
Abstract
The current study evaluated the differential-susceptibility hypothesis in explaining the intergenerational transmission of parenting, using data from the National Longitudinal Study of Adolescent Health (Add Health). Exposure to maternal parenting was measured prospectively when respondents were adolescents and parental stress was measured when they were parents themselves, some 14 years later, on average. Cumulative-genetic plasticity was measured by dominantly coding the presence of putative plasticity alleles from four genes: the 10R allele of DAT1, the A1 allele of DRD2, the 7R allele of DRD4, and the short allele of 5HTTLPR. Results showed that the more plasticity alleles individuals carried (range 0–4), the more that parenting experienced in adolescence predicted future parenting experience. Those respondents with the most plasticity alleles not only experienced the highest levels of parental stress when exposed to negative maternal parenting in adolescence but the lowest levels when exposed to positive maternal parenting in adolescence. These results indicate that differential susceptibility is operative in the case of the intergenerational transmission of parenting, which could explain why estimates of such transmission have proven so modest in studies which fail to consider GXE interactions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The question of why parents parent the way they do is one that has interested developmental scholars and lay persons for quite some time [7]. Although it is widely appreciated that parenting is multiply determined by individual, child and contextual factors [11], perhaps the pre-eminent hypothesis is that how parents were themselves treated as children shapes the ways in which they care for their progeny [60]. Indeed, a variety of theoretical perspectives embrace the view that parenting is intergenerationally transmitted, including life-course [35], attachment [19] and social-learning [3, 53] theories, even if they differ in terms of mechanisms presumed to account for the intergenerational transmission process.
There exists extensive evidence consistent with the claim that that parenting is transmitted across generations. Perhaps the earliest and best known is that pertaining to child maltreatment [5, 6, 26, 62], though much of the relevant data base has been called into question due to reliance on retrospective reports by adults of their rearing experiences; and this is because adults’ recollections of how they were treated in their families of origin are prone to memory errors of omission (i.e., not remembering) and commission (i.e., falsely remembering), as well as to distortion based on current life circumstances (e.g., [6, 8, 40, 65]).
Fortunately, longitudinal studies not reliant on adult recall provide evidence that harsh parenting or high levels of family discord are intergenerationally transmitted (e.g., [23, 44, 50, 55]). Oregon Youth Study investigators studying boys growing up in the highest crime-rate areas of a medium-sized city from age nine followed them up approximately 12 years later, observing that the more these fathers, as boys, experienced poor parental supervision and harsh discipline, the more they provided their toddlers with harsh, inconsistent discipline [22]. Conger and associates [29] obtained similar results for angry and aggressive parenting behavior in a subsample of rural Iowan adolescents followed up 5–7 years later when some of them had become parents. And drawing on a sample from high-risk Seattle neighborhoods, Bailey and colleagues [1] found that both monitoring and harsh discipline experienced around 13.5 years of age predicted the same kind of parenting some 14 years later when children were adults rearing nine-year olds.
It is not just angry-aggressive-hostile parenting, however, that seems to be intergenerationally transmitted. Chen and Kaplan [25] observed that in a large, random sample of 13-year-old Houston school children who were re-contacted in their 30s, the experience of good parenting in early adolescence, defined in terms of consistent discipline and parental acceptance, predicted the provision of constructive parenting in adulthood (i.e., monitoring, communication, involvement, positive affection, inductive discipline). Similar results emerged in a study of adolescent girls (age 13–18) growing up in Rochester, NY whose parenting was studied when they were 20–22 years old [64]. More recently, Belsky and associates [14] observed the parenting of New Zealand women followed since age three as they interacted with their own 3-year olds. These mothers were more likely to behave in a warm, sensitive, stimulating manner if, during early childhood, their own mothers did not hold authoritarian childrearing attitudes; if, during the middle-childhood years, the emotional climate of the family was marked by cohesion, positive expressiveness, and low levels of conflict; and/or if, during the early adolescent years, they experienced a trusting, openly communicative and non-alienated relationship with their parents.
