
Abstract
While psychiatric disorders are common among juvenile delinquents, many mental health problems go undetected, increasing the likelihood for persistent difficulties. This is the first known study to examine mental health referral rates and recidivism in the juvenile justice system. In addition to the study, we review juvenile justice mental health screening to improve detection and treatment. Juvenile criminal records in conjunction with behavioral health screenings were analyzed to determine differences in referrals and recidivism among first time offenders. Recidivism rates were significantly lower (p = 0.04) and time to recidivism was significantly longer (p = 0.03) for those referred specifically for mental health services than for those without any referrals, even after adjusting for offense severity. While black youths had a significantly higher recidivism rate (p = 0.02) and a shorter time to recidivism (p = 0.009) than white youths, there was no significant difference between races when referred specifically for mental health services. Among the groups studied, black youths had the most profound positive effect from mental health referrals (p < 0.0001). This study indicates the importance of detecting mental health problems among juvenile delinquents, especially for black offenders. The apparent protective effect of mental health interventions necessitates screening that better identifies underlying psychosocial factors rather than strict reliance upon diagnostic criteria and self-report. Broader or even universal mental health referrals for juvenile offenders could reduce future legal system involvement and costs to society. We review potential reasons that mental health problems go undetected and provide recommendations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of psychiatric disorders in the juvenile justice population may be as high as 85 %, but less than half of these youths are identified [1, 2]. Mental health referrals generally depend on the cooperation and reliability of the youth (in a confined and legally threatening environment), and criteria from the Diagnostic and Statistical Manual. The use of subjective information provided during intake to the justice system may rely too heavily on openness in a legal situation where an individual may be reluctant to disclose information, especially when the first words uttered to the offenders on their way to detention are: “you have the right to remain silent.” This almost certainly results in undertreatment, which is supported by a study finding 69 % of non-referred youths in juvenile detention meet criteria for psychiatric disorders [3]. Criteria-specific symptom screening may also overlook psychosocial factors influencing criminal behavior that do not meet the threshold for diagnosis, but can improve with mental healthcare nonetheless. For example, family adversity, poor parenting skills, parental criminality, parental psychiatric disturbance, abuse, neglect, abandonment, broken homes, violence, overcrowding, and low socioeconomic status have been associated with juvenile criminality [4–8]. Trauma, with and without resultant posttraumatic stress disorder, is pervasive among juvenile delinquents and puts them at greater risk for recidivism [6–8]. The etiology of criminal behavior may not be evident, especially if juveniles are reluctant to disclose information such as stressors, in a legal setting. Furthermore, when screeners are looking only for “mental illness,” they are apt to miss more general mental health problems that cause significant dysfunction without meeting criteria for a disorder.
It is important not to assume that all criminal behavior implies conduct disorder (CD), or that all youths with CD develop antisocial personality disorder (ASPD). Only about 30 % of those with CD develop ASPD based on average prevalence, but many more develop mood disorders, anxiety disorders and PTSD, suggesting other factors besides psychopathy/sociopathy are implicated in child and adolescent criminal behavior [9]. Those with CD and oppositional defiant disorder commonly also have depression and anxiety, and CD and childhood depression often predict the comorbidity of each other [10].
Simply presenting to the juvenile justice system is a strong indicator of likely externalizing problems (e.g., hyperactivity, impulsivity, aggression), underlying psychosocial problems, and poor coping skills. Many studies have demonstrated that juvenile delinquents are more likely to have problem-solving and social skills deficits which may increase the likelihood of seeking inappropriate or illegal solutions to problems they have an inability to deal with effectively [2]. Criminal behavior among youths can be understood as externalizing behavior related to underlying conflicts within poorly developed psychic structures and unfulfilled psychological needs, further limited by age and immaturity. Externalizing behaviors can be observed in many psychiatric disorders outside of CD, and even in those that do not meet criteria for a specific disorder. For example, childhood hyperactivity, whether or not a part of attention-deficit hyperactive disorder (ADHD), is related to criminal behavior [4]. Persistent juvenile delinquency, itself, is known to be significantly correlated with persistent substance use, persistent internalizing problems (e.g., depression, anxiety, social withdrawal), and ADHD [1, 11]. Childhood psychiatric disorders predict future criminal behavior, even when controlling for past criminal behavior, especially when two or more of the following are comorbid: depression, anxiety, substance use and CD [12]. Interventions such as social skills training have been found to be effective in improving deficits in dealing with these problems, increasing an internal locus of control, and reducing recidivism [2]. Delivering mental health services to juvenile delinquents likely mitigates the risk for recidivism by treating underlying mental health problems.
