
Abstract
Purpose
Using the Wilson–Cleary model of patient outcomes as a conceptual framework, the impact of functional status on health-related quality of life (HRQoL) among older adults was examined, including tests of the mediation provided by life-space mobility.
Methods
Participants were enrollees in a population-based, longitudinal study of mobility among community-dwelling older adults. Data from four waves of the study equally spaced approximately 18 months apart (baseline, 18, 36, and 54 months) were used for participants who survived at least 1 year beyond the 54-month assessment (n = 677). Autoregressive mediation models using longitudinal data and cross-sectional mediation models using baseline data were evaluated and compared using structural equation modeling.
Results
The longitudinal autoregressive models supported the mediating role of life-space mobility and suggested that this effect is larger for the mental component summary score than the physical component summary score of the SF-12. Evidence for a reciprocal relationship over time between functional status, measured by ADL difficulty, and life-space mobility was suggested by modification indices; these model elaborations did not alter the substantive meaning of the mediation effects. Mediated effect estimates from longitudinal autoregressive models were generally larger than those from cross-sectional models, suggesting that mediating relationships would have been missed or were potentially underestimated in cross-sectional models.
Conclusions
These results support a mediating role for life-space mobility in the relationship between functional status and HRQoL. Functional status limitations might cause diminished HRQoL in part by limiting mobility. Mobility limitations may precede functional status limitations in addition to being a consequence thereof.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Measures of mobility in older adults are often used as indicators of health and functioning; yet, the role of mobility in the causal pathways between functional status and health-related quality of life (HRQoL) remains poorly understood. Some studies attempt to understand how demographic, biomedical, psychological, sociological, or environmental variables predict mobility [1, 2], while others have suggested the role of mobility as a predictor of other functional measures [1, 3].
Self-reports of difficulty with activities of daily living (ADLs) are often used to assess functional ability. These classic, clinically relevant indicators reflect what individuals report they are capable of doing. In terms of affecting daily living and quality of life, self-reported functional ability is one important variable that undoubtedly affects mobility, or what individuals actually do [2], which may, in turn, affect standard measures of HRQoL. Indeed, perceived difficulties in performing ADLs have been shown to be related to mobility [1, 2] and mobility has also been shown to be correlated with the physical and mental component summary scores of the SF-12 [1], a commonly used measure of health-related quality of life [4]. However, multivariate conceptual models of functional ability, mobility, and subsequent quality of life are rarely articulated and then evaluated empirically.
Wilson and Cleary [5] developed a theoretical framework to link the biomedical model of health with a quality of life model. Their model focuses on five levels of patient outcomes (i.e., biologic and physiologic variables, symptoms, functioning, general health perceptions, and overall quality of life) and proposes mediating relationships among these variables (e.g., the relationship between symptom status and overall quality of life is mediated by functional status and general health perceptions) in addition to explanatory roles of several personal and environmental variables. Parts of this model have been applied to a variety of patient populations and some have expressly examined the mediated effects implied by the model [6–10].
It is important to note that the Wilson–Cleary model was not intended to completely describe all relationships important to individuals’ health [11]. The model has been adapted, modified, and extended [12–14], and relationships not directly specified in the model have been tested and supported. For example, social support, as an environmental variable in the Wilson–Cleary model, is posited to have direct effects on functional status, general health perceptions, and overall quality of life. However, there is evidence that social support mediates the functional status and quality of life relationship [15]. Others have explicitly examined the mediating role of personal variables proposed to have direct effects in the original Wilson–Cleary model [14]. Given this literature as well as past research suggesting their bivariate relationships [1, 2], an adaptation of the Wilson–Cleary model appears to provide a useful conceptual framework for examining the multivariate relationships among functional status, mobility, and quality of life.
The purpose of this study was to assess whether the relationship between functional status (i.e., ADLs or what individuals report they are capable of doing) and HRQoL is mediated by mobility (i.e., what people actually do in terms of mobility). The general conceptual overview is summarized in Fig. 1. By examining the predictive pathways from functional abilities to HRQoL through mobility over time, this study subjected the testing of this mediation hypothesis to the more rigorous longitudinal analysis methods that are becoming more common to test mediation relationships [16–25]. In the case of true longitudinal mediation, Maxwell and Cole [18] have demonstrated that cross-sectional analyses provide biased estimates of the indirect effect (or mediated effect) in two different models of change, the autoregressive model and a random effects model.

Basic mediation model for the present study. Indirect effect = ab, direct effect = c’, total effect = ab + c’, proportion mediated = ab/(c′ + ab)
Most previous analyses of mediated relationships based on the Wilson–Cleary model have relied on cross-sectional data [6–8]. Some evaluations of the Wilson–Cleary model used longitudinal data, but did not test for mediated effects [26–28] or used only two waves of data [9]. Although with additional assumptions it is possible to provide evidence of mediation with just two waves of data [17], three or more waves of data are usually necessary to subject each leg of the mediated effect to a temporal sequence that would more strongly support a causal interpretation [25, 29].
