
Abstract
Purpose
The EORTC QLQ-H&N35 (H&N35) is widely used to measure quality of life in head and neck cancer patients. The aims of this study were to obtain insight into a) the languages in which the H&N35 has been used and the psychometric properties in those languages, b) the study designs, and c) its acceptance by patients and investigators.
Methods
A systematic literature review was performed searching for all original papers that had used at least one item of the H&N35. Identified papers were read and the information about methodological issues abstracted statistically analysed.
Results
A total of 136 papers were identified. The H&N35 was administered in 19 different languages in 27 countries. The study design was cross-sectional in the majority of studies (53 %), prospective cohort studies (31 %), phase-II-trials (7 %), phase-III-trials (6 %) and case–control studies (1 %). The scales with the highest percentages of missing values were Sexuality (11.5 %) and Speech (7 %). The median Cronbach’s alpha of the multi-item scales ranged from 0.61 (Senses) to 0.93 (Sexuality). Construct validity was rarely investigated. On average, 12 scales (range 0-18) of the instrument were used by the investigators. The scale most often used was swallowing (in 85 % of studies) and least often used was Weight Gain (39 %).
Conclusion
The H&N35 is widely used throughout the world, mainly in observational studies, and has demonstrated robust psychometric features in different languages. However, some methodological problems reported imply that the instrument can be improved in some areas.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
The EORTC Quality of Life Group develops site-specific modules to be used with a core questionnaire, the EORTC QLQ-C30. One of the first was the module for patients with head and neck cancer, the EORTC QLQ-H&N37 [1], later revised and shortened to its final version with 35 items, the H&N35 [2]. This module consists of 7 multi-item scales, measuring pain in the mouth, problems with swallowing, senses, speech, social eating and social contact, and 11 single-item scales, assessing problems with teeth, mouth opening, dry mouth, sticky saliva, coughing, feeling ill, as well as use of analgesics, nutritional supplements, feeding tube and finally weight gain and weight loss.
The module has been translated into 53 languages (February 2012, http://groups.eortc.be) and is in use worldwide as one of the standard instruments for measuring quality of life in head and neck cancer patients [3, 4].
Some issues have been raised that may hamper the use of the H&N35. One criticism occasionally raised is that patients may feel annoyed by some of the items, for example, those enquiring about problems with sexual functioning [5, 6]. A matter of debate is whether this presents difficulty for the researcher who feels uncomfortable in asking such questions or for the patient who feels embarrassed or irritated in answering. Another criticism concerns items that may not be applicable to some of the patients, for example, questions about swallowing solid food administered to patients who are tube fed or about hoarseness when the larynx has been removed [7]. Little is known about the use of the H&N35 in research, on the way the psychometric issues are reflected in different languages, and how well the multi-item scales are accepted by patients and investigators.
The goal of the present study was to review all papers relating to studies that have used the H&N35 module to date, investigating potential methodological problems and benefits. Questions to be answered were as follows:
-
1.
In what languages has the H&N35 been used and validated since it was published (cross-cultural use)?
-
2.
How reliable and valid are the multi-item scales of the H&N35? Were any psychometric problems reported (psychometrics)?
-
3.
How accepted are the questions by the patients, that is, how frequently did they skip specific items or scales (acceptance by patients)?
-
4.
How accepted are the questions and the scales by the investigators, that is, do they omit items or scales (acceptance by investigators)?
-
5.
How often is the H&N35 used for what types of studies?
Methods
The H&N35 contains 35 items which can be condensed into seven multi-item and eleven single-item symptom scales. All EORTC QoL questionnaires result in scales that score from 0 to 100. A score of 100 indicates perfect QoL in the functioning scales, whereas for the symptom scales, it indicates heavy burden.
A systematic review was performed, searching for all publications up to August 2011 that reported data using the H&N35. Databases searched were Pubmed, EMBASE and Social Science Citation Index. Original papers written in the following languages were eligible for this review: Bosnian, Croatian, Dutch, English, French, German, Japanese, Russian, Serbian, Spanish and Turkish. Papers written in Japanese were translated by a native speaker. All other non-English papers were read by the first author (SS) in the original version.
Search terms entered for title, abstract or key words were “H?N35” and “head and neck module”, respectively. The question mark is used for the search electronic in databases to indicate that any single character or none at all is considered correct. For example, a paper using the abbreviation “HN35” as well as a paper using “H&N35” would be included in the search. The results of that search were presented to a group of health care professionals experienced in the treatment of head and neck cancer within the EORTC Quality of Life Group with the opportunity to add papers that had not been detected by the criteria used in the initial search.
All reviews were excluded; only original papers were analysed. Several papers on the same study population were considered eligible for inclusion as long as different data were presented. It was not always possible to determine exactly whether data from the same population were reported or not. Therefore, all papers from the same author or study group were included even if the presented data came presumably from the same patient sample. Duplicate hits, that is, the same article found in different search engines, were removed.
If no access to the full text was available, the paper’s corresponding author was contacted and asked to send a PDF file or a printed copy of the manuscript.
The following details were documented for each paper: the number of patients assessed with the H&N35, cancer site, language in which the H&N35 was administered, information about compliance and missing values, information on or discussion of methodological problems, challenges or advantages, number of H&N35 scales used, estimates of internal consistency (Cronbach’s alpha), construct validity, study design and topic. These details were entered into a database for statistical analysis, using STATA 11 [8]. The analysis included computation of frequencies, percentages and averages (mean, median) as well as testing differences between groups using Kruskal–Wallis tests.
Results
A total of 136 original papers were found that had used the H&N35 (see Fig. 1). Access to the full text was available for 125, with access to the abstract for the remaining 11. A detailed description of the studies can be found in the supplementary material. Considering all papers together, the H&N35 had been completed by 13,969 patients (subject to the assumption that each paper reported on a different study population). Most often, the H&N35 was used in observational studies; 53 % of the studies had a cross-sectional design, 31 % were prospective cohort studies, 7 % phase-II-trials, 6 % phase-III-trials, 1 % case–control studies, and one study reported on a case series.

Flow diagram of literature search
Cross-Cultural Use: The H&N35 was administered in 19 different languages: German (29 papers), Dutch (26), Swedish (15), English (11), French (8), Norwegian (7), Mandarin (7), Cantonese (6), Danish (4), Spanish (5), Polish (3), Portuguese (3), Japanese (3), Czech (1), Greek (1), Italian (1), Korean (1), Sinhala (1) and Turkish (1). Studies were performed in 26 different countries: The Netherlands (25 studies), Germany (22), Sweden (15), Taiwan (9), Norway (7), France (6), Switzerland (6), United Kingdom (6), Denmark (4), Hong Kong (4), Spain (5), Japan (3), Poland (3), Portugal (2), Canada (2), United States (2), Australia (2), and 1 study each in Austria, Belgium, Brazil, Czech Republic, Greece, Italy, Korea, New Zealand, Sri Lanka and Turkey. A breakdown of studies from the different world regions is displayed in Fig. 2.