Unfortunately, there is a paucity of studies—and few recently—about mental health interventions for juvenile delinquents. Those that exist tend to focus on mental health treatment independent of the justice system (e.g., any treatment prior to an arrest) [13, 14], assess referral rates without assessing outcomes (e.g., recidivism) [15, 16], or focus on a single intervention type (e.g., social skills training, multisystemic therapy). This study aims to build upon existing research and, to the authors’ knowledge, is the first study of juvenile delinquents to assess referral rates and recidivism. There is evidence that mental health care prior to juvenile justice involvement can reduce initial offenses and recidivism, especially for serious offenses [13]. Ours is the first known study to focus on recidivism and mental healthcare initiated after the initial offense.
We hypothesize that all offenders would benefit from mental health referrals, and that such services would therefore reduce recidivism. Intervention during the time spent in juvenile detention facilities is especially important because many experts believe that this time can worsen preexisting mental health problems and (further) traumatize youths [13]. Providing mental health services to juvenile offenders may help the justice system to recognize and treat underlying psychopathology, improve coping skills, reduce the negative effects of detention, and decrease future costs to society by reducing recidivism. Our goal is that this initiative will serve as a pilot study for a randomized controlled trial comparing outcomes between universal mental health referrals for first time offenders and referrals as usual.
Methods
Participants
All protocols were approved by the Wright State University Institutional Review Board. Participants were youths (n = 54), aged 14 to 16 years, processed at the Montgomery County Juvenile Justice Center in Dayton, Ohio for their first offense. Data was retrospectively collected from records dated January 23, 2010 (the earliest available electronic medical record) to April 29, 2013. Potential participants were excluded if, when charged, they were aged ≤13 years or ≥17 years, had any previous arrests or incarcerations, had any previous mental health treatment, were arrested only for illicit drug charges (which are managed separately in a drug court and use different mental health services), were not released from detention prior to completion of the study, or if they were referred to the adult criminal system (which is processed and managed separately). The mean age was 15.5 (SD = 0.5) years, 24.1 % were female, 68.5 % were black, and 27.8 % were white. Race was not documented for two youths, who were excluded from analyses that included race. Follow up lasted until a participant recidivated, aged out of the system, or the study was complete, whichever came first.
During processing, participants were screened by justice center mental health staff (i.e., licensed counselors or social workers). 30 (55.6 %) were referred for mental health services, based on the clinical judgment of their behavioral health screeners. Those referred were referred for child and adolescent psychiatry and/or psychotherapy, within the juvenile detention center or in a community mental health center if incarcerated or not, respectively. Despite our intention to exclude participants with substance-related problems (for reasons described earlier and in the discussion), 19 participants were referred for alcohol or other drug (AOD) services. Therefore, we defined the following groups: mental health only (MH Alone, n = 17), No Referral (n = 18), mental health referrals with or without AOD referrals (Total MH, n = 30), no mental health referral with or without AOD referrals (No MH, n = 24), and mental health or AOD referral (Any Referral, n = 36).
Statistical Analyses
Outcome variables were referral rate, recidivism rate (the proportion of individuals who recidivated before the end of the study), and time to recidivism. Those who did not recidivate before study completion are considered right-censored (their time to recidivism is known only to be greater than their time on study). Our primary analyses of recidivism rates and time to recidivism exclude AOD referrals, comparing MH Alone and No Referral. Secondary analyses compare Total MH and No MH.
We adjusted analyses based on offense severity. Severity levels for first and second offenses were determined using a 1–10 scale created by the authors based on the level of the offense (1 = unruly charge, 2 = fourth degree misdemeanor, 3 = third degree misdemeanor, 4 = second degree misdemeanor, 5 = first degree misdemeanor, 6 = fifth degree felony, 7 = fourth degree felony, 8 = third degree felony, 9 = second degree felony, 10 = first degree felony). Offense severity was analyzed both as a continuous variable, and dichotomized as “Misdemeanor/Unruly” vs. “Felony” for simple comparison of lesser and greater offenses (realizing that unruly charges are a status offense). For participants who recidivated, the Wilcoxon signed rank test was used to compare severity levels between first and second offenses. All hypothesis tests were two-sided and at the 0.05 level of significance. Analyses were carried out in R 3.1.2 [17]. Cox regression was carried out using the coxphf package [18].
