
Abstract
Purpose
The aim of the study is to examine the associations of sleep characteristics with health-related quality of life (HRQOL) and sleep health disparities among US young adults using national survey data.
Methods
The study sample consisted of 2,391 young adults aged 20–39 years from the National Health and Nutrition Examination Survey 2005–2008. HRQOL was assessed using the Centers for Disease Control and Prevention’s HRQOL-4 scale. Multivariable logistic regression models were applied to evaluate the sleep–HRQOL associations. Stratified analyses were conducted to examine whether the associations varied by sociodemographic characteristics.
Results
Approximately 35.6 % of young adults slept <7 h, 41.9 % had insomnia, 4.4 % had sleep disorder, and 8.5 % had sleep apnea. More females had insomnia than males (48.6 vs. 35.9 %, P < 0.001). US-born young adults had more sleep disturbances than their foreign-born counterparts. Compared with those sleeping 7–8 h, the adjusted odds ratio of poor general health was 1.60 (95 % confidence interval, 1.08–2.35) for individuals sleeping 6–7 h and 1.88 (1.23–2.86) for those sleeping <6 h. Similar results were found for low mental HRQOL and overall HRQOL. Insomnia, long sleep latency, troubling falling asleep, daytime sleepiness, and frequent sleeping pill use were significantly associated with low mental HRQOL and overall HRQOL. The associations between sleep disturbances and low HRQOL varied little by sex, race/ethnicity, and country of birth.
Conclusions
Sleep disturbances are common among US young adults and are significantly associated with low HRQOL. Objective measures of sleep are warranted to confirm our findings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The effects of sleep disturbances, such as insomnia and daytime sleepiness, are under-recognized in the United States (US) [1]. Several studies have demonstrated that sleep disturbances are common in college students [2–4]. A cross-sectional study of 125 college students aged 17–24 years from an urban Midwestern university in the United States found that over 60 % of college students were poor-quality sleepers, those with poor sleep reported more physical and psychological health problems than did good-quality sleepers [2]. Increasingly, epidemiologic studies have suggested that sleep is an important risk factor of health outcomes such as obesity [5], diabetes [6], cardiovascular disease [7], and mortality [8]. Sleep quality and quantity have also been reported to be correlated with risk-taking behavior, drowsy driving, and academic and job performance [9–13]. A national telephone survey of 7,428 US adults revealed that insomnia was significantly associated with lost work performance and substantial workplace costs [9].
Health-related quality of life (HRQOL), on the other hand, has been increasingly acknowledged as an important outcome measure in clinical trials and health care [14, 15]. Data from the 2001 to 2002 Behavioral Risk Factor Surveillance System (BRFSS) based on random-digit-dialed telephone survey showed that insufficient sleep was associated with impaired HRQOL in US non-institutional adults [16]. To our knowledge, few studies have focused on sleep characteristics and HRQOL among young adults, especially based on national survey data. Access to a large, nationally representative population database would provide a unique opportunity to explore the associations between sleep characteristics and health outcomes (e.g., HRQOL) in racially/ethnically diverse groups of young adults. Furthermore, several studies have suggested that country of birth may explain some health disparities, including sleep disturbances (e.g., insomnia), in the US [17–20]. For example, Seicean et al. [20] reported that Mexican-born US immigrants had more favorable sleep patterns than the general US population. However, little is known about differences in sleep characteristics between US-born and foreign-born young adults and whether country of birth may modify the associations between sleep and HRQOL.
Using nationally representative data, we first estimated the prevalence of sleep disturbances among US young adults according to selected sociodemographic characteristics. Second, we examined the associations of short sleep duration and other sleep disturbances with HRQOL. Third, we conducted stratified analyses to evaluate whether the sleep–HRQOL association varied by sex, race/ethnicity, and country of birth. We hypothesize that (1) sleep disturbances are common among US young adults, especially among female, minority, and US-born individuals; (2) short sleep duration and/or sleep disturbances are significantly associated with low HRQOL; and (3) the sleep–HRQOL association might vary by some demographic characteristics such as sex, race/ethnicity, and country of birth.
Methods
Study design
The National Health and Nutrition Examination Survey (NHANES) is a nationally representative sample of non-institutionalized US civilian residents [21]. All participants in the NHANES provided written informed consent. The NHANES is conducted by the National Center for Health Statistics (NCHS) of the US Centers for Disease Control and Prevention (CDC) and consists of a standardized in-home interview followed by physical examination and blood and urine collection at a mobile examination center. Sociodemographic and health data were obtained through personal interviews by trained professionals. Although the NHANES data are released in 2-year intervals since 1999, information on sleep was only collected since the NHANES 2005–2006 wave. Individuals aged 16 years and older were selected to answer sleep questions. The NHANES 2005–2006 and 2007–2008 waves were used in this study (n = 19,712). As several NHANES studies have included individuals aged from 20 to 39 years as young adults [22, 23] and some variables of interest were only available for participants aged ≥20 years (e.g., illegal drug use), we only included participants aged 20–39 years as young adults in this study. Individuals were excluded from this study if they were aged <20 (n = 9,775) or ≥40 years (n = 6,258). Among those aged 20–39 years (n = 3,679), 378 pregnant women were excluded due to associated changes in sleep physiology. A total of 2,391 young adults aged 20–39 years with complete data on sleep, HRQOL, sociodemographic characteristics, lifestyle factors, and health conditions were included as our analytic sample in this study (Table 1).
