
Abstract
Purpose
This study investigates the relationship among perceived satisfaction from social support, hope, and QOL of PLWHA.
Method
A cross-sectional in design was applied, among a sample of 160 HIV-infected persons receiving treatment, care, and support from eight community-based NGOs. QOL was assessed using the WHO (QOL)-26 tool, and social support was assessed by use of a modified Sarason’s Social Support Questionnaire. A Hope Assessment Scale was also developed.
Results
The non-family support network was greater than family support network. Overall satisfaction from social support and hope was significantly correlated with QOL; the greatest effect of social support was on environmental functioning, and the lowest was on social relationships, emotional support was less a predictor of social relationship than other types of supports.
Conclusion
The effect of perceived satisfaction from social support was through the mediation variable hope. As it has widely been recognized that community-based support is vital for issues of quality of life, strategies to improve social support and hope intervention programs are strongly encouraged. The results of the study have implications for providing care, treatment, and psycho-social support to maintain or enhance quality of life of PLWHA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The development of anti-HIV medicine has led to significant increases in life expectancy and quality of life for people living with HIV/AIDS (PLWHA). The average number of years a PLWHA lives after treatment started with combination antiretroviral therapy is estimated to be 20–35 years [3]. This tends to transform HIV to a chronic disease [33]. Chronic traits of a disease increase demand for care, treatment, and support for PLWHA. In order to fulfill demand for care and treatment, family, friends, and the community can be major sources of support [20]. A number of research studies have indicated that there is a significant relation between social support and quality of life [4, 5, 12, 16, 28, 29, 32, 40, 51].
Hope is an under researched concept in the social aspects of HIV treatment [8]. The concept has been explored minimally within the context of HIV/AIDS [36], previous research on HIV/AIDS mainly focused on the dynamics of hope in the process of caring PLWHA [35], maintaining hope while coping with the end-stage of AIDS and how nurses inspire and instill hope in terminally ill AIDS patients [14]. Akinsola [1] suggested that the goal of fostering hope should focus on how to improve quality of life of the individual. However, thorough research on factors that mediate the relationship between social support and health-related outcome or quality of life on PLWHA is unavailable.
The assumptions made in this paper are:
-
(1)
There will be a significant positive correlation between perceived satisfaction from social support and quality of life, perceived satisfaction from social support and hope and perceived hope and quality of life among PLWHA;
-
(2)
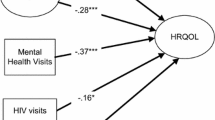
Perceived satisfaction from social support and hope considered together will explain more of the variance of quality of life than either variable considered independently (Fig. 1).

Mediation model among social support, hope, and quality of life
Review of literature
Defining social support
The roots of the concept of social support are found in nineteenth century sociologists such as Durkheim [15], who established the link between diminishing social ties and an increase in suicide [44, 52]. As a concept, it has evolved over time starting with the term “social ties” as used by Durkheim [52].
Caplan [10] describes a social system as others who (1) help people to mobilize their psychological resources in order to deal with emotional problems (linking, loving, and empathy); (2) information (about the environment), (3) instrumental aid (provide an individual with money, material, skills, and advice in order to help them to deal with particularly stressful situations that they are exposed to).
Social support has come to possess different dimensions and is expressed in different forms and different ways. The source of social support can come in the form of emotional support from family, friends, and peers [20]. It can also emanate from social interactions in the community including professionals [9] and even from interaction with the environment [19].
Social support and hope in HIV
Herth [26] examined hope-fostering strategies on PLWHA which were defined as those sources that assist to install, support or restore hope in some way. Further strategies were categorized into seven categories: (1) interpersonal connectedness; mainly focuses on love from family and friends, i.e., meaningful relationships, being loved and giving love; (2) spiritual base focusing on spiritual practice as a source of hope, belief in God and family, belief helps to overcome the suffering; (3) attainable aim direct to setting goals and maintaining independence, goals are further divided into attainable and unattainable; (4) affirmation of worth; focusing on positive relationships within professional careers, helping relationship regarding illness and being treated with courtesy and respect; (5) light heartedness; focusing on friendship with others who are suffering from a same cause, laughing with professionals and laughing as an inner resource; (6) personal attribute; focusing on determination and being a fighter; (7) uplifting memories; focusing on recalling uplifting moments acting as a hope-fostering strategy.
Hindrances to hope were defined as those factors that interfere or inhibit the possibility of attaining or maintaining hope, which constitute: (1) abandonment and isolation, physical and emotional loss of significant others, such as spouse that will not or cannot support patient psychologically, poor communication with professionals; (2) uncontrollable pain and discomfort, continuance of overwhelming pain or discomfort despite repeated attempts to control; and (3) devaluation of personhood, being treated as a non-person having little value.
