
Abstract
Purpose
This study aimed to ascertain the psychometric properties of EuroQol Five Dimensional Questionnaire (EQ-5D-3L) in primary caregivers of children with autism. The convergent validity, discriminant validity, known-groups validity, internal consistency reliability, and floor and ceiling effects of EQ-5D-3L were analyzed.
Methods
A cross-sectional design was used for study purposes. Through an online survey, relevant study information was collected from 316 primary caregivers of children with autism. Study participants were from families of children with autism living in the United States who were registered with the Interactive Autism Network. Convergent validity of the EQ-5D-3L was assessed through its correlation with other measures of similar constructs. Discriminant validity was assessed by observing the correlation of EQ-5D-3L domains with theoretically unrelated constructs. Known-groups validity was tested by comparing EQ-5D-3L index and visual analog scale (VAS) scores across levels of autism severity among the care recipients. Internal consistency reliability of EQ-5D-3L was tested. Lastly, floor and ceiling effects of EQ-5D-3L were assessed.
Results
More than 60 % of participants reported problems of ‘anxiety/depression.’ Convergent and discriminant validity of the EQ-5D-3L was good. Significant correlation (convergent validity) was observed among EQ-5D-3L index and VAS and (SF-12v2) physical component summary and mental component summary scores. Caregivers’ EQ-5D-3L index and VAS scores varied by levels of autism severity among care recipients, providing evidence of known-groups validity. Reliability assessed through Cronbach’s alpha was less than satisfactory; however, corrected item-total correlations were adequate.
Conclusions
The EQ-5D-3L is a psychometrically sound tool to elicit health state preferences among caregivers of children with autism.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism is a neurodevelopmental disorder with the hallmark symptoms of social interaction and communication difficulty and restricted and repetitive behaviors [1]. Autism can be further classified into classic autism, Asperger’s syndrome, and pervasive developmental disorder-not otherwise specified (PDD-NOS). A recent study by the Centers for Disease Control and Prevention (CDC) reported the prevalence of autism among children in the USA to be ~1.13 % [2]. In their review of epidemiological surveys for autism across the world, Elsabbagh et al. [3] reported the global mean prevalence for autism to be 62 per 10,000. Though considerable variability in autism prevalence was found across different regions of the world, the authors noted that autism prevalence did not differ significantly between continental America and Europe. Autism prevalence has been reported to be ~1 % in the UK [4]. Some parts of the world have been found to have a higher prevalence of autism than the USA. Using a population-based sample in Korea, Kim et al. [5] found the prevalence of autism among children aged 7–12 years to be 2.64 %. Notwithstanding the differences in case definition and ascertainment, these results generally indicate that autism may be more prevalent than commonly thought. In the 6-years period between 2002 and 2008, autism prevalence increased by 78 % in the USA [2]. Currently, autism is more prevalent than pediatric diabetes, cancer, and AIDS combined [6], thereby making it a significant public health concern. Autism is five times more common among males as compared to females [2]. The true cause of autism remains unknown; however, recent literature suggests the occurrence of the disorder to be a result of genetic predisposition coupled with an environmental trigger [7].
Since autism is a chronic disorder, the responsibility of providing constant care to children with the disorder falls on the caregivers (generally their parents). This takes a tremendous toll on the physical and emotional health of the caregivers. An abundance of literature has highlighted the negative impact of caring for a child with autism on caregivers’ health and well-being [8–12]. One autism caregiving outcome that has received increasing attention over the past few years is health-related quality of life (HRQOL) [13–16]. An individual’s HRQOL encompasses his/her physical, psychological, and social health, and these domains may be influenced by the experiences and perceptions of the individual [17]. The HRQOL of caregivers not only affects their own personal health, but may also impact the quality of care that they provide to the child with autism. In their study of HRQOL among autism caregivers, Khanna et al. [15] found lower physical and mental health scores among caregivers of children with autism as compared to the general US adult population. Other studies have also reported lower HRQOL scores among caregivers of children with autism in comparison with the general adult population or parents of children with typical development [13, 14, 16]. These studies have been consistent in terms of their use of the Medical Outcomes Study (MOS) Short-Form Health Survey (SF-36 or SF-12) instrument for HRQOL measurement. The SF-36 and SF-12 are commonly used generic health profile instruments.
Although these studies provide useful information regarding the general health status among autism caregivers, limited literature currently exists regarding the preference-based scores for health outcomes among caregivers of these patients. Assessing health state preferences offers certain advantages as compared to the information gleaned from generic health profile measures [18]. Instead of assessing disease presence, absence, or symptom severity, preference-based measures determine an individual’s preference for a being in a particular health condition. Preference-based measures combine both positive and negative aspects of health state and present them as a single number that typically ranges from 0 (death) to 1 (perfect health). By providing a common unit, preference-based measures provide researchers the flexibility to make comparisons across different health populations. Preferences may be determined under conditions of certainty (without any underlying risk) or uncertainty (in the presence of risk). When measured using the former approach, the resulting preferences are termed ‘values,’ while those measured through the later are termed ‘utility.’ Preference values can be ascertained through approaches such as rating scales and time trade-off (TTO), whereas utilities are measured through the standard gamble approach. Preference values (or utilities) are used in calculating quality-adjusted life years (QALYs), which are central to economic evaluations such as cost-utility analysis [19]. Given the scarcity of healthcare resources, data on cost per QALY gained enable adequate resource allocation to treatments or interventions that provide the biggest gain. So unlike health status (as measured using SF-36 or SF-12), preference values and utilities can be used by policy makers or researchers in making decisions in the presence of resource limitations or under uncertain conditions [20].
Preference values and utilities have been traditionally used in patient outcomes assessment; however, they are considered to be equally important parameter in caregiving population. In an insightful piece of work examining the estimation of QALYs for caregivers, Al-Janabi et al. [21] make a strong argument as to why it is essential to ascertain QALYs among caregivers, even when the healthcare interventions are targeted toward the patients. The authors contend that economic evaluations that do not consider all QALY (including health) gains, including among those related to patients, may result in inadequate distribution of healthcare resources. In the context of caregiving population, preference data could be applied toward determining the usefulness of supporting interventions or programs. For example, when examining the cost-effectiveness of a Systemic Care Program for Dementia (SCPD) that focuses on dementia caregivers’ sense of competence against usual care, Spijker et al. [22] calculated the quality of caregivers life (QALY) using preference values elicited through EuroQol Five Dimensional Questionnaire (EQ-5D-3L) [23, 24]. Preference scores for caregivers are also needed in valuations of costs associated with informal care [25]. Changes in preference scores for caregivers may be useful in determining the true cost-effectiveness of a drug aimed at alleviating disease severity of the care recipient [26]. Estimation of health state preferences among caregivers serves a useful purpose and must be incorporated as a critical outcome measure in addition to patient healthcare assessment.