A very recent set of reports published in a special section of the journal Developmental Psychology sought to illuminate the mediators of the intergenerational transmission process (e.g., [49]). Studying a normative sample beginning when children were 10 years old and then as parents some two decades later, Schaffer et al. [59] observed not only that parenting quality was intergenerationally transmitted, but that this process could be at least partially accounted for by the social competence which the children manifested in young adulthood before becoming parents. Relatedly, Neppl and associates [51] reported, after finding that the harsh and positive parenting that rural Iowan adolescents experienced predicted, respectively, the harsh and positive parenting they provided to their own preschool children, that whereas externalizing problems mediated the intergenerational transmission of harsh parenting, it was academic attainment which mediated the cross-generational linkage of positive parenting.
Despite long-standing evidence that parenting is intergenerationally transmitted, including recent work addressing mechanisms of influence, it remains indisputable that the parenting experienced in one generation is by no means inevitably repeated in the next [16, 48]. In fact, several recent studies indicate that only about 15% of the variance in parenting can be accounted for by one’s childrearing history [14, 22, 29], complementing earlier work chronicling a great deal of discontinuity in child maltreatment across generations (e.g., [34, 45]). These observations raise the question of why some parents do and some do not repeat the parenting they experienced while growing up. Although the editors of the aforementioned special section of Developmental Psychology bemoaned the lack of submissions addressing this fundamental concern [16, 30], there exists research investigating this topic (e.g., [13, 34]) discovered, for example, that mistreated children who did not mistreat their own offspring experienced supportive close relationships somewhere along their life-course journey, some with a therapist, others with a romantic partner, including a spouse. Quinton and Rutter [55, 56] called attention to relationship factors as well when it came to accounting for why some English girls whose experience in dysfunctional families which resulted in them growing up in residential institutions parented so much better than their own parents, whereas others did not.
Not considered to date, but central to the research reported herein, is the prospect that genetic factors might play a role in determining which individuals do and do not sustain parenting across generations, a possibility raised by Conger et al. [30] when highlighting the need for additional research on moderators of the intergenerational transmission of parenting. Here we test the gene-X-environment (GXE) interaction hypothesis that individuals carrying more of what Belsky and associates [12, 16] have hypothesized to be “plasticity alleles” prove to be those most likely to have their parenting experience influenced by the parenting they experienced while growing up. Important to appreciate is that the present work examining GXE interaction involving effects of mothering during adolescence on parenting stress in adulthood diverges from most prior GXE work in two fundamental respects. Whereas most GXE research to date is based on the diathesis-stress view that some individuals are more vulnerable than others to the negative effects of contextual adversity [12, 67], the work reported herein is based on the differential-susceptibility hypothesis [9, 10]. This stipulates that not only are certain individuals, often for genetic reasons [12], more prone to function poorly (e.g., become depressed) when confronted with stressful conditions (e.g., negative life events), but that the very same putatively “vulnerable” individuals are also those most likely to benefit from supportive experiences [20].
A recent review of GXE findings chronicling differential susceptibility [17] underscored the need for research that would make it easier to determine whether GXE findings are consistent with diathesis-stress or differential-susceptibility models of environmental action. Considered essential, among other things, was not treating the absence of contextual stress (e.g., not abused) as the positive pole of the environmental continuum being measured. Thus, rather than just determining, for example, whether a child is harshly treated or not, GXE studies should seek to measure indisputably supportive environmental conditions (e.g., positive parenting). In the present work, a composite measure of parenting quality in adolescence ranging from very positive and supportive to very negative/disengaged and unsupportive is used to predict a measure of parenting stress in adulthood, one importantly known to relate systematically to actual parenting behavior [31, 32, 37, 46]. Indeed, in studies of parents of children from toddlerhood to adolescence [2, 28, 47, 66], parental stress has been linked to more punitive and less emotionally supporting parenting and to children’s greater internalizing and externalizing problems. Unfortunately, parenting behavior itself was not assessed in the Add Health project from which this study obtained its data.