Another study on HIV suggested that hope is an important component of effectively dealing with HIV and AIDS. The experience of hope is less just after diagnosis of HIV, and potential sources for fostering hope are (1) receiving support; (2) engaging in meaningful life experiences; (3) perceiving options; (4) receiving treatment; and maintaining quality of life [23].
One of the studies on PLWHA identified four major ways that hope was maintained: by miracles, religion, involvement in work or vocations, and support of family and friends [21]. Specific ways of being in relationships with others include dealing with one’s family, renegotiating the friendship group, helping others with HIV and developing a relationship with a higher power, and in this case, social support act as the functional component of relationships, such as emotional and tangible assistance [5]. A study on HIV infected terminally ill persons indicates that there were significant differences in the level of hope according to diagnosis [26], and hope can help PLWHA to deal with the HIV diagnosis and acts as an internal resource for helping individuals living with HIV to experience increased well-being [25].
One of the studies on women with HIV showed a significant positive relationship between hope and coping, hope and managing the illness, and between hope and spiritual activities. A significant negative relationship was observed between hope, and inability to cope and stigma was associated with less hope [42].
Promoting hope and acceptance of HIV-status enables PLWHA to develop a positive therapeutic relationship with medication, which in turn promotes adherence to treatment. Treatment adherence was related to active participation in social networks [39]. Facilitating hope appears to be an important therapeutic goal in working with newly diagnosed HIV-positive individuals, and hope was connected to longer life for PLWHA [23].
There are two sources of social support that have been discussed in previous studies. The first relates to family and friends, and the second to community-based support, government agencies, and the health care industry [48]. The non-family support mostly comes from nurses or nursing practice, and it is connected with the concepts of nursing, caring, and helping [14], peer counselors and health workers are important to provide referral information (as informational support) for livelihood to receive counseling and medical treatment in the process of fostering hope [1, 23].The support from friends and family is valuable to counter stigma [2, 17].
Social support and quality of life in HIV
Quality of life is defined as a “fighting spirit” associated with longer life expectancies for individuals with HIV/AIDS [37]. Social support of PLWHA was significantly correlated with health-related quality of life [41]. Research on PLWHA indicates that a supportive social environment, particularly friends and family acceptance, was significantly associated with quality of life [16, 28]. Alienation, rejection, and isolation can threaten hope and well-being of PLWHA [38].
Taking care of physical, psychological, and social relationship was important for maintaining health-related quality of life and social support of PLWHA [49]. One of the studies suggested that social support is significantly associated with health-related quality of life, with the exception of physical functioning and bodily pain aspects [6]. A low level of social support causes a worsening of physical functioning [45]. Another study suggested that psychological functioning and physical symptoms were associated with a higher level of social support [54]. Furthermore, the type of social support influences the level of quality of life, as the level of emotional support decreases physical distress, mental distress, activity limitation, depressive symptoms, anxiety symptoms, insufficient sleep, and pain [50], the tangible or functional support seems to be more relevant to PLWHA [18]. Social support from peers was critical for psychological functioning of PLWHA in many circumstances. However, in periods of crisis, family support becomes a more important determinant of psychological functioning [13].
Also, quality of life relates both to adequacy of material circumstances and to personal feelings about these circumstances, and it includes “overall subjective feelings of well-being that are closely related to morale, happiness and satisfaction” [37, 43].
In summary, in terms of research on HIV, the above review of literature showed that hope is an inner resource to experience well-being for long-term survival. Most of the research findings [4, 5, 12, 16, 28, 29, 32, 40, 51] suggested the existence of relationships among aspects of social support and quality of life. Others [1, 14, 35] pointed out relationships among aspects of hopelessness, depression, despair, coping, managing illness, and quality of life. None of the studies explored the relationship among positive aspects of life, which is being ‘hopeful about the future’, perceived satisfaction from social support, and quality of life. Yet, even with some progress, hope has remained a complex and even elusive concept to measure in community settings where PLWHA are receiving care, support, and treatment. A lack of research in the area continues to exist in relation to the HIV/AIDS population. In addition, most of the tools used in previous research in HIV were not specific HIV/AIDS. This research intends to fill the gaps in the conceptual approach of hope as having positive attributes from social support and tools to measure hope and perceived social support specific to HIV.