Exposure variables: sleep characteristics
Study participants completed an interviewer-administered questionnaire regarding sleep habits and sleep characteristics, including items from two previously validated instruments such as the Sleep Heart Health Study Sleep Habits Questionnaire [24] and the Functional Outcomes of Sleep Questionnaire [25] through a computer-assisted personal interviewing system. Sleep duration was identified based on the response to the question: “How much sleep do you usually get at night on weekdays or workdays?” Responses were integer values. Inadequate sleep (short sleep duration) was defined as <7 h/weeknight of sleep (yes/no) [20]. We further categorized sleep duration using the following cut points: <6, 6–7, 7–8, and ≥9 h of sleep.
Insomnia was defined using self-report of physician diagnosis and/or complaints of difficulty initiating or maintaining sleep, early morning awakening, or non-restorative sleep [20, 26, 27]. Individuals who reported experiencing any of the following insomnia symptoms “often” (5–15 times/month) or “almost always” (16–30 times/month) over the past month were considered as having insomnia: (1) “Have trouble falling asleep?”, (2) “Wake up during the night and have difficulty getting back to sleep?”, (3) “Wake up too early in the morning and be unable to get back to sleep?”, and (4) “Feeling unrested during the day, no matter how many hours of sleep had.” Long sleep latency was defined as sleep latency ≥30 min [28]. One question was used to define daytime sleepiness: “Feel overly sleepy during the day?”. Participants who answered “often” (5–15 times/month) or “almost always” (16–30 times/month) to the question were considered as having frequent daytime sleepiness.
Regarding the frequency of taking sleeping pill over the past month, participants were asked the question “Do you take sleeping pills or other medication to help you sleep?” obtained from responses on a 5-point Likert scale. Participants who reported “often” (5–15 times/month) or “almost always” (≥16–30 times/month) use of sleeping pill were categorized as frequent sleeping pill users.
Diagnosed sleep disorder was based on the question: “Have you ever been told by a doctor or other health professional that you have a sleep disorder?” Those with the response “yes” were considered as having a diagnosed sleep disorder. Sleep apnea was defined based on an affirmative answer to the following question: “Have you ever been told by a doctor or other health professional that you have a sleep disorder: sleep apnea?” [29]. Regarding habitual snoring, the following question was asked: “In the past 12 months, how often did you snore while you were sleeping?”. Participants who answered “frequently (≥5 nights/week)” were considered as having habitual snoring, whereas those with response “never”, “rarely (1–2 nights/week)”, or “occasionally” (3–4 nights/week) were considered as having no snoring. Restless legs symptoms (RLS) included leg jerks, leg cramps, and restless legs. Participants who reported “often” (5–15 times/month) or “almost always” (16–30 times/month) having leg jerks or legs cramp while sleeping or having sleep disorder, restless legs were considered as having RLS.
Measures of outcome variable: health-related quality of life (HRQOL)
The CDC developed a 4-item set of HRQOL questions (HRQOL-4) to meet the need for a brief and valid measure of HRQOL in the general population [30]. The HRQOL-4 scale was derived from the original version of the Medical Outcomes Study 36-item Short-Form Survey Instrument (SF-36) [15, 31]. Study subjects responded to the following four questions that assessed general health and recent physical health, mental health, and activity limitation: (1) “Would you say that in general your health is: excellent, very good, good, fair, or poor?” (General health); (2) “Now thinking about your physical health, which includes physical illness and injury, for how many days during the past 30 days was your physical health not good?” (Physically unhealthy days: Physical HRQOL); (3) “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?” (Mentally unhealthy days: Mental HRQOL); (4) “During the past 30 days, for about how many days did poor physical or mental health keep you from doing your usual activities, such as self-care, work, or recreation?” (Activity limitation days). The four single HRQOL measures have been validated in both general and clinical populations, have been found to have acceptable criterion validity, and have been used in numerous epidemiologic studies [31–35].
General health was dichotomized into “good” (excellent, very good, and good) and “poor” (fair and poor) health status. The distributions of physically unhealthy days, mentally unhealthy days, and activity limitation days were dichotomized into <14 days (high HRQOL) and ≥14 days (low HRQOL) because this cut point corresponded to approximately the 90th percentile for physically unhealthy days and mentally unhealthy days in previous research [33]. The 14-day cutoff is often used as a marker for clinical depression and anxiety disorders in clinical practice and research [33]. We also created an overall HRQOL index to summarize the 4-item HRQOL measures by using the 0/1 scores (high vs. low HRQOL) for the 4 HRQOL questions and used it as one of our outcome variables.
Measures of covariates
Sociodemographic characteristics
Study participants’ sociodemographic characteristics included sex, age, race/ethnicity, household poverty/income ratio (PIR), marital status, education level, employment status (work at a job or business), and country of birth. Based on the self-reported information, participants were categorized as non-Hispanic Whites, African Americans, Hispanic Americans, and other racial/ethnic group. PIR is an index of income in relation to family need, derived from household income and federally established poverty thresholds based on family size and annual changes in cost of living [36]. PIR represents adjusted household income [37] and is a widely cited variable on the NHANES dataset. In this study, household income status was categorized as: low income (PIR <1, below the official poverty threshold), middle income (PIR: 1–2), and high income (PIR ≥3). Country of birth was categorized as “US-born” or “Foreign-born” group based on the question “In what country were you born?”