Virtually all GXE work to date has examined, for theoretically sensible reasons, the moderating effect of single genes [21]. This is typically due to the fact that investigators have a theory of gene action stipulating how particular genes influence particular neurotransmitters and thus particular phenotypes [24]. In this work we adopt a different strategy given evidence that multiple genes operate as “plasticity genes” in some GXE research, not just “vulnerability genes” [17], specifically the 10R allele of DAT1 [61], the A1 allele of DRD2 [36], the 7R allele of DRD4 [54] and the short allele of 5HTTLPR [63]. In at least some GXE studies, though certainly not all of them, individuals carrying these particular alleles seem to be affected by a variety of environmental factors in a “for-better-and-for-worse” manner [15], having their functioning both disproportionately undermined and enhanced by, respectively, unsupportive and supportive environmental conditions relative to those not carrying those alleles [12]. Indeed, the latter individuals appear much less and sometimes not at all affected by the very same environmental factors under investigation.
Rather than considering each gene one at a time and testing a series of single gene GXE interactions which might illuminate the genetic conditions under which parenting experienced in childhood proves related to parenting stress experienced in adulthood, we build on the recent work of several investigatory teams that have created composite measures of diverse alleles to predict phenotypic outcomes, based on the view that individual genes have very small effects [33, 41]. But rather than generating a summary index of genetic risk as Beaver and associates [10] did when predicting antisocial phenotypes, we create an index of cumulative-genetic plasticity which reflects the number of putative plasticity alleles in total that an adolescent carries of the set of four listed in the preceding paragraph. This affords testing the hypothesis that not only will cumulative-genetic plasticity moderate the effect of parenting in adolescence on parenting stress in adulthood, but that the more plasticity genes an individual carries, the stronger the parenting effect being evaluated will prove to be.
Methods
Data
The data analyzed in this study were drawn from the National Longitudinal Study of Adolescent Health (Add Health). Previously published reports provide detailed discussions of the data and the sampling design [42, 43, 57]. Briefly, Add Health involves a longitudinal and nationally representative sample of American youths who were enrolled in middle or high school during the 1994–1995 academic year. Four waves of data have been collected thus far; two in adolescence, one in early adulthood, and one when the respondents were in their late 20s or early 30s. Individuals were assessed on a variety of different phenotypes, including their behaviors, personalities, and family environments. Overall, more than 15,000 respondents were interviewed across these four waves [42].
Add Health also contains a subsample of respondents who were genotyped for genetic polymorphisms related to neurotransmission. During wave 3 interviews, respondents who had a sibling or a co-twin, who was also participating in the Add Health Study were asked to submit samples of their buccal cells. In total, 2,612 respondents were included in the DNA subsample of Add Health. Because more than one sibling per household was sampled, the DNA subsample lacked independence in observations, which can lead to downwardly biased standard errors. The lack of independence was corrected in two ways. First, one twin from each monozygotic twin pair was randomly selected and removed from the final analytical sample [38]. Second, all tests of statistical significance for the regression coefficients were estimated using Huber/White standard errors.
Measures
Predictor 1: Parenting Quality
The Add Health data contain a range of items designed to tap the quality of parenting that the adolescent received from their mother. Specifically, prior Add Health researchers have developed three indexes/scales that tap different dimensions of maternal parenting: one that taps maternal involvement, one that taps maternal disengagement, and one that taps maternal attachment [4]. The maternal involvement index measures the extent to which the mother is involved in her child’s life. During wave 1 interviews, youths were asked whether they and their mother had participated in ten different activities during the past month, including playing a sport, going shopping, or watching a movie. Items were coded dichotomously, where a value of “0” indicated that the adolescent and their mother did not engage in the activity and a value of “1” indicated that the adolescent and their mother did engage in the activity. Responses to these ten items were then added together to create the maternal involvement index (Cronbach’s α = .66).
Additionally, youths were also asked two questions that measured the child-mother relationship. In particular, during wave 1 interviews, youths reported on how close they felt to their mother and how much they thought their mother cared about them. Responses to these two questions were coded such that higher values indicated greater attachment. Responses to these questions were summed to create the maternal attachment scale (Cronbach’s α = .49). The third parenting scale available in Add Health measures maternal disengagement. During wave 1 interviews, five questions were asked to adolescents that tapped the extent to which their mothers lacked interest in and/or involvement with them. For instance, youths were asked to report how warm and loving their mother was, how often they talked with their mother, and the overall quality of their relationship with their mother. These questions were coded so that higher values represented more maternal disengagement. Responses to the items were summed together to create the maternal disengagement scale (Cronbach’s α = .83).
