
Abstract
Astaxanthin, a carotenoid, has antioxidant activity as well as many positive effects, such as anticancer and anti-inflammatory effects. We performed a randomized, double-blind, placebo-controlled study to investigate the effects of astaxanthin on lipid profiles and oxidative stress in overweight and obese adults in Korea. In total, 27 subjects with body mass index >25.0 kg/m2 were enrolled and randomly assigned into two groups administered astaxanthin or placebo capsules for 12 weeks. Total cholesterol, triglycerides, high density lipoprotein (HDL) cholesterol, low density lipoprotein (LDL) cholesterol, apolipoprotein A1 (ApoA1), and apolipoprotein B (ApoB) were measured before and after intervention. Malondialdehyde (MDA), isoprostane (ISP), superoxide dismutase (SOD), and total antioxidant capacity (TAC), as oxidative stress biomarkers, were measured at baseline and at 4, 8, and 12 weeks after intervention. LDL cholesterol and ApoB were significantly lower after treatment with astaxanthin, compared with the start of administration, whereas none of the lipid profiles was changed in the placebo group. At the baseline, all four biomarkers were not significantly different between the two groups. Compared with the placebo group, MDA and ISP were significantly lower, but TAC was significantly higher in the astaxanthin group at 12 weeks. These results suggest that supplementary astaxanthin has positive effects by improving the LDL cholesterol, ApoB, and oxidative stress biomarkers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dyslipidemia is a disorder of lipoprotein metabolism, and is one of the reported factors for increased cardiovascular risk. The cause of dyslipidemia is often diet or lifestyle; however, insulin resistance or obesity can also be involved. The dyslipidemic phenotype is commonly associated with obesity, and cardiovascular events are increased in overweight or obese subjects [1]. Another risk factor in obesity is the increased oxidative stress (OS) [2, 3]. OS is associated with metabolic syndrome, which is a collection of medical conditions that increases the risk of developing cardiovascular disease and diabetes. Previous results confirm that obesity-induced OS can play a substantial role in metabolic-syndrome-related diseases, including atherosclerosis, hypertension, and type 2 diabetes [4].
Astaxanthin (3,3’-dihydroxy-β,β’-carotene-4,4’-dione) is a xanthophyll carotenoid pigment, which has positive effects including antioxidant, anticancer, and anti-inflammatory activities [5]. Astaxanthin is distributed primarily in marine organisms, and is isolated from the algae Haematococcus pluvials [6]. Clinical studies have confirmed that astaxanthin has significant effects on lipid peroxidation and inflammation, as well as functional dyspepsia and male infertility [7–10]. Additionally, astaxanthin has been reported to improve lipid metabolism in animal models and humans with dyslipidemia. Astaxanthin supplementation reduces triglyceride and total cholesterol and increases high-density lipoprotein (HDL) cholesterol in obese mice fed a high-fat diet and rats with insulin resistance [11, 12]. Also, administration of astaxanthin for 12 weeks increases serum HDL cholesterol in moderately hypertriglyceridemic subjects [13].
Thus, we performed a randomized, double-blind, placebo-controlled trial to evaluate the positive effects of astaxanthin supplementation on lipid profiles (LPs) and OS state in overweight adults.
Subjects and Methods
Subjects and Study Design
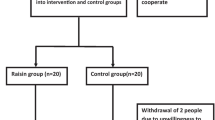
In total, 27 Korean overweight adults (aged 20–55 years; body mass index (BMI) >25.0 kg/m2) who were overweight (body mass index (BMI) >25.0 kg/m2) were enrolled. Exclusion criteria included a history of smoking, excessive alcohol consumption, pregnant or lactating women, diabetes, hypertension, cardiovascular disease, or other chronic diseases, and hepatic or renal dysfunction. Subjects who were taking vitamin supplements or medicines were also excluded. At screening, the health status of all subjects was considered according to medical history, physical examination, and laboratory investigation.
