
Abstract
Purpose
Mental well-being has aroused interest in Europe as an indicator of population health. The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) was developed in the United Kingdom showing good face validity and has been previously adapted into Spanish. The aim of this study is to assess the validity and reliability of the Spanish version of WEMWBS in the general population.
Methods
Cross-sectional home face-to-face interview survey with computer-assisted personal interviewing was administered with the 2011 Catalan Health Interview Survey Wave 3, which is representative of the non-institutionalized general population of Catalonia, Spain. A total of 1,900 participants 15+ years of age were interviewed. The Spanish version of WEMWBS was administered together with socioeconomic and health-related variables, with a hypothesized level of association.
Results
Similar to the original, confirmatory factor analysis fits a one-factor model adequately (CFI = 0.974; TLI = 0.970; RMSEA = 0.059; χ 2 = 584.82; df = 77; p < .001) and has a high internal consistency (Cronbach’s alpha = 0.930; Guttman’s lambda 2 = 0.932). The WEMWBS discriminated between population groups in all health-related and socioeconomic variables, except in gender (p = 0.119), with a magnitude similar to that hypothesized. Overall, mental well-being was higher for the general population of Catalonia (average and whole distribution) than that for Scotland general population.
Conclusions
The Spanish version of WEMWBS showed good psychometric properties similar to the UK original scale. Whether better mental well-being in Catalonia is due to methodological or substantive cultural, social, or environmental factors should be further researched.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is an increasing interest in the mental well-being as an indicator of the health progress of the populations [1]. International organizations such as the Organization for Economic and Co-operation and Development (OECD), the European Commission (EC), and the United Nations (UN) include mental well-being as a possible indicator of societal progress [2]. Mental well-being is a construct reflecting a positive disposition that enables the individual to reach better mental health even in adverse circumstances, and is typically conceptualized to include two components: hedonia and eudaimonia. Hedonia is a psychological state of the subjective experience of happiness and concerns the experience of pleasure versus displeasure broadly construed to include all judgments about the good/bad elements of life [3]. Eudaimonia focuses on cognitive and/or moral aspects of a life well-lived [4], and it occurs when people’s life activities are most congruent with values and are holistically or fully engaged [5].
Mental well-being is recognized for having major consequences for health and social outcomes [6, 7], and for being associated with health-related quality of life (HRQoL) improvements and illness prevention [8, 9]. Higher levels of mental well-being are linked to lower risks of mental and physical disorders, disability, and use of health services, being a strong predictor of mental disorders [10, 11] and all-cause mortality [12]. These findings have attracted the attention of both policymakers and the scientific community, leading to greater efforts for improving its measurement and application [1, 13].
Existing instruments do not measure both hedonic and eudaimonic components of mental well-being, as the Ryff’s Scale of Psychological Well-being [14], the Satisfaction With Life Scale [15], the Positive and Negative Affect Scale [16], the Short Depression-Happiness Scale [17], or the World Health Organization (WHO) Well-being Index [18], and as a consequence, they are not suitable to measure mental well-being as it is most commonly conceptualized. On the other hand, the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) [19] was developed and validated, from both English and Scottish student samples and from two Scottish population datasets, to overcome some of the most relevant shortcomings of existing instruments and measures. Both hedonic and eudaimonic dimensions of mental well-being focused on the positive aspects of mental health including affective–emotional aspects, cognitive–evaluative dimensions, and psychological functioning. The WEMWBS was developed by an expert panel apprising the relevant scientific literature and applying qualitative research with focus groups. It was validated showing that one-factor model was the best fitting model. Furthermore, the WEMWBS is short enough to be used in population-level surveys and it showed high validity and reliability [19]. The WEMWBS was designed to measure positive mental health in a broad spectrum of values, without especial focus in the extremes of the mental health continuum. The WEMWBS concentrates in the assessment of the general population WEMWBS, for monitoring potential changes and comparing values across subpopulations.