An individual’s preference value or utility can be assessed using generic preference-based measures such as the EuroQol Five Dimensional Questionnaire (EQ-5D-3L) [23, 24], Health Utilities Index (HUI-I, II, III) [27], Quality of Well-Being Scale (QWB) [28, 29], and Short Form-Six Dimensions (SF-6D) [30]. These measures have underlying differences with respect to the health dimensions captured, number of questions, and health state valuations [31]. One of the key differences among these instruments is in the valuation technique used to derive preferences for the health states that these instruments capture. The EQ-5D-3L health state valuations is based on TTO, while valuation for HUI and SF-6D is based on standard gamble. As a result, the preference values (or utilities) generated from these measures typically vary. Despite these differences, these measures have a distinct advantage over generic health profile measures in that they not only capture HRQOL information, but also summarize the HRQOL as a single number that typically ranges from a state of perfect health to death.
Given its simplicity and ease of use, the EQ-5D-3L is one of the most commonly used preference-based measures [32]. The EQ-5D-3L includes two components: descriptive system (EQ-5D-3L index) and visual analog scale (EQ-5D-3L VAS) [23, 24]. The EQ-5D-3L index provides information of an individual’s health profile in five domains, with each domain having three response options ranging from ‘no problem’ (1) to ‘extreme problem’ (3). A single summary index score can be derived from the EQ-5D-3L health states. The summary index score for EQ-5D-3L may range from −0.59 (worse than death) to 1.00 (perfect health) [33]. The EQ-5D-3L VAS assesses self-rating of health on a scale of 0–100.
Although the EQ-5D-3L has never been previously used in caregivers of autistic patients, it has been used to study caregiver outcomes in other neurological disorders across different regions of the world [34–39]. Researchers typically use EQ-5D-3L to assess the health impact (HRQOL) of caregiving on caregivers and to study the relationship between HRQOL and other caregiving outcomes (burden, depression, etc.). For example, when studying the HRQOL of caregivers of individuals with Alzheimer’s disease, Serrano-Aguilar et al. [34] found higher frequency of problems in each of the five domains of EQ-5D-3L among caregivers as compared to the general population in Spain. The authors also found an inverse association between caregiver burden and caregivers’ HRQOL. In another similar study, Martinez-Martin et al. [35] found burden and depression scores to be inversely related to EQ-5D-3L index and VAS scores among caregivers of individuals with Parkinson’s disease. Several researchers have also tested the psychometric profile of EQ-5D-3L among patients with neurological and psychiatric disorders such as anxiety disorders, schizophrenia, and Parkinson’s disease [40–47]. König et al. [43] found the EQ-5D-3L to have adequate construct validity and moderate responsiveness among patients with anxiety disorders. Given its low respondent burden and ease of administration, the authors suggested the inclusion of EQ-5D-3L as an assessment measure for overall HRQOL and health state valuations in patients with anxiety disorders. In a sample of patients with schizophrenia, Prieto et al. [40] found the EQ-5D-3L scores to be correlated with measures of patients’ clinical status. The EQ-5D-3L was found to be able to discern HRQOL differences among schizophrenia patients by their degree of severity of illness. These results, along with those of other such studies, reflect that the EQ-5D-3L instrument is a viable option to measure health outcomes across different patient/caregiver populations.
For the EQ-5D-3L to be used in the assessment of preference scores among autism caregivers, it is imperative that the psychometric profile of the instrument be tested in this population. The purpose of this study was to determine the psychometric properties of the EQ-5D-3L instrument among caregivers of children with autism. Specifically, we tested the convergent validity, discriminant validity, known-groups validity, and internal consistency reliability, and assessed floor and ceiling effects of the EQ-5D-3L instrument. Since preference scores in this caregiving population have not been previously determined, studying the psychometric properties of a commonly used preference instrument, that is, EQ-5D-3L, could provide confidence in its use for future research.
Methods
Study sample and procedure
This study was part of a larger project aimed at studying health utilities among caregivers of children with autism. Only the information relevant to study purpose is included in the current study. A cross-sectional online survey of primary caregivers of children with autism was conducted for data collection. Study participants were recruited from families registered with the Interactive Autism Network (IAN) in the USA. The IAN is an online autism community that enables collaboration between researchers and individuals and families affected by autism throughout the USA [48]. It is run by the Kennedy Krieger Institute and funded by Autism Speaks and the Simons Foundation. More than 38,000 participants are registered with the IAN, including over 14,000 individuals with autism. Through IAN portal, autism researchers can gain access to families of individuals with autism who meet study criteria and are willing to participate in research. Among families registered with the IAN, those having (1) a child with autism less than or equal to 18 years of age and (2) no more than one child diagnosed with autism were identified and emailed a cover letter. To protect member identity, the identification of families based on study criteria and cover letter mailing was conducted by the IAN. The cover letter explained the study purpose, emphasized voluntary participation, and included the survey link. Within each family, participation in the study was restricted to the primary caregiver, which was classified as the individual in the family who had the main responsibility for providing daily care to the child with autism. The online survey was administered via Qualtrics online survey software (Qualtrics Inc., Provo, UT). As a token of appreciation, a $15 Amazon gift card was offered to participants who completed the survey. The online survey was closed once the desired number of responses (set at 300) for the larger project was achieved. A total of 326 responses were received during the period May 7–11, 2012. The study received approval from the University of Mississippi (UM) Institutional Review Board (IRB) under exempt status.
The survey included four sections. There were other instruments included in the actual survey besides those described in the study. Since the other measures are not related to present study purpose, they have not been reported here. Section I consisted of instruments used in the assessment of caregiver health status (SF-12v2) [49] and caregiver burden [Caregiver Strain Questionnaire (CGSQ)] [50]. Section II consisted of an assessment of severity of autism in the child [Social Communication Questionnaire (SCQ)] [51]. Section III consisted of items aimed at assessing the relevant sociodemographic information of the caregiver and child with autism. Section IV consisted of the EQ-5D-3L instrument [23, 24]. An online (Web-based) version of the EQ-5D-3L instrument was used in the current study. Participants were re-directed after section III from the Qualtrics online system to the EuroQol Group server system to complete section IV (EQ-5D-3L) of the survey.
