
Abstract
Purpose
To define and understand patient psychological insulin resistance (PIR) and its impact on diabetes management.
Methods
Systematic literature review of peer-refereed journals using the MEDLINE database, including all articles in English from 1985 to 2007. The population included patients with type 1 and type 2 diabetes, insulin naïve, and those currently using insulin. A total of 116 articles were reviewed.
Results
PIR is impacted by patients’ beliefs and knowledge about diabetes and insulin, negative self-perceptions and attitudinal barriers, the fear of side effects and complications from insulin use, as well as lifestyle adaptations, restrictions required by insulin use, and social stigma. These etiological influences, both independently and in combination, constitute a patient’s PIR and may result in the reluctance of patients to both initiate and intensify treatment, leading to delayed treatment initiation and compromised glucose control.
Conclusions
PIR is complex and multifaceted. It plays an important, although often ignored, role in diabetes management. Assisting health care professionals in better understanding PIR from the patient’s perspective should result in improved treatment outcomes. By tailoring treatments to patients’ PIR, clinicians may be better able to help their patients begin insulin treatment sooner and improve compliance, thus facilitating target glycemic control.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Historically, insulin has been an underutilized “last resort” option in diabetes management. However, it is becoming increasingly valued because of its ability to promote appropriate levels of glycemic control, lower risk of long-term complications, and no significant negative effect on the patient’s quality of life [1–5]. “Unfortunately, it (insulin) is not used early enough, often enough, or aggressively enough to allow patients to achieve glycemic goals proven to reduce morbidity and mortality” [6]. The initiation of insulin therapy is often one of the most difficult and important choices that individuals with diabetes have to make. Because insulin use often involves negative perceptions, both the decision and the therapy may present an emotional and logistical hurdle, leading to patient resistance to treatment [7–9].
Psychological insulin resistance (PIR) can be defined as psychological opposition towards insulin use in both people with diabetes and their prescribers. PIR is a multifaceted concept encompassing psychological factors and the complex interaction of these factors when a person faces the decision to start insulin treatment and/or comply with ongoing treatment [10]. PIR represents a complex set of beliefs about the meaning of insulin therapy, poor self-efficacy concerning the skills needed for insulin therapy, fear of injections, and a lack of accurate information [11]. These beliefs can be influenced by past experiences, the attitudes of others, participants’ perceptions of their diabetes, and their understanding of the disease process [12].
Given that more than 50% of people with diabetes are on insulin [13], and the reality that insulin is the most potent drug available to achieve glycemic targets [6], one might assume that insulin initiation or compliance would not be a major clinical issue. In reality, PIR is not an uncommon factor—it is one that negatively influences both the initiation of and compliance with insulin treatment. A majority of insulin-naïve diabetes patients have been shown to believe that insulin will not make a positive difference in their overall health [14], and as many as 73% of type 2 patients beginning a diabetes education program where insulin was to be started were reluctant to do so at first [15]. Forty percent (40%) of insulin-naïve patients do not believe that insulin therapy will help them achieve good glycemic control or improve their prognosis [16]. Further, when examining the willingness of type 2 insulin-naïve diabetes patients to begin insulin if prescribed, it was found that negative attitudes toward insulin were common, with a mean of 3.1 negative beliefs identified per subject [11].
In addition to PIR impacting both the initiation to and compliance with insulin treatment, it may also influence the physical, social, and psychological aspects of quality of life, as well as treatment satisfaction. Sub-optimal glycemic control leads to an increased health burden, which, in turn, may result in a reduced ability to engage in activities and actions that are important to quality of life. Thus, long-term clinical treatment goals may be jeopardized due to short-term patient PIR concerns. Treatment satisfaction, which is a delicate balance between patient-perceived treatment efficacy, burden, and side effects, is also directly impacted by PIR, as these beliefs influence perceptions of satisfaction. For example, PIR due to the fear of weight gain is likely to increase a patient’s psychological and treatment burden and, in turn, may reduce treatment satisfaction.
Unfortunately, even though patient PIR is common, physicians may feel unable to manage their patients’ psychological needs by helping them deal with the fear and anxiety felt about their diabetes and its treatment. Less than half of health care professionals interviewed in the Diabetes Attitudes, Wishes and Needs (DAWN) study felt that they were able to identify and evaluate their patients’ psychological needs [17].
The purpose of this paper is to report the findings of a systematic literature review of peer-refereed journal articles related to defining and understanding patient PIR and its impact on diabetes management. The goal of this research is to assist clinicians in addressing PIR issues with their patients and identifying the optimal insulin treatment for a given patient.
Methods
The literature search was conducted using the US National Library of Medicine’s MEDLINE database. The search included all articles published in English, the first author’s native language, beginning in 1985 and ending in 2007. The goal was to represent the relevant historical and current literature. Cross reference searching using references from the reviewed articles, PubMed, and Google searches was then conducted for additional articles. The search was stopped when saturation of new information was reached and additional searches were not identifying new articles. The keywords and phrases used for the search were: PIR, resistance to insulin therapy, insulin side effects/complications, reluctance to treat diabetes, treatment refusal, barriers to insulin compliance, switching to insulin therapy, racial/ethnic/cultural/gender issues/barriers initiating insulin, patient reluctance insulin, psychological adjustment diabetes/insulin, needle/injection anxiety/phobia/fear, psychological issues diabetes, psycho-social aspects diabetes treatment, patient perceptions, acceptance/adherence insulin, and patient preference insulin. No limitations regarding the type of study design (qualitative, quantitative, and review articles included) were imposed on the search. The study population included patients with type 1 and type 2 diabetes, insulin-naïve, and those currently using insulin. A total of 109 articles were reviewed and the information was qualitatively synthesized according to groupings (e.g., lifestyle adaptations, cultural factors, attitudinal barriers) that emerged as repetitive concepts during the review process (Fig. 1).

Literature selection decision tree
Results
Defining and understanding the full continuum of PIR components
The synthesis of the literature revealed that resistance to initiate insulin or comply with insulin treatment over time may be impacted by patients’ beliefs and knowledge about diabetes and insulin; negative self-perceptions and attitudinal barriers (sense of personal failure or self-blame for the necessity of insulin use, fear of injection); the fear of side effects and complications from insulin use; as well as lifestyle adaptations, restrictions required by insulin use, and social stigma. These etiological influences, whether independently or in combination, constitute a patient’s PIR.