Description of papers analysed. Panel a proportion of studies performed in different world regions. Panel b proportion of study designs used in the studies. Note region is defined as being the region where the study was primarily performed not as the region where the paper was published
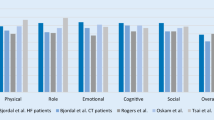
Psychometrics: Sixty-one papers explicitly or implicitly discussed methodological issues of the H&N35. Internal consistency was investigated in 18 papers by means of Cronbach’s alpha and in general appeared to be high, that is Alpha ≥ 70 (Table 1). Moderate or low internal consistency, that is, Alpha < 70, was reported on the Speech [6–9] and Senses [6–8, 10–12] scales. Consequently, the items of the Senses scale were treated as single items in two studies [13, 14]. One study [15] reported a moderate Cronbach’s alpha (0.64) regarding the Pain in the Mouth scale. The average Cronbach’s alpha (computed as the median alpha per scale of all papers where coefficients were reported) ranged from 0.61 (Senses) to 0.93 (Sexuality).
Construct validity was evaluated less frequently. Jayasekara [16] reported overall good construct validity with 87 % scaling successes though the Senses scale exhibited scaling failure, that is, the items were more highly correlated with other scales than with its own scale. Jensen [17] criticised high interscale correlations (> 0.7) as an “indication of overlapping constructs” (p. 35) and, therefore, considered the Social Eating and Social Contact scales to be difficult to differentiate psychometrically and conceptually [17]. On the other hand, he argued that the categorisation of items and scales was sensible because the entire range of the items and scales were covered by the patients’ responses. In a study in laryngeal cancer patients after surgery, items of the Speech scale had scaling failure in 24 %, 1.4 % occurred with Pain in the Mouth and Swallowing, and 0 % in all other multi-item scales [7]. Arraras et al. reported good evidence for sensitivity to change in all scales [12]. Silveira et al. investigated the module’s ability to differentiate symptomatic vs. asymptomatic patients and found good performance except in the following scales: senses, dry mouth, weight gain and weight loss [9]. In three studies, a total H&N35 scale value was calculated based on all head and neck scales [18–20].
Acceptance by patients (missing values): 23 papers reported on percentages of missing values with varying results. The completeness of the questionnaire varied from 66 % [17] to 99 % [21], both studies including patients from Denmark. Scales with missing values included Sexuality, Speech, Teeth and Weight Gain with average percentages of missing values of 11.5, 7.0, 2.7 and 2.0 %, respectively (Table 2). Some authors reported that, regarding the Teeth and Sexuality scales [16, 17, 22], it may remain unclear whether a non-answer was due to the patient being unwilling to answer or because the item did not apply to their status.
The percentage of missing data was unrelated to the region where the study had been performed (P = 0.26 to 0.99).
Acceptance by investigators: The H&N35 consists of 7 multi-item scales and 11 single-item scales. The number of scales reported on in the reviewed studies varied considerably (range: 0 to 18 scales; mean: 12 scales; see Table 3). The use of the scales ranged from 39 % (Weight Gain)—that means that 61 % of the studies did not use or did not report on this scale – to 85 % (Swallowing). Usually, no rationale was given why specific scales were omitted. From the pattern of use, we can see that the scales used least frequently were those where only yes/no answers were possible. These items were reported in less than half of the papers (39 % Weight Gain to 45 % Pain Killers; see Table 3). The Sexuality scale was relatively often (27 %) omitted; however, there were also studies which only used that scale [23, 24]. The number of scales differed significantly between the regions where the study was performed (P = 0.01, see Fig. 3): Whereas in Northern America and in multi-national studies usually all 18 scales were used, on average 12 scales were used in studies performed in Western Europe. No differences were observed according to study designs (P = 0.78).

Number of scales used a per region where the study was performed and b per study design applied. Note displayed are the medians and quartiles. The H&N35 consists of 18 scales
One study group had developed an alternative head and neck module (EORTC QLQ-H&N17) for surgically treated patients [25].
Discussion
This review describes the use of the EORTC module for the measurement of quality of life in head and neck cancer patients, the H&N35. Major objectives were to find out in what languages it has been used and validated, what psychometric properties in the different language versions have been reported, and how well accepted the module is by patients and investigators.
Based on the 136 papers identified and assessed as part of this evaluation, we can conclude that the H&N35 is used by many investigators throughout the world. As many authors investigated or commented on methodological issues of the H&N35, this information could be collated.
Use of the H&N35 in 26 countries and 19 languages to date indicates broad cross-cultural acceptance. It is, however, interesting to note that it had been translated into 53 languages altogether, leaving 34 translations “unused”. Presumably, these translations were requested for trials performed by pharmaceutical companies without publication in academic journals. Most publications came from Western and Northern European Countries and Asia. Although many studies investigating quality of life in head and neck cancer patients are performed in Northern America [26, 27], relatively few have used the H&N35. This can be explained by the fact that, traditionally, Northern American studies make more use of other well-validated instruments such as the Functional Assessment of Cancer Therapy–Head Neck scale [28–31], the University of Washington Quality of Life Questionnaire, or the Performance Status Scales–Head and Neck cancer [32].
Relatively few studies have reported on construct validity. Those that did mainly confirmed the proposed scale structure, though some concerns have been expressed regarding the high interscale correlation, indicating overlapping constructs. Similarly, some authors computed total scores although this was not intended by the developers of the H&N35. Reliability was mainly evaluated using the concept of internal consistency which was satisfactory overall. The only scale with a median Cronbach’s alpha beneath the threshold of 0.70 was Senses. Reasons for this moderate internal consistency may be that smell and taste are different functions, and patients may have problems with the one without difficulties in the other domain. Moderate internal consistency of this scale was found in different languages and study populations; therefore, the two items should perhaps better be handled separately.
All other scales exhibited good to very good consistency coefficients with Sexuality having the highest scores in all but one language. Sensitivity to change was not frequently explicitly investigated, though the H&N35 was used in many prospective studies and changes over time were observed, providing indirect evidence for sensitivity to change. However, explicit investigation of sensitivity to change would be desirable.
Although the H&N35 is relatively long compared to other EORTC quality of life modules, it proved to be well accepted by patients. The reported frequency of missing values was generally low. Only areas where patients might feel that this domain is not applicable to them, for example, problems with teeth when they have dentures, were left out more frequently. Good acceptance of the H&N35 was also found by other authors who compared different QoL measures in head and neck cancer patients [3, 4, 33].
The acceptance by investigators was also high, considering the number of studies using this instrument, although the entire H&N35 was not always used. Items where only a yes/no response format is provided were frequently either not administered to the patients or not reported by the authors. We can only speculate about the reasons for this. One option is that investigators feel that the psychometric properties of Likert scaled response formats are better. Another explanation would be that issues such as weight gain, use of analgesics or feeding tube are considered to be more reliably measured with objective measures instead of patient reported.