This study was approved by the Institutional Review Board of the Clinical Research Institute, Seoul National University Hospital (Seoul, South Korea). Written informed consent was obtained from each participant before enrolment.
This was a prospective, randomized, double-blind trial to evaluate the positive effects of astaxanthin on LPs and OS. Subjects were randomly assigned to astaxanthin and placebo groups. The subjects in the astaxanthin group were instructed to take one 20 mg astaxanthin capsule (Marine Product Tech. Inc., Seongnam, South Korea) once daily after breakfast for 12 weeks. The subjects in the placebo group were instructed to consume one placebo capsule daily. All subjects visited for blood sampling every four weeks and body weight, height, and waist circumference were measured at baseline and at 12 weeks. Each blood sample (approximately 10 ml) was collected via the brachial venous vein and stored at −70 °C (Reveco ULT 1490 D-N-s; Western Medics, Asheville, NC, USA) until analysis of lipid concentration. After centrifugation of blood samples, plasma samples (3 ml, each) were stored until analysis of OS biomarkers. During the study, the subjects were asked to maintain their usual lifestyle and to refrain from taking any vitamins or nutritional supplements. At the end of the study, all subjects were asked to bring back their remaining astaxanthin or placebo capsules and administration reports to assess adherence and adverse drug reactions.
Blood Lipid Profiles
Total cholesterol, triglycerides, HDL cholesterol, low-density lipoprotein (LDL) cholesterol, apolipoprotein A1 (ApoA1), and apolipoprotein B (ApoB) were measured at baseline and at 12 weeks. Total cholesterol and triglyceride concentrations were analyzed by enzymatic colorimetric assay, HDL and LDL cholesterol by homogeneous enzymatic colorimetric assay, and ApoA1 and ApoB by immunoturbidimetry. All samples were analyzed in the Department of Laboratory Medicine, Seoul National University Hospital (Seoul, South Korea).
Oxidative Stress Biomarkers
Malondialdehyde (MDA), 15-isoprostane F2t (ISP; also known as 8-epi-PGF2α, 8-iso-PGF2α, or 8-isoprostane), superoxide dismutase (SOD), and total antioxidant capacity (TAC) were measured to evaluate OS at baseline and at 4, 8, and 12 weeks. Plasma concentrations of MDA, ISP, SOD, and TAC were analyzed using ELISA (Versa MAX; Molecular Devices, Sunnyvale, CA). Assay kits used for the measurement of MDA were purchased from Oxis International (Beverly Hills, CA) and for ISP from Assay Designs (Farmingdale, NY). TAC assay kits were purchased from Oxford Biomedical Research (Oxford, MI) and a SOD assay kit was purchased from Dojindo Laboratories (Kumamoto, Japan).
Statistical Analysis
The sample size was estimated with two-sided 5% significance and 90% power. Data were tested for normality using the Kolmogorov–Smirnov test. To compare between the astaxanthin and placebo groups, the independent sample t-test was used. Student’s paired t-test was used to assess the difference between the intervention times within each group. Pearson’s correlation was used to evaluate the relationship between the parameters. Data are presented as the mean ± standard deviation (SD). The SPSS software (ver. 17.0; Chicago, IL) was used for all statistical analyses and P values < 0.05 were deemed to indicate statistical significance.
Results
Characteristics of Study Subjects
Demographic data and body sizes of all subjects are listed in Table 1. There were no significant differences between the astaxanthin and placebo groups both at baseline and at 12 weeks, except for BMI. At baseline, BMI in the astaxanthin group was significantly higher than in the placebo group. Age was negatively correlated with body weight (Fig. 1a).