The objective of this study was to assess the validity and reliability of the Spanish version of WEMWBS in a representative sample of the general population of Catalonia, Spain, following similar procedures of those used for the original scale. We hypothesized that the Spanish version of WEMWBS would fit a one-factor model and it would discriminate a wide range of socioeconomic and health-related groups. We also expected the WEMWBS to be positively related with indicators of better physical and mental health status (self-perceived health status, HRQoL, physical activity), and negatively related with psychological distress, disability, chronic illness, and difficulties of daily living. Finally, we expected that WEMWBS scores to be associated with individual’s employment civil status and age and, more generally, with variables indicating better socioeconomic status, as income and social class. According to previous studies [20], we did not expect associations between gender and positive mental health.
Methods
The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS)
The WEMWBS measures mental well-being in the previous 2 weeks. It is an ordinal scale comprising 14 positively phrased items [19]. Each item provides a 5-point Likert-type scale from “None of the time” to “All of the time” and a global score is obtained adding all the items (range 14–70), higher scores indicating higher levels of mental well-being. The original version of the WEMWBS showed high reliability, low desirability bias, and the CFA supported the single-factor hypothesis [19]. The original WEMWBS scores showed positive correlations with other mental health, well-being, and overall health scales, and negative correlations with negative affect [19].
The cross-cultural adaptation into Spanish included forward and backward translations with evaluation of its clarity, cultural adequacy, and the use of common language, and preliminary validation showed a high internal consistency, good test–retest reliability, and preliminary construct validity [21].
Study population
The Spanish version of the WEMWBS was administered to a subsample of the participants in the 2011 Catalan Health Interview Survey (CHIS) Wave 3, carried out on a representative sample of the general population older than 15 years of Catalonia, a northeastern region of Spain with about 7.5 million inhabitants. Computer-assisted personal interviews were administered by trained interviewers in the respondents’ homes, from July 2011 to December 2011. Participants were selected using a multistage, random sampling strategy. A weighting factor which took into account age, gender, and municipality was applied to restore the representativeness of the population in Catalonia. More detailed information about sample and survey procedures can be found elsewhere [22].
The interviewee could choose in which language he/she desired to conduct the interview; as a result, 892 (47.0 %) interviews in Spanish were done, 931 (49.0 %) in Catalan, 76 (4.0 %) in both languages, and only one in another language. As a preliminary analysis, we checked that there existed measurement invariance in the WEMWBS responses regardless of the language of the interview. We also underwent multigroup analyses of measurement invariance regarding language. Using an alpha level 0.01, the analyses did allow maintaining the hypothesis of metric (χ 2 = 26.137; df = 14; p = 0.025) and scalar equivalence between language versions (χ 2 = 12.49; df = 14; p = 0.567). Thus, the Spanish and Catalan language samples were aggregated in a single sample because no evidence of non-measurement invariance was found. The joint sample was used in all analyses reported here.
Main validity measures
Health-related and socioeconomic variables hypothesized to be associated with some aspects of well-being were selected from CHIS, analyzed in this study, and further classified. These hypotheses were based on the findings of the original WEMWBS UK validation [19], the preliminary validation with Spanish students [21], and a review on well-being carried out by the New Economics Foundation for policymakers’ [20] relation to the expected magnitude of the association: high, moderate, or low.
Expected high level of association
Self-perceived health status is an important variable assessing current health status and it is predictive of future health status and illness. Self-perceived health status was assessed via a single self-administered 5-point Likert item with the following response options: (1) excellent, (2) very good, (3) good, (4) fair, and (5) poor. The GHQ-12 questionnaire, which is used to identify psychological distress [23, 24] and whose Spanish version is valid and reliable, was also expected to be highly associated with well-being. Scores on the GHQ-12 range from 0 to 12; higher scores show greater psychological distress. Here, the dichotomous scoring method (0-0-1-1) was used [23, 24], and respondents were finally classified as having “good mental health” (total score from 0 to 2) and “at risk of mental disorder” (total score >2) [25, 26].
