
Abstract
Purpose
Documenting the impact of different types of cancer on daily functioning and well-being is important for understanding burden relative to other chronic medical conditions. This study examined the impact of 10 different cancers and 13 other chronic medical conditions on health-related quality of life.
Methods
Health-related quality of life data were gathered on the Medicare Health Outcomes Survey (MHOS) between 1998 and 2002. Cancer information was ascertained using the National Cancer Institute’s surveillance, epidemiology, and end results program and linked to MHOS data.
Results
The average SF-6D score was 0.73 (SD = 0.14). Depressive symptoms had the largest unique association with the SF-6D, followed by arthritis of the hip, chronic obstructive pulmonary disease/asthma, stroke, and sciatica. In addition, the majority of cancer types were significantly associated with the SF-6D score, with significant negative weights ranging from −0.01 to −0.02 on the 0–1 health utility scale. Distant stage of cancer was associated with large decrements in the SF-6D ranging from −0.04 (prostate) to −0.08 (female breast).
Conclusion
A large number of chronic conditions, including cancer, are associated uniquely with decrements in health utility. The cumulative effects of comorbid conditions have substantial impact on daily functioning and well-being of Medicare beneficiaries.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The majority of US adults (133 million) have at least one chronic medical condition [1], and 12 million Americans are living with cancer [2]. Rothrock et al. [1] documented that most medical conditions have a negative impact on daily functioning and well-being, or health-related quality of life (HRQOL) measured by the Patient-Reported Outcomes Measurement Information System® (PROMIS®). Having a single condition had a negative impact on the PROMIS® HRQOL domain scores of about 0.1–0.4 standard deviations (SDs), depending on the condition and the specific HRQOL domain. Having multiple conditions compared to a single condition impacted negatively in the range of 0.2–0.7 SDs.
Smith et al. [3] found that Medicare managed care beneficiaries with cancer had significantly worse physical health (as measured by the SF-36 v.1 physical component summary score) than those without cancer. Beneficiaries with non-small cell lung, non-Hodgkin lymphoma, female breast, colorectal, or bladder cancer reported worse mental health (on SF-36 v. 1 mental component summary score) than did those without cancer. While the SF-36’s two summary scores provide useful information about physical and mental health, a single preference-based score is very helpful when “bottom-line” comparisons of different therapies are needed such as in comparative effectiveness research. Preference-based measures are designed to integrate across domains of health to provide a summary measure anchored relative to “dead” (score of 0) and “perfect health” (score of 1). A preference-based score is essential when a decision about overall health impact is required.
While it is apparent from the work to date that there are significant associations of cancer with HRQOL, the relative impact of cancer and other health conditions on HRQOL overall is unknown. Although individual unique associations of conditions on HRQOL may seem small, a difference of about 0.03 on a 0–1 preference-based measure may be important; interventions that produce that level of difference are non-trivial. In addition, the cumulative effect of multiple conditions could be substantial. Because the likelihood of chronic conditions increases with age, it is especially important to examine the impacts of these conditions on HRQOL among older individuals.
This study uses the SF-6D [4, 5] to estimate the unique impact of different health conditions on HRQOL for Medicare managed care beneficiaries aged 65 years or older. We also investigate the impact of several types of cancers including both highly prevalent (prostate, female breast, colorectal, non-small cell lung) and less common (endometrial, bladder, melanoma, non-Hodgkin lymphoma, and kidney) cancers. We hypothesize that individuals with cancer will have significantly worse SF-6D scores than those without a chronic medical condition. We also hypothesize that those with cancer will have SF-6D scores that are comparable or worse than those with chronic medical conditions other than cancer. But the differences may vary by cancer type. For example, a previous analysis found that lung cancer was more strongly related to decrements in physical and mental health than other cancers [3]. We also hypothesize that more advanced stage of cancer will be associated with worse HRQOL.
Methods
Sample
Our sample is derived from a dataset that links surveillance, epidemiology, and end results (SEER) cancer registry information with the Medicare Health Outcomes Survey (MHOS). A detailed description of the SEER-MHOS data is provided by Ambs et al. [6]. Briefly, the MHOS evaluated outcomes of care provided by health maintenance organizations to Medicare beneficiaries. During the 1998–2003 study period, the MHOS was a yearly survey administered to a random sample of 1,000 Medicare beneficiaries from each managed care plan under contract with the Centers for Medicare and Medicaid Services (CMS). The SEER program includes population-based cancer registry sites throughout the USA that collect standardized clinical and demographic information for persons with incident cancer [7].