Fisher’s Exact Test was used to compare rates between referral groups, sexes, races, and dichotomized first offense severity. Logistic regression was used to test for association between first offense severity level (as a continuous variable) and rates, and to conduct covariate adjusted comparisons. Comparisons of rates are expressed as odds ratios (OR). Kaplan–Meier survival curves were used to illustrate the distribution of time to recidivism. Cox proportional hazards regression and likelihood ratio tests were used to compare time to recidivism between referral groups, sexes, races, and dichotomized first offense severity, to test for associations between first offense severity level (as a continuous variable) and time to recidivism, and to conduct covariate-adjusted comparisons. Comparisons of time to recidivism are expressed as hazard ratios (HR). Sex, race and referral group comparisons are “male vs. female,” “white vs. black,” and “MH Alone vs. No Referral,” and “Total MH vs. No MH,” respectively. An OR > 1 indicates that the group to the right of the “vs.” has the higher rate and, for HR > 1, a shorter time to recidivism.
Results
Table 1 summarizes descriptive statistics for the total sample, and the primary analysis sample which excludes AOD referrals. Of the total participants, 51.9 % reoffended during the follow-up period. For those who recidivated, the average time to recidivism was 221 days. For those who did not, the average time on study was 624 days. Tables 2 and 3 summarize referral rates and recidivism rates, respectively.
Participants were charged with the following initial offenses: theft (15 %), burglary (13 %), domestic violence (9 %), robbery (7 %), aggravated robbery (7 %), illegal conveyance of a deadly weapon (7 %), breaking and entering (4 %), felonious assault (4 %), assault (4 %), disorderly conduct (4 %), and other offenses committed by a single participant (26 %). Approximately 54 % of the initial offenses were felonies, 39 % were misdemeanors and 7 % were unruly charges (e.g., truancy).
Recidivating participants were charged with the following re-offenses: truancy (11 %), theft (7 %), assault (7 %), unruly (7 %), offenses involving underage persons (7 %), curfew violation (7 %), criminal trespassing (7 %), and other offenses committed by a single participant (47 %). Approximately 43 % of re-offenses were misdemeanors, 36 % were unruly charges and 21 % were felonies. The median severity level of the re-offense (4.5) was significantly lower (p = 0.0001) than that of the initial offense (6.0).
First offense severity—dichotomized or as a continuous variable—was not significantly associated with referral rate for MH Alone (p = 0.5661, p = 0.2601, respectively), Total MH (p = 1.0000, p = 0.1431), or any referral (p = 0.7765, p = 0.1294). A one unit decrease in first offense severity was associated with an increase of 4 % in mean time to recidivism (HR = 1.04, p = 0.6430), but this effect was not statistically significant.
Referral Types
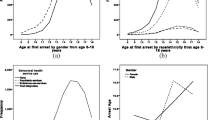
Of the total sample, 31.5 % were referred to MH Alone, and 56.0 % were referred to Total MH. In our primary analysis, recidivism rate was significantly greater (OR = 4.57, p = 0.0437) for those with No Referral (66.7 %) than for MH Alone (29.4 %), and mean time to recidivism was significantly (197 %) greater for MH Alone (HR = 2.97, p = 0.0326). Figure 1 displays the Kaplan–Meier survival curves for MH Alone and No Referral.

Product-limit survival estimates based on referral type, sex, and race
In our secondary analysis, when including AOD referrals, recidivism rate was greater for No MH (62.5 %) than Total MH (43.3 %), but the difference was not statistically significant (OR = 2.15, p = 0.1828). Similarly, Total MH had an average time to recidivism (73 %) greater than No MH, but the difference was not statistically significant (HR = 1.73, p = 0.1509).
After adjusting for first offense severity, recidivism rate remained significantly greater for No Referral compared to MH Alone (OR = 6.83, p = 0.0196), and time to recidivism remained significantly greater among MH Alone (HR = 3.12, p = 0.0271). When comparing time to recidivism between Total MH and No MH, adjusted for first offense severity, there was a significant interaction between severity and group (p = 0.0119). For those with non-felony offenses, the two groups did not differ significantly (HR = 0.76, p = 0.6074). However, for those with felonies, time to recidivism was significantly longer for Total MH (HR = 3.80, p = 0.0211).
Sex Differences
Females had a higher referral rate than males, but the difference was not statistically significant for MH Alone (OR = 1.50, p = 0.7328), Total MH (OR = 1.37, p = 0.7527), or Any Referral (OR = 1.90, p = 0.5061). There was no significant difference in recidivism rate between sexes (OR = 0.74, p = 0.7540). Figure 1 displays the Kaplan–Meier survival curves for the two sexes. Males had an average time to recidivism that was 25 % shorter than females (HR = 0.75, p = 0.5166), but the difference was not statistically significant. For those with mental health referrals, males had a longer (but still non-significant) average time to recidivism (HR = 5.74, p = 0.0590 for MH Alone; HR = 1.84, p = 0.3011 for Total MH).