Lifestyle factors
Participants were asked questions about their participation in sport(s), exercise, or any other recreational activities: “(1) Over the past 30 days, did you do any vigorous activities for at least 10 min that caused heavy sweating or large increases in breathing or heart rate? Some examples of activities are running, lap swimming, aerobics classes, or fast bicycling. (2) Over the past 30 days, did you do any moderate activities for at least 10 min that cause only light sweating or a slight-to-moderate increase in breathing or heart rate? Some examples of activities are brisk walking, bicycling, swimming, dancing, or golf.” Participants were grouped into two categories: with physical activity participation (individuals participated in moderate and/or vigorous recreational activities) and without physical activity participation (individuals did not participate in any moderate or vigorous recreational activities).
Information on current cigarette smoking and alcohol consumption were also asked and included as covariates in this study (yes vs. no). Regarding the caffeine consumption, participants participated in two 24-h dietary recall periods. The first 24-h dietary recall was done during the initial computer-assisted personal interviews, while the second recall occurred 3–10 days later by telephone. From the two 24-h dietary recalls, we calculated average caffeine consumption (mg/day). Caffeine intake from the dietary data included fluid sources (coffee, tea, and soda) and food sources (chocolate) [38]. Illegal drug use was determined by asking participants whether they used marijuana, hashish, cocaine, heroin, or methamphetamine (yes vs. no).
Health conditions
Measured weight and height were used to calculate body mass index (BMI) and to define weight status: normal weight (BMI <25 kg/m2), overweight (BMI 25–29.9 kg/m2), and obesity (BMI ≥30 kg/m2) [39]. Participants who self-reported at least one of the following 15 chronic health conditions were considered as having chronic disease(s): asthma, anemia, arthritis, diabetes, hypertension, chronic heart failure, coronary heart disease, angina pectoris, myocardial infarction, stroke, emphysema, bronchitis, liver disease, thyroid disease, and cancer [29].
Depression was determined by using the Patient Health Questionnaire-9 (PHQ-9). Participants reported how often they were bothered by depressive symptoms over the preceding 2 weeks, with scores on each question ranging from 0 (not at all) to 3 (nearly every day) for a total score ranging from 0 to 27. A total PHQ-9 score ≥10 was considered to be indicative of depressive symptoms (yes vs. no) [40].
Statistical analysis
Primary exposure variables in this study were sleep characteristics; primary outcome variables were general health, physical HRQOL, mental HRQOL, and overall HRQOL index. χ2 tests were used to examine the differences in the percentages of sleep disturbances across sociodemographic characteristics including sex, race/ethnicity, and country of birth. Multivariable logistic regression models were fit to examine the risk factors for sleep disturbances, including sociodemographic and lifestyle factors, as well as health conditions. Multivariable logistic regression models were also fit to evaluate the associations between sleep disturbances and HRQOL with adjustment for potential confounders including sociodemographic and lifestyle factors and health conditions. Adjusted odds ratios (ORs) and 95 % confidence intervals (95 % CIs) were calculated. We also conducted stratified analyses to determine whether associations between sleep disturbances and HRQOL measures (using general health and overall HRQOL index) varied by sex, race/ethnicity, and country of birth. Interaction terms were included and tested for statistical significance in separate models. All analyses were conducted using survey-related commands in SAS (version 9.3; SAS Institute, Inc., Cary, NC, USA) to account for the complex sampling design. Statistical significance was set at two-tailed P values <0.05.
Results
Characteristics of study participants
As shown in Table 2, about half of participants were aged 20–29 years, 47 % were females, 17 % were foreign-born, 81 % had a job or business, 60 % were married or living with a partner, 30 % were current smokers, 64 % had ever used illegal drug, 65 % had alcohol consumption, 31 % were overweight (BMI 25–29 kg/m2), and 28 % were obese (BMI ≥30 kg/m2. Overall, 28 % of young adults had one or more chronic disease(s), and 6 % had clinical depressive symptoms.
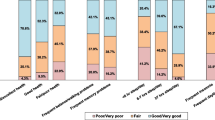
Regarding the HRQOL, 11 % of participants reported having poor general health, 5.4 % had ≥14 physically unhealthy days (low physical HRQOL), 10.9 % had ≥14 mentally unhealthy days (low mental HRQOL) during the past 30 days, and 21.9 % reported a low overall HRQOL (data not shown in tables).
Percentages of sleep disturbances
Approximately 36 % of US young adults had inadequate sleep (sleep <7 h/night), 42 % had insomnia, 16 % had trouble falling asleep, 37 % had sleep latency 30 min or more, 19 % had daytime sleepiness, 4 % took sleeping pills frequently, 4 % had diagnosed sleep disorder, and 9 % had sleep apnea (Table 3). Compared with males, females had a higher percentage of insomnia (48.6 vs. 35.9 %, P < 0.001), trouble falling asleep (19.8 vs. 12.8 %, P = 0.002), and daytime sleepiness (23.1 vs. 15.8 %, P < 0.001). The percentage of young adults with inadequate sleep was the highest for African Americans (51 %), followed by young adults in other racial/ethnic group (37 %), Whites (33.2 %), and Hispanic Americans (30.4 %). US-born young adults had shorter sleep duration and more sleep disturbances than their foreign-born counterparts. The percentages of insomnia and trouble falling asleep were higher in US-born young adults than in foreign-born young adults (45.0 vs. 26.8 %, P < 0.001; 18.5 vs. 4.5 %, P < 0.001, respectively).