Methods
Setting and participants
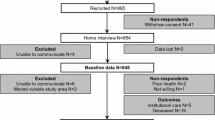
This analysis is based on the data from participants in the University of Alabama at Birmingham (UAB) Study of Aging, a population-based, longitudinal study of mobility among community-dwelling older adults, randomly sampled from a list of Medicare beneficiaries living in one of five counties (two urban and three rural) in central Alabama. African Americans, men, and rural residents were oversampled to provide a balanced sample in terms of race, gender, and rural/urban residence (the study was designed to examine racial differences in mobility among older adults). Individuals in nursing homes and people unable to set their own appointments were excluded. Participants were recruited by mail and followed up by telephone. Trained interviewers conducted baseline in-home interviews between November 1999 and February 2001 with n = 1,000. Follow-up interviews were conducted by telephone. Minimal proxy input for factual questions was available and used for approximately 15 % of the participants [2]. For the primary variables used in the present study, responses did not come from proxy respondents (i.e., they were self-reported). Additional study details can be found elsewhere [2, 30].
For the present study, data from four waves equally spaced approximately 18 months apart (baseline, 18, 36, and 54 months) were analyzed. Participants who did not survive at least one year beyond the 54-month assessment were excluded. Thus, by design, we restricted our analysis to changes over time free of the terminal decline shown to occur in the last year of life on the variables of interest [31]. Of the 1,000 initial participants, 250 died prior to month 54 and 61 died after month 54 but before month 66. An additional 12 participants had no data other than baseline data and were excluded. Thus, 677 participants were used in the present analyses. As expected, compared to excluded individuals, participants in this analysis were younger at baseline, had fewer verified comorbidities, higher life-space mobility scores, less ADL difficulty, and higher HRQoL scores (p < 0.0001 for all comparisons). The original study and the present analysis were approved by the UAB Institutional Review Board, and all participants gave written informed consent.
Measures
Functional status
Physical functional status was measured by self-reported difficulty with ADLs. Participants were asked whether they had difficulty with specific ADLs, and a latent functional status variable was extracted from four dichotomous (yes vs. no) ADL items—transferring, bathing, dressing, and toileting. The factors at each time point were identified by fixing the factor loading of the first ADL (transferring) to be one. Responses to mobility-related ADLs (i.e., using stairs, walking, and getting outside) were also obtained, but these data were excluded from the latent functional status variable due to their conceptual overlap with the LSA. Data on another ADL (eating) were collected but excluded from the analysis because difficulty with this ADL was rarely reported. At some waves, no respondents endorsed this item, constraining the variance and complicating the extraction of a latent functional status variable that included this item at those waves.
Life-space mobility
The UAB Study of Aging Life-Space Assessment (LSA) measures mobility based on the distance each participant reported moving during the 4 weeks preceding the assessment [1, 2, 30, 32]. The instrument assesses mobility in terms of the extent and frequency of movement across five levels (i.e., within one’s home outside the bedroom, areas immediately outside of one’s home, within one’s immediate neighborhood, within one’s town, and outside one’s town), as well as the use of assistance in performing such movements. For each life-space level, participants were asked whether they traveled to that area, how frequently they traveled to that area, and whether they needed help from another person or assistance device to travel to that area. As described previously [1], the life-space composite (LSC) score is calculated by combining life-space level attainment, the frequency of attaining each level, and the degree of independence in achieving each level. Scores ranged from 0 (mobility limited to the room where one sleeps) to 120 (traveled out of town every day without assistance). The two-week follow-up test–retest reliability of the LSC was high (intraclass correlation = 0.96) [1]. This composite score was used as the mobility variable in the analyses. Given its high reliability and its calculation as a composite variable, the observed LSC score was analyzed as the mediator rather than extracting a latent mobility variable. The LSC has been used in this manner in other studies [2, 3, 33].
HRQoL
Version 1 of the SF-12 was used to assess HRQoL. Mental component summary (MCS) and physical component summary (PCS) scores were calculated using procedures described by Ware et al. [4]. These scores are transformed and scaled such that the general US adult population has a population mean of 50 and standard deviation of 10. Test–retest reliabilities of 0.89 and 0.76 have been reported for the SF-12’s PCS and MCS, respectively [4]. Given established, strong measurement properties, and frequent use within the field, MCS and PCS scores were treated as observed variables in all analyses. This is consistent with common practice, and prior research has shown very high correlations with these summary scores and latent variables based on individual items (0.97 for PCS and 0.96 for MCS) [34].
Covariates
The following variables, collected at baseline, were used as covariates in all analyses: sex, race (African American or white), age, recent smoking status (whether the participant smoked in the past year), education, and a verified comorbidity score. Education was divided into year categories: 1 ≤ 6; 2 = 7–11; 3 = 12; 4 ≥ 13.
The Charlson Comorbidity Index reflects the number and severity of comorbidities present in hospitalized patients and depends upon medical record reviews [35]. We used the Charlson comorbidity categories as a guide to calculate a comorbidity score appropriate for community-dwelling older adults. The comorbidity score reflected the number of comorbidities present, but not their severity. The comorbidity score was based on self-reported medical conditions verified either by the use of a prescription medication, physician report, or a hospital discharge diagnosis recorded in the previous 3 years. Verification procedures for these medical conditions have been fully described elsewhere [3, 33].