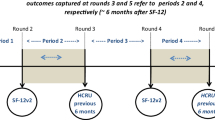
The linked SEER-MHOS dataset includes four MHOS cohorts (baseline and follow-up year): 1998 and 2000; 1999 and 2001; 2000 and 2002; and 2001 and 2003. Response rates to the MHOS baseline surveys ranged from 63 to 72 %. The majority of the MHOSs were completed by mail (88 %), and the rest were administered by phone (12 %). In addition, 12 % of the surveys were completed by a proxy. Across the four cohorts, we identified a total sample of 126,366 persons, both with and without cancer, age 65 or older who had completed at least one survey and responded to the survey questions included in the analysis.
Participants with cancer (n = 22,740; 18 % of the sample) were identified through SEER, and the first survey completed after their cancer diagnosis was used. We restricted this cancer subgroup to those with a first diagnosis of one of nine prevalent cancers: (1) prostate (n = 5,593; 4 % of the sample), (2) female breast (n = 4,311; 3 % of the sample), (3) colorectal (n = 3,012; 2 % of the sample), (4) non-small cell lung (n = 1,792; 1 % of the sample), (5) bladder (n = 1,299; 1 % of the sample), (6) melanoma (n = 1,135; 1 % of the sample), (7) endometrial (n = 902; 1 % of the sample), (8) non-Hodgkin lymphoma (n = 668; 1 % of the sample), and (9) kidney cancer (n = 488; 0.4 % of the sample). The remaining cancer diagnoses were classified as “other” (n = 3,540, 3 % of the sample). Cancer stage data came from SEER. Individuals with more than one cancer diagnosis, or who self-reported cancer, but were not identified in SEER, were excluded. Clauser et al. [8] reported that 13 % of the incident cases had multiple primary cancer diagnoses. For the 103,626 people without a cancer diagnosis, we included the first survey they completed.
Respondents were asked on the MHOS whether they had ever been told by a doctor that they had any of 12 chronic medical conditions: (1) hypertension or high blood pressure (n = 66,968; 53 % of the sample), (2) arthritis of the hip (n = 44,524; 35 % of the sample), (3) arthritis of the hand (n = 40,402; 32 % of the sample), (4) sciatica (n = 26,878; 21 % of the sample), (5) angina or coronary artery disease (n = 18,017; 14 % of the sample), (6) myocardial infarction or heart attack (n = 11,982; 9 % of the sample), (7) stroke (n = 9,479; 8 % of the sample), (8) congestive heart failure (n = 7,893; 6 % of the sample), (9) other heart disease (n = 25,455; 20 % of the sample), (10) diabetes (n = 20,089; 16 % of the sample), (11) chronic obstructive pulmonary disease (n = 15,445; 12 % of the sample), and (12) inflammatory bowel disease (n = 5,882; 5 % of the sample). In addition, they were asked whether they were depressed in the last year (n = 14,815; 12 % of the sample). The percentage of the sample who reported no conditions was 13 % (n = 15,833), 21 % (n = 26,126) reported one condition, 21 % (n = 26,653) reported two conditions, and the remainder reported 3–14 conditions (including cancer).
Measures
The MHOS includes the SF-36 health survey, version 1 [9]. We used the SF-6D preference-based score as the dependent variable in this study. The SF-6D is computed from a subset (11 of the 36 questions) of the SF-36 questionnaire [5]. The SF-6D reduced the SF-36 to six domains (physical functioning, role limitations, social function, pain, emotional well-being, vitality), each comprised of four to six levels, and jointly defined 18,000 health states. Scoring was derived from standard gamble assessments by a population sample from the United Kingdom [5]. We used the revised SF-6D scoring algorithm described by Brazier, Rowen and Hanmer [10]. The algorithm produces scores ranging from 0.30 to 1.00 for those alive [5].
Participants’ self-reported age, gender, race/ethnicity, marital status, education, and income came from the MHOS.