Net familiar income per month was stratified putting an emphasis in lowest familiar income groups but maintaining an enough number of subjects in each group (<600; 601–1,200; 1,201 –1,800; >1,800; does not know; and no responses). Previous literature shows disadvantaged and marginal groups suffer an important impairment in mental well-being but when needs are covered, mental well-being was restored. Employment status was stratified among 6 groups [students; employed; unemployed; retired; other conditions (housewife; not in education, employment, or training and others); and no responses]. Civil status was stratified among 3 groups (single; married; and widowed/divorced/separated).
Expected moderate level of association
The disability variable measures the impairment in some health-related aspects caused by illnesses or accidents. This variable was defined as continuous variable, by the means of the sum of 11 items, and as dichotomous variable (presence and absence). Physical activity was defined in 5 groups ordered by the level of activity (very active; moderately active; mild active; low active; and sedentary). The 3-level EQ-5D is a brief, multi-attribute, generic, preference-based health status measure [27, 28]. The EQ-5D covers five dimensions of health (mobility, self-care, usual activities, pain or discomfort, and anxiety or depression) with three levels of severity in each dimension (no problems, some problems, and extreme problems). We used the Spanish version of EQ-5D and time trade-off preference values from the Catalan general population [29]. EQ-5D scores range from negative values to 1, higher scores indicating better health status, and 0 is equal to death. The single-item EQ-5D visual analogue scale (EQ-5D-VAS) (range 0–100) was also used.
Social class was defined in 6 groups (I = Higher managerial, administrative or professional; II = Intermediate managerial, administrative, or professional; III = Supervisory or clerical and junior managerial, administrative or professional, and skilled manual workers; IV = Semi- and unskilled manual workers; V = Informal or lowest grade workers; no responses) [22].
Expected lower level of association
Age was stratified in meaningful strata for health comparisons, as indicated by previous literature (15–24; 25–44; 45–74; and ≥75 years). Educational level was stratified in 3 groups: (primary = Basic education or lower; secondary = High school studies or equivalent; and higher = University/College studies or higher). Chronic illness was assessed as current presence of any chronic condition, explored by a checklist of 28 self-reported chronic illnesses (e.g., the presence of diabetes, asthma, or anemia), risk factors for chronic illness (e.g., high levels of cholesterol or blood pressure), and 6 open-ended questions. This variable was defined as a dichotomous variable (presence and absence). Difficulties or limitations on daily living measure the functional limitation of an individual for health causes. It is composed by 20, and we categorized it as a dichotomous variable (presence and absence). These questions were administered at all people over or equal to 65 years old, and only people under 65 years old who needed help from other people to make daily activities for health causes.
Statistical analysis
Measurement model and invariance
Confirmatory factor analysis was conducted using mean- and variance-adjusted weighted least squares estimation on the sample polychoric correlation matrix to test the appropriateness of the pre-hypothesized one-factor structure of the WEMWBS. This method is most advisable when ordinal items are skewed [30, 31]. Model fit was tested considering CFI ≥ 0.95, TLI ≥ 0.95, and RMSEA ≤ 0.08 [32]. Due to the large sample size, a chi-squared statistic with p values under 0.05 indicates a significant discrepancy between sample and model covariance structures [33]. However, large sample sizes may lead to an overstatement of lack of fit [34].
Reliability
The distribution of the item responses from complete responders was analyzed in order to detect highly skewed distributions and floor or ceiling effects. Popular responses were quantified in order to assess relevance, sensitivity, and signs of inappropriateness. Model reliability was assessed as the internal consistency of the global score using Cronbach′s alpha and Guttman’s lambda 2 coefficients [35], and model-based internal consistency approach described by Bentler [36]. Values over 0.7 were considered satisfactory for all three coefficients [37, 38]. Corrected item-total score correlations were calculated for each item for further assessment of internal consistency. Adequate item-total score correlations ranged between ≥0.2 and <0.8. Values higher than 0.8 were considered inappropriate, because questions that correlated too highly with other questions provide little additional information [39].