In conclusion, the H&N35 is used by many investigators throughout the world. Some methodological problems (e. g. low internal consistency of some multi-item scales, at times poor compliance of investigators with no/yes scales) have been reported and could be solved, for example, by exchanging problematic items. Although the H&N35 was initially developed for clinical trials, it has been used mainly in observational studies and proved well accepted and feasible in that setting. It has also successfully been implemented in clinical practice [34, 35].
In general, we believe that systematic methodological reviews of frequently used instruments can help to improve existing measures and increase our knowledge on how to develop and improve questionnaires that are psychometrically sound and well accepted by patients and clinicians alike. In addition, it could be useful to collect the raw data of all studies in a central data base, so that direct comparisons between different languages and cultures are possible. This has been done with the EORTC QLQ-C30 [36], but not with the EORTC modules. We recommend that it would be worthwhile to undertake such a task.
References
Björdal, K., Ahlner-Elmqvist, M., Tollesson, E., Jensen, A. B., Razavi, D., Maher, E. J., et al. (1994). Development of an European Organization for Research and Treatment of Cancer (EORTC) questionnaire module to be used in quality of life assessments in head and neck cancer patients. EORTC Quality of Life Study Group, Acta Oncol, 33, 879–885.
Björdal, K., & de Graeff, A. (2000). A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. European Journal of Cancer, 36, 1796–1807.
Mehanna, H. M., & Morton, R. P. (2006). Patients’ views on the utility of quality of life questionnaires in head and neck cancer: a randomised trial. Clinical Otolaryngology, 31, 310–316.
Tschiesner, U., Rogers, S. N., Harreus, U., Berghaus, A., & Cieza, A. (2008). Content comparison of quality of life questionnaires used in head and neck cancer based on the international classification of functioning, disability and health: a systematic review. [Review]. European Archives of Oto-Rhino-Laryngology, 265, 627–637.
Jensen, K., Jensen, A. B., & Grau, C. (2007). Smoking has a negative impact upon health related quality of life after treatment for head and neck cancer. Oral Oncology, 43, 187–192.
Bjordal, K., Hammerlid, E., Ahlner-Elmqvist, M., de Graeff, A., Boysen, M., Evensen, J. F., et al. (1999). Quality of life in head and neck cancer patients: validation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-H&N35. Journal of Clinical Oncology, 17, 1008–1019.
Singer, S., Wollbrück, D., Wulke, C., Dietz, A., Klemm, E., Oeken, J., et al. (2009). Validation of the EORTC QLQ-C30 and EORTC QLQ-H&N35 in Laryngeal Cancer Patients after Surgery. Head and Neck, 31, 64–76.
Zotti, P., Lugli, D., Vaccher, E., Vidotto, G., Franchin, G., & Barzan, L. (2000). The EORTC quality of life questionnaire-head and neck 35 in Italian laryngectomized patients. European organization for research and treatment of cancer, Quality of Life Research, 9, 1147–1153.
Silveira, A. P., Goncalves, J., Sequeira, T., Ribeiro, C., Lopes, C., & Monteiro, E et al. (2010). Patient reported outcomes in head and neck cancer: selecting instruments for quality of life integration in clinical protocols. Head & Neck Oncology 2.
Aarstad, A. K., Aarstad, H. J., & Olofsson, J. (2008). Personality and choice of coping predict quality of life in head and neck cancer patients during follow-up. Acta Oncologica, 47, 879–890.
Sherman, A. C., Simonton, S., Adams, D. C., Vural, E., Owens, B., & Hanna, E. (2000). Assessing quality of life in patients with head and neck cancer: cross-validation of the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Head and Neck module (QLQ-H&N35). Archives of Otolaryngology: Head & Neck Surgery, 126, 459–467.
Arraras, J. I., Arias, F., Tejedor, M., Vera, R., Pruja, E., Marcos, M., et al. (2001). El cuestionario de Calidad de Vida para tumores de cabeza y cuello de la EORTC QLQ-H&N35. Estudio de validacion para nuestro pais. Oncologia, 24, 482–491.
Risberg-Berlin, B., Moller, R. Y., & Finizia, C. (2007). Effectiveness of olfactory rehabilitation with the nasal airflow-inducing maneuver after total laryngectomy: One-year follow-up study. Archives of Otolaryngology: Head & Neck Surgery, 133, 650–654.
Bindewald, J., Oeken, J., Wollbrueck, D., Wulke, C., Dietz, A., Herrmann, E., et al. (2007). Quality of life correlates after surgery for laryngeal carcinoma. Laryngoscope, 117, 1770–1776.
Toth, G., Sakaguchi, T., Mikami, Y., Hirose, H., & Tsukuda, M. (2005). A pilot study of the translation, cultural adaptation and validation of the EORTC head and neck cancer quality of life questionnaire module (QLQ-H&N35) for use in Japan. Auris, Nasus, Larynx, 32, 175–183.
Jayasekara, H., Rajapaksa, L. C., & Aaronson, N. K. (2009). Health-related quality-of-life in patients with head-and-neck cancer in Sri Lanka: psychometric properties of the ‘Sinhala’ version of the EORTC QLQ-H&N35. Psycho-Oncology, 18, 1116–1121.
Jensen, K., Jensen, A. B., & Grau, C. (2006). A cross sectional quality of life study of 116 recurrence free head and neck cancer patients. The first use of EORTC H&N35 in Danish. Acta Oncologica, 45, 28–37.
Aarstad, H. J., Aarstad, A. K., Lybak, S., Monge, O., Haugen, D. F., & Olofsson, J. (2006). The amount of treatment versus quality of life in patients formerly treated for head and neck squamous cell carcinomas. European Archives of Oto-Rhino-Laryngology, 263, 9–15.
Smadja, M., Tessier, C., Menard, M., Brasnu, D., & Crevier-Buchman, L. (2005). Evaluation of the handicap by means of the EORTC scale in partial glossectomies]. [French. Revue de Laryngologie Otologie Rhinologie, 126, 315–322.
Starska, K., Ciechomska, E. A., & Lukomski, M. (2003). Quality of life in patients with laryngeal carcinoma after radical neck dissection]. [Polish. Otolaryngologia Polska, 57, 667–673.
Jensen, K., Lambertsen, K., Torkov, P., Dahl, M., Jensen, A. B., & Grau, C. (2007). Patient assessed symptoms are poor predictors of objective findings. Results from a cross sectional study in patients treated with radiotherapy for pharyngeal cancer, Acta Oncologica, 46, 1159–1168.
Harding, S. A., Hodder, S. C., Courtney, D. J., & Bryson, P. J. (2008). Impact of perioperative hyperbaric oxygen therapy on the quality of life of maxillofacial patients who undergo surgery in irradiated fields. International Journal of Oral and Maxillofacial Surgery, 37, 617–624.
Low, C., Fullarton, M., Parkinson, E., O’Brien, K., Jackson, S. R., Lowe, D., et al. (2009). Issues of intimacy and sexual dysfunction following major head and neck cancer treatment. Oral Oncology, 45, 898–903.