A principal components factor analysis with varimax rotation was then conducted on these three parenting composite measures. The results indicated that the variance–covariance matrix of these the three composites could be accounted for by a single-factor solution. The maternal disengagement scale was reverse-coded such that higher values reflected lower disengagement. Following prior research, [4], the three maternal parenting scales composites were transformed into a weighted factor score to create a measure of parenting quality. The parenting quality factor scale was then divided into quartiles to allow for more stable parameter estimates for the multiplicative interaction terms.
Predictor 2: Cumulative Genetic Plasticity
The genotyping of Add Health subjects was carried out at the Institute for Behavioral Genetics at the University of Colorado [43]. Prior research has identified four of the genetic polymorphisms available in the Add Health Footnote 1 as being related to plasticity: DAT1, DRD2, DRD4, and 5HTTLPR [16]. In particular, the plasticity alleles for each of the genes were as follows: the 10R allele of DAT1, the A1 allele of DRD2, the 7R allele of DRD4, and the short allele of 5HTTLPR. Each polymorphism was assigned a value of “1” if at least one putative plasticity allele was present. The values for each of the genetic polymorphisms were added to create an index of “cumulative-genetic plasticity.” The distribution of the cumulative-plasticity alleles was: 0 plasticity alleles = 0.2% (n = 2), 1 plasticity allele = 12.2% (n = 118), 2 plasticity alleles = 38.8% (n = 376), 3 plasticity alleles = 38.0% (n = 368), and 4 plasticity alleles = 10.8% (n = 105). Because only two cases had 0 plasticity alleles, all of the models were recalculated removing these two cases from the sample and also pooling them with the 1 plasticity allele group. The results were virtually identical and thus the two cases were included in the analyses with their original coding scheme.
Dependent Construct: Parental Stress
During wave 4 interviews, respondents were asked whether they had a biological child. If they responded affirmatively, they then responded to four questions drawn from the Parental Stress Scale [18] gauging, on a 5-point basis (1 = strongly disagree, 5 = strongly agree), the amount of stress that they experienced in being a parent. Specifically, they rated how (a) happy they were in the role of parent and (b) close they felt to their child(ren) (both reverse-coded), and the extent to which their children (c) were a major source of stress in their life and (d) they felt overwhelmed by the responsibility of being a parent. Responses to the four items were summed together to create the parental stress scale (Cronbach’s α = .54). Importantly, prior psychometric research of the Parental Stress Scale has revealed that it is both a reliable and valid way to assess parental stress [18].
Control Variables
Two control variables, gender (0 = female; 1 = male) and race, were included in the analyses. To avoid population stratification effects, race was coded by means of a series of dichotomous dummy variables. Caucasian was coded 0 = non-Caucasian and 1 = Caucasian; African-American was coded 0 = non-African-American and 1 = African-American; and Other was coded 0 = Caucasian or African-American and 1 = Other race. Other race was omitted from the equations and served as the comparison group for Caucasian and African-American.
Results
Statistical analysis involved a series of linked steps. To test for gene-environment correlation between the cumulative-genetic-plasticity index and parenting quality (measured in quartiles), bivariate correlations were estimated first (r = −.05, p > .05). The lack of association meant that any discerned GXE interaction did not simply reflect G:E correlation and thus a possible evocative effect of cumulative genetic plasticity on mothering.
The next set of analyses estimated ordinary least squares (OLS) regression models to examine the interrelationships among the cumulative-genetic-plasticity index, parenting quality, and parental stress. Inspection of the results of the additive model presented in Model 1 of Table 1 reveals no association between cumulative genetic plasticity and parental stress (β = .02, p > .05), but a statistically significant and positive association between parenting quality and parental stress (β = .11, p < .05). Model 2 displays the results of the OLS equation, where a two-way multiplicative interaction term between cumulative genetic plasticity and parenting quality proved to be statistically significant (β = .27, p < .05).