Plots of correlation among demographic data, oxidative stress biomarkers, and lipid profiles
Effect of Astaxanthin on Blood Lipid Profiles
Total cholesterol, triglycerides, HDL cholesterol, LDL cholesterol, ApoA1, ApoB, and ApoA1/ApoB ratio between placebo and astaxanthin groups at both baseline and at 12 weeks are listed in Table 2. The lipid concentrations were not significantly different between the two groups except LDL cholesterol, ApoB, and ApoA1/ApoB ratio. In the astaxanthin group, the LDL cholesterol, ApoB, and ApoA1/ApoB ratio at 12 weeks were significantly lower (by 10.4, 7.59, and 8.22%, respectively) than at baseline.
Correlation Analysis of Lipid Profiles
Age was positively correlated with total cholesterol (Fig. 1b), triglycerides (Fig. 1c), LDL cholesterol, and ApoB (data not shown). Additionally, total cholesterol was positively correlated with triglyceride (Fig. 1d), LDL cholesterol (Fig. 1e), and ApoB (data not shown), and triglyceride was positively correlated with LDL cholesterol and ApoB (data not shown). A proportional relationship between LDL cholesterol and ApoB was also observed (Fig. 1f). HDL cholesterol was positively correlated with ApoA1 (Fig. 1g), while negatively correlated with triglyceride (Fig. 1h).
Effect of Astaxanthin on Oxidative Stress
Plasma concentrations of MDA, ISP, SOD, and TAC in the astaxanthin and placebo groups at baseline and at 4, 8, and 12 weeks are listed in Table 3. In the astaxanthin group, MDA at 8 and 12 weeks was significantly lower (by 17.3 and 29.0%, respectively), and ISP at 8 and 12 weeks was also significantly lower (by 40.2 and 52.9%, respectively), but TAC at 12 weeks was significantly higher (by 30.1%) than in the placebo group.
In the placebo group, MDA at 4, 8, and 12 weeks was significantly lower (by 16.5, 4.59, and 8.26%, respectively). ISP at 4 and 12 weeks was also significantly lower (by 5.95 and 8.96%, respectively), but TAC at 4 and 8 weeks was significantly higher (by 8.45 and 10.1%, respectively) than at baseline. The changes in MDA and ISP, which are biomarkers of lipid peroxidation, were related to the decrease in LDL cholesterol and increase in total cholesterol (Table 2).
In the astaxanthin group, MDA at 4, 8, and 12 weeks was significantly lower (by 9.95, 18.5, and 32.7%, respectively) than at baseline. ISP at 4, 8, and 12 weeks was also significantly lower (by 24.5, 45.1 and 59.0%, respectively) than at baseline, but SOD at 12 weeks was significantly higher (by 30.3%) than the baseline level and TAC at 4, 8, and 12 weeks was also significantly higher (by 20.0, 24.4, and 34.5%, respectively) than at baseline.
In the results of correlation analysis, ISP was negatively correlated with ApoA1 (Fig. 1i) and HDL cholesterol (data not shown).
Patient Compliance and Adverse Events
All subjects in the two intervention groups completed the study. According to the count of remaining capsules, adherence rates were 93.4 and 92.9% in the astaxanthin and placebo groups, respectively. In the astaxanthin group, gastrointestinal adverse events were observed: fecal color changed to red (n = 2, 14.3%) and bowel movements increased (n = 2, 14.3%). Changes in fecal color to red could have been due to the reddish color of astaxanthin. In the placebo group, muscle fatigue (n = 2, 15.4%) and abdominal discomfort (n = 1, 7.69%) were observed. Subjective symptom improvement after astaxanthin intervention included decreased fatigue (n = 4, 28.6%), body weight loss (n = 3, 21.4%), and improved skin condition (n = 2, 14.3%). There were no abnormal changes in the results of renal and hepatic function tests during the study period.