Singer, S., Danker, H., Dietz, A., Kienast, U., Pabst, F., Meister, E. F., et al. (2008). Sexual problems after total or partial laryngectomy. Laryngoscope, 118, 2218–2224.
Maune, S., Bosse, F., Heissenberg, M. C., Schmidt, C., Berens, M., & Kuchler, T. (2002). A concept for the assessment of quality of life in patients with carcinomas of the upper aerodigestive tract. HNO, 50, 347–353.
Rieger, J. M., Zalmanowitz, J. G., & Wolfaardt, J. F. (2006). Functional outcomes after organ preservation treatment in head and neck cancer: a critical review of the literature. International Journal of Oral and Maxillofacial Surgery, 35, 581–587.
Schwartz, S., Patrick, D. L., & Yueh, B. (2001). Quality-of-life outcomes in the evaluation of head and neck cancer treatments. Archives of Otolaryngology: Head and Neck Surgery, 127, 673–678.
Campbell, B. H., Spinelli, K., Marbella, A. M., Myers, K. B., Kuhn, J. C., & Layde, P. M. (2004). Aspiration, weight loss, and quality of life in head and neck cancer survivors. Archives of Otolaryngology: Head and Neck Surgery, 130, 1100–1103.
Ringash, J., Bezjak, A., O’Sullivan, B., & Redelmeier, D. A. (2004). Interpreting differences in quality of life: the FACT-H&N in laryngeal cancer patients. Quality of Life Research, 13, 725–733.
Rogers, L. Q., Courneya, K. S., Robbins, K. T., Malone, J., Seiz, A., Koch, L., et al. (2006). Physical activity and quality of life in head and neck cancer survivors. Supportive Care in Cancer, 14, 1012–1019.
Trivedi, N. P., Swaminathan, D. K., Thankappan, K., Chatni, S., Kuriakose, M. A., & Iyer, S. (2008). Comparison of quality of life in advanced laryngeal cancer patients after concurrent chemoradiotherapy vs total laryngectomy. Otolaryngology-Head and Neck Surgery, 139, 702–707.
List, M. A., Ritter-Sterr, C. A., Baker, T. M., Colangelo, L. A., Matz, G., Pauloski, B. R., et al. (1996). Longitudinal assessment of quality of life in laryngeal cancer patients. Head and Neck, 18, 1–10.
Fisher, S. E., Vikram, A., Donnelly, A., Newsham, A. C., & Johnston, C. (2009). Which questionnaire? Assessing the health related quality of life in patients with head and neck cancer. Oral Oncology, 3, 61.
de Bree, R., Verdonck-de, L. I. M., Keizer, A. L., Houffelaar, A., & Leemans, C. R. (2008). Touch screen computer-assisted health-related quality of life and distress data collection in head and neck cancer patients. Clinical Otolaryngology, 33, 138–142.
Goncalves, J. J., & Rocha, A. M. (2012). A decision support system for quality of life in head and neck oncology patients. Head & Neck Oncology 4.
Scott, N. W., Fayers, P. M., Aaronson, N. K., Bottomley, A., De Graeff, A., Groenvold, M., et al. (2009). Differential item functioning (DIF) in the EORTC QLQ-C30: A comparison of baseline, on-treatment and off-treatment data. Quality of Life Research, 18, 381–388.
Chie, W. C., Hong, R. L., Lai, C. C., Ting, L. L., & Hsu, M. M. (2003). Quality of life in patients of nasopharyngeal carcinoma: validation of the Taiwan Chinese version of the EORTC QLQ-C30 and the EORTC QLQ-H&N35. Quality of Life Research, 12, 93–98.
Ng, R. W. M., & Wei, W. I. (2006). Quality of life of patients with recurrent nasopharyngeal carcinoma treated with nasopharyngectomy using the maxillary swing approach. Archives of Otolaryngology-Head & Neck Surgery, 132, 309–316.
Bower, W. F., Vlantis, A. C., Chung, T. M. L., Cheung, S. K. C., Bjordal, K., & Van Hasselt, C. A. (2009). Quality of life in head and neck cancer patients after surgical resection: translation into Cantonese and validation of the EORTC QLQ-H&N35. Acta Oto-Laryngologica, 129, 779–785.
Nalbadian, M., Nikolaidis, V., Nikolaou, A., Themelis, C., Kouloulas, A., & Vital, V. (2010). Psychometric properties of the EORTC head and neck-specific quality of life questionnaire in disease-free Greek patients with cancer of pharynx and larynx. Quality of Life Research, 19, 761–768.
Lue, B. H., Huang, T. S., & Chen, H. J. (2008). Physical distress, emotional status, and quality of life in patients with nasopharyngeal cancer complicated by post-radiotherapy endocrinopathy. International Journal of Radiation Oncology Biology Physics, 70, 28–34.
Aarstad, A. K., Aarstad, H. J., & Olofsson, J. (2007). Quality of life, drinking to cope, alcohol consumption and smoking in successfully treated HNSCC patients. Acta Oto-Laryngologica, 127, 1091–1098.
Aarstad, A. K. H., Beisland, E., Osthus, A. A., & Aarstad, H. J. (2011). Distress, quality of life, neuroticism and psychological coping are related in head and neck cancer patients during follow-up. Acta Oncologica, 50, 390–398.
Rogers, S. N., Lowe, D., Brown, J. S., & Vaughan, E. D. (1998). A comparison between the University of Washington Head and Neck Disease-Specific measure and the Medical Short Form 36, EORTC QOQ-C33 and EORTC Head and Neck 35. Oral Oncology, 34, 361–372.
Bjordal, K., de Graeff, A., Fayers, P. M., Hammerlid, E., van Pottelsberghe, C., Curran, D., et al. (2000). A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group, European Journal of Cancer, 36, 1796–1807.
Rinkel, R. N., Leeuw, I. M., van Reij, E. J., Aaronson, N. K., & Leemans, C. R. (2008). Speech Handicap Index in patients with oral and pharyngeal cancer: better understanding of patients’ complaints. Head and Neck, 30, 868–874.
Infante-Cossio, P., Torres-Carranza, E., Cayuela, A., Hens-Aumente, E., Pastor-Gaitan, P., & Gutierrez-Perez, J. L. (2009). Impact of treatment on quality of life for oral and oropharyngeal carcinoma. International Journal of Oral and Maxillofacial Surgery, 38, 1052–1058.
Keereweer, S., de Wilt, J. H. W., Sewnaik, A., Meeuwis, C. A., Tilanus, H. W., & Kerrebijn, J. D. F. (2010). Early and long-term morbidity after total laryngopharyngectomy. European Archives of Oto-Rhino-Laryngology, 267, 1437–1444.
Lee, H. F., & Liu, H. E. (2010). Prospective changes of the quality of life for patients newly diagnosed with oral cancer during the acute stage. European Journal of Oncology Nursing, 14, 310–315.