Beliefs and knowledge about diabetes and insulin
Lack of knowledge about diabetes and insulin therapy or erroneous beliefs and misconceptions about the disease and treatment contribute to PIR. For example, some patients believe that insulin, rather than diabetes, causes serious health problems and severe or chronic complications, such as amputation, heart attack, or possibly blindness and even death [1, 8, 18–21].
Patients may also perceive that insulin is for more severe disease [14] and/or that insulin initiation means that they are becoming “more ill,” their disease has dramatically progressed and become more serious, or that they are at the “end of the road” [1, 11, 19, 21–26].
Negative self-perceptions and attitudinal barriers
PIR may be the result of a sense of personal failure or self-blame about the need for insulin treatment. This sense of failure may be the result of feeling that insulin is required because they have “failed” other therapies or failed to control their disease [10, 12, 19] by not properly caring for themselves [1, 23], or being able to self-manage their disease with diet, exercise, or oral medications alone [11]. This sense of personal failure may leave the patient with feelings of failure and guilt [22] and a belief that they will be unable to control the disease in the future, regardless of treatment, and that insulin will not be effective and will not make a positive difference to their overall health [14, 20, 24, 25, 27]. Insulin may also be perceived as a threat or punishment, resulting in anger or betrayal, because patients may feel unfairly punished for poor self-care [12, 28]. Additional negative self-perceptions and attitudinal barriers that may play a part in PIR include: wishful thinking that insulin is not necessary, procrastination regarding treatment [21], the belief that people treat insulin users differently [19], that they are no longer “normal,” that they are now dependent or like a drug addict [12, 29], or that they are inadequately educated or ill-equipped to handle the daily demands of insulin therapy [28].
The attitudinal barrier “fear of injections” consists of multiple components that may result in PIR, including: technical concerns, fear that injections will be painful, fear of inflicting self-harm, fear of self-injecting or dislike of daily injections, general anxiety, and needle phobia. Specifically, technical concerns have been shown to include: anxiety about mastering the skill of giving oneself an injection, the general hassle of taking injections [8, 12], concern about preparing the correct dose of insulin [30], apprehension about the proper technique of needle injection [23], poor self-efficacy, concerns about skills related to administering an injection [31], as well as a general lack of confidence regarding the ability to handle the demands of insulin therapy/regimen [24, 25]. Anticipated fear that the injections may be painful also contributes to a general anxiety about injections [18–20, 22–25, 29]. Additionally, some patients believe that self-injecting insulin is unnatural [12]. These fears regarding self-injection, either independently or in combination, may result in a general injection-related anxiety and/or needle phobia [6, 9, 14, 32]. Although clinical needle phobia is rare (1%) [33], needle “resistance” or “discomfort” has been shown to be common with self-injectable treatments [34].
Lifestyle adaptations and restrictions
Patients may have concerns that insulin adds to the burden and stress that they already experience from managing diabetes on a daily basis [28], and do not feel confident that they can handle the day-to-day demands of insulin therapy [11]. Fears, perceived or real, that insulin therapy will be a source of inconvenience and cause a loss of personal freedom [8, 10, 21, 23] that will severely restrict their lives and be too inconvenient, time-consuming, and complex to manage [1, 6, 11, 19, 24, 25] may also facilitate PIR. Insulin treatment has been associated with a perceived loss of control over one’s life [14, 27], and as a daily restriction that takes over one’s life [12], resulting in a sense of powerlessness [12] and adversely affecting independence and lifestyle [20, 22].
Fear of side effects/complications
Patients may experience PIR as the result of misconceptions regarding their disease, so that they attribute complications of diabetes to insulin use rather than insufficient glycemic control [1, 6, 8, 19–21]. In addition to misconceptions regarding complications, patients also worry about potential side effects and complications, such as weight gain, hypoglycemia, and cardiovascular risk, which may be due to insulin use [8, 11, 19–22, 24–26, 32, 35, 36].
Hypoglycemia and weight gain are the most common side effects leading to PIR. The anticipation of weight gain with insulin therapy and the discipline needed to compensate for it are psychological burdens that can cause negative feelings toward insulin therapy [32, 37]. For those who are already overweight and have a poor cardiovascular risk profile, the prospect of further weight gain can, therefore, be a major barrier to both the initiation and the intensification of insulin for both patients and health care providers [30]. Intentional insulin omission was found in approximately one third of women of all ages with type 1 diabetes [37, 38], with approximately half of the respondents reporting omitting insulin for weight-management purposes [38]. Insulin omission for weight control was frequent among women and may contribute to poor glycemic control and the risk of complications [37]. In addition, increased weight in type 2 diabetes is associated with increased insulin resistance, so weight gain may even compromise the efficacy of treatment [39], thus further reinforcing the belief that insulin is not good for one’s health, and strengthening PIR.
Fear of hypoglycemia can also be a major barrier to achieving optimal glycemic control [40]. Hypoglycemia can give rise to high insecurity; even if one is emotionally prepared for the complication, the thought of future episodes can cause fearful and disturbed feelings. In the attempt to avoid episodes, people with diabetes may modify their maintenance of glycemic levels “not to suppress the blood glucose to avoid hypoglycemia,” especially during work or school hours [41].
Social stigma
Social stigma or discomfort related to treatment for diabetes is the fear, perception, or reality of public misunderstanding about the treatment and/or the nature of diabetes as a chronic disease [42]. It is a major component of treatment satisfaction in diabetes [43]. Given that injectable insulin is the most common delivery system for insulin treatment, it is not surprising that social stigma plays a key role in PIR because vials and syringes carry a strong negative connotation [6, 23] and are usually identified with either intravenous drug addicts or severe illness [22, 42]. The necessity of using syringes in a public place may result in feelings of social embarrassment [22] and social rejection [10]. In addition, it may be inconvenient and frustrating, as persons with diabetes often believe that they have to hide their injections to avoid disturbing other people [44]. Additionally, there may be fears on the part of the patient that the use of syringes would damage their relationships with significant others [18] or that taking insulin will result in family members and friends treating them differently [19]. Thus, the fear of social stigma when injecting in public may impact adherence to treatment, as the absence of a private area in which to inject may result in either injecting too early or, in some cases, the omission of an injection [30].