Discussion
Our previous study showed that supplemental astaxanthin over 3 weeks reduced obesity-induced OS in overweight subjects, with reference to biomarkers of lipid peroxidation and antioxidant activity [14]. The present study was conducted to evaluate the long-term effects of astaxanthin on OS and LPs in overweight and obese subjects. Daily supplementation with 20 mg astaxanthin for 12 weeks significantly lowered LDL cholesterol and ApoB, as well as OS biomarkers. This suggests that astaxanthin may improve oxidative status and LPs in human subjects.
Positive effects of astaxanthin on LPs have been reported in previous animal studies. For example, in a mouse model of obesity, astaxanthin reduced liver triglycerides, plasma triglycerides, and total cholesterol [11]. In an SHR/NDmcr-cp rat model treated with astaxanthin, adiponectin and HDL -cholesterol were increased, but triglycerides and non-esterified fatty acids were decreased by improving insulin resistance [12]. Recently, Yang et al. [15] have also reported that astaxanthin lowers plasma LPs and enhances antioxidant defence in apolipoprotein E knockout mice. One clinical trial evaluated the effect of astaxanthin on LPs [13]. That study, however, was performed in subjects with mild dyslipidemia. Thus, the present study is appropriate to clarify that astaxanthin supplementation improves LPs and prevents lipidemic diseases in human subjects with normal lipid concentrations.
After astaxanthin administration for 12 weeks, LDL cholesterol and ApoB were significantly reduced in the present study (Table 2). ApoB is known as the primary apolipoprotein of LDL cholesterol, and the change in ApoB could be a positive signal, which results in further decreases in LDL cholesterol. ApoB/ApoA1 ratio, or an effective index to predict heart attack risk, is also significantly decreased by astaxanthin [16]. The above results indicate that astaxanthin improves the blood lipid profile by inhibiting synthesis of LDL cholesterol or accelerating its dissolution.
The effects of astaxanthin on obesity-induced OS were reported from our previous study. After 3 weeks of supplementation with 5 and 20 mg astaxanthin, both MDA and ISP were significantly reduced, but, SOD and TAC were significantly increased in both dosage groups [14]. In the present study, we followed up for 12 weeks to evaluate the efficacy and safety of long-term astaxanthin intervention. Astaxanthin reduced MDA and ISP, biomarkers of lipid peroxidation, and increased SOD and TAC, which are biomarkers of the antioxidative system (Table 3). During the study, in total, four adverse reactions were observed, which were mild and short-term. These results suggest that daily supplementation with astaxanthin is safe and protective against OS in overweight and obese subjects.
Four oxidative stress biomarkers, including MDA, ISP, SOD, and TAC, were used in the present study. MDA and ISP are well-known indicators of lipid peroxidation, and SOD and TAC are also representative indicators of antioxidant activity [17–20]. Many studies using these biomarkers have evaluated the status or changes in oxidative stress in human subjects. Sutherland et al. [21] have reported the antioxidant effect of high-dose vitamins in overweight subjects, using ISP. Additionally, Ozata et al. [22] have reported that SOD in an overweight group was lower than in controls, and Melissas et al. [23] have reported that TAC in overweight patients was significantly different before and after weight loss.
In our previous study, the mean plasma concentrations of astaxanthin after 3 week supplementation at doses of 5 and 20 mg were 335 and 677 nM, respectively, which are higher than 200 nM, as an ED50 of astaxanthin [24]. This indicates that the dose of 20 mg astaxanthin in this study was appropriate to evaluate the effects on OS and LPs.
One particularly interesting finding is the possibility that astaxanthin prevents body weight gain. The changes in BMI and body weight in the two intervention groups support this hypothesis. Body weight and BMI hardly changed in the astaxanthin group, whereas they both increased in the placebo group (Table 1). A previous animal study also showed that astaxanthin inhibited increases in body and adipose tissue weights in obese mice fed a high-fat diet [11]. These findings may be meaningful for overweight or obese individuals. However, there was not a significant difference in our study; thus, more studies are needed to evaluate whether astaxanthin truly has a body weight-lowering effect.