Schiefke, F., Akdemir, M., Weber, A., Akdemir, D., Singer, S., & Frerich, B. (2009). FUNCTION. Postoperative morbidity, and quality of life after cervical sentinel node biopsy and after selective neck dissection, head and neck-journal for the sciences and specialties of the head and neck, 31, 503–512.
van den Berg, M. G. A., Rasmussen-Conrad, E. L., van Nispen, L., van Binsbergen, J. J., & Merkx, M. A. W. (2008). A prospective study on malnutrition and quality of life in patients with head and neck cancer. Oral Oncology, 44, 830–837.
Yoshimura, R., Shibuya, H., Miura, M., Watanabe, H., Ayukawa, F., Hayashi, K., et al. (2009). Quality of life of oral cancer patients after low-dose-rate interstitial brachytherapy. International Journal of Radiation Oncology Biology Physics, 73, 772–778.
Arraras, J. I., de la Vega, F., Manterola, A., Vera, G., Martinez, M., Salgado, E., et al. (2005). Quality of life in patients with locally advanced head and neck cancer treated with chemoradiotherapy. Comparison of two protocols using the EORTC questionnaires (QLQ-C30, H&N35). Clinical and Translational Oncology, 7, 398–403.
van Herpen, C. M. L., Mauer, M. E., Mesia, R., Degardin, M., Jelic, S., Coens, C., et al. (2010). Short-term health-related quality of life and symptom control with docetaxel, cisplatin, 5-fluorouracil and cisplatin (TPF), 5-fluorouracil (PF) for induction in unresectable locoregionally advanced head and neck cancer patients (EORTC 24971/TAX 323). British Journal of Cancer, 103, 1173–1181.
Aplak, B., Malkoc, M., Gelecek, N., & Sen, M. (2007). Quality of life of Turkish patients with head and neck cancer. Turkish Journal of Cancer, 37, 129–136.
Baumann, I., Seibolt, M., Zalaman, I., Dietz, K., Maassen, M., & Plinkert, P. (2006). Quality of life in patients with oropharyngeal carcinoma after primary surgery and postoperative irradiation. Journal of Otolaryngology, 35, 332–337.
Beutner, D., Wittekindt, C., Dinh, S., Huttenbrink, K. B., & Guntinas-Lichius, O. (2006). Impact of lateral parotidectomy for benign tumors on quality of life. Acta Oto-Laryngologica, 126, 1091–1095.
Braz, D. S., Ribas, M. M., Dedivitis, R. A., Nishimoto, I. N., & Barros, A. P. (2005). Quality of life and depression in patients undergoing total and partial laryngectomy. Clinics (Sao Paulo, Brazil) 60:135–142.
Breil, L., Crepin, H., Smadja, M., & Crevier-Buchman, L. (2006). Quality of life after oropharyngectomy. Revue de Laryngologie Otologie Rhinologie, 127, 305–314.
Guntinas-Lichius, O., Appenrodt, S., Veelken, F., & Krug, B. (2006). Phase II study of weekly docetaxel and cisplatin in patients with advanced recurrent and metastatic head and neck cancer. Laryngoscope, 116, 613–618.
Guntinas-Lichius, O., Straesser, A., & Streppel, M. (2007). Quality of life after facial nerve repair. Laryngoscope, 117, 421–426.
Guntinas-Lichius, O., Ruhlow, S., Veelken, F., & Klussmann, J. P. (2009). Quality of life during first-line palliative chemotherapy for recurrent and metastatic head and neck cancer with weekly cisplatin and docetaxel. Journal of Cancer Research and Clinical Oncology, 135, 901–908.
Hanna, E., Sherman, A., Cash, D., Adams, D., Vural, E., Fan, C. Y., et al. (2004). Quality of life for patients following total laryngectomy vs chemoradiation for laryngeal preservation. Archives of Otolaryngology: Head & Neck Surgery, 130, 875–879.
Jensen, K., Bonde, J. A., & Grau, C. (2006). The relationship between observer-based toxicity scoring and patient assessed symptom severity after treatment for head and neck cancer. A correlative cross sectional study of the DAHANCA toxicity scoring system and the EORTC quality of life questionnaires, Radiotherapy & Oncology, 78, 298–305.
McMillan, A. S., Pow, E. H., Kwong, D. L., Wong, M. C., Sham, J. S., Leung, L. H., et al. (2006). Preservation of quality of life after intensity-modulated radiotherapy for early-stage nasopharyngeal carcinoma: results of a prospective longitudinal study. Head and Neck, 28, 712–722.
Müller, R., Paneff, J., Köllner, V., & Koch, R. (2001). Quality of life of patients with laryngeal carcinoma: a post-treatment study. European Archives of Oto-Rhino-Laryngology, 258, 276–280.
Nijdam, W. M., Levendag, P. C., Noever, I., Schmitz, P. I., & Uyl-de Groot, C. A. (2008). Longitudinal changes in quality of life and costs in long-term survivors of tumors of the oropharynx treated with brachytherapy or surgery. Brachytherapy, 7, 343–350.
Op de Coul, B. M., Ackerstaff, A. H., van As, C. J., van den Hoogen, F. J., Meeuwis, C. A., Manni, J. J., et al. (2005). Quality of life assessment in laryngectomized individuals: do we need additions to standard questionnaires in specific clinical research projects? Clinical Otolaryngology, 30, 169–175.
Pow, E. H., Kwong, D. L., McMillan, A. S., Wong, M. C., Sham, J. S., Leung, L. H., et al. (2006). Xerostomia and quality of life after intensity-modulated radiotherapy vs. conventional radiotherapy for early-stage nasopharyngeal carcinoma: initial report on a randomized controlled clinical trial. International Journal of Radiation Oncology Biology Physics, 66, 981–991.
Rogers, S. N., Hannah, L., Lowe, D., & Magennis, P. (1999). Quality of life 5–10 years after primary surgery for oral and oro-pharyngeal cancer. Journal of Cranio-Maxillo-Facial Surgery, 27, 187–191.
Shepherd, K. L., & Fisher, S. E. (2004). Prospective evaluation of quality of life in patients with oral and oropharyngeal cancer: from diagnosis to three months post-treatment. Oral Oncology, 40, 751–757.
Silveira, A. P., Goncalves, J., Sequeira, T., Ribeiro, C., Lopes, C., & Monteiro, E et al. (2011). Geriatric oncology: comparing health related quality of life in head and neck cancer patients. Head & Neck Oncology 3.
Stoeckli, S. J., Guidicelli, M., Schneider, A., Huber, A., & Schmid, S. (2001). Quality of life after treatment for early laryngeal carcinoma. European Archives of Oto-Rhino-Laryngology, 258, 96–99.
Tschudi, D., Stoeckli, S., & Schmid, S. (2003). Quality of life after different treatment modalities for carcinoma of the oropharynx. Laryngoscope, 113, 1949–1954.
