
Abstract
The potential of selenium-enriched rye/wheat sourdough bread as a route for supplementing dietary selenium intakes is reported. In addition to their normal diets, 24 female volunteers (24 to 25 years old) were fed either selenium-enriched bread or non-enriched bread each day (68.02 and 0.84 μg selenium day−1 respectively) for 4 weeks. The chemical form of the selenium in the bread had been characterised using HPLC-ICP-MS, which showed that 42% of the extractable selenium was present as selenomethionine. Plasma selenium levels and plasma platelet glutathione peroxidase (GPx1) activity were measured in the volunteers’ blood over a 6-week period. A statistically significant difference (p = 0.001) was observed in the mean percentage change data, calculated from the plasma selenium level measurements for the enriched and control group, over the duration of the study. A comparable difference was not observed for the platelet GPx1 activity (p = 0.756), over the same period. Two weeks after cessation of the feeding stage, i.e., at t = 6 weeks, the mean percentage change value for the selenium plasma levels in the enriched group was still significantly elevated, suggesting that the absorbed selenium had been incorporated into the body’s selenium reserves, and was then being slowly released back into the volunteers’ blood.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Many countries in Europe have reported a downward trend in their populations’ dietary intakes of selenium [1–3]. This is due, in part, to changes in the dietary habits of certain sub-groups within the general population, e.g. reduced calorific intakes and increased consumption of highly processed foods. However, the most significant impact is due to the substitution of North American wheat imports by produce from within Europe [3].
The health implications of this trend are deemed significant because of the reported involvement of selenium in many structural, metabolic and enzymatic processes within the body [4]. The element has been reported to have an involvement in restraining the progression and virulence of certain viral infections [5–7] and, possibly most significantly, it is widely reported for its anti-cancer effects [8, 9]. It has also been connected with correct immune function [10], anti-ageing [11] and male reproductive performance [12]. Any reduction in the dietary intakes of selenium may therefore be seen to be of nutritional and/or clinical concern.
In this study rye/wheat sourdough bread was identified as a potential vehicle for selenium supplementation because it is a dietary staple in many Eastern European countries where, incidentally, intakes of the element can sometimes be low [2]. Advances in the technology associated with the production of the sourdough bread have facilitated enrichment of the product with elevated levels of selenium, mainly in an organic form [13]. Because bread is a staple food, it is often used for dietary supplementation, e.g., with folic acid [14].
Therefore, the aim of the human study described here was to investigate whether consumption of the selenium-enriched sourdough bread had a positive effect on the body’s selenium status and was, therefore, an efficacious dietary source of the element.
Materials and Methods
Subjects
Twenty four female volunteers, aged between 24 and 25 years, were recruited from students at the Technical University of Łόdz, Poland. Informed, written consent was obtained prior to taking a screening blood sample to eliminate those volunteers whose biochemical and haematological indices fell outside of the normal range. The volunteers agreed to exclude selenium-rich supplements and foods during the course of the study but, in all other respects, they were allowed to maintain their normal lifestyle and dietary habits. The Ethical Committee of the Military Medical Academy (WAM) in Łόdz, Poland approved the study.
Test Meals
Two mixed wheat/rye sourdough breads were produced. The rye flour was made from dried and ground rye seedlings which had been grown in either a selenium-rich environment or one containing only normal levels of the element (referred to in this paper as enriched and control material, respectively). Details of the bread making process, including the incorporation and biotransformation of the selenium, are described elsewhere [13].
Bread rolls were baked in sufficient amounts so as to provide enough test material for the duration of the 28-day feeding trial. The breads were dried, at 40°C, homogenised and stored until required for feeding to the volunteers. This removed the possibility of between-roll variability affecting the precision of the selenium utilisation data. The levels of selenium in the control and enriched breads were 0.04 and 3.58 μg g−1 respectively.
Study Design
On each test day, following an overnight fast, the volunteers were fed 19 g of the bread assigned to their particular group, equating to an additional 0.84 and 68.02 μg of selenium for the control and enriched group, respectively. Feeding of the bread was stopped after t = 4 weeks. On the morning of the first test meal (and at the same time 1, 2, 4 and 6 weeks later) samples of blood were drawn by venepuncture into tubes. The tubes (Medlab, Raszyn, Poland) contained sodium citrate (3.2% w/v), and the blood to citrate ratio was 9:1.
Analytical Methods
All reagents were analytical-grade or better (Sigma-Aldrich Company Ltd, Poole, Dorset, UK) and the water was of Millipore-grade (>18.2 MΩ cm−1).