Patients’ perceptions of social stigma for the self-injection of insulin in public can have a restrictive effect on disease-management efforts. The consequence of previous negative experiences, or fear of negative experience, may lead to a lack of motivation due to the inconvenience and embarrassment related to injections [44], patients selecting suboptimal locations to inject themselves while away from home, such as in public toilets, and may also cause some patients to delay injections and avoid social activities [42]. Ultimately, patients’ understanding of and adherence to appropriate diabetes self-management practices may not translate into practice if the perception of social stigma is prevalent [42].
PIR and diabetes management
For any treatment to be optimally efficacious, it must be initiated, be properly dose-adjusted over time, and treatment compliance must be achieved. PIR may be one of the major etiologies explaining both the reluctance of patients to initiate and to intensify treatment [30, 45, 46]. The problems of starting insulin have a more immediate impact and are generally obvious to both clinician and patient. The problems of not initiating or delaying insulin treatment are more remote and may be less obvious to a patient—the progressive increase in the risk of diabetes-related complications [26]. Reluctance to initiate insulin therapy in a timely manner contributes to prolonged periods of poor glycemic control among individuals with diabetes and, ultimately, increases the risk for neuropathic, microvascular, and macrovascular complications [30]. Non-compliance with ongoing insulin treatment presents its own consequences of poor glycemic control and increased risk of complications [36].
PIR at the initiation of insulin treatment is not uncommon, although estimates of its prevalence vary. However, there is growing evidence that some patients refuse to start insulin treatment, despite suboptimal glucose control [47]. A majority of insulin-naïve patients have reported that they were either unwilling (28.2%) or only slightly willing (24.0%) to initiate insulin if prescribed [11]. In a clinical trial of type 2 patients randomized to insulin therapy, 27% initially refused treatment [48]. Further, 73% of type 2 patients beginning a diabetes education program where insulin was to be started were reluctant to do so at first [15].
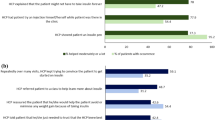
Physicians’ perceived attitudes at the time of diagnosis may be critical to patients’ views about the seriousness of diabetes and their subsequent self-management behavior [49]. Attitudes toward insulin therapy are influenced by patients’ interactions with health professionals, as well as personal experiences, observations, and what others say [8]. In a study of elderly type 2 patients, the main factor (70%) explaining the intention towards insulin treatment was shown to be the opinion of important other persons, especially the treating internist, the family physician, and the diabetes nurse [31]. The patient and provider relationship’s influence on the level of fear of injecting may be particularly strong on the day that patients come in to start insulin. This fear may be exacerbated by patient’s anxieties about revealing their fear to the attending physician [12].
All components of PIR can interfere not only with the initiation of insulin treatment, but also with attempts to intensify and increase compliance with insulin therapy in individuals who are already using insulin [21, 30]. Fewer than one in five people with diabetes (19.4% Type 1 and 16.2% Type 2) reported they complied fully with all aspects of their prescribed regimens [50]. In a study of women with “insulin-dependent diabetes,” poor compliance resulting in insulin omission was linked to disordered eating, poorer glycemic control, more diabetes-related hospitalizations, greater psychological distress (general and diabetes-specific), greater fear of hypoglycemia, higher rates of retinopathy and neuropathy, poorer regimen adherence, and greater fears concerning improved diabetes management, which may lead to weight gain [38].
Although it is clear that the components of PIR influence whether a patient initiates treatment at the optimal time, rather than delaying treatment, and is then compliant with treatment, the relative importance of a given PIR etiological influence may vary depending upon where the patient is in the treatment process. Additionally, the ranking of the various components of PIR in patients who have not begun insulin treatment may differ significantly from factors influencing those already on insulin. For example, for insulin-naïve patients, the perception of how many injections per day will be needed may be a negative influence, whereas insulin-experienced patients are impacted less by the frequency of injections and place more value on improving their glucose control [51]. Further, interviews with patients about barriers that hinder the transition to insulin treatment in insulin-naïve patients compared to ongoing insulin-treated patients found that, for insulin-naïve patients, the belief that diabetes was not a very serious illness was the primary barrier to insulin therapy, whereas it was one of the least important barriers for those already on insulin (47% vs. 7%, P ≤ 0.0001). The primary barriers for insulin-naïve patients were fears associated with the injections (24% vs. 11% for insulin-naïve, P = 0.009), fears of addiction (39% vs. 21%, P = 0.009), and fear of hypoglycemia (12% vs. 4%, P = 0.05) [29].
Implications of new insulin treatments for PIR
There are now new modern insulin analogs and more discreet delivery systems (pen, inhaled, pump) available or under development which have the potential to decrease PIR and improve treatment outcomes. These treatment advances may help to eliminate or reduce many of the key factors that contribute to PIR, namely, social stigma, lifestyle adaptations, and fear of side effects.
The use of a new pen system may help patients to overcome the issues of social stigma and the social embarrassment/comfort issues that are commonly associated with using a vial and syringe in public. A recent literature review concluded that insulin pen devices are discreet and offer patients convenience and flexibility [52]. These pen features may give patients the confidence to overcome issues of needle anxiety and the social embarrassment associated with self-injection and, therefore, may lead to improved adherence to recommended insulin dosing schedules and compliance with multiple-injection regimens. Pen systems may also help to overcome problems with insulin dosing errors and low adherence. This was recently demonstrated in a study of patients with type 2 diabetes treated in a managed care setting who switched from the administration of insulin by vial/syringe to a pre-filled insulin pen device (FlexPen®). Following the switch, the patients demonstrated improved medication adherence, fewer claims for hypoglycemic events, reduced emergency department and physician visits, and lower annual treatment costs [53]. Similarly, the insulin pump may help to reduce PIR. People who use insulin pumps are said to enjoy increased discretion in daily living patterns compared to those using other forms of insulin administration [54]. The insulin pump has been reported by users as being more “convenient” for self-care, expressed in terms of having greater “flexibility” and “freedom” [55].