Methodology
Study design and participants
The study was descriptive and cross-sectional in design, focusing on adults living with HIV/AIDS in Nepal. The underlying criterion for sample selection was PLWHA receiving support from a community-based NGO. Further, the study also relied on a convenient and purposefully selected sample (N = 160). Selection of participants was based on the following criteria: (1) PLWHA receiving care, support, and treatment, (2) PLWHA being at least 18 years old, and (3) PLWHA who were physically able to answer the questionnaire. The study was conducted during 2008–2009, and data collection was undertaken by the author with the support of hired professional research assistants from the National Health Research Council in Nepal. One-to-one interviews were conducted during monthly meetings in eight community-based organizations where PLWHA gather to share their experiences and to receive other support. Prior to the interviews, the purpose of the study was explained to the participants, and with their consent, information was collected agreeing that their names and addresses would not be included in the questionnaire, as well as in research paper.
Measurements
Demographic questionnaire
The first questionnaire was administered to gather information regarding age, gender, type of religion, educational level, occupational status, mode of transmission, duration of living with HIV, stigma, how they handle with stigma and self-reported CD4+ count.
Hope scale
The hope scale was developed particularly for this study. The construct of the scale was based on the meaning of hope defined by 25 PLWHA during in-depth interviews and the hope concept suggested by Hays [24] and Herth [26], which was specific to PLWHA. The “Hope scale” consists of seven items and measures perceived hope. The first item measures hope from engaging in meaningful life, the second item measures hope from personnel willpower, the third item measures level of hopelessness due to discrimination by others, the fourth item measures perceived hope from family love and care, the fifth item measures perceived hope because of help from friends, counselors or health and community workers, the sixth item measures perceived hope from others help with material, such as caring spouse, and the seventh item measures perceived hope from belief in religion or God. The scale was translated into Nepali language and the Nepali version of the scale showed good internal reliability yielding Cranach’s alpha .88. The scale applied a five point value ranging from not at all to extremely hopeful; a higher score indicated better hope.
Social support questionnaire
The social support scale was adapted from the shorter Sarason’s Social Support questionnaire (SSQ-S) developed by Sarason et al. [46]. The SSQ-S original is a 12-item instrument that measures two aspects of perceived social support: six odd-numbered items count social support network (the number of people in the individual’s social support system), the total number of people in the individual’s social support system is further divided into family network and non-family network support and six even-numbered items measures perceived satisfaction from social support network. The overall satisfaction from specific support is based on a six-point scale ranging from very satisfied to very dissatisfied. The original scale was modified into a 14-item scale. The added and modified two odd items were to measure “whom they could really count on when they needed help for” HIV/AIDS-related treatment and help from spouse, for living arrangement, for food, for transportation and others, followed by two even number for level of satisfaction from support. A factor analysis of the seven odd number items outcome revealed three distinct factors and each corresponds to a different support function; the first tangible, the second informational, and the third emotional support. The modified version of HIV-specific social support questionnaire was translated from English into Nepali language and translated back from Nepali into English by independent translators. Each of the domains in the Nepali version of the scale showed good internal reliability, yielding Cronbach’s alpha of .89 emotional, .86 informational, .82 tangible, and .87 for overall support.
Quality of life
The (WHO) QOL-26 tool consists of 26 items and was derived from the (WHO) QOL-100 items tool. It includes seven items in the physical domain (physical state), six items in the psychological domain (cognitive and affective state), three items in the social domain (interpersonal relationship and social role in life), eight items in the environmental domain (relationship to salient feature of the environment), one item for general quality of life, and one item for health-related quality of life combining together as global domain [34]. The PLWHA were required to rate their quality of life in the past 2 weeks. The item scores ranged from 1 to 5, with a higher score indicating a better quality of life. Because the numbers of items were different for each domain, the domain scores were calculated by multiplying the average of the scores of all items in the domain by 4 to standardize all domain scores and make it comparable with other domains [27, 31, 49].
The (WHO) QOL-26 tool is translated in more than 10 different languages; the Hindi version consists of 26 items that show satisfactory psychometric properties and good internal reliability [47]. The Hindi version of (WHO) QOL-26 was translated into Nepali language by an independent translator for the convenience of study participants and the interviewer to understand the items of the questionnaire. The reason behind adapting the Hindi version was that the (WHO) QOL-Hindi was verified as a valid instrument for comprehensively assessing the quality of life in health care settings in India [47]. Also, due to the geographical proximity (open border between Nepal and India) and the historical relationship between the two countries; people from India and Nepal have a lot in common, including culture, language, religion, and value systems. The Nepali version of (WHO) QOL-26 tool showed good internal reliability, Cronbach’s alpha of .85.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) version 17.0. The respondents’ demographics status was presented as a mean and a percentage. Scores of quality of life, social support, and hope scale were presented as a mean, standard deviation and range. Pearson’s correlation analysis was performed to see the correlation between perceived satisfactions from social support, hope, and quality of life. Stepwise hierarchical multiple regression was also conducted to observe the contribution of the independent variables, social support and hope, had on each quality of life domain. To observe the contribution or variance on quality of life by two independent variables, step one represents QOL = B 0 +B 1 (social support) and step two QOL = Y 0 + Y 1 (social support) + Y 2 (hope). The results are presented as multiple R, F ratio, adjusted R 2, R 2 squared change and significance value.