Protective effects of astaxanthin, including antioxidant activity, have been demonstrated in many studies. However, information about the biological mechanism of astaxanthin is still not sufficient. We can speculate based on previous clinical results and pharmacokinetic data, but further studies are required to determine the mechanism of astaxanthin in humans.
In summary, 12 weeks of supplementation with astaxanthin significantly lowered LDL cholesterol and ApoB in overweight subjects. Also, OS biomarkers including MDA, ISP, SOD, and TAC were improved by astaxanthin. Thus, astaxanthin supplementation is apparently safe and effective for prevention of lipidemic diseases and oxidative damage in healthy overweight subjects.
Abbreviations
- ApoA1:
-
Apolipoprotein A1
- ApoB:
-
Apolipoprotein B
- BMI:
-
Body mass index
- HDL:
-
High-density lipoprotein
- ISP:
-
Isoprostane
- LDL:
-
Low-density lipoprotein
- LPs:
-
Lipid profiles
- MDA:
-
Malondialdehyde
- OS:
-
Oxidative stress
- SD:
-
Standard deviation
- SOD:
-
Superoxide dismutase
- TAC:
-
Total antioxidant capacity
References
Remco F, Houshang M, Erik SG, John JP (2008) Obesity and dyslipidemia. Endocrinol Metab Clin N Am 37:623–633
Block G, Dietrich M, Norkus EP, Morrow JD, Hudes M, Caan B, Packer L (2002) Factors associated with oxidative stress in human populations. Am J Epidemiol 156:274–285
Melissas J, Malliaraki N, Papadakis JA, Taflampas P, Kampa M, Castanas E (2006) Plasma antioxidant capacity in morbidly obese patients before and after weight loss. Obes Surg 16:314–320
Ceriello A, Motz E (2004) Is oxidative stress the pathogenic mechanism underlying insulin resistance, diabetes, and cardiovascular disease? The common soil hypothesis revisited. Arterioscler Thromb Vasc Biol 24:816–823
Higuera-Ciapara I, Félix-Valenzuela L, Goyocoolea FM (2006) Astaxanthin: a review of its chemistry and applications. Crit Rev Food Sci Nutr 46:186–196
García-Malea MC, Acién FG, Del Río E, Fernández JM, Cerón MC, Guerrero MG, Molina-Grima E (2009) Production of astaxanthin by Haematococcus pluvialis: Taking the one-step system outdoors. Biotechnol Bioeng 102:651–657
Fassett RG, Healy H, Driver R, Robertson IK, Geraghty DP, Sharman JE, Coombes JS (2008) Astaxanthin vs placebo on arterial stiffness, oxidative stress and inflammation in renal transplant patients xanthin: A randomized controlled trial. BMC Nephrol 9:17
Karppi J, Rissanen TH, Nyyssönen K, Kaikkonen J, Olsson AG, Voutilainen S, Salonen JT (2007) Effects of astaxanthin supplementation on lipid peroxidation. Int J Vitam Nutr Res 77:3–11
Andersen LP, Holck S, Kupcinskas L, Kiudelis G, Jonaitis L, Janciauskas D, Permin H, Wadström T (2007) Gastric inflammatory markers and interleukins in patients with functional dyspepsia treated with astaxanthin. FEMS Immunol Med Microbiol 50:244–248
Comhaire FH, El Garem Y, Mahmoud A, Eertmans F, Schoonjans F (2005) Combined conventional/antioxidant “Astaxanthin” treatment for male infertility: A double blind, randomized trial. Asian J Androl 7:257–262
Ikeuchi M, Koyama T, Takahashi J, Yazawa K (2007) Effects of astaxanthin in obese mice fed a high-fat diet. Biosci Biotechnol Biochem 71:893–899
Hussein G, Nakagawa T, Goto H, Shimada Y, Matsumoto K, Sankawa U, Watanabe H (2007) Astaxanthin ameliorates features of metabolic syndrome in SHR/NDmcr-cp. Life Sci 80:522–529