When comparing MH Alone and No Referral, and Total MH and No MH, there was a significant interaction between sex and group for both recidivism rate (p = 0.0398 and p = 0.0201, respectively) and time to recidivism (p = 0.0136 and 0.0154, respectively). In each case, for males, the groups with mental health referral (MH Alone and Total MH) had significantly lower recidivism rates (OR = 0.38, p = 0.0063 for MH Alone vs. No Referral; OR = 4.70, p = 0.0279 for Total MH vs. No MH) and longer time to recidivism (HR = 7.64, p = 0.0017 for MH Alone vs. No Referral; HR = 2.81, p = 0.0182 for Total MH vs. No MH). For females, the effects were in the opposite direction but not significant (rate: OR = 0.38, p = 1.0000 for MH Alone vs. No Referral; OR = 0.18, p = 0.2657 for Total MH vs. No MH; time: HR = 0.40, p = 0.4033 for MH Alone vs. No Referral; HR = 0.26, p = 0.1656 for Total MH vs. No MH).
Racial Differences
White youths were more likely to receive mental health referrals than black youths, and this difference was statistically different for MH Alone (OR = 0.16, p = 0.0069) but not for Total MH (OR = 0.53, p = 0.3688) or any referral (OR = 0.60, p = 0.5320). Recidivism rate was significantly higher (OR = 4.91, p = 0.0161) for black (64.9 %) than for white youths (26.7 %). Among those with mental health referrals, this difference became non-significant (OR = 0.81, p = 1.000 for MH Alone; OR = 2.51, p = 0.4335 for Total MH), which is displayed in Fig. 2. Recidivism rate was significantly higher among black youths who received No Referral than black youths who received MH Alone (p < 0.0001), but there was no significant difference in recidivism rates between MH Alone and No Referral among white youths (p = 0.2931).

Recidivism rates by race
Figure 1 displays the Kaplan–Meier survival curves for white and black youths. White youths had an average time to recidivism that was significantly longer (252 %) than black youths (HR = 3.52, p = 0.0086). When adjusting for race, time to recidivism (HR = 2.30, p = 0.1158) and recidivism rate (OR = 3.39, p = 0.1134) was no longer significantly different between MH Alone and No Referral. Although there was not a significant interaction between race and group, when stratifying by race, time to recidivism was significantly longer in the MH Alone group for black youths (HR = 4.05, p = 0.0383).
Discussion
Recidivism by Referral Type
As expected, the primary comparison in this study was statistically significant: the recidivism rate was significantly higher, and the time to recidivate was significantly shorter among those without any referrals than those with mental health referrals. Mental healthcare likely reduces recidivism by treating underlying psychopathology and addressing unmet psychological needs; lowering the youth’s stress, shame and anger from legal involvement; and mitigating the effects of legal involvement such as interrupted school attendance, identification with criminality, and potential exposure to other dangerous youths or negative behaviors. Furthermore, reduced recidivism lowers costs to society, both in harms to potential victims, and financial burden to society by reducing legal processing and incarceration costs. Failure to address behaviors can lead to perpetual recidivism and the youth identifying with inherent wrongdoing, acceptance of ineffective efforts to meet their psychological needs, and developing futile appraisal of their future. The individual and societal benefits of reduced recidivism make mental health interventions a worthwhile endeavor. Based on these results, increased usage of referrals or universal mental health referrals for all juvenile offenders may target developmental problems and greatly reduce recidivism. Some have even suggested that integrating juvenile justice and community mental healthcare systems may reduce criminal behavior [13].
When including AOD referrals, recidivism differences were only significant in males and those with a felony as their first offense. The reason we initially planned to exclude substance users is that those receiving AOD referrals should not necessarily be collapsed together with those with mental health referrals or those without any referrals. Previous studies have reported this collapsing together as a limitation and have recommended examining the services separately [15]. To this end, efforts were taken to exclude the juvenile drug court from our sample, but some participants were still referred for AOD services despite not entering the drug court system. In hindsight, this was to be expected considering the near ubiquity of substance use among offenders. However, this means the AOD referral population in this study is not representative of the whole substance using juvenile delinquent population. Therefore, our primary analysis excluded those receiving AOD referrals, and compared those receiving mental health referrals alone to those without any referrals. Among the four intervention groups, those without any referrals had the highest recidivism rate, followed by those with mental health and AOD referrals, AOD Alone, and MH Alone. One might expect those getting the most help (i.e., both a mental health and AOD referral) would have the least recidivism. However, the fact that those receiving both referrals have more recidivism than receiving either alone is likely indicative of substance use causing more severe problems and more treatment-resistance. Substance use is known to increase recidivism rates [8], likely because of impairing judgment, increasing interaction with criminals, and because youth substance use, itself, is a crime. This added risk factor may offset some of the protective effect of mental health services.