Study measures
EuroQol Questionnaire (EQ-5D-3L)
The EQ-5D-3L is a generic HRQOL instrument that includes the EQ-5D-3L index and EQ-5D-3L VAS [23, 24]. The EQ-5D-3L index has five dimensions assessing the domains of mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each item has three possible responses: ‘1, no problems’; ‘2, moderate problems’; and ‘3, extreme problems.’ The response to the five items provides an indication of the degree to which an individual has problems in each domain. An individual’s health status can be described as a five-digit numeral, created by combining the response to the five items. A total of 35 (243) possible health states are captured by the EQ-5D-3L index. Using a set of population-based preference weights, an index score can be generated from the self-reported health states. For the current study, we used the scoring algorithm developed by Shaw et al. [52] to calculate the EQ-5D-3L index score. The preference-weighting system for EQ-5D-3L was generated using a representative sample of 4,048 adults 18 years of age or older in the USA. Through TTO exercises, Shaw et al. [52] established US population-based preference weights for the 243 unique health states of EQ-5D-3L. Index scores could range from −0.11 for health state ‘33333’ (worst health state) to 1.00 for health state ‘11111’ (perfect health state). Luo et al. [53] provided the EQ-5D-3L norms for self-reported health status of the general adult population in the USA.
The EQ-5D-3L VAS includes a vertical graph scale (thermometer shaped) with end points 0 (worst health status) and 100 (best health status). Participants were asked to choose a number from (inclusive) 0 to 100 that best describes their current health state.
Medical Outcomes Study Short-Form Health Survey version 2 (SF-12v2)
The SF-12v2 is a generic health profile instrument that includes 12-items [49]. Similar to its parent survey the SF-36, the SF-12v2 provides summary scores for physical HRQOL (physical component summary [PCS] score) and mental HRQOL (mental component summary [MCS] score). In addition, scores for eight sub-domains—physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health—are also provided. Standard US norm-based scores for the two summary scales and eight subscales were calculated using the QualityMetric SF Health Outcomes™ Scoring Software. Norm-based scores for the SF-12v2 have a mean of 50 and standard deviation of 10 in the general US population. Higher scores indicate better health status [49].
Caregiver Strain Questionnaire (CGSQ)
The 21-item Caregiver Strain Questionnaire (CGSQ) was used to assess the burden experienced by caregivers of children with autism [50]. A 5-point Likert scale is used to measure each item and includes endpoints ‘not at all a problem’ (1) and ‘very much a problem’ (5). Overall burden score can range from 3 to 15, with higher score indicating greater caregiver burden [50]. The CGSQ has been found to have good reliability and validity for the assessment of burden among caregivers of children with autism [54].
Social Communication Questionnaire (SCQ)
The 40-item SCQ (Lifetime version) was used to determine the severity of autism in the child [51]. The parent report SCQ assesses severity in the domains of reciprocal social interaction, communication, and restricted, repetitive, and stereotyped patterns of behavior. Items are measured on a ‘yes/no’ format. A score of 1 is given in the presence of abnormal behavior, while 0 is given in the absence of abnormal behavior. A total score was calculated by summing the scores on individual items [51], with higher score indicating greater severity.
Statistical analysis
Survey data were checked for missing values. Surveys with more than 15 % missing data were removed from analysis. Of the 326 responses received, 10 were removed based on missing data criterion. Thus, a total of 316 responses were analyzed for study purposes. There were no missing values for EQ-5D-3L instrument. The Web-based EQ-5D-3L survey requires users to choose a response option for each element (EQ-5D-3L index and EQ-5D-3L VAS) before proceeding, thereby resulting in complete data. Missing data for all other study measures except SF-12v2 were mean substituted. Although mean substitution can affect estimates for variance and correlations [55], it is considered to be an appropriate approach when the degree of missing data is small [55, 56]. Since the percentage of missing data among the final set of 316 responses was low (0.28 %), mean substitution was considered to an appropriate technique for missing data replacement in the context of this study. The proportion of missing data for the SF-12v2 was 0.32 %. Missing values for SF-12v2 were handled by the missing score estimation technique developed by QualityMetric and undertaken using the QualityMetric SF Health Outcomes™ Scoring Software.
Convergent validity refers to the extent to which different scales measuring the same underlying construct correlate. In order to ascertain the convergent validity of the EQ-5D-3L instrument, the correlation of EQ-5D-3L five index domains with SF-12v2 domains and CGSQ was examined. Spearman rank correlation was used to examine the relationship between the hypothesized constructs. Correlations between 0.1 and 0.29 were considered small, between 0.3 and 0.49 as moderate, and above 0.5 as strong [57]. Based on the general EQ-5D-3L literature [46, 58–62], moderate to strong correlations (direction listed in parenthesis) were hypothesized between the following sets of constructs: EQ-5D-3L ‘mobility’ domain and SF-12v2 ‘physical functioning’ domain (−), EQ-5D-3L ‘anxiety/depression’ domain and SF-12v2 ‘mental health’ domain (−), EQ-5D-3L ‘anxiety/depression’ domain and CGSQ ‘caregiver burden’ (+), EQ-5D-3L ‘pain/discomfort’ domain and SF-12v2 ‘bodily pain’ domain (−), EQ-5D-3L ‘usual activities’ domain and SF-12v2 ‘bodily pain’ (−) and ‘role physical’ domain (−), EQ-5D-3L ‘self-care’ domain and SF-12v2 ‘bodily pain’ (−) and ‘role physical’ domain (−), EQ-5D-3L index and SF-12v2 PCS (+) and MCS (+), EQ-5D-3L index and CGSQ ‘caregiver burden’ (−), EQ-5D-3L VAS and SF-12v2 ‘general health’ domain (+), PCS (+), and MCS (+), and EQ-5D-3L VAS and CGSQ ‘caregiver burden’ (−). A low and insignificant correlation among measures of theoretically unrelated constructs evinces discriminant validity. Discriminant validity was determined by observing the correlation of EQ-5D-3L ‘mobility’ and ‘self-care’ scores with SF-12v2 ‘role emotional,’ ‘mental health,’ and MCS scores. A low and statistically insignificant correlation was expected among these dissimilar constructs.
In the context of this study, the known-groups validity refers to the ability of an instrument to differentiate among participants by severity level. To determine the known-groups validity of the EQ-5D-3L instrument, variation in EQ-5D-3L index and EQ-5D-3L VAS scores by level of autism severity in the child was examined. Prior studies of EQ-5D-3L psychometrics in different patient populations have examined known-groups validity through an examination of variation in EQ-5D-3L index and VAS scores by level of disease severity [46, 63, 64]. Also, studies in autism have shown care recipient disease severity to be a predictor of caregiver HRQOL [15]. Therefore, in this study, we hypothesized that caregiver EQ-5D-3L index and VAS scores would decrease with an increase in autism severity among the care recipient. Caregivers were categorized into tertiles based on the care recipients’ autism severity scores that were measured using the SCQ instrument. Using the Kruskal–Wallis test, the EQ-5D-3L index and EQ-5D-3L VAS scores of caregivers were compared across the tertile categories. A nonparametric test was used because of the non-normal distribution of EQ-5D-3L scores. Post-hoc analyses were conducted using the Mann–Whitney U test. A gradient relationship between caregiver utility scores and level of autism severity in the child was expected, such that utility scores decrease with an increase in autism severity.