Convergent validity
The ability of the WEMWBS total score to distinguish among different groups was assessed. We hypothesized that differences in WEMWBS scores would be found across categories of the main validity variables. As described below, such differences or associations were anticipated to vary in intensity from high to low. Subgroups’ score differences were assessed using Mann–Whitney U test when comparing two independent groups: Kruskal–Wallis when using test for higher than two independent groups, and Jonckheere’s test for ordered differences among groups, as appropriate. Spearman’s rank correlation coefficients were used with continuous variables. Trend analysis was used to detect significant differences in each self-perceived health status with the WEMWBS scores.
The magnitude of the association was estimated with effect size (ES) to compare average differences in mental well-being mean between subgroups in categorical variables and correlation coefficients in continuous variables. The cutoffs and the interpretation of ES were low (|0.20| ≤ ES ≥ |0.50|), moderate (|0.50| < ES ≥ |0.80|), and high (ES >|0.80|) [40, 41]. In the case of continuous measures, the magnitude of the association was assessed by well-established cutoffs for Spearman’s rank correlation coefficients: low (r xy < |0.45|), moderate (|0.45| ≤ r xy ≥ |0.70|), and high (|0.70| > r xy ≤ |1.00|) [41]. Significance tests were all evaluated at the 0.05 level.
Data were analyzed using MPlus, version 5.0 [42] and SPSS version 18.0 (SPSS version 18.0, for Windows, SPSS, Inc., Chicago, Ill.).
Ethics
The CHIS has the rank of official statistics carried out by the Government of the Catalonia region, and it must ensure the confidentiality of the data (Law 23/1998, December 30, of statistics of Catalonia). The content of the CHIS and the whole interview process follows the European Statistics Code of Practice adopted by the European Statistical System Committee [43].
Results
Sample characteristics
Final sample included 1,900 Spanish participants. The characteristics of the sample were as follows 50.2 % were female, the mean age (SD) was 45.9 (18.4), 44.7 % had primary educational level, and 52.2 % were employed. Only 3.4 % reported poor self-perceived health status even though 37.2 % had at least one chronic illness. According to GHQ-12, 13.4 % were at risk of mental disorder and the mean (SD) score of the HRQoL scale EQ-5D index score was 0.88 (0.2) (Table 1).
Psychometric properties
Measurement model and invariance
As mentioned above, no evidence of uniform or non-uniform DIF was found regarding the language of interview, and all analyses presented here were computed for the total combined sample. Goodness of fit for the one-factor confirmatory model was tested. As expected from the large sample size, absolute fit assessed with chi-squared test was significant (χ 2 = 584.82; df = 77; p < 0.001). Nonetheless, CFI, TLI, and RMSEA showed adequate levels of fit (CFI = 0.974; TLI = 0.970; RMSEA = 0.059).
Reliability
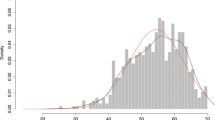
No-item category was without respondents, and item response frequencies showed evidence of skewed distributions. Total score was negatively skewed and leptokurtic (skewness = −1.003; kurtosis = 1.199), mean score was 59.9 (7.8), median score was 59, and inter-quartile ranged between 54 and 66 (Fig. 1). Between 21.4 and 68.9 % responded “all of the time” in some items, but only 6.4 % of the total sample scored the maximum score of the WEMWBS, showing that there was neither ceiling effect (n = 122) nor floor effect (n = 0) (Table 2). WEMWBS showed high internal consistency in total sample (Cronbach’s alpha = 0.930; Guttman’s lambda 2 = 0.932). Model-based internal consistency for the unidimensional model was also very high (0.97). Corrected item-to-total correlations in each item ranged from 0.548 to 0.797 within the desired levels, which supports the contribution of the items to the global score (Table 2).

WEMWBS score distribution in Spanish general population sample
Convergent validity
Table 3 shows the WEMWBS scores by variables’ categories as hypothesized, showing significant differences across subgroups in all socioeconomic and health-related variables assessed, except gender (p = 0.119) (Table 3). In line with prior hypotheses, we observed lower WEMWBS scores in respondents with poorest self-perceived health status. This association followed a quadratic gradient from poor to excellent health (“Poor” ES = −2.946, “Fair” = −1.402 vs. “Excellent;” quadratic trend p < 0.001). There was also a high association with being at risk of mental disorder (“Being at risk of mental disorder” vs. “Good mental health” ES = −1.469) and lowest net familiar income (<600€/month vs. >1,800/month ES = −1.059). Differently from our prior hypotheses, we found a lower magnitude of association than expected in employment status (Unemployed vs. Student ES = −0.622) and civil status (Widowed/Divorced/Separated vs. Married/Living as a couple ES = −0.328) showing moderate and low magnitude of the association, respectively (Table 3).