Offense Severity
For those who recidivated, re-offense severity levels were significantly lower than the severity levels of the first offenses. This finding may be explained by: punishment deterring or decreasing the severity of future criminality, lower threshold for punishing previous offenders, previous offenders being monitored more closely (e.g., lesser offenses that went unnoticed or unpunished previously are punished when the offender is on probation), and/or by the fact that the majority of the total participants were referred to mental health which reduced the mental health factors that contribute to criminality. This may also expose a potential limitation of this study: juvenile justice records may not always accurately measure recidivism (e.g., youths recidivating without being arrested).
This study also found that the severity of the first offense did not influence recidivism, but mental health referrals had a greater positive impact on those with more serious first offenses. This provides hope regarding even the worst offenders: that intervention for all offenders, even the most severe, can reduce recidivism. However, another possibility is that more severe offenses likely to result in longer sentences, decreasing the period of time during the study in which participants were out of detention (i.e., had an opportunity to recidivate). Future studies measuring recidivism with consideration for length of incarceration may elucidate this finding.
Racial Differences
A surprising finding was that, while offense severity and the sex of offenders did not have a statistically significant impact on recidivism, race did. Recidivism rates are significantly higher, and time to recidivate is significantly shorter among black than white youths. Though our statistically significant findings must be given appropriate weight, especially in view of the small sample size, these findings are generally consistent with previous studies that have found juvenile justice involvement is more likely for non-white youths [13, 14]. In accordance with our hypothesis that youth criminal behavior is associated with underlying mental health problems, this may indicate that black youths have increased mental health needs. This is supported by evidence that black juvenile delinquents have the highest rates of psychiatric disorders among all delinquents [15], and black populations, in general, are 30 % more likely to have a disorder compared to non-Hispanic white populations [19]. Black children are also more likely to experience physical abuse, sexual abuse, neglect, violence and broken homes than white children [15, 20], which puts them at greater risk for mental health problems. It may also be related to substance use. While some studies indicate there is no racial difference in substance use within the juvenile justice system [15], black youths in this study were more likely to receive AOD referrals, indicative of substance use (a predictor of recidivism, as stated above), than white youths (likely why black youths were less likely to receive MH alone). Higher recidivism risk among black youths is likely explained by increased presence of underlying psychopathology, psychosocial stressors (e.g., trauma), and substance use.
Though black youths are known to have more mental health problems, there was no statistical difference between the total mental health referral rates of black and white youths. This suggests there are many black offenders who would benefit from mental health services but are not getting referred. Potential explanations include an inherent bias making screeners less likely to detect or refer black youths with mental health problems, and/or black youths being less likely to disclose mental health concerns. Evidence for the former point is unclear as some studies suggest black juvenile delinquents are less likely to receive referrals while others suggest they are more likely [15, 16]. Racial bias preventing black youths from getting the care they need is less likely in our study based on black youths being more likely to receive any mental health, or combined mental health and AOD referrals than white youths. It is more likely that the strongest factor is black youths being reluctant to self-report psychosocial stressors, traumas, and other mental health problems. This has been repeatedly demonstrated in black populations, who are less likely to seek help for mental health than white populations [15–25].
Importantly, when black youths received mental health referrals, they did as well as white youths with referrals, with respect to recidivism. Indeed, when stratifying by race, mental health referrals had a more profoundly positive effect on black youths than any other group studied (in fact, white youths had no significant difference). This suggests that screeners need better methods for detecting mental health problems and thresholds for referring juveniles should be lowered, especially for those with recidivism risk factors (e.g. black, male, substance use).
Improving Mental Health Screening and Referrals
Possible reasons for a reluctance to self-disclose mental health problems and self-reports being highly censored are described in Table 4, including findings based on our extensive review of mental health screening in juvenile offenders. While some factors may be more common among black youths (e.g., stigma, overvaluing self-reliance, a lack of knowledge about mental health, distrust of clinicians from different backgrounds, fear of discrimination, cultural mandate to protect black abusers or violent offenders) [15, 16, 19, 24, 25], most of these deterrents to being forthcoming apply to all juvenile delinquents. For example, while over 90 % of juvenile offenders have a trauma history and up to 49 % have PTSD, there are low rates of disclosing trauma (e.g., only 26 % of sexually abused youth report it within a year, and self-disclosure is even less likely when the youth is connected to the abuser through the community, e.g., a parent, friend, teacher, coach) [33].