Wojtowicz, J. G., Wierzbicka, M., & Szyfter, W. (2001). Zastosowanie ankiety EORTC QLQ C-30 oraz EORTC QLQ H&N35 w okres′laniu jakos′ci zycia przed rozpoczeciem leczenia chirurgicznego u chorych z rozpoznana choroba nowotworowa w obrebie glowy i szyi. [Usefulness of questionnaire EORTC QLQ C-30 and EORTC QLQ H&N C-35 in assessment of quality of life before surgical treatment in patients with head and neck cancer]. Otolaryngologia polska The Polish otolaryngology, 55, 627–634.
Zwahlen, R. A., Dannemann, C., Gratz, K. W., Studer, G., Zwahlen, D., Moergeli, H., et al. (2008). Quality of life and psychiatric morbidity in patients successfully treated for oral cavity squamous cell cancer and their wives. Journal of Oral and Maxillofacial Surgery, 66, 1125–1132.
Salas, S., Baumstarck-Barrau, K., Alfonsi, M., Digue, L., Bagarry, D., Feham, N., et al. (2009). Impact of the prophylactic gastrostomy for unresectable squamous cell head and neck carcinomas treated with radio-chemotherapy on quality of life: Prospective randomized trial. Radiotherapy and Oncology, 93, 503–509.
Al Nawas, B., Al Nawas, K., Kunkel, M., & Grotz, K. A. (2006). Quantifying radioxerostomia: salivary flow rate, examiner’s score, and quality of life questionnaire. Strahlentherapie und Onkologie, 182, 336–341.
Bjordal, K., Ahlner-Elmqvist, M., Hammerlid, E., Boysen, M., Evensen, J. F., Biorklund, A., et al. (2001). A Prospective Study of Quality of Life in Head and Neck Cancer Patients. Part II: Longitudinal Data, Laryngoscope, 111, 1440–1452.
Ciuman, R., Mohr, C., Kroger, K., & Dost, P. (2007). The forearm flap: assessment of functional and aesthetic outcomes and quality of life. American Journal of Otolaryngology, 28, 367–374.
Finizia, C., Hammerlid, E., Westin, T., & Lindstrom, J. (1998). Quality of life and voice in patients with laryngeal carcinoma: a posttreatment comparison of laryngectomy (salvage surgery) versus radiotherapy. Laryngoscope, 108, 1566–1573.
Hammerlid, E., Bjordal, K., Ahlner-Elmqvist, M., Boysen, M., Evensen, J. F., Biorklund, A., et al. (2001). A prospective study of quality of life in head and neck cancer patients. Part I: at diagnosis, Laryngoscope, 111, 669–680.
Infante-Cossio, P., Torres-Carranza, E., Cayuela, A., Gutierrez-Perez, J. L., & Gili-Miner, M. (2009). Quality of life in patients with oral and oropharyngeal cancer. International Journal of Oral and Maxillofacial Surgery, 38, 250–255.
Verdonck-de Leeuw, I. M., van Bleek, W. J., Leemans, C. R., & de Bree, R. (2010). Employment and return to work in head and neck cancer survivors. Oral Oncology, 46, 56–60.
Bahannan, A. A., Zabrodsky, M., Cerny, L., Chovanec, M., & Lohynska, R. (2007). Quality of life following endoscopic resection or radio-therapy for early glottic cancer. Saudi Medical Journal, 28, 598–602.
Borggreven, P. A., Aaronson, N. K., Verdonck-de Leeuw, I. M., Muller, M. J., Heiligers, M. L., Bree, R., et al. (2007). Quality of life after surgical treatment for oral and oropharyngeal cancer: a prospective longitudinal assessment of patients reconstructed by a microvascular flap. Oral Oncology, 43, 1034–1042.
Roh, J. L., Kim, D. H., Kim, S. Y., & Park, C. I. (2007). Quality of life and voice in patients after laser cordectomy for Tis and T1 glottic carcinomas. Head and Neck, 29, 1010–1016.
Alicikus, Z. A., Akman, F., Ataman, O. U., Dag, N., Orcin, E., Bakis, B., et al. (2009). Importance of patient, tumour and treatment related factors on quality of life in head and neck cancer patients after definitive treatment. European Archives of Oto-Rhino-Laryngology, 266, 1461–1468.
Huang, T. L., Tsai, W. L., Chien, C. Y., Lee, T. F., & Fang, F. M. (2010). Quality of life for head and neck cancer patients treated by combined modality therapy: the therapeutic benefit of technological advances in radiotherapy. Quality of Life Research, 19, 1243–1254.
Verdonck-de Leeuw, I. M., de Bree, R., Keizer, A. L., Houffelaar, T., Cuijpers, P., van der Linden, M. H., et al. (2009). Computerized prospective screening for high levels of emotional distress in head and neck cancer patients and referral rate to psychosocial care. Oral Oncology, 45, E129–E133.
Leung, S. W., Lee, T. F., Chien, C. Y., Chao, P. J., Tsai, W. L., & Fang, F. M. (2011). Health-related Quality of life in 640 head and neck cancer survivors after radiotherapy using EORTC QLQ-C30 and QLQ-H&N35 questionnaires. BMC Cancer 11. doi:10.1186/1471-2407-11-128
Lundstrom, E., Hammarberg, B., & Munck-Wikland, E. (2009). Voice Handicap and Health-Related Quality of Life in Laryngectomees: Assessments with the Use of VHI and EORTC Questionnaires. Folia Phoniatrica et Logopaedica, 61, 83–92.
Oates, J., Clark, J. R., Read, J., Reeves, N., Gao, K., & O’Brien, C. J. (2008). Integration of prospective quality of life and nutritional assessment as routine components of multidisciplinary care of patients with head and neck cancer. Anz Journal of Surgery, 78, 34–41.
Abendstein, H., Nordgren, M., Boysen, M., Jannert, M., Silander, E. M., Ahlner-Elmqvist, M., et al. (2005). Quality of Life and Head and Neck Cancer: A 5 Year Prospective Study. Laryngoscope, 115, 2183–2192.
Allison, P. J. (2002). Alcohol consumption is associated with improved health-related quality of life in head and neck cancer patients. Oral Oncology, 38, 81–86.
Bozec, A., Poissonnet, G., Converset, S., Lattes, L., Chamorey, E., Demard, F., et al. (2007). Head and neck reconstructive surgery with free flaps and quality of life: a prospective study. Revue de Laryngologie Otologie Rhinologie, 128, 11–18.
de Graeff, A., de Leeuw, J. R., Ros, W. J., Hordijk, G. J., Blijham, G. H., & Winnubst, J. A. (2001). Sociodemographic factors and quality of life as prognostic indicators in head and neck cancer. European Journal of Cancer, 37, 332–339.
Evensen, J. F., Bjordal, K., Knutsen, B. H., Olsen, D. R., Store, G., & Tausjo, J. E. (2002). Side effects and quality of life after inadvertent radiation overdosage in brachytherapy of head-and-neck cancer. International Journal of Radiation Oncology Biology Physics, 52, 944–952.
Fang, F. M., Chien, C. Y., Kuo, S. C., Chiu, H. C., & Wang, C. J. (2004). Changes in quality of life of head-and-neck cancer patients following postoperative radiotherapy. Acta Oncologica, 43, 571–578.