Analysis plan
The analyses were performed using SAS 9.3 and STATA 12 software. We provide descriptive statistics for the sample, followed by least square regression adjusted means on the SF-6D. The SF-6D mean was slightly lower than the median (0.73 vs. 0.75), indicating minor negative skewness (-0.37) and an approximately normal distribution of standard errors for regression coefficients [11]. We estimated the unique associations of each chronic condition with the SF-6D, controlling for the other conditions, education (8th grade or less; some high school; high school graduate; some college; 4 year college graduate; >4 year college degree), gender, marital status (married; widowed; separated; divorced; never married), age, race/ethnicity (Hispanic; non-Hispanic white; non-Hispanic black; Asian; American Indian; other race; race/ethnicity missing), income (<$10,000/year; $10,000–19,999/year; $20,000–29,999/year; $30,000–39,999/year; $40,000–49,999/year; $50,000–79,999/year; $80,000 and above; do not know or missing income), whether a proxy completed the survey, and mode of administration (mail vs. telephone).
We also evaluated whether there were interactions between the four most prevalent cancers (female breast, prostate, colorectal, lung) and the 13 non-cancer chronic conditions in the model. We examined whether stage of disease was related to SF-6D scores for the four most prevalent cancers (female breast, prostate, colorectal, non-small cell lung). For uniformity across conditions, we coded stage of disease into localized cancer, distant (metastatic) cancer, and onstage. Regression parameter standard errors were adjusted for clustering at the health plan level using the sandwich estimator of variance [12].
Recycled predictions [13], or averaging of individual marginal effects, are used to understand the incremental effect of an independent variable on a dependent variable. We used recycled predictions to obtain adjusted SF-6D means for each cancer and non-cancer condition group. We created two variants of these predicted score. In the first approach, we fixed all other independent variables other than the condition being predicted at their means. In the second approach, we fixed the 22 other conditions at zero and the remaining independent variables at their means. The advantage of fixing the other conditions at the mean (first approach) is that the adjusted scores correspond to the overall sample mean on the dependent variable. However, this approach can yield counterintuitive results. In our data, for example, the unstandardized beta for sciatica (−0.037) is more negative than for GI (−0.031) yet the recycled prediction based on the means for the other conditions is slightly larger for sciatica (0.701) than GI (0.700). This occurs because sciatica is more prevalent than GI–the mean for sciatica (0.21) is larger than that for GI (0.05). Hence, when we predict the GI score, the larger sciatica mean drives the estimated GI score down more than the GI mean drives down the estimated sciatica score. The second approach (fixing the other conditions at zero) avoids these sorts of differences between the betas and the recycled predictions but the predicted scores are higher and do not correspond to the sample mean on the dependent variable.
Results
As shown in Table 1, the sample of 126,366 respondents had an average age of 74 years (range 65–106). Forty-five percent were male, 79 % non-Hispanic white, 60 % married, and 27 % had less than a high school degree. The median income was less than $30,000. The average number of reported chronic medical conditions other than cancer was 2.44 (range = 0–13). Sample characteristics for those with and without cancer were similar, but those with cancer were more likely to be male, white, and married.
The average SF-6D score in the entire sample was 0.73 (SD = 0.14), ranging from 0.30 to 1.00. Only 0.16 and 1 % of the sample had the lowest and highest observed scores, respectively. SF-6D scores were consistent across the 4 MHOS cohorts, with the same mean and SD observed for each cohort as for the entire sample.
The regression model with 43 degrees of freedom in the numerator accounted for 39 % of the (adjusted) variance in the SF-6D (see Table 2). All except two conditions (melanoma, endometrial cancer) had significant unique negative associations with the SF-6D score. As a sensitivity analysis to address the concern that depressive symptoms overlap with the dependent variable, we reran the regression model without it and found little impact on the coefficients for the other conditions.