Those screening or treating mental health problems in juvenile delinquents can better help these troubled youths with methods recommended in Table 5. We include recommendations by the Consensus Conference on Mental Health Assessments in Juvenile Justice Settings [1], and the American Academy of Child and Adolescent Psychiatry [26]. Improved screening and psychoeducation can enhance self-awareness of previously unrecognized problems, how they can manifest in behavior, and increase the perceived need for treatment. This is especially important considering that self-awareness of mental and emotional status has been positively linked to mental healthcare utilization among black populations, who in general are less likely to recognize mental health symptoms as problems [25]. It is important to realize that the juvenile justice system is often the first contact with mental healthcare that these youths have ever had [15]. No assumptions should be made about mental health literacy. It is equally important that screeners realize the importance of treating mental health problems and their effect on behavior. Too often psychosocial problems (e.g., a history of trauma) and developmental problems (e.g., a youth clearly not on the same track as their peers) are recognized but not referred for treatment simply because the youth does not meet symptomatic criteria for a disorder (criteria which are almost always for adults, and may not necessarily or accurately apply to children and adolescents). With regards to development, one could surmise that earlier deficits in the formation of trust, emotional regulation, and competency can bring a youth into adolescence at a disadvantage for developing peer relationships and becoming more independent from parents. Juvenile justice involvement, though often necessary, highlights the youth’s misstep at striving towards independence within societal norms.
Those that refer juveniles to mental health vary in training and roles (e.g., psychiatrists, psychologists, nurses, social workers, licensed counselors, judges, detention center staff, probation officers, parents). In most cases, screeners will require and benefit from training specific to mental health in the juvenile justice system (in addition to general mental health training) to improve interviewing techniques and diagnostic skills, and direct supervision by credentialed professionals for those who are not credentialed themselves.
We recommend research to validate juvenile recidivism risk assessment instruments for screening. While many studies have assessed risk factors, most screening and treatment decisions are still based on clinician perceptions [29]. The present system requires subjective self-report of symptoms or suggestive collateral history to prompt referral, whereas an improved instrument could introduce an index of risk that correlates with mental health problems and recidivism.
Limitations and Recommendations for Future Research
Limitations of this study include site-specific demographics and methods for referral, retrospective data collection, and juvenile justice records as a source for data. Additionally, this study does not address duration or quality of interventions. Due to limited access to data we were unable to determine exactly what services participants received once referred. While our lack of consistent intervention (e.g., multisystemic therapy [30]) may be viewed as a limitation, it makes the study more naturalistic and, more importantly, the fact that recidivism significantly improved despite a non-specific treatment modality suggests that any mental healthcare is likely protective. Nevertheless, not all interventions are panaceas, as indicated by findings that up to 45 % of those referred to community mental health systems after juvenile detention still have impairment associated with psychiatric disorders 5 years later [31].
Because this study lacks randomization, we cannot eliminate possible confounding factors differentiating referral groups that may influence recidivism. To the contrary, the factor we predicted to most likely influence referrals was offense severity, which was actually found to not have a significant influence. Nevertheless, even if those referred are more likely to only engage in criminal behavior briefly and those not referred are more likely to have “life-course-persistent antisocial behavior,” the latter group still warrants treatment—and likely even more significant interventions for their neuropsychological problems and criminogenic environments [32]. We hypothesize that mental health treatment would still have a positive effect in randomized studies even in those who would otherwise screen negative, indicating mental health problems are not being detected by current screening methods, but further research is needed.
The chief limitation of the study, small sample size, is largely due to strict inclusion criteria. The age criteria was chosen because the typical age of first offenses in this center is 14–16, offenses prior to 14 are rare and often unusually severe, and youths no older than 16 were selected to allow for significant time of follow up prior to aging out of the juvenile system. We also excluded those with prior mental health and legal histories, and drug possession charges, to eliminate potential variables and specifically focus on early mental health interventions for first time offenders. Our hypothesis was that mental health problems are a factor in criminality and treatment can reduce recidivism, even for those without obvious risk factors (e.g., prior mental health treatment, prior legal involvement, early age of first offense). Despite the small sample size and strict inclusion criteria, statistically significant findings were demonstrated. Nevertheless, this pilot study demonstrates a need for additional and larger studies to examine the impact of mental health services on future criminal behavior. Our initial plan was to assess several additional factors (e.g., trauma history, academic problems, parental factors), but these factors were not consistently assessed or documented in the records. That speaks to the importance of our recommendations that these factors always be assessed in juvenile offenders, and also reinforces our goal that future studies will be able to have the funding and support necessary to train screeners and track these important factors.