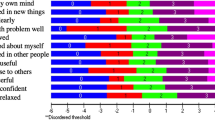
As hypothesized, a moderate association of WEMWBS scores was shown for social class and sedentary respondents. Negative and moderate associations were found in psychological distress (Fig. 2). Respondents with any disability showed higher ES than expected and number of disabilities had lower correlations than expected (Table 3; Fig. 2). Finally, low-magnitude associations with lower WEMWBS scores were found in respondents with any chronic illness and education. A higher association than expected was found in respondents with any limitation of daily living showing high and moderate ES, respectively (Table 3).

Scatter plot and Spearman’s correlations between the Spanish version of WEMWBS and the GHQ-12, EQ-5D scales, and a number of disabilities
Discussion
Building on a previous preliminary work on a student’s sample [21], this study adds important information about measurement model and invariance, reliability, and convergent validity of the Spanish version of WEMWBS in the adult general population. The previous study showed that it is an intelligible instrument and covered some concepts associated with well-being, providing reliable and valid estimates in a very similar way to the original instrument. These results suggest that the original and the adapted versions have cross-cultural equivalence. Nevertheless, some differences may exist between general populations of Catalonia and Scotland regarding the level of mental well-being, as indicated by a more skewed distribution of the WEMWBS scores in the former, compared with the quasi-normal distribution in the latter. These differences deserve further research.
The WEMWBS has become one of the most used instruments to measure mental well-being, making it useful in health population-level surveys and allowing for international comparisons. The validation of this questionnaire will provide the Spanish research community with an instrument apt to explore those factors with a positive impact on people’s lives that might help study to develop ways for empowering individuals, so that they can improve their own lives, all the while helping us to assess important areas of people’s emotional and social needs concept [44].
Both Spanish and Scottish versions of the WEMWBS were developed as an instrument for assessment in the general population fitting a one-factor model. The factor structure tested in our study shows that a single factor adequately reproduces item relationships, lending support to the scale theoretical model of well-being as proposed by the original authors. However, the Spanish adaptation of the WEMWBS found differences in score and distribution with the Scottish sample. While the Scottish sample is quite normally distributed with a mean of 50.29 (95 % CI 49.6–50.89), the Spanish sample was highly skewed distributions with a significantly higher mean of 59.9 (95 % CI 52.1–67.7). Noticeably, both the original Scottish and the Spanish samples fit a similar model, which points at real differences in the latent positive mental health trait distribution. However, we cannot rule out spurious effects arising from social desirability bias or real cultural differences between both samples. Further research is needed to establish whether the source of the reason for dissimilar distributions resides in true differences in well-being or cultural issues affecting the questionnaire model. Such study would require measurement invariance analyses with the data from both populations. Provided that no DIF is found between both populations, potentially fruitful lines of research open regarding the causes (e.g., social determinants of health) of these differences.
Our study has several limitations that deserve further comment. First, a gold standard measure of mental well-being does not exist. In order to overcome this, we adopted a pragmatic approach and covered a wide range of aspects related to mental well-being using several different instruments. In previous reports, the Spanish version of the WEMWBS had shown the ability to measure positive and negative affect and life satisfaction [21]. The current study added evidence of a moderate negative association with psychological distress and a mild positive association with HRQoL. Therefore, even acknowledging that complete validity could not be established, the Spanish version of the WEMWBS shows very similar validity to the original version. Second, the cross-sectional nature of the designs impeded the assessment of scale responsiveness. Recently, Maheswaran et al. showed good responsiveness of WEMWBS in a wide range of mental health interventions [45]. There is therefore need of pursuing evidence about the responsiveness of the Spanish WEMWBS in an appropriate longitudinal study. Finally, we could not administer some questionnaires related to mental well-being concepts, used in the original validation, because of the unavailability of validated Spanish versions. Nevertheless, some questionnaires and instruments were used in the Spanish validation of the WEMWBS and showed that satisfaction with life, overall health, HRQoL, and positive affect were positively covered with mental well-being, and psychological distress and negative affect were negatively covered. These results suggest that the Spanish version of the WEMWBS covers a wide range of positive and negative aspects of health and might suggest the instruments used in the original validation, but not administered in the Spanish validation, could be covered, too.