The internal consistency reliability of EQ-5D-3L instrument was determined using Cronbach’s alpha. A Cronbach’s alpha value of greater than or equal to 0.70 is considered adequate [65]. Corrected item-total correlations were also determined and used to observe the reliability of individual items. A correlation value greater than 0.20 of an item with the total score sans item is considered acceptable [66]. Floor and ceiling effects for the EQ-5D-3L instrument were assessed by determining the percentage of participants who received the lowest (floor effect) and highest (ceiling effect) possible scores. These effects are considered to be absent when the percentage of participants with lowest (floor) or highest (ceiling) possible score is less than or equal to 20 % [67].
For tests of statistical significance, P values less than 0.05 were used. Data analyses were performed using Statistical Package for Social Sciences (SPSS) version 20.0 (SPSS Inc., Chicago, IL).
Results
Sample characteristics
Table 1 lists the sociodemographic characteristics of caregivers and care recipients. The final sample included 316 primary caregivers of children with autism. The mean age of participants was 41.3 years (±6.9). In terms of gender, race, and marital status, a majority of participants were female (93.7 %), white (87.3 %), and married (80.4 %), respectively. In order to put into perspective the characteristics of caregivers in our study, we compared our sample characteristics to those of caregivers of children with special health care needs in the USA [68]. The average of our sample was similar to national caregiver population (41.3 vs. 40.6 years). When compared to the national caregiver population for children with special health care needs, a higher proportion of our sample included females (93.7 vs. 72 %) and white (87.3 vs. 60 %). A higher proportion of our sample were married (80.4 vs. 53 %), college graduate (36.4 vs. 17 %), working full-time (38.3 vs. 35 %), and had income $50,000 or more (72.7 vs. 37 %) as compared to national caregiver population for children with special health care needs. Most (91 %) of the caregivers in our sample were mothers of children with autism, which is consistent with the general autism literature [69, 70]. As per the child with autism, 60.8 % had classic autism, 18.4 % had Asperger’s syndrome, and 20.3 % had PDD-NOS. Though the exact distribution of different forms of autism is not available in the literature, a higher prevalence of classic autism has been indicated [71]. Almost 80 % of children with autism were male, which is consistent with the general prevalence estimates for this disorder [2]. The average age of the care recipients was 9.5 years (±3.9).
EQ-5D-3L descriptives
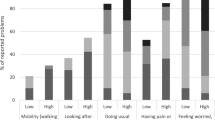
Figure 1 depicts the response received for the EQ-5D-3L instrument. Almost three-fifths of participants reported having problems in the domain of ‘anxiety/depression.’ Half of the participants reported having problems with ‘pain/discomfort,’ and one-fourth indicated problems with ‘usual activities’. For each of the five domains, very few participants indicated having ‘extreme problems.’ Least problems were indicated in the ‘self-care’ domain. The mean EQ-5D-3L index score of caregivers was 0.82 (±0.16), and the mean EQ-5D-3L VAS score was 76.00 (±16.11).

Distribution of the EQ-5D-3L health states among study participants (N = 316)
Table 2 lists the five most common EQ-5D-3L health states among caregivers of children with autism. Almost 24 % of participants reported being in perfect health state (‘11111’) and had an index score of ‘1.00’. These participants had an average EQ-5D-3L VAS score of 87.83 (±7.5). Cumulatively, the top five EQ-5D-3L health states accounted for more than three-fourths (78.2 %) of participants. The average EQ-5D-3L index score for participants in the top five health states was 0.8723 (±0.0873), while the average VAS score for this group was 79.78 (±12.94).
Convergent and discriminant validity
Table 3 describes the correlation between EQ-5D-3L domains and relevant study constructs (SF-12v2 and CGSQ). All hypothesized relationships for convergent validity except for those between EQ-5D-3L ‘self-care’ domain and SF-12v2 ‘bodily pain’ and ‘role physical’ domain were supported. Low, but statistically significant, correlation was observed between EQ-5D-3L ‘self-care’ and SF-12v2 ‘bodily pain’ (−0.225, P < 0.001) and ‘role physical’ (−0.166, P = 0.003) domain. Among the hypothesized relationships, the strongest correlation was observed between the EQ-5D-3L VAS and SF-12v2 ‘general health’ domain (0.663, P < 0.001). The EQ-5D-3L index and VAS were significantly correlated with SF-12v2 PCS and MCS domains. Higher caregiver burden scores were associated with lower EQ-5D-3L index (−0.358, P < 0.001) and VAS (−0.322, P < 0.001) scores. As hypothesized for indices of discriminant validity, a low and statistically insignificant correlation was observed between scores for EQ-5D-3L ‘mobility’ and ‘self-care’ domains and SF-12v2 ‘role emotional,’ ‘mental health,’ and MCS domains.
Known-groups validity
Results from Kruskal–Wallis test revealed significant differences in caregivers EQ-5D-3L index and EQ-5D-3L VAS scores by care recipients’ levels of autism severity (Table 4). Post-hoc analysis revealed that the median (range) index scores were lower among the third tertile (i.e., most severe) autism severity group as compared to the first (i.e., least severe) [0.81 (0.20–1.00) vs. 0.83 (0.26–1.00), P = 0.005] and second [0.81 (0.20–1.00) vs. 0.84 (0.29–1.00), P = 0.012] tertile groups. Similarly, EQ-5D-3L VAS scores were lower among the third tertile group as compared to the first and second tertile groups. No significant differences were noted between the first and second tertiles on either the index or the VAS scores.
Reliability
The five-item EQ-5D-3L instrument had internal consistency reliability (Cronbach’s alpha) of 0.63, which was less than the acceptable criteria of 0.70. However, all corrected item-total correlations were higher than the minimal acceptable value of 0.20 (Table 5).
Floor and ceiling effects
Roughly 24 % of participants had the highest possible index score of 1.00, indicating the presence of ceiling effect for EQ-5D-3L index. These participants reported ‘no problems’ in the five health domains (‘11111’) and had scores indicative of a perfect health state. Floor effect was absent, since none of the participants reported the lowest possible health state (‘33333’). When observing the distribution of EQ-5D-3L VAS, no floor or ceiling effects were seen. Roughly 3 % of participants had the highest possible score (100) and none had the lowest score (0).