Results
The demographic and clinical characteristics of the study sample are summarized in Table 1. Of the 160 HIV-infected person included in study, 68.7% were male and 31.3% were female, 20% of them were between 18 and 25 years old, 44.4% were between 25 and 32%, 26.8% were between 33 and 40, and 8.8% were over 40 years old. In addition, 26% were unmarried, 54% were married, 14.4% were widow, and 5% were divorced. It was also found out that 83.8% of respondents were Hindu, 1.8% were Buddhist, 9.4% were Muslims, and 5% were Christian. In terms of education, 18.7% were uneducated, 33.7% had received primary education, 19.4% had higher education, 28.2% of respondents had high school education, and 19.4% had higher education. The data on occupation showed that 21.9% were employed where as 60% were unemployed and 18.1% were involved in social work in community-based NGOs. Time since diagnosis, 25.1% were in 2008–2009, 32.5% were 2–4 years ago, 6.9% were between 5 and 8 years, and 35.5% were more than 8 years.
The acknowledge risk factors showing 43.8% injecting drug user, 21.8% had infection cause of sex with other than a partner and 34.4% were infected by their husbands and 26.9% had <200 cells/μL CD4 count blood level, and 73.1% had more than 200 cells/μL.
The mean standard deviation and range of score for the social support, hope, and quality of life scale are presented in Table 2. The mean score was 5.15 for overall satisfaction from social support, 3.87 for hope, 14.01 for physical capacity, 14.36 for psychological functioning, 12.48 for social relationship, 13.66 environmental functioning, and 6.73 for global domains of quality of life.
As predicted, a significant positive correlation was found between the perceived overall satisfaction from the social support and all domain of quality of life, physical capacity (r = .296, p = .000), psychological functioning (r = .243, p = .001), social relationship (r = .152, p = .029), environmental functioning (r = .398, p = .000), and global functioning (r = .286, p = .000). Satisfaction with informational, tangible, and emotional support was a stronger predictor of physical functioning, psychological functioning, environmental functioning, and global domains of quality of life than social relationship. The correlations obtained between perceived satisfaction from social support and the domains of quality of life are summarized in Table 3.
As predicted, a significant positive correlation was found between overall perceived satisfaction from social support and hope (r = .296, p = .001), satisfaction with informational (r = .273, p = .000) and tangible (r = .267, p = .000). Satisfaction with tangible and informational support was a stronger predictor of hope than emotional satisfaction (r = .240, p = .001). The results of the correlation are summarized in Table 4.
As predicted, a significant positive correlation was found between hope and quality of life domain, although hope is significantly correlated with all domains of quality of life, hope was a stronger predictor for the environmental functioning (r = .445, p = .000) than the other four domains of the quality of life. The result of the correlations is summarized in Table 5.
As predicted, perceived satisfaction with social support and hope considered together would explain more variance in quality of life than either variables considered independently, implying stepwise hierarchical multiple regression perceived satisfaction from social support was entered into regression equation on the first step. The adjusted R 2 shows that 7% of variance in physical functioning (F = 14.095, p = .000), 5% of variance in psychological functioning (F = 10.371, p = .002), 2% of variance in social relationship (F = 4.319, p = .039), 17% of variance in environmental functioning (F = 33.212, p = .000), and 8% of variance in global functioning (F = 14.321, p = .000) domains of quality of life were explained by overall satisfaction from perceived social support.
Entering hope into equation at step two, the adjusted R 2 indicates that 15% of variance in physical functioning (F = 14.508, p = .000) explaining an additional 7% of variance, 14% variance in psychological functioning (F = 13.594, p = .000) explaining an additional 8% variance, 9.8% variance in social relationship (F = 9.331, p = .000) explaining an additional 8% variance, 27% variance in environmental functioning (F = 30.364, p = .000) explaining an additional 10% variance, 12.% of variance in global functioning (F = 11.762, p = .004) explaining an additional 4% variance of domains in quality of life. The variance in environmental functioning explained by the satisfaction with social support independently or considered together was greater than the other domain of quality of life. Together perceived satisfaction with social support and hope was significantly explained more by variance in quality of life. The result of the stepwise hierarchical multiple regression of quality of life on the independent variables are summarized in Table 7.