Risk factors for sleep disturbances
Multivariable logistic regression models showed that females were 22 % less likely to have inadequate sleep than males (OR 0.78; 95 % CI 0.61, 0.99) and 59 % less likely to have sleep apnea (OR 0.41; 95 % CI 0.27, 0.62), but were 64 % more likely to have insomnia (OR 1.64; 95 % CI 1.31, 2.04) and 49 % more likely to have daytime sleepiness (OR 1.49; 95 % CI 1.13, 1.96) (data not shown in tables). Individuals aged 30–39 years were 31 % more likely to have snoring than those aged 20–29 years. Education level was significantly and inversely related to sleep duration. Young adults with higher education level were more likely to report insomnia, daytime sleepiness, and sleep disorder. Those with higher PIR were less likely to have inadequate sleep, use sleeping pill, and have sleep disorder. Both African Americans and other racial/ethnic group were more likely to have inadequate sleep. Foreign-born young adults were less likely to have inadequate sleep, sleep disorder, and trouble falling asleep. Those with a job or business were 41 % less likely to have trouble falling asleep (OR 0.59; 95 % CI 0.42, 0.81). Young adults who were married or living with a partner were less likely to have long sleep latency, but were more likely to report sleep apnea (OR 1.58; 95 % CI 0.99, 2.53).
Physical activity participation was inversely associated with sleep latency (data not shown in tables). Smoking and alcohol drinking were significantly related to high risks of inadequate sleep, insomnia, and snoring. Illegal drug use was significantly associated with insomnia, long sleep latency, daytime sleepiness, while caffeine consumption was related to RLS. Chronic disease and depression were strongly and significantly related to inadequate sleep, long sleep latency, daytime sleepiness, sleeping pill use, insomnia, and RLS. Obesity was significantly associated with sleep disorder, sleep apnea, and snoring.
Associations between sleep characteristics and HRQOL
After adjustment for potential confounders, sleep disturbances were significantly associated with low HRQOL (Table 4). Young adults who slept <7 h were more likely to report poor general health (OR 1.66; 95 % CI 1.19, 2.30), low physical HRQOL (OR 1.58; 95 % CI 1.01, 2.46), low mental HRQOL (OR 1.39; 95 % CI 0.96, 2.00), and low overall HRQOL (OR 1.54; 95 % CI 1.21, 1.96) than those sleeping ≥7 h. Compared with young adults who reported having 7–8 h of sleep, the adjusted OR of poor general health was 1.60 (95 % CI 1.08, 2.35) for those sleeping 6–7 h and 1.88 (95 % CI 1.23, 2.86) for individuals sleeping <6 h. Similar results were found for sleep duration with overall HRQOL. Insomnia and daytime sleepiness were significantly associated with poor general health, low mental HRQOL, and low overall HRQOL. Those with sleep latency ≥30 min, trouble falling asleep, and sleeping pill use were more likely to have low mental HRQOL and low overall HRQOL. We found that sleep disorder, sleep apnea, snoring, and RLS were not significantly associated with HRQOL.
Stratified analyses for the sleep–HRQOL association
As shown in Table 5, the significant association between inadequate sleep and HRQOL (poor general health domain) varied little by sex, race/ethnicity, and country of birth (all P interaction > 0.05). Although a significant association between daytime sleepiness and poor general health was observed in men but not in women, the interaction term was not significant (P interaction = 0.113). We found associations between insomnia and poor general health across racial/ethnic groups (P interaction = 0.505). A significant association between long sleep latency and poor general health was found among foreign-born but not US-born young adults; however, the interaction term was not significant (P interaction = 0.355). The significant associations for insomnia and daytime sleepiness with poor general health varied little by country of birth (both P interaction > 0.05). We found similar results for the overall HRQOL index stratified by sex, race/ethnicity, and country of birth (data not shown in tables).
Discussion
The transition from adolescence to young adulthood marks the beginning of biological, cognitive, and physiological changes in addition to increases in academic demands and psychosocial stress [42]. Hormonal changes, alterations in neuromuscular tone, and changes in lifestyle factors such as energy drinks, alcohol consumption, and cigarette smoking may contribute to the development of sleep disturbances among young adults [43, 44]. Using nationally representative data, we found that sleep disturbances were common in US young adults. Approximately 42 % had insomnia, 19 % had daytime sleepiness, and 4 % took sleeping pills frequently. African Americans had the highest percentage of short sleep, while Whites had more insomnia than other racial/ethnic groups. US-born young adults had more sleep disturbances than their foreign-born counterparts. Short study duration and other sleep disturbances were significantly associated with low HRQOL, independent of sociodemographic and lifestyle factors and health conditions.
Sleep disturbances and related risk factors
Several studies have found that sleep problems are common among college students [2–4, 45]. A small cross-sectional study reported that more than 60 % of US college students had poor sleep [2]. Sing et al. [45] reported that 69 % of college students in Hong Kong had insomnia, and stress and depression significantly predicted insomnia. Another cross-sectional study reported that 27 % of nursing students in Italy had insomnia [4]. Unsatisfactory academic progress and its related psychosocial stress in college students may increase the risk of sleep disturbances [4, 45]. On the other hand, insufficient sleep and sleep disturbances also cause poor academic and job performance [9–13].