Supplementary analyses evaluated the two-way interaction between cumulative genetic plasticity and parenting quality in closer detail. First, simple slopes were calculated for each of the plasticity groups and difference-in-coefficients z-tests were estimated to determine which of the slopes differed significantly from each other [52]; see Table 2. Of particular importance, the simple slope for the 4-plasticity-allele group was statistically significant and differed significantly from the simple slopes for the 1-, the 2- and the 3-plasticity-allele groups (z = 3.17, 2.29, 2.73, respectively, all p < .05). (Because only two cases carried 0 plasticity alleles, they were excluded from these analyses.) The simple slopes among the 1-, 2-, and 3-plasticity-allele groups were not significantly different from each other.
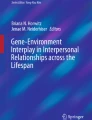
Last, the slopes for each of the plasticity allele subgroups were plotted across the four quartiles of the parenting quality scale. Figure 1 portrays these plots and shows a clear pattern of results consistent with the differential susceptibility hypothesis. In particular, individuals in the 4-plasticity-allele group scored lowest on parental stress when reared by the most supportive mothers and highest on the parental stress scale when reared by the most negative mothers. Inspection of the Figure and the estimates presented in Table 2 indicate that individuals with 2 and 3 plasticity alleles appeared to be more affected by their rearing history, also in a “for-better-and-for-worse” manner, depending on the quality of parenting experienced in adolescence, than those with only 1 plasticity allele.

The association between parenting quality and parental stress as a function of plasticity alleles
Discussion
The fact that parenting has been found to be transmitted across generations, but only to a modest extent, inspired the work presented here by raising the possibility that this could be due to the fact that individuals differ in their susceptibility to rearing [9, 10, 20]. After all, if individuals more and less susceptible are not distinguished, then average estimates of intergenerational transmission could both under- and over-estimate effects of parenting experienced on the experience of parenting. The current study investigated whether gene-environment interaction might contribute to understanding the intergenerational transmission of parenting.
To do so, the DNA subsample of Add Health was analyzed to examine the interrelationships among maternal parenting experienced by the respondent during adolescence, the respondent’s own experience of parental stress—obtained on average 14 years after the parenting-in-adolescence measurement–and a measure of the respondent’s cumulative genetic plasticity. Although it would have been preferable to have measurements of actual parenting rather than of parenting stress, no such data were available for analysis in Add Health. The fact that parental stress is a known predictor of parenting mitigates this study limitation somewhat [31, 32, 46]. Nevertheless, it will be important to determine whether the results reported here for what might be regarded as a proxy measure of parenting—parenting stress—extend to actual parenting.
Two broad findings emerged from this inquiry. First, there was a statistically significant interaction between parenting quality and cumulative genetic plasticity in the prediction of parental stress during adulthood. This finding suggests that parenting quality differentially affects future parental stress depending on genotype—and thus could at least partially explain why estimates of transmission across generations are not as strong as might perhaps be expected on the basis of theory. Second, and perhaps even more importantly, analyses conducted to examine whether the GXE interaction was consistent with the diathesis-stress or differential-susceptibility model of environmental action proved indisputably consistent with differential-susceptibility. Recall that respondents in the 4-plasticity-allele group who were exposed to the most positive maternal parenting as adolescents scored the lowest on parental stress during adulthood and, at the same time, respondents in the 4-plasticity-allele group who were exposed to the most negative maternal parenting as adolescents scored the highest on parental stress during adulthood (see Fig. 1). Although not nearly as pronounced, a similar pattern of findings surfaced for the 2- and 3- plasticity-allele groups. This “for-better-and-for-worse” finding is precisely what the differential-susceptibility hypothesis predicts [12, 15]; see also [20].
Even though the results reported extend the range of phenotypes that the differential-susceptibility hypothesis applies to, the findings need to be interpreted with caution for a number of reasons. To begin with, the cumulative genetic plasticity index employed in this study was created from only four genes. Belsky and associates [16, 12] have called attention to others, however, that appear to operate in a differential-susceptibility, not just diathesis-stress manner, including COMT and DRD3. Unfortunately, Add Health respondents were only genotyped for a handful of genes and this thus constrained the cumulative plasticity index that could be used in this inquiry. Given that single genes tend to have such small effects [58], one cannot but wonder, had additional putative plasticity genes been available for analysis, whether findings consistent with differential susceptibility would have been even more pronounced.