Preparation of Blood Fractions
Fresh blood samples were centrifuged to separate the plasma and plasma platelets from the whole blood. To obtain the plasma fraction, blood was centrifuged at 1,500×g for 5 min. To obtain the platelet fraction, samples of blood had to undergo a two-stage separation. Firstly, centrifugation at 100×g for 10 min, followed by collection of the supernatant which was then centrifuged again, at 900×g for 15 min. The platelet-containing pellet was washed 3 times using Hanks buffer (each washing was followed by centrifugation at 900×g for 10 min). The washed pellet was suspended in saccharose solution (2 ml, 0.32 M). All samples were stored at −70°C until required for analysis.
Measurement of Platelet Glutathione Peroxidase-1 (GPx1) Activity
Immediately prior to measurement of platelet GPx1 activity, careful defrosting of the samples was performed (2 h, 4°C) so as to minimise the possibility of changes due to sample-handling differences. The platelets were disrupted by sonication prior to centrifugation (20,000×g for 10 min, 4°C). Measurement of the platelet GPx1 was performed using the method described by Belsten and Wright [15]. Plasma protein concentrations were determined using a colorimetric method [16] and the data used in the normalisation of the GPx1 activity (expressed as U/mg protein).
Measurement of Selenium
Details of measurement of total selenium by hydride generation-inductively coupled plasma-mass spectrometry (HG-ICP-MS) are described elsewhere [13].
Selenium Speciation Analysis
The methods used to characterise the selenium species in the bread samples are described in detail elsewhere [13].
Quality Assurance and Quality Control (QA/QC) Procedures Undertaken during the Measurement of Total Selenium in the Plasma Samples
All stages of the analytical procedures used in the determination of total selenium in the plasma and bread samples were accredited by the United Kingdom Accreditation Scheme (UKAS) to ISO-17025. Each acid digestion batch included the following QA and QC materials: Seronorm-human serum and NIST 2670-freeze-dried urine (both from LGC Promochem, Teddington, UK), at least 4 procedural blanks and 1 spiked procedural blank.
QA/QC Procedures Undertaken during the Speciation Analysis of the Bread Samples
There are no certified reference materials available for individual selenium species in foods. However, candidate reference materials (wheat flour and yeast—EU funded project: G6RD-CT-2001-00473/SEAS) were used as part of the QA procedures accompanying the selenium speciation analysis of the experimental breads [13].
QA/QC Procedures Undertaken during the Measurement of Platelet GPx1 Activity
A quantity of human blood was taken prior to the start of the human study, for use as an in-house reference material (IHRM) in the measurement of platelet GPx1 activity. The platelet fraction was collected, prepared as above, sub-sampled into vials and stored at −70°C. Aliquots of the IHRM were analysed alongside the volunteers’ platelet samples, and the data used to normalise the test data, thereby minimising between-batch analytical variability.
Statistical Analysis
A repeated measures analysis of variance was performed with the applied treatment as a factor. This analysis takes into account the within-subject variation, i.e. the correlation between successive time points on the same subject. In addition, formal comparisons between the controlled and enriched groups were made at each time point of the study, using the estimate of variation calculated in the repeated measures analyses. Analyses of selenium and GPx1 were performed separately in the form of concentration and percentage change from baseline (week 0), using GenStat8.
Results
Human Study Data
Table 1 presents the plasma selenium concentration and the plasma platelet GPx1 activity data for the 24 volunteers, during the 6 weeks (5 time points) of the intervention study.
Table 2 reports the statistical data resulting from the analysis of the mean percentage changes observed in the two selenium status markers. The important values to be noted in the table are highlighted in bold (F-prob for time by treatment interaction), and reflect the effect of feeding the enriched bread over the whole period of the study.
Speciation of Selenium in the Breads Fed to the Human Study Volunteers
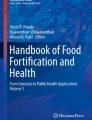
Figure 1 shows the HPLC-ICP-MS chromatograms obtained from the enriched and control breads. In Fig. 1a the selenomethionine peak is at t = 212 s, but is not present in Fig. 1b, i.e., the chromatogram obtained from the non-enriched control bread. The identity of this peak was confirmed by electrospray-mass spectrometric (ES-MS) analysis, and was shown to account for 42% of the total Se-containing peak areas. It was not possible to establish the identity of the other peaks in the chromatogram due to their low concentrations in the breads. However, what can be said is that their retention times do not correspond to those of the inorganic selenium forms, selenate or selenite [13].