Despite these limitations, current results indicate that the WEMWBS fits adequately as one-factor model in the population, and covers a wide range of aspects of well being to compensate the lack of a gold standard. Moreover, the cognitive debriefing in the initial phases of the adaptation process [21] supports the good face validity of the questionnaire. These results suggest that our conclusions hold true. Moreover, the Spanish version was able to discriminate a wide range of socioeconomic groups and health-related conditions. Discriminative capacity of the WEMWBS among socioeconomic groups makes possible to take studies about social, economic, or health inequities and, among health-related conditions, points at the ability of the WEMWBS to measure the impact of chronic physical and mental conditions on mental well-being
Comparison of the Spanish and Scottish versions of the WEMWBS
Unidimensionality of the WEMWBS
Both Spanish and Scottish versions of the WEMWBS were developed as an instrument fitting a one-factor model. The factor structure tested in our study shows that a single factor adequately reproduces item relationships, lending support to the scale theoretical model of well-being as proposed by the original authors. Moreover, this factor is identically associated with the items, both in factor loading and item means, when comparing language groups. Nevertheless, the internal consistency of the Spanish version might suggest redundancy. Similar results were found for the English version. To solve this, Tennant et al. [19] developed a shortened English version of WEMWBS with 7 items [46]. Further research is needed about the internal consistency of the Spanish version and the development of a shortened questionnaire, as appropriate.
Discrimination of socioeconomic groups and health-related conditions
Both versions discriminated between a wide range of socioeconomic groups and health-related conditions. Discriminative capacity of the WEMWBS between socioeconomic groups makes possible to take studies about social, economic, or health inequalities and, between health-related conditions, points at the ability of the WEMWBS to measure the impact of chronic physical and mental conditions on mental well-being. Finally, we must point out that the WEMWBS provides a useful mental well-being measure that allows approaching positive health and aspects related with positive health covering mental well-being as a whole. International organizations such as OECD, the EC, and the UN are currently moving their interest for studying population welfare from economic indicators such as gross national product to individual perceptions of well-being. The WEMWBS is a valid indicator, which approaches mental health from a positive point of view, sensitive to aspects such as good functionality, satisfaction with life, happiness, and HRQoL. The scale provides clinicians with an instrument for initial exploration of mental health status understood as a continuum, and out of its pathological extremes. The WEMWBS is also valid to detect changes in negative aspects of health, as for instance mental distress, illness, disability, and impairment in functionality in individuals. Results indicate that it is also sensitive to social and economic characteristics usually associated with better health status as well as it can detect improvements in a wide range of participants occurring in mental health interventions [45]. Even though the present study is cross-sectional, and does not cover the instrument’s sensitivity to change, our results point toward an adequate responsiveness to individual or environmental changes. In this fashion, the WEMWBS would allow monitoring the evolution of positive mental health of a population or subpopulations in regular health surveys, which makes it useful for policy makers.
Conclusions
The Spanish version of the WEMWBS has adequate equivalence with the original version, it shows high levels of internal consistency and reliability, and it fits adequately as one dimension of mental well-being. It is a short measure, which is acceptable and meaningful to general population groups and capable of distinguishing between different population groups and health conditions. The scale is likely to appeal to those evaluating mental health promotion initiatives, because of its positive focus. The general population of Catalonia showed, on average, a better mental well-being than that in the Scottish general population. Given the similar psychometric properties of both versions of the questionnaire, research is needed to further assess the role of determinants of well-being in both populations.