Limiting this study, too, was the fact that the outcome to be explained, parental stress (in the absence of a direct measure of parenting), was based on only four items and, as a result, had only moderate internal consistency. Such fallibility of measurement of the dependent variable could also have attenuated the discerned effects of the predictor variables used in this inquiry [39]. This seems quite conceivable because the power needed to detect statistical interactions is significantly greater than needed for evaluation of main effects [27].
An additional limitation of the measurement was that the dependent construct, parental stress, only assessed the negative side of the parenting experience. A more appropriate measurement strategy when testing for differential-susceptibility is to include measures that range from positive to negative [12]. In most GXE studies, especially those conducted in psychiatric genetics, however, the absence of a negative environment (e.g., not maltreated) or outcome (e.g., not depressed) is treated as positive. Central to the differential-susceptibility hypothesis is the proposition that plasticity alleles contribute to positive outcomes in the face of positive environments, not just negative outcomes in the face of adversity, as presumed by the diathesis-stress perspective. Thus, in the case of measurements like parental stress that do not capture the positive pole of the parenting experience (other than absence of stress), the ability to detect the “for better” part of the “for-better-and-for-worse” differential-susceptibility hypothesis becomes extremely difficult. That such a pattern of findings emerged in this inquiry despite this measurement handicap also provides a basis for wondering whether findings would have been stronger had the parenting-experience outcome been evaluated across the full negative-to-positive range, just as the parenting-in-adolescence predictor was.
Notes
The Add Health respondents were also genotyped for a polymorphism in the promoter region of the MAOA gene. However, since MAOA is X-linked, including this polymorphism in the plasticity index would necessitate separate models for males and females. Given that there is not a theoretical reason to believe that plasticity would differentially affect males and females in terms of parenting, we opted to exclude MAOA from the analyses and analyze males and females simultaneously.
References
Bailey JA, Hill KG, Oesterle S, Hawkins JD, The Social Development Research Group: Parenting practices and problem behavior across three generations. Developmental Psychology 45:1214–1226, 2009.
Baker BL, McIntyre LL, Blacher J, Crnic K, Edelbrock C, Low C: Preschool children with and without developmental delay: Behavior problems and parenting stress over time. Journal of Intellectual Disability Research 47:217–230, 2003.
Bandura A: Social Learning Theory. Englewood Cliffs, Prentice-Hall, 1977.
Beaver KM, Sak A, Vaske J, Nilsson J: Genetic risk, parent-child relations, and antisocial phenotypes in a sample of African-American males. Psychiatry Research 17:160–164, 2010.
Belsky J: Three theoretical models of child abuse: A critical review. International Journal of Child Abuse and Neglect 2:37–49, 1978.
Belsky J: Child maltreatment: An ecological integration. American Psychologist 35:320–335, 1980.
Belsky J: The determinants of parenting: A process model. Child Development 55:83–96, 1984.
Belsky J: Etiology of child maltreatment: A developmental-ecological analysis. Psychological Bulletin 114:413–434, 1993.
Belsky J: Variation in susceptibility to rearing influences: An evolutionary argument. Psychological Inquiry 8:182–186, 1997.
Belsky J: Differential Susceptibility to Rearing Influences: An Evolutionary Hypothesis and Some Evidence. In: Ellis B, Bjorklund D (Eds) Origins of the Social Mind: Evolutionary Psychology and Child Development. New York, Guildford, pp. 139–163, 2005.
Belsky J, Jaffee S: The Multiple Determinants of Parenting. In: Cicchetti D, Cohen D (Eds) Developmental Psychopathology, 2nd edn., Vol. 3: Risk, Disorder and Adaptation. New York, Wiley, pp. 38–85, 2006.
Belsky J, Pluess M: Beyond diathesis-stress: Differential susceptibility to environmental influence. Psychological Bulletin 135:885–908, 2009.
Belsky J, Youngblade L, Pensky E: Childrearing history, marital quality and maternal affect: Intergenerational transmission in a low-risk sample. Development and Psychopathology 1:291–304, 1990.