The faster onset to action of modern rapid-acting insulin analogs (such as insulin aspart, insulin lispro, or insulin glulisine) may also reduce PIR. These new rapid-acting insulins can be taken together with food instead of waiting the 30 min required for regular human insulin. Therefore, it is not necessary to carefully plan the timing of pre-prandial insulin treatment in relationship to meals, thus, reducing lifestyle adaptations and restrictions.
Regarding side effects, the incidence of hypoglycemia is reduced using modern long-acting insulin analogs (insulin detemir and insulin glargine) compared with human intermediate-acting insulin (NPH insulin) [56–59]. Moreover, one of the new modern long-acting insulin analogs (insulin detemir) has also been found to be superior to human NPH insulin in relation to weight gain [57, 58, 60, 61].
Discussion
Given the significant influence of PIR on diabetes outcomes, there is a clinical imperative to understand the full spectrum of etiological factors that may either independently or in combination result in PIR. Assisting health care professionals to better understand the complex and multifaceted aspects of PIR from the patients’ perspective should result in improved insulin treatment outcomes. Key components of PIR, such as social stigma, lifestyle changes, and fear of side effects, should be addressed and discussed when initiating patients on insulin. Health care professionals can facilitate the acceptance of insulin by employing strategies to help patients overcome psychological barriers to insulin therapy [62]. Clinicians should directly address PIR concerns with patients at the time of considering insulin initiation, as well as over the course of treatment. Revisiting PIR issues with patients during treatment is critical, as the relative importance of a given PIR component may vary over time and be influenced by changes in the treatment regime. By tailoring treatments to patients’ PIR, clinicians may be better able to help their patients begin insulin treatment sooner and improve compliance, thus, facilitating target glycemic control. Modern insulin analogs and pen systems offer the promise of novel insulin treatment with improved technological features. However, the important task of addressing and discussing PIR with patients remains the clinician’s responsibility.
The task of understanding the impact of the multifaceted components of PIR is made even more challenging by the realization that factors such as gender, socio-economic status, and cultural differences are likely barriers in the acceptance and mastery of insulin treatment [17]. For example, limited reimbursement for pharmacy costs or difficulty with access to health care may negatively impact patients’ ability to care for themselves and their diabetes appropriately [18, 63]. Women have been found to be more unwilling than men (32.0% vs. 21.1%; P < 0.001) to initiate insulin therapy [11]. In a small sample, it was shown that women are also more likely to perceive insulin as punishment, whereas men view insulin more as a form of treatment that may help them [12].
This paper has focused on the patient PIR and its impact on treatment. However, it is important to remember that physicians have also been shown to experience PIR for their patients and just over half of physicians and nurses agree that insulin can have a positive impact on care [64]. Physician attitudes, such as doubts about a patient’s compliance with treatment, fears of hypoglycemia or weight status, expectations that patients would not cope with repeated blood tests, impressions based on previous physician experience with insulin, concerns about the patient’s age, and the perception that the disease is so severe that even insulin would not help the patient, have all been reported as physician barriers to initiating treatment [29].
Conclusion
Reducing the negative influence of psychological insulin resistance (PIR) on treatment outcomes should be a clinical priority. Appreciating and understanding the multifaceted and complex nature of PIR and discussing the etiology of a given patient’s PIR is an important first step. The incorporation of well-validated clinical measures assessing PIR, as well as further research on the impact of interventions to reduce PIR, are essential. Based on this information, clinicians can help patients overcome their PIR by working together to establish self-sufficiency and increase patients’ sense of control over their lives [14]. Clinicians should emphasize the simplicity of the treatment in order to decrease their patients’ fear of dependency on insulin and its consequent disruption of their way of life [28]. Tailoring insulin treatment modalities, such as the use of modern insulin analogs and insulin pen devices, may greatly reduce PIR by mitigating the fear of lifestyle changes and side effects, as well as the social stigma associated with using insulin in a vial and syringe.
Abbreviations
- PIR:
-
Psychological insulin resistance
References
Brunton, S. A., Davis, S. N., & Renda, S. M. (2006). Overcoming psychological barriers to insulin use in type 2 diabetes. Clinical Cornerstone, 8(Suppl 2), S19–S26. doi:10.1016/S1098-3597(06)80012-8.
Riddle, M. C. (2002). The underuse of insulin therapy in North America. Diabetes/Metabolism Research and Reviews, 18, S42–S49. doi:10.1002/dmrr.277.
United Kingdom Prospective Diabetes Study (UKPDS) Group. (1995). Overview of 6 years’ therapy of type II diabetes: A progressive disease (UKPDS 16). Diabetes, 44, 1249–1258. doi:10.2337/diabetes.44.11.1249.
United Kingdom Prospective Diabetes Study (UKPDS) Group. (1998). Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet, 352, 837–853. doi:10.1016/S0140-6736(98)07019-6.
United Kingdom Prospective Diabetes Study (UKPDS) Group. (1999). Quality of life in type 2 diabetic patients is affected by complications but not by intensive policies to improve blood glucose or blood pressure control (UKPDS 37). Diabetes Care, 22, 1125–1136. doi:10.2337/diacare.22.7.1125.
Meece, J. (2006). Dispelling myths and removing barriers about insulin in type 2 diabetes. The Diabetes Educator, 32, 9S–18S. doi:10.1177/0145721705285638.
Fitzgerald, J. T., Gruppen, L. D., Anderson, R. M., Funnell, M. M., Jacober, S. J., Grunberger, G., et al. (2000). The influence of treatment modality and ethnicity on attitudes in type 2 diabetes. Diabetes Care, 23, 313–318. doi:10.2337/diacare.23.3.313.
Hunt, L. M., Valenzuela, M. A., & Pugh, J. A. (1997). NIDDM patients’ fears and hopes about insulin therapy. The basis of patient reluctance. Diabetes Care, 20(3), 292–298. doi:10.2337/diacare.20.3.292.
Zambanini, A., Newson, R. B., Maisey, M., & Feher, M. D. (1999). Injection related anxiety in insulin-treated diabetes. Diabetes Research and Clinical Practice, 46(3), 239–246. doi:10.1016/S0168-8227(99)00099-6.
Bogatean, M. P., & Hâncu, N. (2004). People with type 2 diabetes facing the reality of starting insulin therapy: Factors involved in psychological insulin resistance. Practical Diabetes International, 21(7), 247–252. doi:10.1002/pdi.670.