The National Sleep Foundation recommends that healthy adults sleep 7–9 h/day [27]. The 2001–2002 BRFSS study found that over one-fourth of US adults (26 %) reported frequent sleep insufficiency [16]. The National Health Interview Survey 2004–2007 showed that 30 % of civilian employed US adults reported an average sleep duration of ≤6 h/day [41]. Our study showed that 36 % of young adults slept <7 h and 14 % slept <6 h. The percentage of young adults with short sleep was higher in our study than the one among college students (21 % slept <7 h; 6 % slept <6 h) from 24 countries reported by Steptoe et al. [46]. US-born young adults were more likely to have insomnia and other sleep disturbances than their foreign-born counterparts. Consistent with our findings, a recent study reported that Mexican-born US immigrants had longer sleep duration and less insomnia symptoms than the general US population [20]. We also found that obese individuals were more likely to have sleep disorder and sleep apnea than their non-obese counterparts, similar to previous studies [47, 48]. We found that high education level, chronic disease, depression, cigarette smoking, and illegal drug use were significantly associated with insomnia among US young adults. Modifications of these lifestyle behaviors may be vital to the effective control of sleep disturbances among young adults.
The Coronary Artery Risk Development in Young Adults (CARDIA) study (Chicago) of 669 US adults aged 38–50 years showed significant race–sex differences in average sleep duration: 6.7 h for White women, 6.1 h for White men, 5.9 h for African American women, and 5.1 h for African American men [20]. The 2010 Sleep in America poll released by the National Sleep Foundation (NSF) revealed significant differences in the sleep habits across racial/ethnic groups [27]. While African Americans reported the least amount of sleep [27], Whites reported the highest rate of diagnosis for insomnia, similar to our current findings. We also found that African Americans had longer sleep latency than other racial/ethnic groups, which was consistent with the NSF report. African Americans spend more time in bed without sleeping but watching TV or other activities than other racial/ethnic groups [27]. In our study, women were more likely to have insomnia and daytime sleepiness than men, although women reported longer sleep duration than men. We also found that depression was highly linked to insomnia. These findings were consistent with previous reports [27, 49]. Hormonal changes related to the menstrual cycle [50], nighttime awakenings to take care of children and/or other family members, and tasks and responsibilities more commonly performed by women may increase their vulnerability to disturbed sleep and contribute to gender difference in sleep disturbances [50, 51]. Our findings based on nationally representative data provide additional evidence that sleep disturbances are common and are related to many risk factors in US young adults.
Sleep disturbances in relation to impaired HRQOL
Previous research has reported mixed results regarding the associations of sleep disturbances with HRQOL [46, 52, 53]. A cross-sectional study of middle-aged residents of San Diego in the US found no relationship between sleep duration and HRQOL [53]. Another cross-sectional study of UK adults from the Whitehall II Study and US adults from the Western New York Health Study reported significant, consistent associations between short sleep duration and physical and mental domains of HRQOL, while there was no significant association between long sleep duration and mental domain of HRQOL [52]. The 2001–2002 BRFSS study found that adults with frequent sleep insufficiency were significantly more likely than those without frequent sleep insufficiency to report poor general health, frequent physical and mental distress, activity limitations, as well as impaired HRQOL [16]. Steptoe et al. [46] reported that short sleep duration was related to poor self-rated health in both men and women from 27 universities, while longer sleep duration was not related to general health. Similar to prior research [16, 46, 52], our study showed that young adults with short sleep (<6 h) were more likely to have poor general health and low HRQOL (e.g., mental domain and overall HRQOL). This association was independent of potential confounders. Consistent with previous findings [46, 52], we found no significant association between long sleep duration and poor general health or overall HRQOL. Although sleep research of middle-aged and older participants has documented adverse health effects from both short and long sleep [6, 54], sleep duration may be related to different health outcomes across age groups [46]. Younger adults typically sleep longer than middle-aged and older adults, which may reflect primary physiological processes [55].
Several studies have consistently shown that insomnia is independently associated with impaired HRQOL in clinic patients [56, 57] and the general population [14, 58]. Katz and McHorney [56] reported that the prevalence of insomnia was 50 % among patients aged ≥40 years with chronic medical or psychiatric conditions, and insomnia was independently associated with impaired HRQOL across several domains, especially mental health and general health perceptions. Similar to prior reports, we found that insomnia among US young adults was independently associated with poor general health, low mental HRQOL, and low overall HRQOL. Mental aspects of HRQOL might be strongly affected by sleep characteristics compared with physical aspects of HRQOL. Sleep deprivation and insomnia are highly associated with daytime sleepiness and fatigue, which may lead to impairments in functioning optimally and mental HRQOL eventually.
To our knowledge, no published report has examined whether the associations between sleep disturbances and HRQOL are modified by sociodemographic characteristics. In this study, we found that the associations between sleep and HRQOL varied little by sex, race/ethnicity, or country of birth, contrary to our hypothesis. This might be due to self-reported sleep information used in our study. African Americans and Hispanic Americans might have underestimated their sleep disturbances. One recent study, for example, revealed that African Americans and Hispanic Americans were relatively optimistic in their ratings than Whites [59]. Future studies that deploy objective measures of sleep may overcome limitations associated with reliance on self-reported sleep measures.
Our study and previous research provide strong evidence that sleep disturbances are highly related to low HRQOL. The possible mechanism underlying this link might be that inadequate sleep and sleep disturbances can affect immune system and the ability to function optimally, impair performance of school, work, and social activities on a daily basis, and can have a major impact on physical, mental, emotional well-being, and overall HRQOL [16, 60].
Study strengths and limitations
Our study has several strengths. First, it is based on nationally representative data. This allows greater generalizability than previous small studies. Second, we performed a robust set of data analyses to examine the associations between sleep disturbances and HRQOL by controlling for potential confounders. Third, the brief measure of HRQOL used in our study has been validated and used to examine HRQOL in the general populations [33, 35].