Additional findings
Although it was not part of the assumption in this study, the relationship among demographic, health-related variables and the main study variables was investigated. The Pearson correlations were calculated among the variables: age, gender, occupation, education, years of living with HIV, acknowledged risk factor, stigma, and CD4+ count, overall satisfaction from social support, hope, physical functioning, psychological functioning, social relationship, environmental functioning and global domain of quality of life. Only gender was significantly correlated with overall satisfaction (r = .174, p = .029), hope (r = .369, p = .000), physical functioning (r = .213, p = .007), psychological functioning (r = . 256, p = .001), social relationship (r = .213, p = .007), environmental functioning (r = .312, p = .000), and global (r = .224, p = .002) domain of quality of life, the outcome of correlation is summarized in Table 6.
Discussion
The aim of the study was first to assess the level of satisfaction from social support, the level of hope and the quality of life of PLWHA, second to examine the relationship among social support, hope, and quality of life. This study applied hope as a mediation factor between social support and quality of life.
Furthermore, while many of the previous studies have been limited to specific risk factor groups or specific age groups such as elderly, gay people or persons with AIDS, this study focused on participants with various geographical features, such as mountainous, hilly, and lowland areas, and consisted of a heterogeneous group of PLWHA. It is plausible to argue that this study is reflective of the general HIV population in the context of risk factor and age group distribution and other characteristics in Nepal, therefore, the findings of the study may be generalized to HIV-infected people being cared, supported, and treated in other community settings in Nepal.
Social support should not be conceptualized simply in terms of availability, but in its perceived adequacy. Social support may not be considered useful unless the individual perceives it as supportive. It has been proposed that the qualitative components of perceived satisfaction from three major components of social support i.e., informational, tangible, and emotional supports [24] are considered more important than the quantitative aspects of social support [51]. Perception is generally a better predictor of health outcome than the receipt [53].
The result of the correlation analyses shows that satisfaction with social support was significantly correlated with all domains in the quality of life. These findings support those found in previous studies, which show that social support was significantly correlated with quality of life [27, 41, 51]. The greatest impact of social support was on environmental functioning, whereas the lowest impact was on social relationship (Table 3). This study’s finding was different from previous studies by Bastardo and Kimberlin [6], Jia et al. [29], and Remor [45], who suggested that that social support was not correlated with the physical functioning, and only psychological functioning was correlated with social support [54]. Furthermore, satisfaction from the informational and tangible support was a better predictor of quality of life except social relationship domain (Table 3).
The findings of this study show that mean score of family support network was less than the non-family support network (Table 2), the family support is a major source of emotional support [13, 48], limited emotional support can inhibit social relationship [50], and a study by Friedland et al. [16] and Ichikawa [28]) suggested that family acceptance was significantly related to the social relationship of quality of life. Harris and Larsen [22] suggested that non-family members such as health workers, counselors, volunteers, and friends have vital contributions in providing information and tangible support for livelihood and treatment. Therefore, the concept of providing information support should be based on the information to acquire emotional support from family and other social relations, which would further increase the social relationship of PLWHA.
Overall satisfaction from social support was significantly correlated with hope, and this finding is similar to that which shows hope was positively associated with perceived social support by PLWHA [55]. Again, satisfaction from emotional support was less of a predictor of levels of hope than informational and tangible support. A similar finding has been reported by [1, 5, 18, 24] indicating instrumental or informational support seems more relevant to people living with HIV when patients experience AIDS-related symptoms.
Hope was significantly correlated with all domains of the quality of life. This finding is collaborated by similar findings in which hope was found to be an important internal resource for the increased functioning of PLWHA [11, 25]. The greatest impact of hope was on environmental functioning and the lowest was on global functioning. The employment status, Table 1, showed that 18.1% of the respondents were engaged as support provider and they were working as counselors or assisting in the referral system. They called themselves a social worker, which, in turn, puts them in the company of others who are also infected with HIV. This is in line with the hope-fostering strategy suggested by Herth [26]. The argument states that being around others who have HIV and who have been living long healthy lives helps PLWHA to experience hope that they may also have a long healthy life, the findings in this study showed that not only being around others, but also receiving various types of support from PLWHA can foster hope which leads to better quality of life. This study’s findings confirm that social support has impact on the all domains of quality of life and hope.
The result from the regression analysis showed that the effect of social support on the quality of life was through the mediation variable hope, when controlling other demographic characteristics. Although the independent variables, social support plus hope, together explain significant amount of variance in quality of life (Table 7), there still exists a large number of variance unexplained.