HPLC-ICP-MS chromatograms showing the selenium profiles of the enriched and control breads; a is the chromatogram obtained from the selenium-enriched bread and b is the chromatogram obtained from the control bread
Analytical QA/QC Data
The recovery of selenium from the CRMs was as follows; Seronorm = 97 ± 8.5% (n = 37) and NIST2670 = 98 ± 7.4% (n = 42). Mean values for the recovery of spike were 101 ± 8.2% (n = 18). A limit of detection (LOD) for the procedure was 5 ng g−1.
QA Data Obtained during the Speciation Analysis of the Bread Samples
The percentage extraction efficiency for the candidate reference material was 64.8 ± 2.5% and the LOD for the procedure was calculated to be 0.002 μg g−1 (reported as selenomethionine).
Discussion
Plasma Selenium Concentration
From Tables 1 and 2, it can be seen that the calculated mean percentage change value shows that the difference between the control and enriched groups was highly significant over the duration of the study (p < 0.001). The percentage change in the mean concentration of the two groups was similar at week 1, but was significantly greater at weeks 2, 4 and 6. It should be noted that even 2 weeks after cessation of the feeding stage, the samples at week 6 still showed elevated plasma selenium levels. This suggests that the absorbed selenium had been successfully incorporated into the volunteers’ body reservoirs and was then being slowly released back into the blood.
Platelet GPx1 Activity
Tables 1 and 2b shows that there was no statistically significant difference in the mean percentage change observed in the platelet GPx1 activity between the control and enriched groups during the study (p = 0.756). This may be due to the plasma selenium levels, at the start of the feeding regime, being sufficiently high [mean ± SD: 56.3 ± 6 (μg L−1) and range: 48–65 (μg L−1)] as to have already induced maximal expression of the enzyme. However, using the calculation used by Zachara and Wasowicz [17], the average plasma selenium level of 58.2 μg L−1 (measured in the t = 0 samples of the 24 volunteers) equates to a dietary selenium intake of ∼39 μg day−1. This value is significantly below the 60 μg day−1 Reference Nutrient Intake for females proposed by the UK government Department of Health in 1991 [18] and recommended in ‘Guidelines for Poland’ [19]. It is therefore uncertain whether the selenium status of the volunteers would have been sufficiently high to result in maximal GPx1 expression prior to the study onset.
An alternative explanation is that, as the chemical form of the selenium in the enriched bread was shown to be mainly present in organic forms of the element, i.e. selenomethionine and selenium-containing proteins [13, 20], the volunteers’ GPx1 status would not be significantly affected, particularly at the conservative levels of supplementation used in this study. This hypothesis is supported by Neve [21], who concluded that, although organic forms of selenium increased blood-selenium concentrations to a greater extent than inorganic forms, the latter had a greater effect on GPx production. Brown et al. [22], who fed volunteers pure selenomethionine, reported that GPx activity showed little or no response to supplementation, despite the plasma selenium concentration increasing. Similarly, from a study where long-term supplementation with selenate and selenomethionine had been carried out, Thomson et al. [23] concluded that selenomethionine was quickly incorporated into a general tissue-protein pool, while inorganic selenate was more directly available for GPx synthesis. Neve et al. [24] reported that GPx1 activity was only affected after 45 days of dietary intervention with selenomethionine (at 100 μg/day), a conclusion which may explain the response observed in the current study.
The work presented here was part of a multi-disciplinary investigation into the physicochemical properties and bioavailability of selenium from enriched sourdough bread, developed as a potential vehicle for dietary supplementation. If the issue surrounding the lack of effect on GPx1 status is to be addressed, any future study would need to be conducted over a much longer intervention period (possibly up to 3 months) and at a higher level of enrichment (probably 100 μg day−1).