We believe our findings warrant future research about the cost of referrals, which we hypothesize would demonstrate that increased funding for early mental health interventions would significantly reduce total public spending on these youths later in life (e.g., the cost of legal proceedings and imprisonment, mental and general healthcare services, unemployment compensation and entitlement subsidies, lost tax revenue from greater time spent unemployed and incarcerated) [27, 28]. Cost-benefit analyses may evoke action on the part of policy-makers.
Conclusion
This study found a favorable impact of mental health interventions on recidivism among youths involved in the juvenile justice system, but suggests that current screening and referral procedures are inadequate. Subjective screening should not be taken at face value as the sole determinant of psychopathology or disposition. Juvenile delinquents are children and adolescents with externalizing behaviors that can pose danger to others, and incur great social costs required to facilitate the legal process and subsequent sentencing disposition, to include incarceration. Interventions to address the individual mental health needs of offending youths can serve to reduce externalizing psychopathology, reduce recidivism, intervene in adolescent development, and also limit the burden of cost to society. This is especially true for black youths, who have been consistently shown in this and previous studies to be more likely to be involved in the juvenile justice system (and often under-referred), but have as good of outcomes as white youths when receiving mental health referrals after first-time offenses. For these reasons, improving mental health screening, expanding the amount of mental health referrals among initial offenders and, perhaps, even universally referring all juvenile offenders would be beneficial for these youths, their families and society as a whole. It is important to remember that juvenile delinquents are developing children, many of whom have developmental problems. The juvenile justice system cannot rely solely on punishment as a means of reducing crime and must utilize interventions addressing the underlying deficits and dysfunction that are driving behaviors. Sometimes curbing criminal behavior requires going beyond the basics of teaching right and wrong, and simply providing consequences. Having a mental health problem does not imply a lack of responsibility for behavior, and even depressed and traumatized children need to learn that their behavior has consequences. However, for those making polices, and those processing, screening and treating juvenile offenders, it is important to consider the old adage: the reason these children behave “bad” is often because they are mad and sad—and we can help with that.
References
Wasserman GA, Jensen PS, Ko SJ, et al.: Mental health assessments in juvenile justice: Report on the consensus conference. Journal of the American Academy of Child and Adolescent Psychiatry 42(7):752–761, 2003.
Cunliffe T: Arresting youth crime: A review of social skills training with young offenders. Adolescence 27(108):891–900, 1992.
Rogers KM, Pumariega AJ, Atkins DL, et al.: Conditions associated with identification of mentally ill youths in juvenile detention. Community Mental Health Journal 42(1):25–40, 2006.
Elander J, Simonoff E, Pickles A, et al.: A longitudinal study of adolescent and adult conviction rates among children referred to psychiatric services for behavioural or emotional problems. Criminal Behaviour and Mental Health 10(1):40–59, 2000.
Mulder E, Brand E, Bullens R, et al.: Risk factors for overall recidivism and severity of recidivism in serious juvenile offenders. International Journal of Offender Therapy and Comparative Criminology 55(1):118–135, 2011.
Moore E, Gaskin C, Indig D: Childhood maltreatment and post-traumatic stress disorder among incarcerated young offenders. Child Abuse and Neglect 37(10):861–870, 2013.
Ryan JP, Williams AB, Courtney ME: Adolescent neglect, juvenile delinquency and the risk of recidivism. Journal of Youth and Adolescence 42(3):454–465, 2013.
Dembo R, Turner G, Sue CC, et al.: Predictors of recidivism to a juvenile assessment center. International Journal of the Addictions 30(11):1425–1452, 1995.
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edn. Arlington, VA, American Psychiatric Association, pp. 469–475, 659–663, 2013.
Brensilver M, Negriff S, Mennen FE, et al.: Longitudinal relations between depressive symptoms and externalizing behavior in adolescence: Moderating effects of maltreatment experience and gender. Journal of Clinical Child & Adolescent Psychology 40(4):607–617, 2011.
Loeber R, Stouthamer-Loeber M, White HR: Developmental aspects of delinquency and internalizing problems and their association with persistent juvenile substance use between ages 7 and 18. Journal of Clinical Child Psychology 28(3):322–332, 1999.
Copeland WE, Miller-Johnson S, Keeler G, et al.: Childhood psychiatric disorders and young adult crime: A prospective, population-based study. American Journal of Psychiatry 164(11):1668–1675, 2007.