Verified conditions were put into twelve comorbidity categories based on the work of Charlson et al. [35]. The disease categories included: (1) congestive heart failure; (2) angina pectoris or heart attack; (3) valvular heart disease; (4) peripheral arterial disease; (5) hypertension; (6) diabetes mellitus; (7) chronic obstructive lung disease or asthma; (8) kidney disease; (9) liver disease; (10) cancer other than skin cancer; (11) any neurological disorder including stroke, Parkinson’s disease, seizures, or Alzheimer’s disease; and (12) gastrointestinal disease including stomach, bowel, or digestive problems. The number of verified medical condition categories present was used to calculate the comorbidity score. Thus, the comorbidity score could range from 0 to 12.
Sex, race, and recent smoking status were dichotomous variables while age, education, and comorbidity score were treated as continuous variables in all analyses.
Statistical analysis
Statistical mediation suggests that the causal effect of one variable on another is transmitted through a third variable called a mediator or intervening variable [36]. A variety of statistical methods for assessing mediation have been proposed [37]. The presence of longitudinal data provides additional data analysis options [17, 18, 20, 25], and the present analysis evaluated the proposed mediated effect utilizing an autoregressive approach.
The basic premise of autoregressive models is that the values of variables at future time points depend in part on values at earlier time points. The simplest of these models involves one variable measured at multiple time points for a set of individuals. This basic model (the univariate simplex model [38, 39]) was extended to an autoregressive mediation model [17, 40], involving the variables: X (the independent variable), M (the mediator), and Y (the outcome).
A basic framework for the analysis can be found in Fig. 2. For clarity, only structural paths (i.e., no measurement paths, no residual covariances) for the main variables (i.e., no covariate paths) are included in Fig. 2. A modified set of steps for autoregressive mediation modeling was utilized [17, 20]. Prior to fitting any longitudinal models, a cross-sectional assessment of mediation was evaluated using baseline data. Next, an initial autoregressive mediation model (i.e., Model 1’s) was fit separately for MCS and PCS as outcome variables based on the paths outlined in Fig. 2.Footnote 1 Although measurement invariance over time for the latent functional status variable based on ADLs was not assumed (i.e., factor loadings and thresholds were free to vary over time), these models did include covariates as control variables as well as covariances between residual terms of downstream endogenous variables within the same wave. This last model component is recommended by Anderson and Williams [41] and the presence of significant and meaningful covariation among these residuals implies the possibility of confounding due to variables missing from the model. Failing to specify such covariances may lead to biased estimates [17]. Following this step, a test of measurement invariance over time for the functional status variable was performed by constraining both thresholds and loadings to be equal across waves.

Autoregressive mediation model framework for the present study. Measurement paths (i.e., for functional status), covariate paths, and covariances between residual terms of downstream endogenous variables within the same wave are estimated but have been omitted for simplicity. FS functional status, LSC composite measure of life-space mobility, and MCS and PCS mental component summary score and physical component summary score of the SF-12, respectively
After these autoregressive measurement modeling options were finalized, the indirect effect (or mediated effect) of functional status on HRQoL through life-space mobility was estimated by the product of coefficients method and evaluated for statistical significance using both the Sobel test [42] and a bias-corrected bootstrap confidence interval with 1,000 draws [43]. In addition, the proportion-mediated effect was calculated as a measure of mediation effect size. This measure consists of the ratio of the mediated effect to the total effect and represents the proportion of the total effect that is mediated by the intervening variable [37].
With four waves of data, it is possible to estimate both time-specific indirect effects and the overall (or total) indirect effect [17, 23, 40]. As outlined in Fig. 2, there are three time-specific indirect effects (with the estimate of each indirect effect based on the product of coefficients method):
-
1.
FS1 → FS2 → LSC3 → PCS4 (or MCS4) = x 1 × a 2 × b 3
-
2.
FS1 → LSC2 → LSC3 → PCS4 (or MCS4) = a 1 × m 2 × b 3
-
3.
FS1 → LSC2 → PCS3 (or MCS3) → PCS4 (or MCS4) = a 1 × b 2 × y 3
The overall indirect effect of FS1 → PCS4 (or MCS4) is the sum of these three time-specific indirect effects. This addresses the question of whether LSC mediates the effect of FS1 on PCS4 (or MCS4) at any time between waves 1 and 4 (rather than at some specific point), a question usually of greater interest to researchers [17, 23]. Thus, both time-specific and overall indirect effects were calculated and evaluated for significance.
In addition to the measure of indirect effect, the fit of the models to the data was evaluated using various fit indices including the chi-square goodness-of-fit statistic, the root mean square error of approximation (RMSEA), comparative fit index (CFI), and the weighted root mean square residual (WRMR). Good model fit is indicated by a small chi-square value (this test is quite sensitive to sample size), an RMSEA less than 0.05 [44], a CFI above 0.95 [45], and a WRMR of less than 1.0 [46].
Following the test of the initial mediation models (Model 1’s), the potential for omitted paths was evaluated using modification indices and expected parameter change values. Adjustments evaluated were those that could be justified theoretically, including: (1) covariances between measurement errors for the same ADLs measured at several time points, (2) wave-skipping autoregressive paths (e.g., FS4 predicted by FS3 and FS2), (3) cross-lagged relations (e.g., FS2 predicted by LSC1), (4) autocorrelation residuals (e.g., residual variance of FS3 with the residual variance of FS2), (5) contemporaneous paths (e.g., LSC2 predicted by FS2), and additional direct effects (e.g., PCS4 (or MCS4) predicted by FS2). Effects going backward in time were not considered. Elaborated models (Model 2’s) based on the results of these specification searches were then estimated separately for MCS and PCS. This approach allowed for the inclusion of fit-based model enhancements, some of which might have the potential to alter the size and/or significance of the indirect effect, so the tests of the mediated effects were repeated in the modified models.