Adjusted mean scores (recycled predictions) using the first approach (fixing other conditions to their mean values) rounded to two decimal places were 0.73 (melanoma), 0.72 (endometrial cancer, colorectal cancer, female breast cancer, prostate cancer, bladder cancer, non-Hodgkin lymphoma, kidney cancer, myocardial infarction/heart attack, hypertension, angina/coronary artery disease, other heart disease), 0.71 (other cancer, non-small cell lung cancer, diabetes, arthritis of the hand), 0.70 (congestive heart failure, arthritis of the hip, inflammatory bowel disease, sciatica, chronic obstructive pulmonary disease), 0.69 (stroke), and 0.61 (depressive symptoms). Adjusted mean scores using the second approach are given in the last column of Table 2.
Only 6 of the 52 two-way interactions between the four most prevalent cancers and the 13 non-cancer conditions were statistically significant (p < 0.05). Small negative coefficients were found for the interactions between colorectal cancer and diabetes, and lung cancer and chronic obstructive pulmonary disease/asthma, while small positive coefficients were found between sciatica and lung cancer, hypertension and prostate cancer, hypertension and colorectal cancer, and other heart disease and female breast cancer. We do not interpret these interactions given the inconsistent directions and because they could have occurred by chance.
There were small numbers of distant stage cancer (26 female breast, 61 prostate, 48 colorectal, and 47 lung) but distant stage of disease was significantly associated with worse health utility scores, with distant stage of disease being worse than localized disease by 0.044 for prostate cancer, 0.046 for colorectal cancer, 0.058 for lung cancer, and 0.077 for female breast cancer.
Discussion
The average SF-6D score in this sample (0.73) is similar to the mean of 0.77 reported for participants 70–79 years of age in the National Health Measurement Study during 2005–2006 [14]. The lower mean in this sample is understandable given that the majority of respondents (88 %) completed the survey by mail, whereas telephone mode of data collection was used for the National Health Measurement Study. Telephone administration tends to yield more positive HRQOL scores [15]. The average SF-36 v. 1 physical component and mental component summary scores (T-score metric with 50 mean and SD of 10 in US general population) were 42 and 52, respectively. Hence, this sample of older individuals had substantially worse physical health (large effect size) but slightly better mental health (small effect size) than the US adult general population. The means for the MHOS sample are very similar to those observed for persons ages 65–74 in the US general population where the PCS and MCS were 43 and 53, respectively [16].
The strongest association with the SF-6D preference-based score was observed for depressive symptoms (−0.131). This is not surprising because the depression question was the only one that had a 1-year reference period. Other health conditions captured in the MHOS could have occurred recently or several years ago because people were asked whether they had ever been told by a doctor that they had the condition. Further, a strong negative association of depression with the SF-6D was expected because the measure includes mental health items. Thus, depressive symptoms are represented to some extent on both sides of the equation. Dropping depressive symptoms from the model had no impact on the interpretation of the associations for the other 20 comorbid conditions that had significant unique associations with the SF-6D score.
The largest decrements in HRQOL for the remaining conditions were observed for arthritis of the hip, sciatica, chronic obstructive pulmonary disease/asthma, stroke, inflammatory bowel disease, and congestive heart failure (betas ranging from −0.029 to −0.044). In contrast, the smallest significant associations were −0.006.
The four conditions with the strongest significant unique associations with the SF-6D in this study (arthritis of the hip, sciatica, chronic obstructive pulmonary disease/asthma, stroke) were found to have relatively large associations with the SF-36 physical component summary score by Smith et al. [3]. Three of the conditions also had strong associations with the SF-36 mental health summary score, while arthritis of the hip was not as strongly related [3].
The majority of cancer types were significantly associated with the SF-6D score, with beta coefficients (rounded to two decimal places) ranging from −0.01 to −0.02 on the 0–1 health utility scale. These results are similar to what was observed in a sample of 38,678 individuals from the 2000–2002 in the medical expenditure panel survey by Sullivan et al. [17]. Specifically, Sullivan et al. [17] reported “disabilities” of −0.02 for prostate cancer, −0.01 for breast cancer, and −0.01 for other cancer.
Walters and Brazier [18] reviewed 7 studies and found that estimates of the minimally important difference (MID) for the SF-6D ranged from 0.01 to 0.05 with a weighted mean of 0.03. Similarly, Khanna et al. [19] reported MID estimates of about 0.03 in a sample of persons with systemic sclerosis. Hence, the magnitudes of the unique associations of types of cancer with health utility score are not trivial. In comparison, the largest unique association of chronic conditions (other than depressive symptoms) with the SF-6D in the current study was −0.04.