Polonsky, W. H., Fisher, L., Guzman, S., Villa-Caballero, L., & Edelman, S. V. (2005). Psychological insulin resistance in patients with type 2 diabetes: The scope of the problem. Diabetes Care, 28(10), 2543–2545. doi:10.2337/diacare.28.10.2543.
Morris, J. E., Povey, R. C., & Street, C. G. (2005). Experiences of people with type 2 diabetes who have changed from oral medication to self-administered insulin injections. Practical Diabetes International, 22(7), 239–243. doi:10.1002/pdi.829.
Centers for Disease Control and Prevention (CDC). (2008). National Center for Health Statistics, Division of Health Interview Statistics, data from the National Health Interview Survey. Age-adjusted percentage of adults with diabetes using diabetes medication, by type of medication, United States, 1997–2003. Data computed by personnel in the Division of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Available online at: http://www.cdc.gov/diabetes/statistics/meduse/table2.htm.
Polonsky, W. H., & Jackson, R. A. (2004). What’s so tough about taking insulin? Addressing the problem of psychological insulin resistance in type 2 diabetes. Clinical Diabetes, 22, 147–150. doi:10.2337/diaclin.22.3.147.
Okazaki, K., Goto, M., Yamamoto, T., Tsujii, S., & Ishii, H. (1999). Barriers and facilitators in relation to starting insulin therapy in type 2 diabetes [abstract]. Diabetes, 48, A1319.
Snoek, F. J., Skovlund, S. E., & Pouwer, F. (2007). Development and validation of the insulin treatment appraisal scale (ITAS) in patients with type 2 diabetes. Health and Quality of Life Outcomes, 5, 69. doi:10.1186/1477-7525-5-69.
Alberti, G. (2002). The DAWN (Diabetes Attitudes, Wishes and Needs) study. Practical Diabetes International, 19(1), 22a–24a. doi:10.1002/pdi.305.
Haque, M., Emerson, S. H., Dennison, C. R., Navsa, M., & Levitt, N. S. (2005). Barriers to initiating insulin therapy in patients with type 2 diabetes mellitus in public-sector primary health care centres in Cape Town. South African Medical Journal, 95(10), 798–802.
Rubin, R. R., & Peyrot, M. (2001). Psychological issues and treatments for people with diabetes. Journal of Clinical Psychology, 57, 457–478. doi:10.1002/jclp.1041.
Funnell, M. M. (2007). Overcoming barriers to the initiation of insulin therapy. Clinical Diabetes, 25, 36–38. doi:10.2337/diaclin.25.1.36.
Peragallo-Dittko, V. (2007). Removing barriers to insulin therapy. The Diabetes Educator, 33, 60S–65S. doi:10.1177/0145721707301210.
Leslie, C. A., Satin-Rapaport, W., Matheson, D., Stone, R., & Enfield, G. (1994). Psychological insulin resistance: A missed diagnosis? Diabetes Spectrum, 7, 52–57.
Ho, E. Y., & James, J. (2006). Cultural barriers to initiating insulin therapy in Chinese people with type 2 diabetes living in Canada. Canadian Journal of Diabetes, 30(4), 390–396.
Kruger, D. F. (2007). The other “insulin resistance”: Overcoming barriers to insulin use and encouraging diabetes self-management. The Diabetes Educator, 33, 80S–81S. (Intro.).
Kruger, D. F. (2007). Tying it all together: Matching insulin regimens to individual patient needs. The Diabetes Educator, 33, 91S–95S. doi:10.1177/0145721707302060.
Phillips, P. (2005). Type 2 diabetes—Failure, blame and guilt in the adoption of insulin therapy. The Review of Diabetic Studies: RDS, 2(1), 35–39. doi:10.1900/RDS.2005.2.35. Epub May 10, 2005.
Davis, S. N., & Renda, S. M. (2006). Psychological insulin resistance: Overcoming barriers to starting insulin therapy. The Diabetes Educator, 32, 146S–152S. doi:10.1177/0145721706289226.
Funnell, M. M., Kruger, D. F., & Spencer, M. (2004). Self-management support for insulin therapy in type 2 diabetes. The Diabetes Educator, 30, 274–280. doi:10.1177/014572170403000220.
Nakar, S., Yitzhaki, G., Rosenberg, R., & Vinker, S. (2007). Transition to insulin in Type 2 diabetes: Family physicians’ misconceptions of patients’ fears contributes to existing barriers. Journal of Diabetes and its Complications, 21(4), 220–226. doi:10.1016/j.jdiacomp.2006.02.004.
Korytkowski, M. (2002). When oral agents fail: Practical barriers to starting insulin. International Journal of Obesity and Related Metabolic Disorders, 26(Suppl 3), S18–S24. doi:10.1038/sj.ijo.0802173.
Wolffenbuttel, B. H., Drossaert, C. H., & Visser, A. P. (1993). Determinants of injecting insulin in elderly patients with type II diabetes mellitus. Patient Education and Counseling, 22(3), 117–125. doi:10.1016/0738-3991(93)90091-A.
Stotland, N. L. (2006). Overcoming psychological barriers in insulin therapy. Insulin, 1, 38–45. doi:10.1016/S1557-0843(06)80006-0.
Snoeck, F. J. (2001). Psychological insulin resistance. Diabetes Voice, 46(3), 27–28.
Brod, M., Hoomans, E. H. M., & Wiebinga, C. J. (2007). Understanding the impact of controlled ovarian stimulation (COS) on women’s functioning and well-being. Annual meeting of the European Society for Human Reproductive Endocrinology, Lyon, France. Poster presentation.
Carver, C. (2006). Insulin treatment and the problem of weight gain in type 2 diabetes. The Diabetes Educator, 32(6), 910–917. doi:10.1177/0145721706294259.
Delahanty, L. M., Grant, R. W., Wittenberg, E., Bosch, J. L., Wexler, D. J., Cagliero, E., et al. (2007). Association of diabetes-related emotional distress with diabetes treatment in primary care patients with Type 2 diabetes. Diabetic Medicine, 24(1), 48–54. doi:10.1111/j.1464-5491.2007.02028.x.