References
Abdallah, S., Mahony, S., Marks, N., Michaelson, J., Seaford, C., Stoll, L. et al. (2011). http://www.neweconomics.org/publications/measuring-our-progress. Accessed 15 Sep 2012.
Organisation for Economic and Co-operation and Development (2007). http://www.oecd.org/. Accessed 1 Sep 2012.
Diener, E., & Diener, M. (1995). Cross-cultural correlates of life satisfaction and self-esteem. Journal of Personality and Social Psychology, 68, 653–663.
Berridge, K. C., & Kringelbach, M. L. (2011). Building a neuroscience of pleasure and well-being. Psychol Well Being, 1, 1–3.
Waterman, A. S. (1993). Two conceptions of happiness: Contrasts of personal expressiveness (eudaimonia) and hedonic enjoyment. Journal of Personality and Social Psychology, 64, 678–691.
Huppert, F. A., & Wittington, J. E. (2012). Positive mental health in individuals and populations. Oxford: Oxford University Press.
Linley, P. A., & Joseph, S. (2012). Positive psychology in practice. NJ: Wiley.
Seligman, M. E., & Csikszentmihalyi, M. (2000). Positive psychology. An introduction. American Psychologist, 55, 5–14.
Keyes, C. L. (2007). Promoting and protecting mental health as flourishing: a complementary strategy for improving national mental health. American Psychologist, 62, 95–108.
Tennant, R., Fishwick, R., Platt, S., Joseph, S., & Stewart-Brown, S. (2012). Monitoring positive mental health in Scotland: validating the Affectometer 2 scale and developing the Warwick-Edinburgh Mental Well-being scale for the UK. Edinburgh: NHS Health Scotland.
Keyes, C. L., Dhingra, S. S., & Simoes, E. J. (2010). Change in level of positive mental health as a predictor of future risk of mental illness. American Journal of Public Health, 100, 2366–2371.
Keyes, C. L., & Simoes, E. J. (2012). To flourish or not: Positive mental health and all-cause mortality. American Journal of Public Health, 102, 2164–2172.
The Scottish Government (2011). http://www.scotland.gov.uk/Topics/Statistics/Browse/Health/scottish-health-survey. Accessed 12 July 2012.
Ryff, C. D., & Keyes, C. L. (1995). The structure of psychological well-being revisited. Journal of Personality and Social Psychology, 69, 719–727.
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49, 71–75.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal of Personality and Social Psychology, 54, 1063–1070.
Joseph, S., Linley, P. A., Harwood, J., Lewis, C. A., & McCollam, P. (2004). Rapid assessment of well-being: The Short Depression-Happiness Scale (SDHS). Psychol Psychother, 77, 463–478.
Bench, P. (2004). Measuring the dimensions of psychological general well-being by the WHO-5. QoL Newsletter, 32, 15–16.
Tennant, R., Hiller, L., Fishwick, R., Platt, S., Joseph, S., Weich, S., et al. (2007). The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual Life Outcomes, 5, 63–76.
Stoll, L., Michaelson, J., & Seaford, C. (2012). http://www.neweconomics.org/sites/neweconomics.org/files/Well-being_Evidence_for_Policy_final.pdf. Accessed 22 Aug 2012.
Lopez, M. A., Gabilondo, A., Codony, M., Garcia-Forero, C., Vilagut, G., Castellvi, P., et al. (2013). Adaptation into Spanish of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS) and preliminary validation in a student sample. Quality of Life Research, 22, 1099–1104.
IDESCAT. (2008). www.gencat.cat/salut/esca. Accessed 8 March 2012.
Goldberg, D., & Williams, P. (1988). A user’s guide to the General Health questionnaire. Windsor, UK: NFER-Nelson.
Goldberg, D. P., & Blackwell, B. (1970). Psychiatric illness in general practice. A detailed study using a new method of case identification. British Medical Journal, 1, 439–443.
Lobo, A., & Muñoz, P. E. (1996). Cuestionario de salud general GHQ (General Health Questionnaire). Guía para el usuario de las distintas versiones en lengua española validadas. Barcelona: Masson.