While the individual impact of conditions including cancer was typically not large, the differences could matter in group comparisons. For example, a difference of 0.02 on the utility scale would be considered cost-effective if it cost about $1,000 to produce (i.e., $50,000/QALY). Moreover, the cumulative effect of multiple conditions is substantial as evidenced by the plethora of significant unique associations in the regression model. In fact, the adjusted score for those reporting any one condition was on average 0.03 lower than those reporting no conditions, while the adjusted score for those reporting two or more conditions was on average 0.11 lower (results not reported earlier). Finally, the decrements in HRQOL cumulate over time, so the full impact relative to those without chronic conditions is the observed decrement multiplied by the number of years with the condition.
We found that stage of disease had a profound impact on HRQOL. Those with distant (metastatic) stage of disease had health utility scores that were 0.044–0.077 worse than those with localized cancer. Because the number of people with distant stage of disease was so small in the dataset, the overall relationship of cancer with health utility scores was determined entirely by those with less advanced disease when stage was excluded from the model. The large negative decrement in HRQOL in late stage of disease highlights the importance of clinical interventions to ameliorate these negative effects on functioning and well-being.
Although this study has a number of strengths, it also has limitations. Due to the cross-sectional design, we are unable to make definite conclusions about directionality. In addition, other than stage of cancer the study does not have information about the severity of the chronic conditions examined, nor the time when the condition was diagnosed. A previous study found similar SF-36 scores by time since diagnosis but there was some indication of a healthy survivor effect in colorectal and lung cancer patients [3]. We also have not captured information about some common conditions among older individuals such as osteoporosis, benign prostatic hypertrophy, or dementia. Aside from cancer, we had to rely on self-reports of chronic conditions. However, data comparing comorbidities self-reported on the same survey we used (MHOS) versus abstraction of medical records suggest reasonably good correspondence, with median specificity (% of time condition is not self-reported when it is not in the medical record) and sensitivity (% of time condition is self-reported when it is in the medical record) of 69 and 91 %, respectively [20]. In addition, the data were collected using both mail surveys and telephone interviews and included some proxy responses. But we adjusted for these variables in the regression model. Moreover, the SEER-MHOS dataset includes four MHOS cohorts and data collected back in 1998. However, average SF-6D scores for the four cohorts were exactly the same, indicating no temporal shifts. While some preference-based measures (e.g., the EQ-5D) have been criticized for lack of sensitivity [21], the results of this study suggest that the SF-6D is sensitive to the impact of cancer on HRQOL. However, previous research indicates that different preference measures may not yield the same results [22]. The current work needs to be replicated in other large-scale surveys of cancer patients using different preference-based measures.
This study provides important information about the relative burden of different chronic conditions on HRQOL in Medicare beneficiaries. It indicates that a large number of conditions are associated uniquely with decrements in health utility and that the cumulative effects are substantial. In addition, distant stage of disease for the four big cancers (female breast, prostate, colorectal, lung) is associated with large, negative impact on utility among older individuals in the United States. The findings reported here are particularly important given the aging US population and increasing number of persons 65 years and older. As SEER-MHOS adds new cohorts and larger sample sizes by stage of disease become available, further investigation of the impact of cancer and stage of disease will be possible. Tracking the association of chronic conditions and stage of disease on HRQOL periodically can give providers and federal agencies such as the Center for Medicare and Medicaid Services important information about the extent to which the health needs of older Americans are being addressed.
References
Rothrock, N. E., Hays, R. D., Spritzer, K., et al. (2010). Relative to the general US population chronic diseases are associated with poorer health-related quality of life as measured by the patient-reported outcomes measurement information system (PROMIS). Journal of Clinical Epidemiology, 63, 1195–1204.
Altekruse SF, Kosary CL, Krapcho M, et al (eds) SEER Cancer Statistics Review 1975–2007 National Cancer Institute: Bethesda MD. Available from URL: http://seer.cancer.gov/csr/1975_2007 Accessed 27 Aug 2012.
Smith, A. W., Reeve, B. B., Bellizzi, K. M., et al. (2008). Cancer comorbidities and health-related quality of life of older adults. Health Care Financing Review, 29, 41–56.