Discussion
This study assessed the psychometric properties of the EQ-5D-3L for use among primary caregivers of children with autism. The EQ-5D-3L is a commonly used generic utility instrument, which has been previously validated in several different patient populations [42, 72–75]. A thorough review of the literature did not reveal any previous study that has determined the psychometric profile of the EQ-5D-3L among autism caregivers. The conciseness of the EQ-5D-3L offers low respondent burden. Further, the availability of both online and paper versions provides researchers the flexibility of using this instrument in different settings. These factors, together with the EQ-5D-3L instrument’s ability to provide information concerning patient preferences, makes it an appealing choice for studies, including the current one, aimed at HRQOL measurement. The convergent validity, discriminant validity, known-groups validity, internal consistency reliability, and floor and ceiling effects of the EQ-5D-3L instrument were evaluated in this study. Considering that there is no autism-specific utility instrument currently available, the EQ-5D-3L presents a psychometrically sound option for researchers who aim to assess HRQOL among this growing population of caregivers.
Study results revealed EQ-5D-3L to have good construct (convergent, discriminant, and known-groups) validity. All except two of the hypothesized relationships of EQ-5D-3L with relevant constructs in the study were supported, thereby providing good evidence of its convergent validity. The EQ-5D-3L domains correlated well with similar domains in the SF-12v2 instrument. Both instruments are among the most commonly used in the patient-reported outcomes literature. The SF-12v2 has been previously used in studies of autism caregiving [13, 15, 16] and indicated to perform well. The EQ-5D-3L provides good alternative to measure caregiver HRQOL, with the added advantage of ascertaining caregiver preferences for health states. As expected, the EQ-5D-3L index and VAS scores were significantly related to caregiver burden. This is the first study to highlight the relationship between caregiver burden and general utility instrument. Future studies may use the EQ-5D-3L to further investigate the role played by burden and other caregiving situational factors in influencing caregivers’ health state preferences. In the present study, an insignificantly low correlation was found among EQ-5D-3L ‘mobility’ and ‘self-care’ scores and SF-12v2 ‘role emotional,’ ‘mental health,’ and MCS scores, thereby demonstrating support for EQ-5D-3L discriminant validity.
As hypothesized, the EQ-5D-3L index and VAS scores were lower for caregivers who had a child with autism with extreme severity, that is, had SCQ score in third tertile, as compared to those with a child with low (first tertile) or moderate (second tertile) severity. This provides some evidence of the EQ-5D-3L instrument ability to distinguish between known groups of autism caregivers. However, this result should be interpreted in the presence of the fact that the scores for the first and second tertile were statistically insignificant. A plausible explanation for this finding could be that the classification of autism severity among the care recipient into tertiles was arbitrary and not based on scoring structure of the autism severity instrument (SCQ) used in the study. Alternatively, it is possible that the EQ-5D-3L was not sensitive enough to discern differences in preference values among caregivers having child with ‘low’ and ‘moderate’ autism severity. When studying HRQOL among caregivers of elderly patients with Alzheimer’s, Bell et al. [76] found a lack of variation in preference scores (captured using HUI-II) among caregivers by care recipient disease severity. The authors indicated that generic preference-weighted instruments may not be sensitive enough to capture variation in health state preferences by disease severity. In contrast, Tilford et al. [77] were able to detect differences in preference scores (captured using QWB) among caregivers of children with spina bifida by level of disease severity. Our results suggest that the EQ-5D-3L is sensitive in terms of distinguishing preference scores among caregivers at the higher end of disease severity with those at lower and medium end, but is unlikely to perform well in comparing preferences among the latter two groups.
The internal consistency reliability of the EQ-5D-3L instrument was lower (0.63 Cronbach’s alpha) than the acceptable limit of 0.70 [65]. However, reliability assessed through corrected item-total correlations was satisfactory. A true interpretation of internal consistency of the EQ-5D-3L is unclear, considering that the instrument includes one question for each health domain [78]. It may also be reflective of some heterogeneity among these domains. Ceiling effects were present in index scores, with almost one in five participants reporting a perfect health state. Prior studies of EQ-5D-3L psychometric profile in different patient populations have also reported the presence of ceiling effects [45, 79]. The presence of ceiling effects may present some challenges in EQ-5D-3L responsiveness, but is unlikely to limit its ability to serve as a useful generic utility instrument. Floor effects were absent for index scores. Floor and ceiling effects were absent for the EQ-5D-3L VAS.
There are few limitations in the study. The study was conducted among caregivers of children with autism who were registered with the IAN. It is likely that families of children with autism registered with the IAN have greater access to resources and increased awareness of the disorder. With more than 38,000 members including individuals with autism, family members, and caregivers, the number of individuals registered with the IAN still constitutes a small proportion of the ~2 million individuals that are affected with autism in the USA. Therefore, the results of the proposed study may not be generalizable to all families of children with autism. When comparing our sample characteristics to national profile of caregivers of children with special healthcare needs [68], differences were observed. Our sample had more females and whites, and generally ranked higher on indicators of socioeconomic status. It should be noted that our sample included only primary caregivers of children with autism, while the comparator group included any caregiver that provided unpaid care to a child with special healthcare needs [68]. Further, autism has been found to be more prevalent among whites [2] and in families of higher socioeconomic status [80]. When examining the relationship between autism and socioeconomic status among a population-based sample of children in the USA, Durkin et al. [81] found an increasing prevalence of autism with socioeconomic status, reflecting a dose–response curve. The authors suggested that there may be a causal link between socioeconomic advantage and the risk of developing autism. Another large epidemiological investigation involving more than 4,000 children with autism in the state of California found the risk of autism to increase with maternal education [82]. These factors may explain some of the differences, particularly the higher socioeconomic status, observed among our sample as compared to the national profile of caregivers of children with special healthcare needs. Since a cross-sectional design was used for study purposes, we could not test the criterion validity (predictive validity) and test–retest reliability of the EQ-5D-3L instrument. Future studies could test the usefulness of EQ-5D-3L among autism caregivers using a longitudinal research design.