Hiroshi Y, Hidekatsu Y, Kumie I, Yoshiharu T, Takashi K, Hiroki T, Norio T (2010) Administration of natural astaxanthin increases serum HDL-cholesterol and adiponectin in subjects with mild hyperlipidemia. Atherosclerosis 209:520–523
Choi HD, Kim JH, Chang MJ, Kyu-Youn Y, Shin WG (2011) Effects of astaxanthin on oxidative stress in overweight and obese adults. Phytother Res [Epub ahead of print]
Yang Y, Seo JM, Nguyen A, Pham TX, Park HJ, Park Y, Kim B, Bruno RS, Lee J (2011) Astaxanthin-rich extract from the green alga Haematococcus pluvialis lowers plasma lipid concentrations and enhances antioxidant defense in apolipoprotein E knockout mice. J Nutr 141:1611–1617
McQueen MJ, Hawken S, Wang X, Ounpuu S, Sniderman A, Probstfield J, Steyn K, Sanderson JE, Hasani M, Volkova E, Kazmi K, Yusuf S, INTERHEART study investigators (2008) Lipids, lipoproteins, and apolipoproteins as risk markers of myocardial infarction in 52 countries (the INTERHEART study): A case-control study. Lancet 372:224–233
Michel F, Bonnefont-Rousselot D, Mas E, Drai J, Thérond P (2008) Biomarkers of lipid peroxidation: Analytical aspects. Ann Biol Clin 66:605–620
Morrow JD, Chen Y, Brame CJ, Yang J, Sanchez SC, Xu J, Zackert WE, Awad JA, Roberts LJ (1999) The isoprostanes: Unique prostaglandin-like products of free-radical-initiated lipid peroxidation. Drug Metab Rev 31:117–139
Bannister WH, Rotilio G (1987) Aspects of the structure, function, and applications of superoxide dismutase. CRC Crit Rev Biochem 22:111–180
Apak R, Güçlü K, Ozyürek M, Karademir SE, Altun M (2005) Total antioxidant capacity assay of human serum using copper(II)-neocuproine as chromogenic oxidant: The CUPRAC method. Free Radic Res 39:949–961
Sutherland WH, Manning PJ, Walker RJ, de Jong SA, Ryalls AR, Berry EA (2007) Vitamin E supplementation and plasma 8-isoprostane and adiponectin in overweight subjects. Obesity (Silver Spring) 15:386–391
Ozata M, Mergen M, Oktenli C, Aydin A, Sanisoglu SY, Bolu E, Yilmaz MI, Sayal A, Isimer A, Ozdemir IC (2003) Increased oxidative stress and hypozincemie in male obesity. Clin Biochem 35:627–631
Melissas J, Malliaraki N, Papadakis JA, Taflampas P, Kampa M, Castanas E (2006) Plasma antioxidant capacity in morbidly overweight patients before and after weight loss. Obes Surg 16:314–320
Miki W (1991) Biological functions and activities of animal carotenoids. Pure Appl Chem 63:141–146
Acknowledgments
This work was supported by a grant of the Korea Health 21 R&D project, Ministry of Health and Welfare, South Korea (A050376). The authors would like to thank all subjects participated in this study. No writing assistance was acquired for this paper. The contributions of the authors to the manuscript are as follows. H.C.: study design, data collection, samples analyses, data analyses and writing of the manuscripts; Y.Y.: study design and coordination; W.S.: study design, coordination and reviewing the manuscript. All authors read and approved the final manuscript.
Disclosure
The authors declared no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Choi, H.D., Youn, Y.K. & Shin, W.G. Positive Effects of Astaxanthin on Lipid Profiles and Oxidative Stress in Overweight Subjects. Plant Foods Hum Nutr 66, 363–369 (2011). https://doi.org/10.1007/s11130-011-0258-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11130-011-0258-9