The outcome of additional findings showed that there was statistically significant mean differences between male and female (male = 4.2, female = 2.9. p = .003) in terms of overall social network. This study found that HIV-infected females experienced less perceived satisfaction from social support, which, in turn, concurs the finding that HIV-infected women receive less social support [31]. This may refer to Beine’s [7] proposed dominant cultural model of HIV/AIDS, in which he suggested that widely shared understanding of HIV/AIDS as a fetal, infectious, and sexually transmitted disease and further suggested that the common themes regarding HIV/AIDS as a “bad person’s” disease, HIV/AIDS as the result of bad karma, while bad karma and bad persons refer to those who involve in promiscuity and prostitution which are against the moral and traditional customs. Cultural values such as accuses for transmitting disease to their husband, shyness, fear of stigmatization, and discrimination prevent women from disclosing their status, not to seek medical support or advices [30]. Furthermore, socio-cultural factors may influence the social support, hope, and quality of life of women participants in this study.
Conclusion
Correlation analysis showed that social support was significantly associated with hope and quality of life, and hope was also significantly associated with quality of life; however, social relationship had less of a correlation than other domains. Emotional support was less of a predictor of quality of life and hope. Increasing social support and increasing hope together may have influence a better quality of life in this sample.
Although the independent variables social support and hope account for a significant amount of variance of quality of life, there is still a large number of variance remaining unexplained. Further research is suggested to investigate other sources of variance in the domains of quality of life of person being cared, treated, and supported in community setting in Nepal.
Community-based workers and health professionals should provide tangible support and inform to HIV-infected persons about psycho-social support from friends and family, particularly to females. The regression analysis also showed that the effect of social support on quality of life was mainly through the mediation variable hope, suggesting that improving social support will increase hope, which, in turn, would improve their quality of life.
References
Akinsola, H. A. (2001). Fostering hope in people living with AIDS in Africa: The role of primary health-care workers [review]. Australian Journal of Rural Health, 9(4), 158–165.
Andrews, S. (1995). Social support as a stress buffer among human immunodeficiency virus-seropositive urban mothers [case reports]. Holistic Nursing Practice, 10(1), 36–43.
Antiretroviral Therapy Cohort, C. (2008). Life expectancy of individuals on combination antiretroviral therapy in high-income countries: A collaborative analysis of 14 cohort studies [research support, non-US Gov’t]. Lancet, 372(9635), 293–299.
Ashton, E., Vosvick, M., Chesney, M., Gore-Felton, C., Koopman, C., O’Shea, K., et al. (2005). Social support and maladaptive coping as predictors of the change in physical health symptoms among persons living with HIV/AIDS [article]. Aids Patient Care and STDs, 19(9), 587–598.
Barroso, J. (1997). Social support and long-term survivors of AIDS [article]. Western Journal of Nursing Research, 19(5), 554–573.
Bastardo, Y. M., & Kimberlin, C. L. (2000). Relationship between quality of life, social support and disease-related factors in HIV-infected persons in Venezuela. Aids Care-Psychological and Socio-Medical Aspects of Aids/Hiv, 12(5), 673–684.
Beine, D. K. (2003). Ensnared by AIDS: Cultural contexts of HIV/AIDS in Nepal (p. 411). Kantipath, Kathmandu, Nepal: Mandala Book Point.
Bernays, S., Rhodes, T., & Barnett, T. (2007). Hope: A new way to look at the HIV epidemic [article]. Aids, 21, S5–S11.
Brashers, D. E. (2002). Belonging to AIDS activist group helps HIV + to cope. Journal of Social and Personal Relationships, 19, 113–130.
Caplan, G. (1974). Support systems and community mental health. New York: Behavioral Publications.
Chammas, G. Y. (1999). Hope, functional status, and quality of life in hospitalized patients with human immunodeficiency virus infection and acquired immunodeficiency syndrome (doctoral dissertation, Columbia University Teachers College, 1999). Dissertation Abstracts International, 60(03), 1027B (UMI No. 9921384).
Chesney, M. A., Chambers, D. B., Taylor, J. M., & Johnson, L. M. (2003). Social support, distress, and well-being in older men living with HIV infection [article]. Jaids-Journal of Acquired Immune Deficiency Syndromes, 33, S185–S193.
Crystal, S., & Kersting, R. C. (1998). Stress, social support, and distress in a statewide population of persons with AIDS in New Jersey [article]. Social Work in Health Care, 28(1), 41–60.
Cutcliffe, J. R. (1995). How do nurses inspire and instill hope in terminally ill HIV patients [article]. Journal of Advanced Nursing, 22(5), 888–895.