A major limitation of this study is its cross-sectional study design, thus the inability to delineate causality, in other words, we are unable to detect whether sleep disturbances lead to low HRQOL or vice versa. Future longitudinal studies with serial assessments of sleep and HRQOL change are warranted to thoroughly elucidate bidirectional associations between sleep disturbances and HRQOL among young adults. Another limitation is that sleep disturbances were assessed by self-reported questionnaire. Objective measures of sleep are warranted to confirm our findings. Furthermore, our study only included US young adults aged 20–39 years. Thus, the results might not be generalized to other populations or other age groups. The findings were only based on participants with complete data. However, we found no significant differences in the sleep, HRQOL, and sociodemographic characteristics between participants included in this study and those excluded from this study. In addition, similar to other studies, HRQOL is based on a brief 4-item questionnaire that is subject to measurement error and report bias, although the questions have been validated.
Despite these limitations, our study has important clinical and public health implication, given that short sleep duration and sleep disturbances are common among US young adults and are significantly associated with low HRQOL. Young adults will play a key role when they become professional. Our study emphasizes the needs for recognition and appropriate management of sleep disturbances among young adults. Considering the various adverse health consequences of sleep disturbances, efforts to expedite screening and treatment are indicated to help improve HRQOL among young adults. Our findings also underscore the need to educate young adults on the importance of adequate sleep and potential influences of sleep disturbances on HRQOL.
In conclusion, our study based on nationally representative data showed that sleep disturbances such as inadequate sleep and insomnia were common among US young adults. Sleep disturbances were significantly associated with low HRQOL. These associations varied little by sex, race/ethnicity, and country of birth. Our study demonstrates the need to assess sleep disturbances and identify those most at risk of adverse health consequences. Short sleep and insomnia may be more of a concern for young adults in the United States. Our findings suggest that identification and appropriate screening of sleep disturbances among young adults may increase their sleep quality and HRQOL. Further prospective studies, with objective measures of sleep duration and sleep quality, are needed to examine the bidirectionality and causal relation of sleep disturbances with diminished HRQOL. Given the significant associations between sleep disturbances and HRQOL observed in our study, appropriate intervention programs may be important to be developed in order to improve sleep quality and HRQOL among young adults.
Abbreviations
- BMI:
-
Body mass index
- BRFSS:
-
Behavioral Risk Factor Surveillance System
- CDC:
-
Centers for Disease Control and Prevention
- CI:
-
Confidence interval
- HRQOL:
-
Health-related quality of life
- NCHS:
-
National Center for Health Statistics
- NHANES:
-
National Health and Nutrition Examination Survey
- NSF:
-
National Sleep Foundation
- OR:
-
Odds ratio
- PIR:
-
Poverty/income ratio
- RLS:
-
Restless legs syndrome
References
US Department of Health and Human Services, National Institutes of Health. National Heart, Lung, and Blood Institute, National Center on Sleep Disorders Research. (2003). National sleep disorders research plan. Available at: http://www.nhlbi.nih.gov.ezp-prod1.hul.harvard.edu/health/prof/sleep/res_plan/sleep-rplan.pdf. Accessed August 1, 2012.
Lund, H. G., Reider, B. D., Whiting, A. B., & Prichard, J. R. (2010). Sleep patterns and predictors of disturbed sleep in a large population of college students. Journal of Adolescent Health, 46(2), 124–132.
Veldi, M., Aluoja, A., & Vasar, V. (2005). Sleep quality and more common sleep-related problems in medical students. Sleep Medicine, 6(3), 269–275.
Angelone, A. M., Mattei, A., Sbarbati, M., & Di Orio, F. (2011). Prevalence and correlates for self-reported sleep problems among nursing students. Journal of Preventative Medicine & Hygiene, 52(4), 201–208.
Chen, X., Beydoun, M. A., & Wang, Y. (2008). Is sleep duration associated with childhood obesity? A systematic review and meta-analysis. Obesity (Silver Spring), 16(2), 265–274.
Yaggi, H. K., Araujo, A. B., & McKinlay, J. B. (2006). Sleep duration as a risk factor for the development of type 2 diabetes. Diabetes Care, 29(3), 657–661.
Redline, S., & Foody, J. (2011). Sleep disturbances: Time to join the top 10 potentially modifiable cardiovascular risk factors? Circulation, 124(19), 2049–2051.
Kripke, D. F., Garfinkel, L., Wingard, D. L., Klauber, M. R., & Marler, M. R. (2002). Mortality associated with sleep duration and insomnia. Archives of General Psychiatry, 59(2), 131–136.
Kessler, R. C., Berglund, P. A., Coulouvrat, C., Hajak, G., Roth, T., Shahly, V., et al. (2011). Insomnia and the performance of US workers: Results from the America insomnia survey. Sleep, 34(9), 1161–1171.
Gaultney, J. F. (2011). The prevalence of sleep disorders in college students: Impact on academic performance. Journal of American College Health, 59(2), 91–97.
Taylor, D. J., & Bramoweth, A. D. (2010). Patterns and consequences of inadequate sleep in college students: Substance use and motor vehicle accidents. Journal of Adolescent Health, 46(6), 610–612.
Curcio, G., Ferrara, M., & De Gennaro, L. (2006). Sleep loss, learning capacity and academic performance. Sleep Medicine Reviews, 10(5), 323–337.