Sanchez-Lopez, M. P., & Dresch, V. (2008). The 12-Item General Health Questionnaire (GHQ-12): Reliability, external validity and factor structure in the Spanish population. Psicothema, 20, 839–843.
Dolan, P. (1997). Modeling valuations for EuroQol health states. Medical Care, 35, 1095–1108.
The EuroQol Group. (1990). EuroQoL -A new facility for the measurement of health-related quality of life. Health Policy, 16, 199–208.
Badia, X., Schiaffino, A., Alonso, J., & Herdman, M. (1998). Using the EuroQoI 5-D in the Catalan general population: Feasibility and construct validity. Quality of Life Research, 7, 311–322.
Muthen, B., & Kaplan, D. (1985). A comparison of some methodologies for the factor analysis of non-normal Likert variables. British Journal of Mathematical and Statistical Psychology, 38, 171–189.
Muthen, B., & Kaplan, D. (1992). A comparison of some methodologies for the factor analysis of non-normal Likert variables: A note on the size of the model. British Journal of Mathematical and Statistical Psychology, 45, 19–30.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modelling, 6, 1–55.
Bentler, P. M., & Bonnet, D. G. (1980). Significance tests and goodness of fit in the anlaysis of covariance structures. Psychological Bulletin, 88, 58–77.
Cole, D. F. A. (1987). Utility of confirmatory factor analysis in test validation research. Journal of Consulting and Clinical Psychology, 55, 584–594.
Sijtsma, K. (2009). On the use, misuse and the very limited usefulness of Cronbach’s Alpha. Psychometrika, 74, 107–120.
Bentler, P. M. (2008). Alpha, dimension-free and model-based internal consistency reliability. Psychometrika, 74, 137–143.
Helms, J., Henze, K., Sass, T., & Mifsud, V. (2006). Treating Cronbach’s alpha realiability coefficients as data in counseling research. The Counseling Psychologist, 34, 630–660.
Weir, J. P. (2005). Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res, 19, 231–240.
Streiner, G. L., & Normal, R. D. (1989). Health measurement scales a practical guide a their development and use. Oxford: Oxford University Press.
Kazis, L. E., Anderson, J. J., & Meenan, R. F. (1989). Effect sizes for interpreting changes in health status. Medical Care, 27, S178–S189.
Cohen, A. (1988). Statistical power for the behavioral sciences. Hillsdale, NJ: Lawrence Eribaum.
Muthen, L. K., & Muthen, B. O. (2010). MPlus user’s guide (1998–2010). Los Angeles, CA: Muthen & Muthen.
Eurostat. (2011). http://www.idescat.cat. Accessed 26 July 2011.
Michaelson, J., Mahony, S., & Schifferes, J. (2012). http://www.neweconomics.org/publications/measuring-well-being. Accessed 23 Aug 2012.
Maheswaran, H., Weich, S., Powell, J., & Stewart-Brown, S. (2012). Evaluating the responsiveness of the Warwick Edinburgh Mental Well-Being Scale (WEMWBS): Group and individual level analysis. Health Qual Life Outcomes, 10, 156–164.
Stewart-Brown, S., Tennant, A., Tennant, R., Platt, S., Parkinson, J., & Weich, S. (2009). Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual Life Outcomes, 7, 15–23.
Acknowledgments
This work was supported by the grants from Instituto de Salud Carlos III (CD12/00440). Additional support included a grant from DIUE of Generalitat de Catalunya (2009 SGR 1095), and the support of Agència de Salut Pública de Catalunya, Subdirecció General de Drogodependències, Generalitat de Catalunya, Spain. The authors are indebted to Núria Duran Adroher and Oriol Cunillera for assistance in the management of databases. We also thank Carme Gasull and Roser Busquets for her assistance in the manuscript preparation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Castellví, P., Forero, C.G., Codony, M. et al. The Spanish version of the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) is valid for use in the general population. Qual Life Res 23, 857–868 (2014). https://doi.org/10.1007/s11136-013-0513-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-013-0513-7