All analyses were conducted in Mplus 6.11 (Muthén & Muthén, Los Angeles, CA). To account for the categorical functional status indicators (i.e., ADLs), a robust weighted least squares estimator (i.e., WLSMV) was used [47]. There were 677 complete cases at wave 1, 651 at wave 2, 626 at wave 3, and 611 at wave 4. Rather than listwise deletion (i.e., analyzing only those with complete data at all four waves), the WLSMV estimator in Mplus used the total available sample for analysis. Such estimates are consistent under the assumption of missing at random with respect to covariates (MARX) and more efficient than listwise deletion [48].
Results
Table 1 provides means and standard deviations or frequencies for the main study variables and covariates. In addition, the numbers of cases for each variable at each time point are provided. The functional status variable, as well as the SF-12’s PCS and MCS, demonstrated good internal consistencies.Footnote 2 Cronbach’s alpha for the ADL measure was 0.72, 0.85, 0.87, and 0.92 at waves 1, 2, 3, and 4, respectively. For PCS, Cronbach’s alpha was 0.85, 0.86, 0.88, and 0.90 at waves 1, 2, 3, and 4, respectively. For MCS, Cronbach’s alpha was 0.76, 0.81, 0.83, and 0.84 at waves 1, 2, 3, and 4, respectively. For all models tested, all factor loadings for the latent functional status variable were significantly different from zero (p < 0.0001) and all standardized loadings were greater than 0.75, with most near 0.9.
Because functional status was conceptualized as a latent variable represented by difficulty with multiple ADL items over time, it was possible to assess factorial invariance across waves. Initial models based on Fig. 2 (with separate models for PCS and MCS as outcome variables) were estimated allowing functional status factor loadings and thresholds to freely vary over time and compared to models where thresholds and loadings were constrained to be equal across waves. The WLSMV estimator in Mplus precludes the use of traditional chi-square difference testing to evaluate invariance. Thus, the DIFFTEST option in Mplus was used [49] in which a significant finding indicates a lack of measurement invariance. For both the PCS and MCS models, this test for the lack of invariance was statistically significant (Δχ2 = 37.65, df = 21, p = 0.0142; Δχ2 = 42.21, df = 21, p = 0.004 for PCS and MCS models, respectively). However, for relatively large samples, the test for invariance can be statistically significant (i.e., indicating a lack of invariance) even when there are only minor differences in model parameters [50, 51]. Examination of fit indices that take model parsimony into account indicated that the value of the RMSEA was actually reduced from the unconstrained to the invariant models (0.041 → 0.038 and 0.039 → 0.037, for PCS and MCS models, respectively) and the value of CFI was either increased or remained unchanged (0.981 → 0.982 and 0.983 → 0.983, for PCS and MCS models, respectively) with the addition of invariance constraints. These findings support an interpretation that the deviations from perfect measurement invariance were quite small and of no practical significance.Footnote 3 Thus, all subsequent models were tested using the constrained invariant factor loadings and thresholds over time for the functional status variable.
Results of the longitudinal mediation models with measurement invariance constraints imposed for functional status are summarized in Table 2. The fit indices for Model 1’s based on the framework in Fig. 2 indicated good model fit for both PCS and MCS. For PCS, only one time-specific indirect effect was statistically significant (FS1 → LSC2 → PCS3 → PCS4), but the total indirect effect was statistically significant using both the Sobel test and the bias-corrected bootstrap method (95 % CI: −1.282, −0.062). About 13 % of the total effect of functional status on PCS was mediated through LSC. With MCS as the outcome variable, all three time-specific indirect effects were statistically significant as well as the total indirect effect (using both the Sobel test and the bias-corrected bootstrap method [95 % CI: −1.17, −0.235)]. About 44 % of the total effect of functional status on MCS was mediated by LSC. However, the direct effect of functional status on MCS was only marginally significant (p = 0.051), suggesting the possibility of complete mediation of the functional status and MCS relationship by LSC.
Modification indices were used to suggest additional paths, and these results can be found in Table 2. In addition, completely standardized path coefficients for the original paths as well as the newly added paths can be found in Figs. 3 and 4 for the PCS and MCS models, respectively. Newly added paths consisted of either wave-skipping autoregressive paths (e.g., FS4 predicted by FS2) or cross-lagged relations (e.g., FS2 predicted by LSC1). Modification indices suggested no other paths that would lead to substantial improvements in model fit after these paths were included. Thus, no additional paths were added for covariances between measurement errors for the same ADLs measured at several time points, autocorrelation residuals, contemporaneous paths, or additional direct effects. As expected, model fit improved significantly with the addition of the paths listed in Table 2. More importantly, the significance of the functional status → life-space mobility → HRQoL total indirect effect was maintained for both PCS and MCS. According to the Model 2’s, almost 20 % of the total effect of functional status on PCS was mediated through LSC, while it appears that all of the relationship between functional status and MCS is mediated by LSC (i.e., p = 0.691 for the direct effect of functional status on MCS).

