analysis revealed only indirect effects of SES on QoL by social functioning, depressive symptoms, and self-efficacy. Our results imply that SES does not directly affect QoL. Nonetheless, SES does influence a person’s social and psychological functioning and consequently influences a person’s QoL. Several studies questioned the size of the direct relationship between SES and QoL. This relationship appeared to be relatively minimal for people habituating in developed countries. In a number of review studies, it was reported that measures of SES explain only 2–3 % of the variance in individual subjective well-being [15, 61]. It is suggested that once basic needs are fulfilled, such as having food, shelter, and clothing, income is of negligible relevance [61]. In our multivariate model, we discovered more substantial relationships. According to our model, 20.8 % of the variance in QoL was explained by SES, social functioning, depressive symptoms, and self-efficacy.
Physical function is not related to QoL in our study sample. This is not in accordance with correlational studies that actually ascertained relationships between measures of physical function and feelings of well-being or QoL [20, 22–24]. A plausible explanation for the variance between our results and other studies may be that our study population was relatively (physically) healthy. Our study population experienced a considerable range in physical function from below to above standard. All participants were community-dwelling older adults, independent of help or care from others, and reporting no or only minor problems with daily living. As supported by several studies, we expect that physical function will only influence the QoL if activities of daily living are impaired. In nursing home residents, being physically mobile was mentioned as a prerequisite for independence and mentioned as a determinant of QoL [62]. Additionally, a study of Garatachea et al. [20] demonstrated that there were diminished feelings of subjective well-being for dependent, less physically active subjects compared with those who were independent and less physically active.
According to our analyses, poor social functioning, reporting depressive symptoms, and experiencing minimal self-efficacy contribute to a less fulfilled QoL. The amount of social functioning and depressive symptoms are, moreover, described as direct determinants of QoL [16, 17]. However, self-efficacy is often specified to have an indirect influence on QoL through determinants of QoL, e.g., physical activity [63]. Self-efficacy is defined as the evaluation and the conviction in one’s individual abilities to achieve particular goals [64]. Most studies examined self-efficacy beliefs in the capacity of executing specific health behaviors such as performing physical exercises or employing a healthy diet. Alternatively, we measured global self-efficacy in our study sample whereby global self-efficacy was determined to be a direct determinant of QoL and not merely having an indirect influence on QoL through indicators of physical and psychosocial health. It appears that persons who believe that individual actions are responsible for successful achievements are generally inclined to adopt beneficial health behavior that may contribute to an enhanced QoL [64]. Some concepts of self-efficacy are associated with concepts of QoL from a need-satisfaction perspective. It is possible that the extent to which people succeed in achieving their goals may be associated with the degree in which human needs are satisfied. It is also plausible that persons who succeed in easily achieving their goals, more often fulfill their needs and subsequently experience an improved QoL.
When we compare our results to models that explain socioeconomic health differences, we can determine certain resemblances, for example, explanations provided in the reserve capacity model indicate similarities. This model suggests that those persons with a low SES have a more moderate bank of psychosocial resources and, consequently, are more inclined to develop inferior physical health [65]. Findings supporting this framework are in accordance with our results. We also ascertained an indirect relationship between SES and QoL through psychosocial determinants. We contend that this framework may also be applied to explain socioeconomic differences in QoL.
A number of methodological issues may be relevant while interpreting our results. First, we employed a cross-sectional study design. Therefore, we concentrated on the current situation and did not investigate determinants of change in QoL. To establish whether the proposed relationships maintain over a period of time and to specify the direction of cause and effect, longitudinal randomized controlled trials in more substantial study samples will be required. Second, the mean age of participants with a low SES was significantly higher compared with participants with a high SES. However, this difference in mean age was only 3 years. Therefore, we presuppose that this difference is not clinically relevant and would not have influenced our findings. Additionally, we noticed a somewhat skewed gender distribution in relationship to the SES. In our study sample, as well as in the general population of older adults, older females are more often less educated and receive less income than older males. Third, all study participants live in a developed economy meeting their basic needs such as having food, shelter, clothing, sanitation, education, and healthcare. We may expect that income has a greater effect on the well-being of persons living in underdeveloped economies [61]. Therefore, in order to draw conclusions about the relationship between SES and QoL in older adults living in underdeveloped countries, our study should be replicated in other districts and countries.