Brazier, J., Roberts, J., & Deverill, M. (2002). The estimation of a preference-based measure of health from the SF-36. Journal of health economics, 21, 271–292.
Brazier, J., & Roberts, J. (2004). The estimation of a preference-based measure of health from the SF-12. Medical Care, 42, 851–859.
Ambs, A., Warren, J. L., Bellizzi, K. M., et al. (2008). Overview of the SEER-medical health outcomes survey (MHOS) linked dataset. Health Care Financing Review, 29, 5–22.
Ries LAG, Melbert D, Krapcho M, et al (eds.) SEER Cancer Statistics Review 1975–2004 Available from URL: http://seer.cancer.gov/csr/1975_2004/ Based on November 2006 SEER data submission. Accessed 27 Aug 2012.
Clauser, S. B., Arora, N. K., Bellizzi, K. M., et al. (2008). Disparities in HRQOL of cancer survivors and non-cancer managed care enrollees. Health Care Financing Review, 29, 23–40.
Ware, J. E., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36): Conceptual framework and item selection. Medical Care, 30, 473–483.
Brazier, J., Rowen, D., & Hanmer, J. (2008). Revised SF-6D scoring programmes: a summary of improvements. Patient Reported Outcomes Newsletter, 48, 16–17. Fall.
Lumley, T., Diehr, P., Emerson, S., & Chen, L. (2002). The importance of the normality assumption in large public health data sets. Annual Review Publish Health, 23, 151–169.
Williams, R. L. (2000). A note on robust variance estimation for cluster-correlated data. Biometrics, 56, 645–646.
Basu, A., & Rathouz, P. J. (2005). Estimating marginal and incremental effects on health outcomes using flexible link and variance function models. Biostatistics, 6, 93–109.
Hanmer, J. (2009). Predicting an SF-6D preference-based score using MCS and PCS scores from the SF-12 or SF-36. Value Health, 12, 958–966.
Hays, R. D., Kim, S., Spritzer, K. L., et al. (2009). Effects of mode and order of administration on generic health-related quality of life scores. Value Health, 12, 1035–1039.
Ware JE, Kosinski M, Keller SD. (1994). SF-36 physical and mental health summary scales: A user’s manual boston massachusetts: New England medical center.
Sullivan, P. W., Lawrence, W. F., & Ghushchyan, V. (2005). A national study of preference-based scores for chronic conditions in the United States. Medical Care, 43, 736–749.
Walters, S. J., & Brazier, J. E. (2003). What is the relationship between the minimally important difference and health state utility values? The case of the SF-6D. Health Quality Life Outcomes, 11, 1–4.
Khanna, D., Furst, D. E., Wong, W. K., et al. (2007). Reliability validity and minimally important differences of the SF-6D in systemic sclerosis. Quality of Life Research, 16, 1083–1092.
Miller, D. R., Rogers, W. H., Kazis, L. E., et al. (2008). Patients’ self-report of diseases in the medicare health outcomes Survey based on comparisons of linked survey and medical data from the veterans administration. The Journal of ambulatory care management, 31, 161–177.
Garau, M., Shah, K., Mason, A. R., et al. (2011). Using QALYs in cancer: A review of the methodological limitations. Pharmacoeconomics, 29, 673–685.
Feeny, D., Spritzer, K., Hays, R. D., et al. (2011). Agreement about identifying patients who change over time: Cautionary results in cataract and heart failure patients. Medical Decision Making, 32, 273–286.
Acknowledgements
This project was supported by NCI internal funds. Dr. Hays was also supported in part by grants from NIA (P30AG021684) and the NIMHD (2P20MD000182). The SEER-MHOS linked data set is now in the public domain. More information about the data set is available at http://outcomes.cancer.gov/surveys/seer-mhos/. For questions, technical support is available at SEER-MHOS@azqio.sdps.org.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hays, R.D., Reeve, B.B., Smith, A.W. et al. Associations of cancer and other chronic medical conditions with SF-6D preference-based scores in Medicare beneficiaries. Qual Life Res 23, 385–391 (2014). https://doi.org/10.1007/s11136-013-0503-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-013-0503-9