Conclusion
To the best of our knowledge, this is the first study to test the psychometric properties of the EQ-5D-3L among caregivers of children with autism. The EQ-5D-3L was found to have good convergent and discriminant validity and met study hypothesis. The EQ-5D-3L domains correlated well with theoretically similar domains from other instruments (convergent validity) and had low correlation with unrelated constructs (discriminant validity). Known-groups validity was good, and the EQ-5D-3L scores varied as expected across known-groups. Mixed results were seen as per the homogeneity of EQ-5D-3L items. Though the Cronbach’s alpha was slightly lower than the generally acceptable 0.70 value, the corrected item-total correlations were adequate. Floor effects were absent, but ceiling effects were seen for EQ-5D-3L index scores. The EQ-5D-3L VAS did not have floor and ceiling effects. As the research on studying HRQOL outcomes among caregivers of children with autism gains increasing prominence, it may be of value to also document their preferences for health states. The EQ-5D-3L is a viable preference-based generic instrument that has been widely used in the health outcomes literature. As found in the current study, the instrument also works well in autism caregiving population.
Abbreviations
- EQ-5D-3L:
-
EuroQol Five Dimensional Questionnaire
- VAS:
-
Visual analog scale
- IAN:
-
Interactive Autism Network
- PDD-NOS:
-
Pervasive developmental disorder-not otherwise specified
- CDC:
-
Centers for Disease Control and Prevention
- HRQOL:
-
Health-related quality of life
- CGSQ:
-
Caregiver Strain Questionnaire
- SCQ:
-
Social Communication Questionnaire
- SF-12v2:
-
Medical Outcomes Study Short-Form Health Survey version 2
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text revision). Washington, D.C.: American Psychiatric Press.
Baio, J. (2012). Prevalence of autism spectrum disorders: Autism and developmental disabilities monitoring network, 14 sites, United States, 2008. Surveillance Summaries, 61(SS03), 1–19.
Elsabbagh, M., Divan, G., Koh, Y. J., Kim, Y. S., Kauchali, S., Marcín, C., et al. (2012). Global prevalence of autism and other pervasive developmental disorders. Autism Research, 5(3), 160–179.
Baron-Cohen, S., Scott, F. J., Allison, C., Williams, J., Bolton, P., Matthews, F. E., et al. (2009). Prevalence of autism-spectrum conditions: UK school-based population study. The British Journal of Psychiatry, 194(6), 500–509.
Kim, Y. S., Leventhal, B. L., Koh, Y. J., Fombonne, E., Laska, E., Lim, E. C., et al. (2011). Prevalence of autism spectrum disorders in a total population sample. American Journal of Psychiatry, 168(9), 904–912.
Geraghty, M. E., Depasquale, G. M., & Lane, A. E. (2010). Nutritional intake and therapies in autism a spectrum of what we know: Part 1. ICAN: Infant, Child, & Adolescent Nutrition, 2(1), 62–69.
Hertz-Picciotto, I., Croen, L. A., Hansen, R., Jones, C. R., van de Water, J., & Pessah, I. N. (2006). The CHARGE study: An epidemiologic investigation of genetic and environmental factors contributing to autism. Environmental Health Perspectives, 114(7), 1119–1125.
Bebko, J. M., Konstantareas, M. M., & Springer, J. (1987). Parent and professional evaluations of family stress associated with characteristics of autism. Journal of Autism and Developmental Disorders, 17(4), 565–576.
Duarte, C. S., Bordin, I. A., Yazigi, L., & Mooney, J. (2005). Factors associated with stress in mothers of children with autism. Autism: The International Journal of Research and Practice, 9(4), 416–427.
Davis, N. O., & Carter, A. S. (2008). Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: Associations with child characteristics. Journal of Autism and Developmental Disorders, 38(7), 1278–1291.
Barker, E. T., Hartley, S. L., Seltzer, M. M., Floyd, F. J., Greenberg, J. S., & Orsmond, G. I. (2011). Trajectories of emotional wellbeing in mothers of adolescents and adults with autism. Developmental Psychology, 47(2), 551–561.
Giallo, R., Wood, C. E., Jellett, R., & Porter, R. (2011). Fatigue, wellbeing and parental self-efficacy in mothers of children with an Autism Spectrum Disorder. Autism: The International Journal of Research and Practice, [Epub ahead of print]. doi:10.1177/1362361311416830.
Allik, H., Larsson, J. O., & Smedje, H. (2006). Health-related quality of life in parents of schoolage children with Asperger syndrome or high-functioning autism. Health and Quality of Life Outcomes, 4, 1.
Lee, G. K., Lopata, C., Volker, M. A., Thomeer, M. L., Nida, R. E., Toomet, J. A., et al. (2009). Health-related quality of life of parents of children with high-functioning autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 24(4), 227–239.
Khanna, R., Madhavan, S. S., Smith, M. J., Patrick, J. H., Tworek, C., & Becker-Cottrill, B. (2011). Assessment of health-related quality of life among primary caregivers of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 41(9), 1214–1227.
Rizk, S., Pizur-Barnekow, K., & Darragh, A. R. (2011). Leisure and social participation and health-related quality of life in caregivers of children with autism. Occupation, Participation and Health, 31(4), 164–171.
Testa, M. A., & Simonson, D. C. (1996). Assesment of quality-of-life outcomes. New England of Journal Medicine, 334, 835–840.
Bennett, K., & Torrance, G. (1996). Measuring health state preferences and utilities: Rating scale, time trade-off and standard gamble techniques. In B. Spilker (Ed.), Quality of life and pharmacoeconomics in clinical trials (2nd ed., pp. 253–266). Philadelphia: Lippincott-Raven.
Torrance, G. W., & Feeny, D. (1989). Utilities and quality-adjusted life years. International Journal of Technology Assessment in Health Care, 5(4), 559–575.
Tsevat, J. (2000). What do utilities mean? Medical Care, 38(9 Suppl), 160–164.
Al-Janabi, H., Flynn, T. N., & Coast, J. (2011). QALYs and carers. Pharmacoeconomics, 29(12), 1015–1023.
Spijker, A., Verhey, F., Graff, M., Grol, R., Adang, E., Wollersheim, H., et al. (2009). Systematic care for caregivers of people with dementia in the ambulatory mental health service: Designing a multicentre, cluster, randomized, controlled trial. BMC Geriatrics, 9(1), 21.
The, EuroQol Group. (1990). EuroQol—A new facility for the measurement of health-related quality of life. Health Policy, 16(3), 199–208.
EQ-5D User Guide. http://www.euroqol.org/fileadmin/user_upload/Documenten/PDF/Folders_Flyers/UserGuide_EQ-5D-3L.pdf. Accessed 17 August 2012.
Koopmanschap, M. A., van Exel, N., Van Den Berg, B., & Brouwer, W. B. (2008). An overview of methods and applications to value informal care in economic evaluations of healthcare. Pharmacoeconomics, 26(4), 269–280.