The results that are presented indicate potential determinants to address in order to ultimately enhance QoL in both (relative) low- and high-SES older adults. Longitudinal analyses are required to determine whether the proposed relationships maintain over a period of time. To improve QoL in older adults, we need an increased focus on the socioeconomic psychosocial differences and subsequently develop tailored interventions to improve psychosocial functioning in the community-dwelling older population.
References
Moons, P., Budts, W., & De Geest, S. (2006). Critique on the conceptualisation of quality of life: A review and evaluation of different conceptual approaches. International Journal of Nursing Studies, 43(7), 891–901.
Barcaccia, B., Esposito, G., Matarese, M., Bertolaso, M., Elvira, M., & De Marinis, M. G. (2013). Defining quality of life: A wild-goose chase? Europe’s Journal of Psychology, 9(1), 185–203.
Holmes, S. (2005). Assessing the quality of life: Reality or impossible dream? A discussion paper. International Journal of Nursing Studies, 42(4), 493–501.
Brown, J., Bowling, A., & Flynn, T. (2004). Models of quality of life: A taxonomy, overview and systematic review of the literature. Bristol, London: European Population Forum for Ageing Research
Farquhar, M. (1995). Elderly people’s definitions of quality of life. Social Science and Medicine, 41(10), 1439–1446.
Gasper, D. (2010). Understanding the diversity of conceptions of well-being and quality of life. The Journal of Socio-Economics, 39(3), 351–360.
WHOQOL group. (1995). The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Social Science & Medicine, 41(10), 1403–1409.
Wilhelmson, K., Andersson, C., Waern, M., & Allebeck, P. (2005). Elderly people’s perspectives on quality of life. Ageing and Society, 25(4), 585–600.
Gabriel, Z., & Bowling, A. (2004). Quality of life from the perspectives of older people. Ageing and Society, 24(5), 675–691.
Netuveli, G., & Blane, D. (2008). Quality of life in older ages. British Medical Bulletin, 85, 113–126.
Ruta, D., Camfield, L., & Donaldson, C. (2007). Sen and the art of quality of life maintenance: Towards a general theory of quality of life and its causation. The Journal of Socio-Economics, 36(3), 397–423.
Costanza, R., Fisher, B., Ali, S., Beer, C., Bond, L., Boumans, R., et al. (2007). Quality of life: An approach integrating opportunities, human needs, and subjective well-being. Ecological Economics, 61(2), 267–276.
George, L. K. (2010). Still happy after all these years: Research frontiers on subjective well-being in later life. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 65(3), 331–339.
Huguet, N., Kaplan, M. S., & Feeny, D. (2008). Socioeconomic status and health-related quality of life among elderly people: Results from the Joint Canada/United States Survey of Health. Social Science and Medicine, 66(4), 803–810.
Pinquart, M., & Sörensen, S. (2000). Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychology and Aging, 15(2), 187–224.
Zaninotto, P., Falaschetti, E., & Sacker, A. (2009). Age trajectories of quality of life among older adults: Results from the English Longitudinal Study of Ageing. Quality of Life Research, 18(10), 1301–1309.
Brett, C. E., Gow, A. J., Corley, J., Pattie, A., Starr, J. M., & Deary, I. J. (2012). Psychosocial factors and health as determinants of quality of life in community-dwelling older adults. Quality of Life Research, 21(3), 505–516.
Bowling, A., Seetai, S., Morris, R., & Ebrahim, S. (2007). Quality of life among older people with poor functioning. The influence of perceived control over life. Age and Ageing, 36(3), 310–315.
Netz, Y., Wu, M., Becker, B. J., & Tenenbaum, G. (2005). Physical activity and psychological well-being in advanced age: A meta-analysis of intervention studies. Psychology and Aging, 20(2), 272.
Garatachea, N., Molinero, O., Martínez-García, R., Jiménez-Jiménez, R., González-Gallego, J., & Márquez, S. (2009). Feelings of well being in elderly people: Relationship to physical activity and physical function. Archives of Gerontology and Geriatrics, 48(3), 306–312.
Olivares, P. R., Gusi, N., Prieto, J., & Hernandez-Mocholi, M. A. (2011). Fitness and health-related quality of life dimensions in community-dwelling middle aged and older adults. Health and Quality of Life Outcomes, 9, 117.
Chang, M., Kim, H., Shigematsu, R., Nho, H., Nishijima, T., & Tanaka, K. (2001). Functional fitness may be related to life satisfaction in older Japanese adults. International Journal of Aging and Human Development, 53(1), 35–50.