Completely standardized parameter estimates from the final model (i.e., Model 2) with PCS as the outcome variable including fit-based model enhancements. Measurement paths (i.e., for functional status), covariate paths, and covariances between residual terms of downstream endogenous variables within the same wave are estimated but have been omitted for simplicity. Parameter estimates are located above the corresponding path. FS functional status, LSC composite measure of life-space mobility, and MCS and PCS mental component summary score and physical component summary score of the SF-12, respectively

Completely standardized parameter estimates from the final model (i.e., Model 2) with MCS as the outcome variable including fit-based model enhancements. Measurement paths (i.e., for functional status), covariate paths, and covariances between residual terms of downstream endogenous variables within the same wave are estimated but have been omitted for simplicity. Parameter estimates are located above the corresponding path. FS functional status, LSC composite measure of life-space mobility, and MCS and PCS mental component summary score and physical component summary score of the SF-12, respectively
As a basis for comparison to the longitudinal autoregressive models, the mediating role of life-space mobility in the relationship between functional status and HRQoL was evaluated cross-sectionally using baseline data. This cross-sectional analysis was conducted on both the 677 cases used in the longitudinal analysis and the complete sample at baseline (n = 1,000). The latter analysis was conducted because this is the approach that would have been used to evaluate the mediated relationship had no longitudinal data been available. Model fit in all cross-sectional models was acceptable, but the proportion-mediated effects were generally smaller in the cross-sectional models (PCS: about 5 %; MCS: about 21 %) compared to the longitudinal models, and in one case, the mediated effect was not statistically significant (for PCS with the complete sample at baseline—results available upon request).
Discussion
The association between functional status and quality of life in older adults is well established [15, 52, 53]; this study sought to investigate a potential reason for this relationship, namely the role of life-space mobility. Longitudinal analyses supported the predicted mediating role of life-space mobility in the relationship between functional status and HRQoL, a set of relationships adapted from the Wilson–Cleary model of patient outcomes. Results suggest that functional status limitations defined by ADL difficulty predict lower levels of life-space mobility which in turn predicted diminished HRQoL. Given these relationships, interventions designed to maintain or enhance ADL independence with the ultimate goal of preserving or improving quality of life should consider the mediating role of life-space mobility in this relationship. This variable may itself serve as a potential target for intervention or serve to provide greater insight into the functional status and quality of life relationship, thereby providing more information concerning the development and testing of interventions. Others have suggested the usefulness of the addition of life-space mobility measures to standard ADL assessment strategies [32].
The mediating role of life-space mobility appears to be more significant with the SF-12’s MCS as the outcome compared to PCS. The final level of the Wilson–Cleary model, overall quality of life, has been represented by different measures. Some have used HRQoL measures (generic or disease-specific) [8, 54–56], while others have used life satisfaction measures [9, 27] or measures of mental health [6] and psychological distress [7, 14]. The items in the SF-12 most strongly related to PCS are closely related to physical functioning. Höfer and colleagues [54] used the physical functioning scale of the SF-36, which is a large part of PCS scores, as a measure of functional status. Given the conceptual overlap between functional status, life-space mobility, and PCS, it is not surprising that the mediating role of life-space mobility is less significant with PCS relative to MCS. MCS is more consistent with the end level in the Wilson–Cleary model.
Although not tested as an a priori hypothesis, the presence of cross-lagged relationships between functional status and life-space mobility as originally indicated by modification indices and subsequently tested in elaborated models suggests that functional status levels not only influence changes in life-space mobility, but also show effects in response to changes in mobility. This finding is consistent with previous suggestions that mobility limitations may precede difficulties with specific ADL tasks [1], in addition to being an outcome of functional status changes [2]. The potential reciprocal relationship offers additional support for including both traditional methods of functional assessment and life-space mobility measures in a comprehensive assessment strategy for older adults [32]. Other evaluations of the Wilson–Cleary model have examined such reciprocal effects. For example, Mathisen and colleagues [27] note reciprocal causal effects over time between general health perceptions and overall quality of life. Wilson and Cleary [5] note the possibility of such effects, and other researchers have called for an examination of these bidirectional relationships [7, 9]. Further research is required to support the view that the Wilson–Cleary model be modified to explicitly incorporate bidirectional causal effects.
Estimates of mediation effects from autoregressive models were only partially consistent with estimates from cross-sectional analyses. For example, researchers might have concluded that there was no significant mediation of the functional status and PCS relationship using all available cases at baseline. Longitudinal models revealed larger indirect effects as a percentage of total effects when compared to cross-sectional models, even suggesting complete mediation with MCS as the outcome.
To our knowledge, this is the first test of mediated relationships implied by the Wilson–Cleary model to use longitudinal data with three or more waves of data. There are several benefits of using longitudinal rather than cross-sectional data to evaluate mediation processes [20, 25, 40]. First, more information regarding the temporal sequentiality of the independent variable, the mediator, and the outcome variable is provided with longitudinal data, a critical underlying assumption of the causal relationships involved in mediation. Similarly, causal effects often take time to develop, and variables measured at the same time may not allow for the necessary development time. Second, associations between variables in cross-sectional models capture both time-varying and time-invariant covariances between participants, but longitudinal models allow these two sources of covariance to be separated and tested more directly in line with the causal assumptions of the mediation model. Finally, individuals may serve as their own control in assessing some relationships, thereby potentially controlling for static differences among individuals. Variables often have effects on themselves, such that variables at later times are related to the same variable at earlier times. Cross-sectional models implicitly assume these autoregressive effects are zero, and substantial bias can be introduced as a result. Autoregressive effects adjust for these relationships, and accordingly adjust the time-varying associations that are being tested as part of the causal model.