Durkheim, E. (1984). The division of labor in society. New York: The Free Press.
Friedland, J., Renwick, R., & McColl, M. M. (1996). Coping and social support as determinants of quality of life in HIV/AIDS [article]. Aids Care-Psychological and Socio-Medical Aspects of Aids/Hiv, 8(1), 15–31.
Galvan, F. H., Davis, E. M., Banks, D., & Bing, E. G. (2008). HIV stigma and social support among African Americans [research support, N.I.H., extramural; research support, non-US gov’t]. AIDS Patient Care STDS, 22(5), 423–436.
Gant, L. M., & Ostrow, D. G. (1995). Perceptions of social support and psychological adaptation to sexually acquired HIV among white and African-American men [article]. Social Work, 40(2), 215–224.
Gottlieb, B. H. (1983). Social support strategies: Guidelines for mental health practice. Beverly Hills, CA: Sage.
Greenberger, E., Chen, C. S., Tally, S. R., & Dong, Q. (2000). Family, peer, and individual correlates of depressive symptomatology among US and Chinese adolescents. Journal of Consulting and Clinical Psychology, 68(2), 209–219.
Hall, B. A. (1994). Ways of maintaining hope in HIV disease.
Harris, G. E., & Larsen, D. (2007). HIV peer counseling and the development of hope: Perspectives from peer counselors and peer counseling recipients [article]. Aids Patient Care and STDS, 21(11), 843–859.
Harris, G. E., & Larsen, D. (2008). Understanding hope in the face of an HIV diagnosis and high-risk behaviors [article]. Journal of Health Psychology, 13(3), 401–415.
Hays, R. B., Turner, H., & Coates, T. J. (1992). Social support, aids-related symptoms, and depression among gay men [article]. Journal of Consulting and Clinical Psychology, 60(3), 463–469.
Heinrich, C. R. (2003). Enhancing the perceived health of HIV seropositive men [article]. Western Journal of Nursing Research, 25(4), 367–382.
Herth, K. (1990). Fostering hope in terminally-ill people [review]. Journal of Advanced Nursing, 15(11), 1250–1259.
Hirabayashi, N., Fukunishi, I., Kojima, K., Kiso, T., Yamashita, Y., Fukutake, K., et al. (2002). Psychosocial factors associated with quality of life in Japanese patients with human immunodeficiency virus infection. Psychosomatics, 43(1), 16–23.
Ichikawa, M., & Natpratan, C. (2006). Perceived social environment and quality of life among people living with HIV/AIDS in northern Thailand [article]. Aids Care-Psychological and Socio-Medical Aspects of Aids/Hiv, 18(2), 128–132.
Jia, H. G., Uphold, C. R., Wu, S., Reid, K., Findley, K., & Duncan, P. W. (2004). Health-related quality of life among men with HIV infection: Effects of social support, coping, and depression [article]. Aids Patient Care and STDS, 18(10), 594–603.
Karki, S. (2008). HIV/Aids situation in Nepal: Transition to women (Master thesis), Linkoping University, Sweden.
Klein, K., Armistead, L., Devine, D., Kotchick, B., Forehand, R., Morse, E., et al. (2000). Socioemotional support in African American families coping with maternal HIV: An examination of mothers’ and children’s psychosocial adjustment [article]. Behavior Therapy, 31(1), 1–26.
Koopman, C., Gore-Felton, C., Marouf, F., Butler, L. D., Field, N., Gill, M., et al. (2000). Relationships of perceived stress to coping, attachment and social support among HIV-positive persons [article]. Aids Care-Psychological and Socio-Medical Aspects of Aids/Hiv, 12(5), 663–672.
Kucera, K. A. (1998). Case management of the HIV/AIDS client [review]. Journal of Case Management, 7(2), 62–66.
Kuyken, W., Orley, J., Power, M., Herrman, H., Schofield, H., Murphy, B., et al. (1995). The world health organization quality of life assessment (WHOQOL): Position paper from the world health organization. Social Science and Medicine, 41(10), 1403–1409.
Kylma, J. (2005). Despair and hopelessness in the context of HIV: A meta-synthesis on qualitative research findings [article]. Journal of Clinical Nursing, 14(7), 813–821.
Kylma, J., Vehvilainen-Julkunen, K., & Lahdevirta, J. (2003). Dynamics of hope in HIV/AIDS affected people: An exploration of significant others’ experiences. Research and Theory for Nursing Practice, 17(3), 191–205.
Leserman, J., Perkins, D. O., & Evans, D. L. (1992). Coping with the threat of AIDS: The role of social support. American Journal of Psychiatry, 149(11), 1514–1520.