References
Combs GF Jr (2001) Selenium in global food systems. Br J Nutr 85:517–547
Wasowicz W, Gromadzinska J, Rydzynski K, Tomczak J (2003) Selenium status of low-selenium area residents: Polish experience. Toxicol Lett 137 (1–2):95–101
Reilly CW (1996) Selenium in food and health. Blackie Academic & Professional, London
Rayman MP (2000) The importance of selenium to human health. Lancet 356:233–241
Beck MA, Shi Q, Morris VC, Levander OA (1995) Rapid genomic evolution of a non-virulent Coxsackievirus B3 in selenium deficient mice results in selection of identical virulent isolates. Nat Med 1(5):433–436
Nelson HK, Shi Q, Van Dael P, Schiffrin EJ, Blum S, Barclay D, Levander OA, Beck MA (2001) Host nutritional selenium status as a driving force for influenza virus mutations. FASEB J 15:1846–1848
Broome CS, McArdle F, Kyle J, Andrews F, Hart CA, Arthur JR, Jackson MJ (2002) Functional effects of selenium supplementation in healthy UK adults. Free Radic Biol Med 33(Suppl 1):S261–S264
Combs GF Jr, Clarke LC (1999) Selenium and cancer. In: Heber D, Blackburn GL (eds) Nutrition oncology. Academic, New York, pp 125–222
Ganther HE (1999) Selenium metabolism, selenoproteins and mechanisms of cancer prevention: complexities with thioredoxin reductase. Carcinogenesis 20:1657–1666
Arthur JR, McKenzie RC, Beckett GJ (2003) Selenium in the immune system. J Nutr 133:1457S–1459S
Ravaglia G, Forti P, Maioli F, Bastagli L, Facchini A, Mariani E, Savarino L, Sassi S, Cucinotta D, Lenaz G (2000) Effect of micronutrient status on natural killer cell immune function in healthy free-living subjects aged >/=90y. Am J Clin Nutr 71:590–598
Ursini F, Heim S, Kiess M, Maiorino M, Roveri A, Wissing J, Flohe L (1999) Dual function of the selenoprotein PHGPx during sperm maturation. Science 285:1393–1396
Bryszewska MA, Ambroziak W, Diowksz A, Baxter MJ, Langford NJ, Lewis DJ (2005) Changes in the chemical form of selenium during the manufacture of a selenium-enriched sourdough bread for use in a human nutrition study. Food Addit Contam 22:135–140
Gujska E, Majewska K (2005) Effect of baking process on added folic acid and endogenous folates stability in wheat and rye breads. Plant Foods Hum Nutr 60(2):37–42
Belsten JL, Wright AJ (1995) European community-FLAIR common assay for whole-blood glutathione peroxidase (GSH-Px): results of an inter-laboratory trial. Eur J Clin Nutr 49(12):921–927
Smith PK, Krohn RI, Hermanson GT, Mallia AK, Gartner FH, Provenzano MD, Fujimoto EK, Goeke NM, Olson BJ, Klenk DC (1985) Measurement of protein using bicinchoninic acid. Anal Biochem 150(1):76–85
Zachara B, Wasowicz W (1994) Selenium concentration in blood components of Polish sub-populations and in some other countries. Proceedings of the Scientific Session of the Polish Academy of Sciences. Arsenic and selenium in the environment. Polish Academy of Sciences, Warszawa, pp 104–109
Department of Health (1991) Dietary reference values for food energy and nutrients for the UK, COMA. HM Stationary Office, London
Ziemlanski S, Wartanowicz B, Panczenko-Kresowska J (1998) Zmiany w stanie zdrowia osób w wieku podeszlym z Warszawy w okresie 5 lat. Zyw Czlow Metab 2:111–121
Bryszewska MA, Ambroziak W, Rudzinski J, Lewis DJ (2005) The use of HPLC-ICP-MS to investigate the distribution of selenium in wheat flour proteins. Anal Bioanal Chem 382:1279–1287
Neve J (1995) Human selenium supplementation as assessed by changes in blood selenium concentration and glutathione peroxidase activity. J Trace Elem Med Biol 9:65–73
Brown KM, Pickard K, Nicol F, Beckett GJ, Duthie GG, Arthur JR (2000) Effects of organic and inorganic selenium supplementation on selenoenzyme activity in blood lymphocytes, granulocytes, platelets and erythrocytes. Clin Sci 98:593–599
Thomson CD, Robinson MF, Butler JA, Whanger PD (1993) Long-term supplementation with selenate and selenomethionine: selenium and glutathione peroxidase (EC 1.11.1.9) in blood components of New Zealand women. Br J Nutr 69:577–588
Neve J, Vertongen F, Capel P (1988) Selenium supplementation in healthy Belgian adults: response in platelet glutathione peroxidase activity and other blood indices. Am J Clin Nutr 48:139–143
Acknowledgements
This study was carried out with financial support through EC contract IC-IT-98-0193, “Improved Methods for the Production of Polish and Ukrainian Fermented Foods (IMPPUFF)”. MAB gratefully acknowledges KBN grant 6-P06G-057-20. Neill Walker is thanked for his contribution to discussions regarding the statistical approaches used in this work. This paper is dedicated to Rodger, brother of JL, who passed away, unexpectedly, during preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bryszewska, M.A., Ambroziak, W., Langford, N.J. et al. The Effect of Consumption of Selenium Enriched Rye/Wheat Sourdough Bread on the Body’s Selenium Status. Plant Foods Hum Nutr 62, 121–126 (2007). https://doi.org/10.1007/s11130-007-0051-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11130-007-0051-y