Takata, Y., Ansai, T., Soh, I., Awano, S., Yoshitake, Y., Kimura, Y., et al. (2010). Quality of life and physical fitness in an 85-year-old population. Archives of Gerontology and Geriatrics, 50(3), 272–276.
Spirduso, W. W., & Cronin, D. L. (2001). Exercise dose–response effects on quality of life and independent living in older adults. Medicine and Science in Sports and Exercise, 33(6), S598–S608.
Brydon, L., Edwards, S., Mohamed-Ali, V., & Steptoe, A. (2004). Socioeconomic status and stress-induced increases in interleukin-6. Brain, Behavior, and Immunity, 18(3), 281–290.
Cohen, S., & Janicki-Deverts, D. (2012). Who’s stressed? Distributions of psychological stress in the United States in probability samples from 1983, 2006, and 2009. Journal of Applied Social Psychology, 42(6), 1320–1334.
Broese van Groenou, M. I., & Van Tilburg, T. (2003). Network size and support in old age: Differentials by socio-economic status in childhood and adulthood. Ageing and Society, 23(05), 625–645.
Stringhini, S., Berkman, L., Dugravot, A., Ferrie, J. E., Marmot, M., Kivimaki, M., et al. (2012). Socioeconomic status, structural and functional measures of social support, and mortality: The British Whitehall II Cohort Study, 1985–2009. American Journal of Epidemiology, 175(12), 1275–1283.
Savikko, N., Routasalo, P., Tilvis, R. S., Strandberg, T. E., & Pitkälä, K. (2005). Predictors and subjective causes of loneliness in an aged population. Archives of Gerontology and Geriatrics, 41(3), 223–233.
Kubzansky, L. D., Subramanian, S., Kawachi, I., Fay, M. E., Soobader, M., & Berkman, L. F. (2005). Neighborhood contextual influences on depressive symptoms in the elderly. American Journal of Epidemiology, 162(3), 253–260.
Mair, C., Roux, A. D., & Galea, S. (2008). Are neighbourhood characteristics associated with depressive symptoms? A review of evidence. Journal of Epidemiology and Community Health, 62(11), 940–946.
Stimpson, J. P., Ju, H., Raji, M. A., & Eschbach, K. (2007). Neighborhood deprivation and health risk behaviors in NHANES III. American Journal of Health Behavior, 31(2), 215–222.
Koster, A., Bosma, H., van Groenou, M. I. B., Kempen, G. I., Penninx, B. W., van Eijk, J. T., et al. (2006). Explanations of socioeconomic differences in changes in physical function in older adults: Results from the Longitudinal Aging Study Amsterdam. BMC Public Health, 6(1), 244.
Broese van Groenou, M. I., Deeg, D. J., & Penninx, B. W. (2003). Income differentials in functional disability in old age: Relative risks of onset, recovery, decline, attrition and mortality. Aging Clinical and Experimental Research, 15(2), 174–183.
Joreskog, K., & Sorbom, D. (1989). LISREL 7: A guide to the program and applications. Chicago, IL: SPSS Inc.
Thomas, S., Reading, J., & Shephard, R. J. (1992). Revision of the physical activity readiness questionnaire (PAR-Q). Canadian Journal of Sport Sciences, 17(4), 338–345.
Statistics Netherlands. (1989). Health interview survey in the Netherlands. Voorburg/Heerlen: Statistics Netherlands.
Ruwaard, D., Kramers, P., Van den Berg Jeths, A., & Achterberg, P. (1993). Public health status and forecasts. The health status of the Dutch population over the period 1950–2010. The Hague, The Netherlands: National Institute for Public Health and the Environment.
Hyde, M., Wiggins, R. D., Higgs, P., & Blane, D. B. (2003). A measure of quality of life in early old age: The theory, development and properties of a needs satisfaction model (CASP-19). Aging & Mental Health, 7(3), 186–194.
Bowling, A. (2009). The psychometric properties of the older people’s quality of life questionnaire, compared with the CASP-19 and the WHOQOL-OLD. Current Gerontology and Geriatrics Research, 2009, 298950.
Gierveld, J. D. J., & Van Tilburg, T. (2006). A 6-item scale for overall, emotional, and social loneliness confirmatory tests on survey data. Research on Aging, 28(5), 582–598.