Miller, J. F. (1989). Hope-inspiring strategies of the critically ill. Applied Nursing Research, 2(1), 23–29.
Nama, S. L., Fielding, K., Avalos, A., Dickinson, D., Gaolathe, T., & Geissler, P. W. (2008). The relationship of acceptance or denial of HIV-status to antiretroviral adherence among adult HIV patients in urban Botswana (vol 67, pg 301, 2008). Social Science and Medicine, 67(11), 1934.
Ncama, B. P., McInerney, P. A., Bhengu, B. R., Corless, I. B., Wantland, D. J., Nicholas, P. K., et al. (2008). Social support and medication adherence in HIV disease in KwaZulu-Natal, South Africa [article]. International Journal of Nursing Studies, 45(12), 1757–1763.
Nunes, J. A., Raymond, S. J., Nicholas, P. K., Leuner, J. D., & Webster, A. (1995). Social support, quality of life, immune function, and health in persons living with HIV. Journal of Holistic Nursing, 13(2), 174–198.
Phillips, K. D., & Sowell, R. L. (2000). Hope and coping in HIV-infected African-American women of reproductive age [research support, non-US gov’t]. Journal of National Black Nurses Association, 11(2), 18–24.
Rabkin, J. G., Remien, R., Katoff, L., & Williams, J. B. W. (1993). Resilience in adversity among long-term survivors of AIDS. Hospital & Community Psychiatry, 44(2), 162–167.
Rawls, A. W. (1997). Durkheim’s epistemology: The initial critique, 1915–1924. Sociological Quarterly, 38(1), 111–145.
Remor, E. (2002). Social support and quality of life in the HIV infection [comparative study; english abstract; research support, non-US gov’t]. Atencion Primaria, 30(3), 143–148.
Sarason, I. G., Levine, H. M., Basham, R. B., & Sarason, B. R. (1983). Assessing social support: The social support questionnaire [article]. Journal of Personality and Social Psychology, 44(1), 127–139.
Saxena, S., Chandiramani, K., & Bhargava, R. (1998). WHOQOL-Hindi: A questionnaire for assessing quality of life in health care settings in India [article]. National Medical Journal of India, 11(4), 160–165.
Shippy, R. A. (2007). Taking care of each other. GMHC Treat Issues, 21(2), 7–8.
Srisurapanont, M., Sambatmai, S., & Jarusuraisin, N. (2001). HIV-seropositive results, health-related quality of life, and social support: A 24-week prospective study in Thailand [article]. Aids Patient Care and STDS, 15(4), 211–215.
Strine, T. W., Chapman, D. P., Balluz, L., & Mokdad, A. H. (2008). Health-related quality of life and health behaviors by social and emotional support. Their relevance to psychiatry and medicine. Social Psychiatry and Psychiatric Epidemiology, 43(2), 151–159.
Swindells, S., Mohr, J., Justis, J. C., Berman, S., Squier, C., Wagener, M. M., et al. (1999). Quality of life in patients with human immunodeficiency virus infection: Impact of social support, coping style and hopelessness [article]. International Journal of STD and AIDS, 10(6), 383–391.
Vaux, A., & Harrison, D. (1985). Support network characteristics associated with support satisfaction and perceived support. American Journal of Community Psychology, 13(3), 245–268.
Wethington, E., & Kessler, R. C. (1986). Perceived support, received support, and adjustment to stressful life events [article]. Journal of Health and Social Behavior, 27(1), 78–89.
Yang, M.-H., Chen, Y.-M., Kuo, B. I.-T., & Wang, K.-Y. (2003). Quality of life and related factors for people living with HIV/AIDS in Northern Taiwan. The Journal of Nursing Research, 11(3), 217–226.
Zich, J., & Temoshok, L. (1987). Perceptions of social support in men with AIDS and ARC-relationship with distress and hardiness. Journal of Applied Social Psychology, 17(3), 193–215.
Acknowledgments
The study was funded by Nagoya University (Japan) under the Global Practicum Program 2008–2009. I would like to thank all the participants in this study and acknowledge the following contributors to the field survey: Mr. Arun Sah, Mr. kshitij Gartaulla, Mr. Sanjeev Parajuli, Miss Isha K.C, Mr. Madhav Adhikari, and Mrs. Parbata Panday. I also thank Professor Yoshihiko Nishimura and Professor Yoshiaki Nishikawa for their valuable guidance for developing framework for this research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yadav, S. Perceived social support, hope, and quality of life of persons living with HIV/AIDS: a case study from Nepal. Qual Life Res 19, 157–166 (2010). https://doi.org/10.1007/s11136-009-9574-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-009-9574-z