Foster EM, Qaseem A, Connor T: Can better mental health services reduce the risk of juvenile justice system involvement? American Journal of Public Health 94(5):859–865, 2004.
Cuellar AE, Markowitz S, Libby AM: Mental health and substance abuse treatment and juvenile crime. Journal of Mental Health Policy and Economics 7(2):59–68, 2004.
Rawal P, Romansky J, Jenuwine M, et al.: Racial differences in the mental health needs and service utilization of youth in the juvenile justice system. The Journal of Behavioral Health Services & Research 31(3):242–254, 2004.
Rogers KM, Zima B, Powell E, et al.: Who is referred to mental health services in the juvenile justice system? Journal of Child and Family Studies 10(4):485–494, 2002.
R: a language and environment for statistical computing. http://www.R-project.org. Accessed 27 Jan 2015.
Coxphf: Cox regression with Firth’s penalized likelihood. http://CRAN.R-project.org/package=coxphf. Accessed 27 Jan 2015.
Holden KB, McGregor BS, Blanks SH, et al.: Psychosocial, socio-cultural, and environmental influences on mental health help-seeking among African-American men. Journal of Men’s Health 9(2):63–69, 2012.
Lanier P, Maguire-Jack K, Walsh T, et al.: Race and ethnic differences in early childhood maltreatment in the United States. Journal of Developmental and Behavioral Pediatrics 35(7):419–426, 2014.
Snowden LR: Barriers to effective mental health services for African Americans. Mental Health Services Research 3(4):181–187, 2001.
Cheng TC, Lo CC: Racial disparities in intimate partner violence and in seeking help with mental health. Journal of Interpersonal Violence, 2014. doi:10.1177/0886260514555011.
Stevens-Watkins D, Sharma S, Knighton JS, et al.: Examining cultural correlates of active coping among African American female trauma survivors. Psychological Trauma 6(4):328–336, 2014.
Tillman S, Bryant-Davis T, Smith K, et al.: Shattering silence: Exploring barriers to disclosure for African American sexual assault survivors. Trauma, Violence, & Abuse 11(2):59–70, 2010.
Jang Y, Yoon H, Chiriboga DA, et al.: Bridging the gap between common mental disorders and service use: The role of self-rated mental health among African Americans. The American Journal of Geriatric Psychiatry, 2014. doi:10.1016/j.jagp.2014.02.010.
Penn JV, Thomas C: Practice parameter for the assessment and treatment of youth in juvenile detention and correctional facilities. Journal of the American Academy of Child and Adolescent Psychiatry 44(10):1085–1098, 2005.
Shepherd J, Farrington D, Potts J: Impact of antisocial lifestyle on health. Journal of Public Health 26(4):347–352, 2004.
Auty KM, Farrington DM, Cold JW: Intergenerational transmission of psychopathy and mediation via psychosocial risk factors. British Journal of Psychiatry 206(1):26–31, 2015.
Koegl CJ, Farrington DP, Augimeri LK: Clinician perceptions of childhood risk factors for future antisocial behavior. Journal of Clinical Child & Adolescent Psychology 38(4):564–575, 2009.
van der Stouwe T, Asscher JJ, Stams GJ, et al.: The effectiveness of multisystemic therapy (MST): A meta-analysis. Clinical Psychology Review 34(6):468–481, 2014.
Teplin LA, Welty LJ, Abram KM, et al.: Prevalence and persistence of psychiatric disorders in youth after detention: A prospective longitudinal study. Archives of General Psychiatry 69(10):1031–1043, 2012.
Moffitt TE: Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychological Review 100(4):674–701, 1993.
Peterson S, Negron-Munoz R, Levin A: Juvenile Offenders: Identifying PTSD, Court Concerns and Care. Ft. Lauderdale: American Academy of Psychiatry and the Law 46th Annual Meeting. Presented 22–25 Oct 2015.
Acknowledgments
We appreciate the Wright State University Boonshoft School of Medicine Department of Psychiatry for funding the statistical analysis of this research, Drs. William Klykylo and Christina Weston for assistance in the development of study protocol, and the Wright State University Department of Statistics and Dr. Harry Khamis for assistance in the development of study protocol and initial analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Zeola, M.P., Guina, J. & Nahhas, R.W. Mental Health Referrals Reduce Recidivism in First-Time Juvenile Offenders, But How Do We Determine Who is Referred?. Psychiatr Q 88, 167–183 (2017). https://doi.org/10.1007/s11126-016-9445-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11126-016-9445-z