Fang, F. M., Liu, Y. T., Tang, Y., Wang, C. J., & Ko, S. F. (2004). Quality of life as a survival predictor for patients with advanced head and neck carcinoma treated with radiotherapy. Cancer, 100, 425–432.
Fang, F. M., Chien, C. Y., Tsai, W. L., Chen, H. C., Hsu, H. C., Lui, C. C., et al. (2008). Quality of life and survival outcome for patients with nasopharyngeal carcinoma receiving three-dimensional conformal radiotherapy vs. intensity-modulated radiotherapy-a longitudinal study. International Journal of Radiation Oncology Biology Physics, 72, 356–364.
Fang, F. M., Tsai, W. L., Chien, C. Y., Chiu, H. C., Wang, C. J., Chen, H. C., et al. (2005). Changing quality of life in patients with advanced head and neck cancer after primary radiotherapy or chemoradiation. Oncology, 68, 405–413.
Hammerlid, E., Silander, E., Hornestam, L., & Sullivan, M. (2001). Health-related quality of life three years after diagnosis of head and neck cancer–a longitudinal study. Head and Neck, 23, 113–125.
Nordgren, M., Jannert, M., Boysen, M., Ahlner-Elmqvist, M., Silander, E., Bjordal, K., et al. (2006). Health-related quality of life in patients with pharyngeal carcinoma: a five-year follow-up. Head and Neck, 28, 339–349.
Nordgren, M., Hammerlid, E., Bjordal, K., Ahlner-Elmqvist, M., Boysen, M., & Jannert, M. (2008). Quality of life in oral carcinoma: a 5-year prospective study. Head and Neck, 30, 461–470.
Nordgren, M., Abendstein, H., Jannert, M., Boysen, M., Ahlner-Elmqvist, M., Silander, E., et al. (2003). Health-related quality of life five years after diagnosis of laryngeal carcinoma. International Journal of Radiation Oncology Biology Physics, 56, 1333–1343.
Oates, J., Clark, J., Read, J., Reeves, N., Gao, K., Jackson, M., et al. (2007). Prospective Evaluation of Quality of Life and Nutrition before and after Treatment for Nasopharyngeal Carcinoma. Archives of Otolaryngology: Head & Neck Surgery, 133, 533–540.
Öhrn, K. E. O., Sjödèn, P.-O., Wahlin, Y.-B., & Elf, M. (2001). Oral health and quality of life among patients with head and neck cancer or haematological malignancies. Supportive Care in Cancer, 9, 528–538.
Petruson, K. M., Silander, E. M., & Hammerlid, E. B. (2003). Effects of psychosocial intervention on quality of life in patients with head and neck cancer. Head and Neck, 25, 576–584.
Petruson, K. M., Silander, E. M., & Hammerlid, E. B. (2005). Quality of life as predictor of weight loss in patients with head and neck cancer. Head and Neck, 27, 302–310.
Birkhaug, E. J., Aarstad, H. J., Aarstad, A. K., & Olofsson, J. (2002). Relation between mood, social support and the quality of life in patients with laryngectomies. European Archives of Oto-Rhino-Laryngology, 259, 197–204.
Derks, W., de Leeuw, J. R., Hordijk, G. J., & Winnubst, J. A. (2003). Elderly patients with head and neck cancer: short-term effects of surgical treatment on quality of life. Clinical Otolaryngology & Allied Sciences, 28, 399–405.
Finizia, C., Palme, C., & Bergman, B. (2002). A longitudinal study of the Swedish Self-Evaluation of Communication Experiences after Laryngeal Cancer questionnaire in patients treated for laryngeal cancer. Acta Oncologica, 41, 262–268.
Johansson, M., Ryden, A., & Finizia, C. (2008). Self evaluation of communication experiences after laryngeal cancer: A longitudinal questionnaire study in patients with laryngeal cancer. BMC Cancer, 8, 80.
Schliephake, H., & Jamil, M. U. (2002). Prospective evaluation of quality of life after oncologic surgery for oral cancer. International Journal of Oral and Maxillofacial Surgery, 31, 427–433.
Schliephake, H., & Jamil, M. U. (2002). Impact of intraoral soft-tissue reconstruction on the development of quality of life after ablative surgery in patients with oral cancer. Plastic and Reconstructive Surgery, 109, 421–430.
Hammerlid, E., & Taft, C. (2001). Health-related quality of life in long-term head and neck cancer survivors: a comparison with general population norms. British Journal of Cancer, 84, 149–156.
Ackerstaff, A. H., Balm, A., Rasch, C., de Boer, J., Wiggenraad, R., Rietveld, D., et al. (2009). First-year quality of life assessment of an intra-arterial (radplat) versus intravenous chemoradiation phase III trial. Head and Neck, 31, 77–84.
Pourel, N., Peiffert, D., Lartigau, E., Desandes, E., Luporsi, E., & Conroy, T. (2002). Quality of life in long-term survivors of oropharynx carcinoma. International Journal of Radiation Oncology Biology Physics, 54, 742–751.
Curran, D., Giralt, J., Harari, P., Ang, K., Cohen, R., Kies, M., et al. (2007). Quality of life in head and neck cancer patients after treatment with high-dose radiotherapy alone or in combination with cetuximab. Journal of Clinical Oncology, 25, 2191–2197.
Jenewein, J., Zwahlen, R. A., Zwahlen, D., Drabe, N., Moergeli, H., & Buchi, S. (2008). Quality of life and dyadic adjustment in oral cancer patients and their female partners. European Journal of Cancer Care, 17, 127–135.
Singer, S., Meyer, A., Kienast, U., Rust, V., Taschner, R., Wulke, C., et al. (2007). Use of adaptive devices by laryngectomees. Rehabilitation, 46, 356–362.
Ho, K. F., Farnell, D. J. J., Routledge, J. A., Burns, M. P., Sykes, A. J., Slevin, N. J., et al. (2010). Comparison of patient-reported late treatment toxicity (LENT-SOMA) with quality of life (EORTC QLQ-C30 and QLQ-H&N35) assessment after head and neck radiotherapy. Radiotherapy and Oncology, 97, 270–275.
Derks, W., de Leeuw, J. R., Hordijk, G. J., & Winnubst, J. A. (2005). Reasons for non-standard treatment in elderly patients with advanced head and neck cancer. European Archives of Oto-Rhino-Laryngology, 262, 21–26.
Gryczynski, M., Pajor, A., Ciechomska, E. A., & Starska, K. (2003). Significance of support groups for patients after total laryngectomy for laryngeal carcinoma]. [Polish. Otolaryngologia Polska, 57, 213–219.
Jellema, A. P., Langendijk, H., Bergenhenegouwen, L., van der Reijden, T. J. K., Leemans, R., Smeele, L., et al. (2001). The efficacy of Xialine in patients with xerostomia resulting from radiotherapy for head and neck cancer: a pilot-study. Radiotherapy and Oncology, 59, 157–160.