There are several limitations of the present study to consider. Although longitudinal analyses provide advantages over cross-sectional views of mediation, the data analyzed in the present study are still considered observational. Longitudinal structural equation modeling cannot prove causality in these kinds of designs, but it can test whether a proposed causal model is plausible and whether it provides good fit to the observed data. In the present study, 18 months separated each wave. The timing and spacing of measurements can influence the detection and estimation of effects in longitudinal studies [57], and the 18-month interval may not have been optimal to detect more rapidly transmitting causal effects. Missing data are usually problematic in any longitudinal study. It is not surprising that a substantial number of participants did not survive the entire study period. These individuals were excluded as the intent of the study was to examine the mediated effect of interest in a population not experiencing the terminal decline in functional status and mobility that occurs in the last year of life [31]. Different mechanistic models may need to be developed to assess relationships occurring in the period of the terminal drop. A smaller number of individuals failed to complete certain assessments during the study period. We assumed that the missing data mechanism in this data set was missing at random with respect to covariates [48]. For other missing data mechanisms, other approaches such as multiple imputation [58] or pattern-mixture modeling [59] would be more appropriate. Finally, although the model modification through specification searches only considered theoretical plausible paths, it is important to note that such modifications can lead to model misspecifications.
Conclusion
The present longitudinal analysis, based on an autoregressive model, supports the mediating role of life-space mobility and suggests that this role is more significant with the MCS of the SF-12 as the outcome than the PCS. Evidence for a reciprocal relationship over time between functional status and life-space mobility was suggested by the modification indices, which is consistent with other modifications of the Wilson–Cleary model. These elaborations to the model did not alter the substantive meaning of the mediation effects. Several authors have advocated for the use of longitudinal designs when evaluating mediation relationships. The present study provides an example of one approach for testing mediation with longitudinal data.
Notes
Separate models were fit for PCS and MCS primarily for the ease of presentation of results and because each variable was considered a separate end point. It is possible to estimate one complete model containing both PCS and MCS. Given that the PCS and MCS were originally constructed to be orthogonal, there should be little difference in the results based on separate models and results from a single model considering both PCS and MCS. Indeed, when considering the final models reported in the current analysis, there were no substantive differences in findings when comparing separate estimation models for PCS and MCS and a single, combined model.
The nature of the calculation of the LSC score limits the applicability of internal consistency reliability and thus Cronbach’s alpha is not reported for the LSC; as stated earlier, past research reports high levels of test–retest reliability for this measure.
As suggested by one anonymous reviewer, in addition to examining chi-square change and model fit statistics for assessing measurement invariance, one should consider whether any meaningful differences in the estimates of interest occur between models with constrained invariant parameters and those where parameters are freely estimated. In the present study, the mediated effects were highly similar between models with measurement invariance for functional status and those with non-invariance. For example, the total mediated effect estimate for the PCS Model 2 assuming invariant thresholds and loadings (see Table 2) was −0.88 (p < 0.0001); this same effect was −0.90 (p < 0.0001) in a model with non-invariance. An examination of the time-specific indirect effects revealed similar results; p values for these indirect effects differed in the third decimal place, if at all.
References
Baker, P. S., Bodner, E. V., & Allman, R. M. (2003). Measuring life-space mobility in community-dwelling older adults. Journal of the American Geriatrics Society, 51(11), 1610–1614.
Peel, C., Baker, P. S., Roth, D. L., Brown, C. J., Bodner, E. V., & Allman, R. M. (2005). Assessing mobility in older adults: The UAB Study of Aging Life-Space Assessment. Physical Therapy, 85(10), 1008–1019.
Brown, C. J., Roth, D. L., Allman, R. M., Sawyer, P., Ritchie, C. S., & Roseman, J. M. (2009). Trajectories of life-space mobility after hospitalization. Annals of Internal Medicine, 150(6), 372–378.
Ware, J. E., Kosinski, M., & Keller, S. D. (2002). SF-12: How to score the SF-12 physical and mental health summary scales (4th ed.). Lincoln, RI: QualityMetric Incorporated.
Wilson, I. B., & Cleary, P. D. (1995). Linking clinical variables with health-related quality of life: A conceptual model of patient outcomes. JAMA, 273(1), 59–65.
Sousa, K., & Kwok, O. (2006). Putting Wilson and Cleary to the test: Analysis of a HRQOL conceptual model using structural equation modeling. Quality of Life Research, 15(4), 725–737.
Baker, S. R., Pankhurst, C. L., & Robinson, P. G. (2007). Testing relationships between clinical and non-clinical variables in xerostomia: A structural equation model of oral health-related quality of life. Quality of Life Research, 16(2), 297–308.
Ryu, E., West, S. G., & Sousa, K. H. (2007). Mediation and moderation: testing relationships between symptom status, functional health, and quality of life in HIV patients. Multivariate Behavioral Research, 44(2), 213–232.