Bryden, K. S., Neil, A., Mayou, R. A., Peveler, R. C., Fairburn, C. G., & Dunger, D. B. (1999). Eating habits, body weight, and insulin misuse. A longitudinal study of teenagers and young adults with type 1 diabetes. Diabetes Care, 22(12), 1956–1960. doi:10.2337/diacare.22.12.1956.
Polonsky, W. H., Anderson, B. J., Lohrer, P. A., Aponte, J. E., Jacobson, A. M., & Cole, C. F. (1994). Insulin omission in women with IDDM. Diabetes Care, 17, 1178–1185. doi:10.2337/diacare.17.10.1178.
Albu, J., & Raja-Khan, N. (2003). The management of the obese diabetic patient. Primary Care: Clinics in Office Practice, 30(2), 465–491. doi:10.1016/S0095-4543(03)00043-5.
Saleh, M., & Grunberger, G. (2001). Hypoglycemia: An excuse for poor glycemic control? Clinical Diabetes, 19(4), 161–167. doi:10.2337/diaclin.19.4.161.
Shiu, A. T., & Wong, R. Y. (2002). Fears and worries associated with hypoglycaemia and diabetes complications: Perceptions and experience of Hong Kong Chinese clients. Journal of Advanced Nursing, 39(2), 155–163. doi:10.1046/j.1365-2648.2002.02255.x.
Shiu, A. T., Kwan, J. J., & Wong, R. Y. (2003). Social stigma as a barrier to diabetes self-management: Implications for multi-level interventions. Journal of Clinical Nursing, 12(1), 149–150. doi:10.1046/j.1365-2702.2003.00735.x.
Cappelleri, J. C., Gerber, R. A., Kourides, I. A., & Gelfand, R. A. (2000). Development and factor analysis of a questionnaire to measure patient satisfaction with injected and inhaled insulin for type 1 diabetes. Diabetes Care, 23, 1799–1803. doi:10.2337/diacare.23.12.1799.
Hayes, R. P., Bowman, L., Monahan, P. O., Marrero, D. G., & McHorney, C. A. (2006). Understanding diabetes medications from the perspective of patients with type 2 diabetes: Prerequisite to medication concordance. The Diabetes Educator, 32(3), 404–414. doi:10.1177/0145721706288182.
Siddiqui, N. I. (2007). Evaluation of inhaled insulin therapy for diabetes mellitus. Mymensingh Medical Journal, 16(2), 237–245.
Jani, R., Triplitt, C., Reasner, C., & Defronzo, R. A. (2007). First approved inhaled insulin therapy for diabetes mellitus. Expert Opinion on Drug Delivery, 4(1), 63–76. doi:10.1517/17425247.4.1.63.
Mudaliar, S. (2007). Inhaled insulin using AERx insulin diabetes management system (AERx iDMS). Expert Opinion on Investigational Drugs, 16(10), 1673–1681. doi:10.1517/13543784.16.10.1673.
United Kingdom Prospective Diabetes Study (UKPDS) Group. (1995). Relative efficacy of randomly allocated diet, sulphonylurea, insulin, or metformin in patients with newly diagnosed non-insulin dependent diabetes followed for three years. British Medical Journal, 310, 83–88.
Dietrich, U. C. (1996). Factors influencing the attitudes held by women with type II diabetes: A qualitative study. Patient Education and Counseling, 29, 13–23. doi:10.1016/0738-3991(96)00930-5.
Skovlund, S. E., Peyrot, M., & DAWN International Advisory Panel. (2005). The Diabetes Attitudes, Wishes, and Needs (DAWN) program: A new approach to improving outcomes of diabetes care. Diabetes Spectrum, 18, 136–142. doi:10.2337/diaspect.18.3.136.
Hauber, A. B., Johnson, F. R., Sauriol, L., & Lescrauwaet, B. (2005). Risking health to avoid injections: Preferences of Canadians with type 2 diabetes. Diabetes Care, 28(9), 2243–2245. doi:10.2337/diacare.28.9.2243.
Korytkowski, M., Niskanen, L., & Asakura, T. (2005). FlexPen: Addressing issues of confidence and convenience in insulin delivery. Clinical Therapeutics, 27(Suppl B), S89–S100. doi:10.1016/j.clinthera.2005.11.019.
Lee, W. C., Balu, S., Cobden, D., Joshi, A. V., & Pashos, C. L. (2006). Medication adherence and the associated health-economic impact among patients with type 2 diabetes mellitus converting to insulin pen therapy: An analysis of third-party managed care claims data. Clinical Therapeutics, 28(10), 1712–1725. Discussion 1710–1711. doi:10.1016/j.clinthera.2006.10.004.
Kanakis, S. J., Watts, C., & Leichter, S. B. (2002). The business of insulin pumps in diabetes care: Clinical and economic considerations. Clinical Diabetes, 20, 214–216. doi:10.2337/diaclin.20.4.214.
Ritholz, M. D., Smaldone, A., Lee, J., Castillo, A., Wolpert, H., & Weinger, K. (2007). Perceptions of psychosocial factors and the insulin pump. Diabetes Care, 30(3), 549–554. doi:10.2337/dc06-1755.
Kølendorf, K., Ross, G. P., Pavlic-Renar, I., Perriello, G., Philotheou, A., Jendle, J., et al. (2006). Insulin detemir lowers the risk of hypoglycaemia and provides more consistent plasma glucose levels compared with NPH insulin in Type 1 diabetes. Diabetic Medicine, 23(7), 729–735. doi:10.1111/j.1464-5491.2006.01862.x.
Hermansen, K., Davies, M., Derezinski, T., Martinez Ravn, G., Clauson, P., & Home, P. (2006). A 26-week, randomized, parallel, treat-to-target trial comparing insulin detemir with NPH insulin as add-on therapy to oral glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetes Care, 29(6), 1269–1274. doi:10.2337/dc05-1365.
De Leeuw, I., Vague, P., Selam, J. L., Skeie, S., Lang, H., Draeger, E., et al. (2005). Insulin detemir used in basal-bolus therapy in people with type 1 diabetes is associated with a lower risk of nocturnal hypoglycaemia and less weight gain over 12 months in comparison to NPH insulin. Diabetes, Obesity & Metabolism, 7, 73–82. doi:10.1111/j.1463-1326.2004.00363.x.