Riechelmann, H., Meling, D., Messer, P., Richter, H. P., Rettinger, G., & Antoniadis, G. (2006). Subcranial resection of malignant tumors infiltrating the anterior skull base]. [German. Laryngo- Rhino- Otologie, 85, 426–434.
Roberge, C., Tran, M., Massoud, C., Poiree, B., Duval, N., Damecour, E., et al. (2000). Quality of life and home enteral tube feeding: a French prospective study in patients with head and neck or oesophageal cancer. British Journal of Cancer, 82, 263–269.
van der Schroeff, M. P., Derks, W., Hordijk, G. J., & de Leeuw, R. J. (2007). The effect of age on survival and quality of life in elderly head and neck cancer patients: a long-term prospective study. European Archives of Oto-Rhino-Laryngology, 264, 415–422.
Rhemrev, R., Rakhorst, H. A., Zuidam, J. M., Mureau, M. A., Hovius, S. E., & Hofer, S. O. (2007). Long-term functional outcome and satisfaction after radial forearm free flap reconstructions of intraoral malignancy resections. Journal of Plastic, Reconstructive & Aesthetic Surgery: JPRAS, 60, 588–592.
Olthoff, A., Ewen, A., Wolff, H. A., Hermann, R. M., Vorwerk, H., Hille, A., et al. (2009). Organ Function and Quality of Life after Transoral Laser Microsurgery and Adjuvant Radiotherapy for Locally Advanced Laryngeal Cancer. Strahlentherapie und Onkologie, 185, 303–309.
Baumann, I., Seibolt, M., Zalaman, I. M., Dietz, K., Plinkert, P. K., & Maassen, M. M. (2005). Quality of life in patients with oropharyngeal carcinoma. Gender influences the subjective evaluation. HNO, 54, 376–381.
Harnisch, W., Brosch, S., Schmidt, M., & Hagen, R. (2008). Breathing and voice quality after surgical treatment for bilateral vocal cord paralysis. Archives of Otolaryngology-Head & Neck Surgery, 134, 278–284.
Dirix, P., Abbeel, S., Vanstraelen, B., Hermans, R., & Nuyts, S. (2009). Dysphagia after chemoradiotherapy for head-and-neck squamous cell carcinoma: Dose-effect relationships for the swallowing structures. International Journal of Radiation Oncology Biology Physics, 75, 385–392.
Teguh, D. N., Levendag, P. C., Noever, I., Voet, P., van der Est, H., van Rooij, P., et al. (2009). Early hyperbaric oxygen therapy for reducing radiotherapy side effects: Early results of a randomized trial in oropharyngeal and nasopharyngeal cancer. International Journal of Radiation Oncology Biology Physics, 75, 711–716.
Bindewald, J., Herrmann, E., Dietz, A., Wulke, C., Meister, E. F., Wollbruck, D., et al. (2007). Quality of life and voice intelligibility in laryngeal cancer patients–relevance of the “satisfaction paradox”]. [German. Laryngo- Rhino- Otologie, 86, 426–430.
Teguh, D. N., Levendag, P. C., Sewnaik, A., Hakkesteegt, M. M., Noever, I., Voet, P., et al. (2008). Results of fiberoptic endoscopic evaluation of swallowing vs. radiation dose in the swallowing muscles after radiotherapy of cancer in the oropharynx. Radiotherapy and Oncology, 89, 57–63.
Schneider, A., Guidicelli, M., & Stockli, S. J. (2000). Quality of life after treatment of laryngeal carcinoma: surgery versus radiotherapy]. [German. Schweizerische Medizinische Wochenschrift - Supplementum, 116, 31S–34S.
Beetz, I., Burlage, F. R., Bijl, H. P., Hoegen-Chouvalova, O., Christianen, M. E. M. C., Vissink, A., et al. (2010). The Groningen Radiotherapy-Induced Xerostomia questionnaire: Development and validation of a new questionnaire. Radiotherapy and Oncology, 97, 127–131.
Rinkel, R. N., Verdonck-de Leeuw, I. M., Langendijk, J. A., van Reij, E. J., Aaronson, N. K., & Leemans, C. R. (2009). The psychometric and clinical validity of the SWAL-QOL questionnaire in evaluating swallowing problems experienced by patients with oral and oropharyngeal cancer. Oral Oncology, 45, E67–E71.
Jellema, A. P., Doornaert, P., Slotman, B. J., Leemans, C. R., & Langendijk, J. A. (2005). Does radiation dose to the salivary glands and oral cavity predict patient-rated xerostomia and sticky saliva in head and neck cancer patients treated with curative radiotherapy? Radiotherapy and Oncology, 77, 164–171.
Jellema, A. P., Slotman, B. J., Doornaert, P., Leemans, C. R., & Langendijk, J. A. (2007). Unilateral versus bilateral irradiation in squamous cell head and neck cancer in relation to patient-rated xerostomia and sticky saliva. Radiotherapy and Oncology, 85, 83–89.
Roesink, J. M., Schipper, M., Busschers, W., Raaijmakers, C. P., & Terhaard, C. H. (2005). A comparison of mean parotid gland dose with measures of parotid gland function after radiotherapy for head-and-neck cancer: implications for future trials. International Journal of Radiation Oncology Biology Physics, 63, 1006–1009.
Levendag, P. C., Teguh, D. N., Voet, P., van der Est, H., Noever, I., de Kruijf, W. J., et al. (2007). Dysphagia disorders in patients with cancer of the oropharynx are significantly affected by the radiation therapy dose to the superior and middle constrictor muscle: a dose-effect relationship. Radiotherapy and Oncology, 85, 64–73.
Risberg-Berlin, B., Ylitalo, R., & Finizia, C. (2006). Screening and rehabilitation of olfaction after total laryngectomy in Swedish patients: results from an intervention study using the Nasal Airflow-Inducing Maneuver. Archives of Otolaryngology: Head & Neck Surgery, 132, 301–306.
Teguh, D. N., Levendag, P. C., Noever, I., van Rooij, P., Voet, P., van der Est, H., et al. (2008). Treatment techniques and site considerations regarding dysphagia-related quality of life in cancer of the oropharynx and nasopharynx. International Journal of Radiation Oncology Biology Physics, 72, 1119–1127.
Wittekindt, C., Kassens, G., Bramlage, S., Eckel, H. E., Goldschmidt, O., Schrappe, M., et al. (2002). Qualitätsbewertende Indikatoren in einer HNO-Klinik. HNO, 50(6), 553–559.
Zumtobel, M., End, A., Bigenzahn, W., Klepetko, W., & Schneider, B. (2006). Reduced quality of life in patients with unilateral vocal cord paralysis after thoracic surgery [German]. Chirurg, 77, 518–522.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Singer, S., Arraras, J.I., Chie, WC. et al. Performance of the EORTC questionnaire for the assessment of quality of life in head and neck cancer patients EORTC QLQ-H&N35: a methodological review. Qual Life Res 22, 1927–1941 (2013). https://doi.org/10.1007/s11136-012-0325-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-012-0325-1