Lubben, J., Blozik, E., Gillmann, G., Iliffe, S., von Renteln Kruse, W., Beck, J. C., et al. (2006). Performance of an abbreviated version of the Lubben Social Network Scale among three European community-dwelling older adult populations. The Gerontologist, 46(4), 503–513.
Kempen, G., & Van Eijk, L. (1995). The psychometric properties of the SSL12-I, a short scale for measuring social support in the elderly. Social Indicators Research, 35(3), 303–312.
Bouma, J., Ranchor, A. V., Sanderman, R., & Van Sonderen, E. (2012). Assessment of symptoms of depression by means of the CES-D: A manual. Groningen: Stichting Drukkerij Regenboog.
Lewinsohn, P. M., Seeley, J. R., Roberts, R. E., & Allen, N. B. (1997). Center for Epidemiologic Studies Depression Scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychology and Aging, 12(2), 277.
Sherer, M., Maddux, J. E., Mercandante, B., Prentice-Dunn, S., Jacobs, B., & Rogers, R. W. (1982). The self-efficacy scale: Construction and validation. Psychological Reports, 51(2), 663–671.
Bosscher, R. J., & Smit, J. H. (1998). Confirmatory factor analysis of the general self-efficacy scale. Behaviour Research and Therapy, 36(3), 339–343.
Rikli, R. E., & Jones, C. J. (1999). Development and validation of a functional fitness test for community-residing older adults. Journal of Aging and Physical Activity, 7, 129–161.
Podsiadlo, D., & Richardson, S. (1991). The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. Journal of the American Geriatrics Society, 39(2), 142.
Brown, A. F., Ettner, S. L., Piette, J., Weinberger, M., Gregg, E., Shapiro, M. F., et al. (2004). Socioeconomic position and health among persons with diabetes mellitus: A conceptual framework and review of the literature. Epidemiologic Reviews, 26(1), 63–77.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Lawrence Erlbaum.
Enders, C. K., & Bandalos, D. L. (2001). The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural Equation Modeling, 8(3), 430–457.
Allison, P. (2012). Handling missing data by maximum likelihood. Cary, NC: SAS Institute Inc. (paper 312-2012).
Wheaton, D. (1977). Assessing reliability and stability in panel models. Sociological Methodology, 8, 84–136.
Tabachnick, B., & Fidell, L. (2001). Using multivariate statistics. Boston: Pearson Education, Allyn & Bacon.
Barrett, P. (2007). Structural equation modelling: Adjudging model fit. Personality and Individual Differences, 42(5), 815–824.
Steiger, J. H. (2007). Understanding the limitations of global fit assessment in structural equation modeling. Personality and Individual Differences, 42(5), 893–898.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107(2), 238.
MacCallum, R. C., Browne, M. W., & Sugawara, H. M. (1996). Power analysis and determination of sample size for covariance structure modeling. Psychological Methods, 1(2), 130.
Ahuvia, A. C. (2002). Individualism/collectivism and cultures of happiness: A theoretical conjecture on the relationship between consumption, culture and subjective well-being at the national level. Journal of Happiness Studies, 3(1), 23–36.
Schenk, L., Meyer, R., Behr, A., Kuhlmey, A., & Holzhausen, M. (2013). Quality of life in nursing homes: results of a qualitative resident survey. Quality of Life Research, 22(10), 2929–2938.
White, S. M., Wójcicki, T. R., & McAuley, E. (2009). Physical activity and quality of life in community dwelling older adults. Health and Quality of life outcomes, 7(10).
Bandura, A. (1997). Self-efficacy: The exercise of control. New York: Freeman.
Gallo, L. C., Bogart, L. M., Vranceanu, A., & Matthews, K. A. (2005). Socioeconomic status, resources, psychological experiences, and emotional responses: A test of the reserve capacity model. Journal of Personality and Social Psychology, 88(2), 386.
Acknowledgments
The study was funded by ZonMw: The National Care for the Elderly Program (The Netherlands), Contract No.: 60.61900.98.452.
Ethical standard
The study has been approved by the ethical committee of the Institute of Human Movement Sciences Groningen and has been performed in accordance with the ethical standards as stated in the 1964 Declaration of Helsinki and its later amendments. All persons granted their informed consent prior to their inclusion in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bielderman, A., de Greef, M.H.G., Krijnen, W.P. et al. Relationship between socioeconomic status and quality of life in older adults: a path analysis. Qual Life Res 24, 1697–1705 (2015). https://doi.org/10.1007/s11136-014-0898-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-014-0898-y