Rosenstock, J., Dailey, G., Massi-Benedetti, M., Fritsche, A., Lin, Z., & Salzman, A. (2005). Reduced hypoglycemia risk with insulin glargine: A meta-analysis comparing insulin glargine with human NPH insulin in type 2 diabetes. Diabetes Care, 28(4), 950–955. doi:10.2337/diacare.28.4.950.
Haak, T., Tiengo, A., Draeger, E., Suntum, M., & Waldhäusl, W. (2005). Lower within-subject variability of fasting blood glucose and reduced weight gain with insulin detemir compared to NPH insulin in patients with type 2 diabetes. Diabetes, Obesity & Metabolism, 7, 56–64. doi:10.1111/j.1463-1326.2004.00373.x.
Raslová, K., Tamer, S. C., Clauson, P., & Karl, D. (2007). Insulin detemir results in less weight gain than NPH insulin when used in basal-bolus therapy for type 2 diabetes mellitus, and this advantage increases with baseline body mass index. Clinical Drug Investigation, 27(4), 279–285. doi:10.2165/00044011-200727040-00007.
Funnell, M. M. (2008). Quality of life and insulin therapy in type 2 diabetes mellitus. Insulin, 3, 31–36. doi:10.1016/S1557-0843(08)80009-7.
Snoek, F. J. (2002). Breaking the barriers to optimal glycaemic control—what physicians need to know from patients’ perspectives. International Journal of Clinical Practice. Supplement, 129, 80–84.
Peyrot, M., Rubin, R. R., Lauritzen, T., Skovlund, S. E., Snoek, F. J., Matthews, D. R., et al.; The International DAWN Advisory Panel. (2005). Resistance to insulin therapy among patients and providers: Results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study. Diabetes Care, 28(11), 2673–2679. doi:10.2337/diacare.28.11.2673.
Additional references included in review
Abraira, C., & Duckworth, W. (2003). The need for glycemic trials in type 2 diabetes. Clinical Diabetes, 21(3), 107–111.
Akram, K., Pedersen-Bjergaard, U., Borch-Johnsen, K., & Thorsteinsson, B. (2006). Frequency and risk factors of severe hypoglycemia in insulin-treated type 2 diabetes: A literature survey. Journal of Diabetes and its Complications, 20, 402–408.
Almér, L. O., Wollmer, P., Jonson, B., & Troedsson Almér, A. (2002). Insulin inhalation with absorption enhancer at meal-times results in almost normal postprandial insulin profiles. Clinical Physiology and Functional Imaging, 22(3), 218–221.
Assmann, G., Schulte, H., Funke, H., & von Eckardstein, A. (1998). The emergence of triglycerides as a significant independent risk factor in coronary artery disease. European Heart Journal, 19(Suppl M), M8–M14.
Barnett, A. H., & Bellary, S. (2007). Inhaled human insulin (Exubera): Clinical profile and patient considerations. Vascular Health and Risk Management, 3(1), 83–91.
Barnett, A. H., Dreyer, M., Lange, P., Serdarevic-Pehar, M.; On Behalf of the Exubera Phase III Study Group. (2006). An open, randomized, parallel-group study to compare the efficacy and safety profile of inhaled human insulin (Exubera) with glibenclamide as adjunctive therapy in patients with type 2 diabetes poorly controlled on metformin. Diabetes Care, 29(8), 1818–1825.
Bellary, S., & Barnett, A. H. (2006). Inhaled insulin (Exubera): Combining efficacy and convenience. Diabetes & Vascular Disease Research, 3(3), 179–185.
Berlin, I., Bisserbe, J. C., Eiber, R., Balssa, N., Sachon, C., Bosquet, F., et al. (1997). Phobic symptoms, particularly the fear of blood and injury, are associated with poor glycemic control in type I diabetic adults. Diabetes Care, 20(2), 176–178.
Black, C., Cummins, E., Royle, P., Philip, S., & Waugh, N. (2007). The clinical effectiveness and cost-effectiveness of inhaled insulin in diabetes mellitus: A systematic review and economic evaluation. Health Technology Assessment, 11(33), 1–126.
Blaha, M. J., & Elasy, T. A. (2006). Adherence to insulin and the risk of glucose deterioration. Diabetes Care, 29(8), 1982–1983.
Caballero, A. E. (2007). Cultural competence in diabetes mellitus care: An urgent need. Insulin, 2, 80–91.
Campos, C. (2007). Addressing cultural barriers to the successful use of insulin in hispanics with type 2 diabetes. Southern Medical Journal, 100(8), 812–820.
Cefalu, W. T. (2001). Novel routes of insulin delivery for patients with type 1 or type 2 diabetes. Annals of Medicine, 33(9), 579–586.
Chesla, C. A., & Chun, K. M. (2005). Accommodating type 2 diabetes in the Chinese American family. Qualitative Health Research, 15(2), 240–255.
Clark, M. (2007). Psychological insulin resistance: A guide for practice nurses. Journal of Diabetes Nursing, 11(2), 53–56.
Cramer, J. A., Okikawa, J., Bellaire, S., & Clauson, P. (2004). Compliance with inhaled insulin treatment using the AERx iDMS Insulin Diabetes Management System. Diabetes Technology & Therapeutics, 6(6), 800–807.
de Galan, B. E., Simsek, S., Tack, C. J., & Heine, R. J. (2006). Efficacy and safety of inhaled insulin in the treatment of diabetes mellitus. Netherlands Journal of Medicine, 64(9), 319–325.
Díez, J. J., & Iglesias, P. (2003). Inhaled insulin—A new therapeutic option in the treatment of diabetes mellitus. Expert Opinion on Pharmacotherapy, 4(2), 191–200.
Dunn, C., & Curran, M. P. (2006). Spotlight on inhaled human insulin (exubera((r))) in diabetes mellitus. Treatments in Endocrinology, 5(5), 329–331.
Fineberg, S. E. (2006). Diabetes therapy trials with inhaled insulin. Expert Opinion on Investigational Drugs, 15(7), 743–762.
Freemantle, N., Blonde, L., Duhot, D., Hompesch, M., Eggersten, R., Hobbs, F. D. R., et al. (2005).Availability of inhaled insulin promotes greater perceived acceptance of insulin therapy in patients with type 2 diabetes. Diabetes Care, 28, 427–428.