Wyrwich, K., Harnam, N., Locklear, J., Svedsäter, H., & Revicki, D. (2011). Understanding the relationships between health outcomes in generalized anxiety disorder clinical trials. Quality of Life Research, 20(2), 255–262.
Heslin, K., Stein, J., Heinzerling, K., Pan, D., Magladry, C., & Hays, R. (2011). Clinical correlates of health-related quality of life among opioid-dependent patients. Quality of Life Research, 20(8), 1205–1213.
Wilson, I., & Kaplan, S. (1995). Clinical practice and patients’ health status: How are the two related? Medical Care, 33(4 Suppl), AS209–AS214.
Ferrans, C., Zerwic, J., Wilbur, J., & Larson, J. (2005). Conceptual model of health-related quality of life. Journal of Nursing Scholarship, 37(4), 336–342.
Maurice-Stam, H., Oort, F., Last, B., & Grootenhuis, M. (2009). A predictive model of health-related quality of life in young adult survivors of childhood cancer. European Journal of Cancer Care, 18(4), 339–349.
Schulz, T., Niesing, J., Stewart, R. E., Westerhuis, R., Hagedoorn, M., Ploeg, R. J., et al. (2012). The role of personal characteristics in the relationship between health and psychological distress among kidney transplant recipients. Social Science & Medicine. doi: 10.1016/j.socscimed.2012.05.028 [Epub ahead of print].
Newsom, J. T., & Schulz, R. (1996). Social support as a mediator in the relation between functional status and quality of life in older adults. Psychology and Aging, 11(1), 34–44.
Cheong, J., MacKinnon, D. P., & Khoo, S. T. (2003). Investigation of mediational processes using parallel process latent growth curve modeling. Structural Equation Modeling, 10(2), 238–262.
Cole, D. A., & Maxwell, S. E. (2003). Testing mediation models with longitudinal data: Questions and tips in the use of structural equation modeling. Journal of Abnormal Psychology, 112(4), 558–577.
Maxwell, S. E., & Cole, D. A. (2007). Bias in cross-sectional analyses of longitudinal mediation. Psychological Methods, 12(1), 23–44.
Little, T. D., Preacher, K. J., Selig, J. P., & Card, N. A. (2007). New developments in latent variable panel analyses of longitudinal data. International Journal of Behavioral Development, 31(4), 357–365.
MacKinnon, D. P. (2008). Longitudinal mediation analysis. In D. P. MacKinnon (Ed.), Introduction to statistical mediation analysis (pp. 193–236). New York: Lawrence Erlbaum.
Liu, L. C., Flay, B. R., & Aban Aya Investigators. (2009). Evaluating mediation in longitudinal multivariate data: Mediation effects for the Aban Aya youth project drug prevention program. Prevention Science, 10(3), 197–207.
Audrain-McGovern, J., Rodriguez, D., & Kassel, J. D. (2009). Adolescent smoking and depression: Evidence for self-medication and peer smoking mediation. Addiction, 104(10), 1743–1756.
Selig, J. P., & Preacher, K. J. (2009). Mediation models for longitudinal data in developmental research. Research in Human Development, 6(2–3), 144–164.
Negriff, S., Ji, J., & Trickett, P. (2011). Exposure to peer delinquency as a mediator between self-report pubertal timing and delinquency: A longitudinal study of mediation. Development and Psychopathology, 23(1), 293–304.
Roth, D. L., & MacKinnon, D. P. (2012). Mediation analysis with longitudinal data. In J. T. Newsom, R. N. Jones, & S. M. Hofer (Eds.), Longitudinal data analysis: A practical guide for researchers in aging, health, and social sciences (pp. 181–216). New York: Routledge.
Wilson, I., & Cleary, P. (1997). Clinical predictors of declines in physical functioning in persons with AIDS: Results of a longitudinal study. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology, 16(5), 343–349.
Mathisen, L., Andersen, M. H., Veenstra, M., Wahl, A. K., Hanestad, B. R., & Fosse, E. (2007). Quality of life can both influence and be an outcome of general health perceptions after heart surgery. Health and Quality of Life Outcomes, 5, 27.
Devine, K., Reed-Knight, B., Loiselle, K., Simons, L., Mee, L., & Blount, R. (2011). Predictors of long-term health-related quality of life in adolescent solid organ transplant recipients. Journal of Pediatric Psychology, 36(8), 891–901.
Collins, L. M., Graham, J. W., & Flaherty, B. P. (1998). An alternative framework for defining mediation. Multivariate Behavioral Research, 33(2), 295–312.
Allman, R. M., Sawyer, P., & Roseman, J. M. (2006). The UAB Study of Aging: Background and prospects for insights into life-space mobility among older African-Americans and Whites in rural and urban settings. Aging Health, 2(3), 417–428.
Wolinsky, F., Bentler, S., Hockenberry, J., Jones, M., Obrizan, M., Weigel, P., et al. (2011). Long-term declines in ADLs, IADLs, and mobility among older Medicare beneficiaries. BMC Geriatrics, 11, 43.
Parker, M., Baker, P. S., & Allman, R. M. (2002). A life-space approach to functional assessment of mobility in the elderly. Journal of Gerontological Social Work, 35(4), 35–55.