Busschbach, J. J., Brouwer, W. B., Van Der Donk, A., Passchier, J., & Rutten, F. F. (1998). An outline for a cost-effectiveness analysis of a drug for patients with Alzheimers disease. Pharmacoeconomics, 13(1 Part 2), 21–34.
Feeney, D., Torrance, G. W., & Gabriel, S. E. (1996). Health Utilities Index. Philadelphia, PA: Lippincott-Raven.
Kaplan, R. M., Atkins, C. J., & Timms, R. (1984). Validity of a quality of well-being scale as an outcome measure in chronic obstructive pulmonary disease. Journal of Chronic Diseases, 37(2), 85–95.
Balaban, D. J., Sagi, P. C., Goldfarb, N. I., & Nettler, S. (1986). Weights for scoring the quality of well-being instrument among rheumatoid arthritics: A comparison to general population weights. Medical Care, 24(11), 973–980.
Brazier, J., Usherwood, T., Harper, R., & Thomas, K. (1998). Deriving a preference-based single index from the UK SF-36 Health Survey. Journal of Clinical Epidemiology, 51(11), 1115–1128.
Brazier, J., Roberts, J., Tsuchiya, A., & Busschbach, J. (2004). A comparison of the EQ-5D and SF-6D across seven patient groups. Health Economics, 13(9), 873–884.
Räsänen, P., Roine, E., Sintonen, H., Semberg-Konttinen, V., Ryynänen, O. P., & Roine, R. (2006). Use of quality-adjusted life years for the estimation of effectiveness of health care: A systematic literature review. International Journal of Technology Assessment in Health Care, 22(2), 235–241.
Khanna, D., & Tsevat, J. (2007). Health-related quality of life-an introduction-page 2. American Journal of Managed Care, 13(Suppl 9), S218–S223.
Serrano-Aguilar, P. G., Lopez-Bastida, J., & Yanes-Lopez, V. (2006). Impact on health-related quality of life and perceived burden of informal caregivers of individuals with Alzheimer’s disease. Neuroepidemiology, 27(3), 136–142.
Martínez-Martín, P., Benito-Leon, J., Alonso, F., Catalan, M. J., Pondal, M., Zamarbide, I., et al. (2005). Quality of life of caregivers in Parkinson’s disease. Quality of Life Research, 14(2), 463–472.
Martínez-Martín, P., Forjaz, M. J., Frades-Payo, B., Rusiñol, A. B., Fernández-García, J. M., Benito-León, J., et al. (2007). Caregiver burden in Parkinson’s disease. Movement Disorders, 22(7), 924–931.
Brouwer, W. B., Van Exel, N., van de Berg, B., Dinant, H. J., Koopmanschap, M. A., & van den Bos, G. A. (2004). Burden of caregiving: Evidence of objective burden, subjective burden, and quality of life impacts on informal caregivers of patients with rheumatoid arthritis. Arthritis Care & Research, 51(4), 570–577.
Sewitch, M. J., McCusker, J., Dendukuri, N., & Yaffe, M. J. (2004). Depression in frail elders: Impact on family caregivers. International Journal of Geriatric Psychiatry, 19(7), 655–665.
Andrén, S., & Elmståhl, S. (2008). The relationship between caregiver burden, caregivers’ perceived health and their sense of coherence in caring for elders with dementia. Journal of Clinical Nursing, 17(6), 790–799.
Prieto, L., Sacristan, J. A., Hormaechea, J. A., Casado, A., Badia, X., & Gomez, J. C. (2004). Psychometric validation of a generic health-related quality of life measure (EQ-5D) in a sample of schizophrenic patients. Current Medical Research and Opinion, 20(6), 827–835.
König, H. H., Roick, C., & Angermeyer, M. C. (2007). Validity of the EQ-5D in assessing and valuing health status in patients with schizophrenic, schizotypal or delusional disorders. European Psychiatry, 22(3), 177–187.
Kunz, S. (2010). Psychometric properties of the EQ-5D in a study of people with mild to moderate dementia. Quality of Life Research, 19(3), 425–434.
König, H. H., Born, A., Günther, O., Matschinger, H., Heinrich, S., Riedel-Heller, S. G., et al. (2010). Validity and responsiveness of the EQ-5D in assessing and valuing health status in patients with anxiety disorders. Health and Quality of Life Outcomes, 8, 47.
Coucill, W., Bryan, S., Bentham, P., Buckley, A., & Laight, A. (2001). EQ-5D in patients with dementia an investigation of inter-rater agreement. Medical Care, 39(8), 760–771.
Luo, N., Low, S., Lau, P. N., Au, W. L., & Tan, L. C. S. (2009). Is EQ-5D a valid quality of life instrument in patients with Parkinson’s disease? A study in Singapore. Annals of the Academy of Medicine, Singapore, 38(6), 521–528.
Schrag, A., Selai, C., Jahanshahi, M., & Quinn, N. P. (2000). The EQ-5D—A generic quality of life measure—Is a useful instrument to measure quality of life in patients with Parkinson’s disease. Journal of Neurology, Neurosurgery and Psychiatry, 69(1), 67–73.
Wolfs, C. A., Dirksen, C. D., Kessels, A., Willems, D. C., Verhey, F. R., & Severens, J. L. (2007). Performance of the EQ-5D and the EQ-5D+ C in elderly patients with cognitive impairments. Health and Quality of Life Outcomes, 5(1), 33.
Interactive Autism Network (IAN) website. https://www.ianresearch.org/login. Accessed 26 March 2012.
Ware, J. E., Kosinski, M., Turner-Bowker, D. M., & Gandek, B. (2002). User’s manual for the SF-12v2 Health survey (with a supplement documenting SF-12 health survey). Lincoln, RI: Quality Metric Incorporated.
Brannan, A. M., Heflinger, C. A., & Bickman, L. (1997). The Caregiver Strain Questionnaire: Measuring the impact on the family of living with a child with serious emotional problems. Journal of Emotional and Behavioral Disorders, 5(4), 212–222.
Rutter, M., Bailey, A., & Lord, C. (2003). Social Communication Questionnaire-WPS (SCQ-WPS). Los Angeles, CA: Western Psychological Services.
Shaw, J. W., Johnson, J. A., & Coons, S. J. (2005). US valuation of the EQ-5D health states: Development and testing of the D1 valuation model. Medical Care, 43(3), 203–220.
Luo, N., Johnson, J. A., Shaw, J. W., Feeny, D., & Coons, S. J. (2005). Self-reported health status of the general adult US population as assessed by the EQ-5D and Health Utilities Index. Medical Care, 43(11), 1078–1086.