Williams, A. F., Tefft, B. C., & Grabowski, J. G. (2012). Graduated driver licensing research, 2010–present. Journal of Safety Research, 43(3), 195–203.
Leger, D., Scheuermaier, K., Philip, P., Paillard, M., & Guilleminault, C. (2001). SF-36: Evaluation of quality of life in severe and mild insomniacs compared with good sleepers. Psychosomatic Medicine, 63(1), 49–55.
Ware, J. E., Jr., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care, 30(6), 473–483.
Strine, T. W., & Chapman, D. P. (2005). Associations of frequent sleep insufficiency with health-related quality of life and health behaviors. Sleep Medicine, 6(1), 23–27.
Montez, J. K., & Eschbach, K. (2008). Country of birth and language are uniquely associated with intakes of fat, fiber, and fruits and vegetables among Mexican-American women in the United States. Journal of the American Dietetic Association, 108(3), 473–480.
Eldeirawi, K. M., & Persky, V. W. (2006). Associations of acculturation and country of birth with asthma and wheezing in Mexican American youths. Journal of Asthma, 43(4), 279–286.
Sundquist, J., & Winkleby, M. (2000). Country of birth, acculturation status and abdominal obesity in a national sample of Mexican-American women and men. International Journal of Epidemiology, 29(3), 470–477.
Seicean, S., Neuhauser, D., Strohl, K., & Redline, S. (2011). An exploration of differences in sleep characteristics between Mexico-born US immigrants and other Americans to address the Hispanic paradox. Sleep, 34(8), 1021–1031.
Centers for Disease Control and Prevention, National Center for Health Statistics National Health and Nutrition Examination Survey data. Accessed July 9, 2012.
Flegal, K. M., Carroll, M. D., Kit, B. K., & Ogden, C. L. (2012). Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. Journal of the American Medical Association, 307(5), 491–497.
Saydah, S., Bullard, K. M., Imperatore, G., Geiss, L., & Gregg, E. W. (2013). Cardiometabolic risk factors among US adolescents and young adults and risk of early mortality. Pediatrics, 131(3), e679–e686.
Unruh, M. L., Redline, S., An, M. W., Buysse, D. J., Nieto, F. J., Yeh, J. L., et al. (2008). Subjective and objective sleep quality and aging in the sleep heart health study. Journal of the American Geriatrics Society, 56(7), 1218–1227.
Chasens, E. R., Ratcliffe, S. J., & Weaver, T. E. (2009). Development of the FOSQ-10: A short version of the Functional Outcomes of Sleep Questionnaire. Sleep, 32(7), 915–919.
Roth, T. (2007). Insomnia: Definition, prevalence, etiology, and consequences. Journal of Clinical Sleep Medicine, 3(5 Suppl), S7–S10.
National Sleep Foundation. ‘Sleep in America’ poll. Available at: http://www.sleepfoundation.org. Accessed August 1, 2012.
Plantinga, L., Rao, M. N., & Schillinger, D. (2012). Prevalence of self-reported sleep problems among people with diabetes in the United States, 2005–2008. Preventing Chronic Disease, 9, E76.
Li, C., Ford, E. S., Zhao, G., Croft, J. B., Balluz, L. S., & Mokdad, A. H. (2010). Prevalence of self-reported clinically diagnosed sleep apnea according to obesity status in men and women: National Health and Nutrition Examination Survey, 2005–2006. Preventive Medicine, 51(1), 18–23.
Hennessy, C. H., Moriarty, D. G., Zack, M. M., Scherr, P. A., & Brackbill, R. (1994). Measuring health-related quality of life for public health surveillance. Public Health Reports, 109(5), 665–672.
Moriarty, D. G., Zack, M. M., & Kobau, R. (2003). The Centers for Disease Control and Prevention’s Healthy Days Measures—Population tracking of perceived physical and mental health over time. Health and Quality of Life Outcomes, 1, 37.
Ounpuu, S., Chambers, L. W., Chan, D., & Yusuf, S. (2001). Validity of the US behavioral risk factor surveillance system’s health related quality of life survey tool in a group of older Canadians. Chronic Diseases in Canada, 22(3–4), 93–101.
Ford, E. S., & Li, C. (2008). Metabolic syndrome and health-related quality of life among US adults. Annals of Epidemiology, 18(3), 165–171.
Andresen, E. M., Catlin, T. K., Wyrwich, K. W., & Jackson-Thompson, J. (2003). Retest reliability of surveillance questions on health related quality of life. Journal of Epidemiology and Community Health, 57(5), 339–343.
Ford, E. S., Mannino, D. M., Homa, D. M., Gwynn, C., Redd, S. C., Moriarty, D. G., et al. (2003). Self-reported asthma and health-related quality of life: Findings from the behavioral risk factor surveillance system. Chest, 123(1), 119–127.
Harper, S., & Lynch, J. (2007). Trends in socioeconomic inequalities in adult health behaviors among US states, 1990–2004. Public Health Reports, 122(2), 177–189.
Ali, M. K., Bullard, K. M., Beckles, G. L., Stevens, M. R., Barker, L., Narayan, K. M., et al. (2011). Household income and cardiovascular disease risks in US children and young adults: Analyses from NHANES 1999–2008. Diabetes Care, 34(9), 1998–2004.