Ritchie, C., Locher, J., Roth, D., McVie, T., Sawyer, P., & Allman, R. (2008). Unintentional weight loss predicts decline in activities of daily living function and life-space mobility over 4 years among community-dwelling older adults. Journal of Gerontology. Series A, Biological Sciences and Medical Sciences, 63(1), 67–75.
Okonkwo, O. C., Roth, D. L., Pulley, L., & Howard, G. (2010). Confirmatory factor analysis of the validity of the SF-12 for persons with and without a history of stroke. Quality of Life Research, 19(9), 1323–1331.
Charlson, M., Pompei, P., Ales, K., & MacKenzie, C. (1987). A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. Journal of Chronic Diseases, 40(5), 373–383.
Hoyle, R. H., & Kenny, D. A. (1999). Sample size, reliability, and tests of statistical mediation. In R. H. Hoyle (Ed.), Statistical strategies for small sample research (pp. 195–222). Thousand Oaks, CA: Sage.
MacKinnon, D. P. (2008). Introduction to statistical mediation analysis. New York: Lawrence Erlbaum.
Marsh, H. W. (1993). Stability of individual differences in multiwave panel studies: Comparison of simplex models and one-factor models. Journal of Educational Measurement, 30(2), 157–183.
Curran, P. J., & Bollen, K. A. (2001). The best of both worlds: Combining autoregressive and latent curve models. In L. M. Collins & A. G. Sayer (Eds.), New methods for the analysis of change (pp. 107–135). Washington, DC: American Psychological Association.
Gollob, H. F., & Reichardt, C. S. (1991). Interpreting and estimating indirect effects assuming time lags really matter. In L. M. Collins & J. L. Horn (Eds.), Best methods for the analysis of change: recent advances, unanswered questions, future directions (pp. 243–259). Washington, DC: American Psychological Association.
Anderson, S. E., & Williams, L. J. (1992). Assumptions about unmeasured variables with studies of reciprocal relationships: The case of employee attitudes. Journal of Applied Psychology, 77(5), 638–650.
Sobel, M. E. (1982). Asymptotic confidence intervals for indirect effects in structural equation models. Sociological Methodology, 13, 290–312.
MacKinnon, D. P., Lockwood, C. M., & Williams, J. (2004). Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research, 39(1), 99–128.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural equation models (pp. 136–162). Newbury Park, CA: Sage.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55.
Yu, C. Y. (2002). Evaluating cutoff criteria of model fit indices for latent variable models with binary and continuous outcomes. Doctoral dissertation, University of California, Los Angeles.
Muthén, B. (1984). A general structural equation model with dichotomous, ordered categorical, and continuous latent variable indicators. Psychometrika, 49(1), 115–132.
Asparouhov, T., & Muthén, B. (2010). Weighted least squares estimation with missing data. http://www.statmodel.com/download/GstrucMissingRevision.pdf. Accessed 1 Aug 2011.
Muthén, L. K., & Muthén, B. O. (1998–2010). Mplus user’s guide (6th edn). Los Angeles, CA: Muthén & Muthén.
Millsap, R. E. (2005). Four unresolved problems in studies of factorial invariance. In A. Maydeu-Olivares & J. J. McArdle (Eds.), Contemporary psychometrics: A festschrift to Roderick P. McDonald (pp. 153–171). Mahwah, NJ: Erlbaum.
Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). New York: The Guilford Press.
Andersen, C., Wittrup-Jensen, K., Lolk, A., Andersen, K., & Kragh-Sørensen, P. (2004). Ability to perform activities of daily living is the main factor affecting quality of life in patients with dementia. Health and Quality of Life Outcomes, 2, 52.
Vest, M., Murphy, T., Araujo, K., & Pisani, M. (2011). Disability in activities of daily living, depression, and quality of life among older medical ICU survivors: A prospective cohort study. Health and Quality of Life Outcomes, 9, 9.
Höfer, S., Benzer, W., Alber, H., Ruttmann, E., Kopp, M., Schüssler, G., et al. (2005). Determinants of health-related quality of life in coronary artery disease patients: A prospective study generating a structural equation model. Psychosomatics, 46(3), 212–223.
Heo, S., Moser, D., Riegel, B., Hall, L., & Christman, N. (2005). Testing a published model of health-related quality of life in heart failure. Journal of Cardiac Failure, 11(5), 372–379.
Saban, K., Penckofer, S., Androwich, I., & Bryant, F. (2007). Health-related quality of life of patients following selected types of lumbar spinal surgery: A pilot study. Health and Quality of Life Outcomes, 5, 71.
Collins, L. M., & Graham, J. W. (2002). The effect of the timing and spacing of observations in longitudinal studies of tobacco and other drug use: Temporal design considerations. Drug and Alcohol Dependence, 68(Suppl1), S85–S96.
Schafer, J. L. (1997). Analysis of incomplete multivariate data. London: Chapman & Hall.
Hedeker, D., & Gibbons, R. D. (1997). Application of random-effects pattern-mixture models for missing data in longitudinal studies. Psychological Methods, 2(1), 64–78.
Acknowledgments
The UAB Study of Aging is funded through a grant from the National Institute on Aging (R01 AG015062).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bentley, J.P., Brown, C.J., McGwin, G. et al. Functional status, life-space mobility, and quality of life: a longitudinal mediation analysis. Qual Life Res 22, 1621–1632 (2013). https://doi.org/10.1007/s11136-012-0315-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-012-0315-3