Khanna, R., Madhavan, S. S., Smith, M. J., Tworek, C., Patrick, J. H., & Becker-Cottrill, B. (2012). Psychometric properties of the Caregiver Strain Questionnaire (CGSQ) among caregivers of children with autism. Autism: The International Journal of Research and Practice, 16(2), 179–199.
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7(2), 147–177.
Fox-Wasylyshyn, S. M., & El-Masri, M. M. (2005). Handling missing data in self-report measures. Research in Nursing & Health, 28(6), 488–495.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Lawrence Earlbaum Associates.
Lubetkin, E. I., Jia, H., & Gold, M. R. (2004). Construct validity of the EQ-5D in low-income Chinese American primary care patients. Quality of Life Research, 13(8), 1459–1468.
Nowels, D., McGloin, J., Westfall, J. M., & Holcomb, S. (2005). Validation of the EQ-5D quality of life instrument in patients after myocardial infarction. Quality of Life Research, 14(1), 95–105.
Savoia, E., Fantini, M. P., Pandolfi, P. P., Dallolio, L., & Collina, N. (2006). Assessing the construct validity of the Italian version of the EQ-5D: Preliminary results from a cross-sectional study in North Italy. Health and Quality of Life Outcomes, 4(1), 47.
Kontodimopoulos, N., Pappa, E., Niakas, D., Yfantopoulos, J., Dimitrakaki, C., & Tountas, Y. (2008). Validity of the EuroQoL (EQ-5D) instrument in a Greek general population. Value in Health, 11(7), 1162–1169.
Mahadeva, S., Wee, H. L., Goh, K. L., & Thumboo, J. (2009). The EQ-5D (Euroqol) is a valid generic instrument for measuring quality of life in patients with dyspepsia. BMC Gastroenterology, 9(1), 20.
Ellis, J. J., Eagle, K. A., Kline-Rogers, E. M., & Erickson, S. R. (2005). Validation of the EQ-5D in patients with a history of acute coronary syndrome. Current Medical Research and Opinion, 21(8), 1209–1216.
Lang, H. C., Chuang, L., Shun, S. C., Hsieh, C. L., & Lan, C. F. (2010). Validation of EQ-5D in patients with cervical cancer in Taiwan. Supportive Care in Cancer, 18(10), 1279–1286.
Nunnally, J. C. (1978). Assessment of reliability. Psychometric theory (2nd ed., pp. 225–255). New York: MacGraw-Hill Series.
Streiner, D. L., & Norman, G. R. (1995). Health measurement scale, a practical guide to their development and use (2nd ed.). Oxford: Oxford University Press.
Holmes, W., & Shea, J. (1997). Performance of a new, HIV/AIDS-targeted quality of life (HATQOL) instrument in asymptomatic sero-positive individuals. Quality of Life Research, 6(6), 561–571.
National Alliance for Caregiving and AARP. Caregiving in the US 2009. http://www.caregiving.org/data/Caregiving_in_the_US_2009_full_report.pdf. Accessed 1 March 2013.
Rodrigue, J. R., Morgan, S. B., & Geffken, G. R. (1992). Psychosocial adaptation of fathers of children with autism, Down syndrome, and normal development. Journal of Autism and Developmental Disorders, 22(2), 249–263.
Phetrasuwan, S., & Shandor Miles, M. (2009). Parenting stress in mothers of children with autism spectrum disorders. Journal for Specialists in Pediatric Nursing, 14(3), 157–165.
Fombonne, E., Simmons, H., Ford, T., Meltzer, H., & Goodman, R. (2001). Prevalence of pervasive developmental disorders in the British nationwide survey of child mental health. Journal of the American Academy of Child and Adolescent Psychiatry, 40(7), 820–827.
Aggarwal, R., Wilke, C. T., Pickard, S., Vats, V., Mikolaitis, R., Fogg, L., et al. (2009). Psychometric properties of the EuroQol-5D and Short From-6D in patients with systemic lupus erythematosus. The Journal of Rheumatology, 36(6), 1209–1216.
Oster, C., Willembrand, M., Dyster-Aas, J., Kildal, M., & Ekselius, L. (2009). Validation of EuroQoL questionnaire in burn injured adults. Burns, 35(5), 723–732.
Zhao, F. L., Yue, M., Yang, H., Wang, T., & Wu, J. H. (2010). Validation and comparison of EuroQol and short form 6D in chronic prostatitis patients. Value in Health, 13(5), 649–656.
Stochl, J., Croudace, T., Perez, J., Birchwood, M., Lester, H., & Marshall, M. Usefulness of EQ-5D for evaluation of health-related quality of life in young adults with first-episode psychosis. Quality of Life Research [Epub ahead of print]. doi:10.1007/s11136-012-0222-7.
Bell, C. M., Araki, S. S., & Neumann, P. J. (2001). The association between caregiver burden and caregiver health-related quality of life in Alzheimer disease. Alzheimer Disease and Associated Disorders, 15(3), 129–136.
Tilford, J. M., Grosse, S. D., Robbins, J. M., Pyne, J. M., Cleves, M. A., & Hobbs, C. A. (2005). Health state preference scores of children with spina bifida and their caregivers. Quality of Life Research, 14(4), 1087–1098.
Lipscomb, J., Gotay, C. C., & Snyder, C. (2005). Outcomes assessment in cancer. Cambridge, MA: Cambridge University Press.
Schweikert, B., Hahmann, H., & Leidl, R. (2006). Validation of the EuroQol questionnaire in cardiac rehabilitation. Heart, 92(1), 62–67.
Becker, K. G. (2012). Autism, autoimmune disease and socioeconomic status. Autism: The International Journal of Research and Practice, 2(104), 2.
Durkin, M. S., Maenner, M. J., Meaney, F. J., Levy, S. E., DiGuiseppi, C., Nicholas, J. S., et al. (2010). Socioeconomic inequality in the prevalence of autism spectrum disorder: Evidence from a US cross-sectional study. PLoS ONE, 5(7), e11551.
Croen, L. A., Grether, J. K., & Selvin, S. (2002). Descriptive epidemiology of autism in a California population: Who is at risk? Journal of Autism and Developmental Disorders, 32(3), 217–224.
Acknowledgments
This study was financially supported by a New Investigator Award from the American Association of Colleges of Pharmacy (AACP), Alexandria, VA.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khanna, R., Jariwala, K. & Bentley, J.P. Psychometric properties of the EuroQol Five Dimensional Questionnaire (EQ-5D-3L) in caregivers of autistic children. Qual Life Res 22, 2909–2920 (2013). https://doi.org/10.1007/s11136-013-0423-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-013-0423-8