Davis, N. J., Vaughan, C. P., Johnson, T. M., II, Goode, P. S., Burgio, K. L., Redden, D. T., et al. (2013). Caffeine Intake and its Association with Urinary Incontinence in United States men: Results from National Health and Nutrition Examination Surveys 2005–2006 and 2007–2008. Journal of Urology, 189(6), 2170–2174.
National Institutes of Health. (1998). Clinical guidelines on the identification, evaluation and treatment of overweight and obesity in adults: The evidence report. Washington, DC: National Institutes of Health.
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613.
Luckhaupt, S. E., Tak, S., & Calvert, G. M. (2010). The prevalence of short sleep duration by industry and occupation in the National Health Interview Survey. Sleep, 33(2), 149–159.
Lohsoonthorn, V., Khidir, H., Casillas, G., Lertmaharit, S., Tadesse, M. G., Pensuksan, W. C., et al. (2012). Sleep quality and sleep patterns in relation to consumption of energy drinks, caffeinated beverages, and other stimulants among Thai college students. Sleep and Breathing (in press).
Singh, V., Pandey, S., Singh, A., Gupta, R., Prasad, R., & Singh Negi, M. P. (2012). Study pattern of snoring and associated risk factors among medical students. Bioscience Trends, 6(2), 57–62.
Pullman, A. W., Masters, R. C., Zalot, L. C., Carde, L. E., Saraiva, M. M., Dam, Y. Y., et al. (2009). Effect of the transition from high school to university on anthropometric and lifestyle variables in males. Applied Physiology, Nutrition and Metabolism, 34(2), 162–171.
Sing, C. Y., & Wong, W. S. (2011). Prevalence of insomnia and its psychosocial correlates among college students in Hong Kong. Journal of American College Health, 59(3), 174–182.
Steptoe, A., Peacey, V., & Wardle, J. (2006). Sleep duration and health in young adults. Archives of Internal Medicine, 166(16), 1689–1692.
Redline, S., Tishler, P. V., Schluchter, M., Aylor, J., Clark, K., & Graham, G. (1999). Risk factors for sleep-disordered breathing in children. Associations with obesity, race, and respiratory problems. American Journal of Respiratory and Critical Care Medicine, 159((5 Pt 1)), 1527–1532.
Peppard, P. E., Young, T., Palta, M., Dempsey, J., & Skatrud, J. (2000). Longitudinal study of moderate weight change and sleep-disordered breathing. Journal of the American Medical Association, 284(23), 3015–3021.
Harris, T. (2003). Depression in women and its sequelae. Journal of Psychosomatic Research, 54(2), 103–112.
Dzaja, A., Arber, S., Hislop, J., Kerkhofs, M., Kopp, C., Pollmacher, T., et al. (2005). Women’s sleep in health and disease. Journal of Psychiatric Research, 39(1), 55–76.
Hislop, J., & Arber, S. (2003). Understanding women’s sleep management: Beyond medicalization–healthicization? Sociology of Health & Illness, 25(7), 815–837.
Stranges, S., Dorn, J. M., Shipley, M. J., Kandala, N. B., Trevisan, M., Miller, M. A., et al. (2008). Correlates of short and long sleep duration: A cross-cultural comparison between the United Kingdom and the United States: The Whitehall II Study and the Western New York Health Study. American Journal of Epidemiology, 168(12), 1353–1364.
Jean-Louis, G., Kripke, D. F., & Ancoli-Israel, S. (2000). Sleep and quality of well-being. Sleep, 23(8), 1115–1121.
Ayas, N. T., White, D. P., Manson, J. E., Stampfer, M. J., Speizer, F. E., Malhotra, A., et al. (2003). A prospective study of sleep duration and coronary heart disease in women. Archives of Internal Medicine, 163(2), 205–209.
Floyd, J. A., Medler, S. M., Ager, J. W., & Janisse, J. J. (2000). Age-related changes in initiation and maintenance of sleep: A meta-analysis. Research in Nursing & Health, 23(2), 106–117.
Katz, D. A., & McHorney, C. A. (2002). The relationship between insomnia and health-related quality of life in patients with chronic illness. Journal of Family Practice, 51(3), 229–235.
Hatoum, H. T., Kong, S. X., Kania, C. M., Wong, J. M., & Mendelson, W. B. (1998). Insomnia, health-related quality of life and healthcare resource consumption. A study of managed-care organisation enrollees. Pharmacoeconomics, 14(6), 629–637.
Paine, S. J., Gander, P. H., Harris, R. B., & Reid, P. (2005). Prevalence and consequences of insomnia in New Zealand: Disparities between Maori and non-Maori. Australian and New Zealand Journal of Public Health, 29(1), 22–28.
Dowd, J. B., & Todd, M. (2011). Does self-reported health bias the measurement of health inequalities in US adults? Evidence using anchoring vignettes from the Health and Retirement Study. Journals of Gerontology Series B, Psychological Sciences and Social Sciences, 66(4), 478–489.
Manocchia, M., Keller, S., & Ware, J. E. (2001). Sleep problems, health-related quality of life, work functioning and health care utilization among the chronically ill. Quality of Life Research, 10(4), 331–345.
Acknowledgments
This study was supported by grants from NIH/NIMHD (T37-MD001449) and NIH/NCRR/NCATS (8UL1TR000170).
Conflict of interest
The authors of this manuscript have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chen, X., Gelaye, B. & Williams, M.A. Sleep characteristics and health-related quality of life among a national sample of American young adults: assessment of possible health disparities. Qual Life Res 23, 613–625 (2014). https://doi.org/10.1007/s11136-013-0475-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-013-0475-9