Funnell, M. M. (2006). The Diabetes Attitudes, Wishes, and Needs (DAWN) study. Clinical Diabetes, 24, 154–155.
Garg, S., Rosenstock, J., Silverman, B. L., Sun, B., Konkoy, C. S., de la Peña, A., et al. (2006). Efficacy and safety of preprandial human insulin inhalation powder versus injectable insulin in patients with type 1 diabetes. Diabetologia, 49(5), 891–899. Epub Feb 28, 2006.
Gerber, R. A., Cappelleri, J. C., Kourides, I. A., & Gelfand, R. A. (2001). Treatment satisfaction with inhaled insulin in patients with type 1 diabetes: A randomized controlled trial. Diabetes Care, 24(9), 1556–1559.
Harris, M. I., Eastman, R. C., Cowie, C. C., Flegal, K., & Eberhardt, M. S. (1999). Racial and ethnic differences in glycemic control of adults with type 2 diabetes. Diabetes Care, 22, 403–408.
Hermansen, K., & Davies, M. (2007). Does insulin detemir have a role in reducing risk of insulin-associated weight gain? Diabetes, Obesity and Metabolism, 9, 209–217.
Hollander, P. A., Blonde, L., Rowe, R., Mehta, A. E., Milburn, J. L., Hershon, K. S., et al. (2004). Efficacy and safety of inhaled insulin (exubera) compared with subcutaneous insulin therapy in patients with type 2 diabetes: Results of a 6-month, randomized, comparative trial. Diabetes Care, 27(10), 2356–2362.
Hunt, L. M., Arar, N. H., Larme, A. C., Rankin, S. H., & Anderson, R. M. (1998). Contrasting patient and practitioner perspectives in type 2 diabetes management. Western Journal of Nursing Research, 20(6), 656–682.
Leichter, S. B. (2005). Problems that extend visit time and cost in diabetes care: 1. How depression may affect the efficacy and cost of care of diabetic patients. Clinical Diabetes, 23(2), 53–54.
Martinez, L., Consoli, S. M., Monnier, L., Simon, D., Wong, O., Yomtov, B., et al. (2007). Studying the Hurdles of Insulin Prescription (SHIP): Development, scoring and initial validation of a new self-administered questionnaire. Health and Quality of Life Outcomes, 5, 53.
McAuley, L. (2001). Inhaled insulin for the treatment of diabetes mellitus. Issues in Emerging Health Technologies, 18, 1–4.
Mollema, E. D., Snoek, F. J., Pouwer, F., Heine, R. J., & van der Ploeg, H. M. (2000). Diabetes Fear of Injecting and Self-Testing Questionnaire: A psychometric evaluation. Diabetes Care, 23, 765–769.
Odegard, P. S., & Capoccia, K. (2007). Medication taking and diabetes: a systematic review of the literature. The Diabetes Educator, 33(6), 1014–1029. Discussion 1030–1031.
Petrak, F., Stridde, E., Leverkus, F., Crispin, A. A., Forst, T., & Pfutzner, A. (2007). Development and validation of a new measure to evaluate psychological resistance to insulin treatment. Diabetes Care, 30(9), 2199–2204.
Peyrot, M., Rubin, R. R., & Siminerio, L. M. (2006). Physician and nurse use of psychosocial strategies in diabetes care: Results of the cross-national Diabetes Attitudes, Wishes and Needs (DAWN) study. Diabetes Care, 29(6), 1256–1262.
Polonsky, W. H., Fisher, L., Dowe, S., & Edelman, S. (2003). Why do patients resist insulin therapy? [abstract]. Diabetes, 52, A417.
Rave, K., Bott, S., Heinemann, L., Sha, S., Becker, R. H., Willavize, S. A., et al. (2005). Time-action profile of inhaled insulin in comparison with subcutaneously injected insulin lispro and regular human insulin. Diabetes Care, 28(5), 1077–1082.
Rosenstock, J., Cappelleri, J. C., Bolinder, B., & Gerber, R. A. (2004). Patient satisfaction and glycemic control after 1 year with inhaled insulin (Exubera) in patients with type 1 or type 2 diabetes. Diabetes Care, 27(6), 1318–1323.
Rosenstock, J., Muchmore, D., Swanson, D., & Schmitke, J. (2007). AIR Inhaled Insulin System: A novel insulin-delivery system for patients with diabetes. Expert Review of Medical Devices, 4(5), 683–692.
Sadri, H., MacKeigan, L. D., Leiter, L. A., & Einarson, T. R. (2005). Willingness to pay for inhaled insulin: A contingent valuation approach. Pharmacoeconomics, 23(12), 1215–1227.
Siminerio, L. (2006). Challenges and strategies for moving patients to injectable medications. The Diabetes Educator, 32(Suppl 2), 82S–90S.
Skovlund, S. E., van der Ven, N., Pouwer, F., & Snoek, F. J. (2003). Appraisal of insulin treatment in type 2 diabetes patients with and without previous experience of insulin therapy [abstract]. Diabetes, 52, A419.
Skyler, J. S., Jovanovic, L., Klioze, S., Reis, J., & Duggan, W.; Inhaled Human Insulin Type 1 Diabetes Study Group. (2007). Two-year safety and efficacy of inhaled human insulin (Exubera) in adult patients with type 1 diabetes. Diabetes Care, 30(3), 579–585.
Stratton, I. M., Adler, A. I., Neil, H. A. W., Matthews, D. R., Manley, S. E., Cull, C. A., et al. (2000). Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ, 321, 405–412.
Vinik, A. (2007). Advancing therapy in type 2 diabetes mellitus with early, comprehensive progression from oral agents to insulin therapy. Clinical Therapeutics, 29, 1236–1253.
White, J. R., Davis, S. N., Cooppan, R., Davidson, M. B., Mulcahy, K., Manko, G. A., et al. (2003). Clarifying the role of insulin in type 2 diabetes management. Clinical Diabetes, 21, 14–21.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Brod, M., Kongsø, J.H., Lessard, S. et al. Psychological insulin resistance: patient beliefs and implications for diabetes management. Qual Life Res 18, 23–32 (2009). https://doi.org/10.1007/s11136-008-9419-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-008-9419-1