Belsky J, Jaffee SR, Sligo J, Woodward L, Silva PA: Intergenerational transmission of warm-sensitive-stimulating parenting: A prospective study of mothers and fathers of 3-year-olds. Child Development 76:384–396, 2005.
Belsky J, Bakermans-Kranenburg MJ, van Ijzendoorn MH: For better and for worse: Differential Susceptibility to environmental influences. Current Directions in Psychological Science 16(6):300–304, 2007.
Belsky J, Conger R, Capaldi DM: The intergenerational transmission of parenting: Introduction to the special section. Developmental Psychology 45:1201–1204, 2009.
Belsky J, Jonassaint C, Pluess M, Stanton M, Brummett B, Williams R: Vulnerability genes or plasticity genes? Molecular Psychiatry 14:746–754, 2009.
Berry JO, Jones WH: The parental stress scale: Initial psychometric evidence. Journal of Social and Personal Relationships 12:463–472.
Bowlby J: Attachment and Loss. Attachment, Vol. 1. New York, Basic Books, 1969.
Boyce WT. Ellis BJ: Biological sensitivity to context: I. An evolutionary-developmental theory of the origins and functions of stress reactivity. Development and Psychopathology 17(2):271–301, 2005.
Burmeister M, McInnis MG, Zollner S: Psychiatric genetics: Progress amid controversy. Nature Reviews Genetics 9(7):527–540, 2008.
Capaldi D, Pears K, Patterson G, Owen L: Continuity of parenting practices across generations in an at-risk sample: A prospective comparison of direct and mediated associations. Journal of Abnormal Child Psychology 31:127–142, 2003.
Caspi A, Elder GH: Emergent Family Patterns: The Intergenerational Construction of Problem Behavior and Relationships. In: Hinde R, Stevenson-Hinde J (Eds) Relationships Within Families. Oxford, Oxford University Press, pp. 218–240, 1988.
Caspi A, Moffitt TE: Gene-environment interactions in psychiatry: Joining forces with neuroscience. Nature Reviews Neuroscience 7(7):583–590, 2006.
Chen Z, Kaplan H: The intergenerational transmission of constructive parenting. Journal of Marriage and the Family 63:17–31, 2001.
Cicchetti D, Rizley R: Developmental perspectives on the etiology, intergenerational transmission and sequelae of child maltreatment. New Directions for Child Development 11:31–56, 1981.
Cohen J, Cohen P, West SG, Aiken LS: Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, 3rd edn. Mahwah, Lawrence Erlbaum, 2003.
Conger RD, Patterson GR, Ge X: It takes two to replicate: A mediational model for the impact of parents’ stress on adolescent adjustment. Child Development 66:80–97, 1995.
Conger R, Nellpl T, Kim K, Scaramella L: Angry and aggressive behaviour across three generations: A prospective, longitudinal study of parents and children. Journal of Abnormal Child Psychology 31:143–160, 2003.
Conger R, Capaldi D, Belsky J: The intergenerational transmission of parenting: Closing comments for the special section. Developmental Psychology 45:1276–1283, 2009.
Crnic KA, Greenberg MT: Minor parenting stresses with young children. Child Development 61:1628–1637, 1990.
Crnic KA, Gaze C, Hoffman C: Cumulative parenting stress across the preschool period: Relations to maternal parenting and child behaviour at age 5. Infant and Child Development 14:117–132, 2005.
De Quervain DJF, Papassotiropoulos A: Identification of a genetic cluster influencing memory performance and hippocampal activity in humans. Proceedings of the National Academy of Sciences of the United States of America 103:4270–4274, 2006.
Egeland B, Jacobvitz D, Papatola K: Intergenerational Continuity of Abuse. In: Gelles R, Lancaster J (Eds) Child Abuse and Neglect: Biosocial Dimensions. New York, Aldine, pp. 255–276, 1987.
Elder G: History and the Life Course. In Bertaux D (Ed) Biography and Society: The Life History Approach in the Social Sciences. Beverly Hills, Sage, pp. 77–115, 1981.
Elovainio M, Jokela M, Kivimaki M, Pulkki-Raback L, Lehtimaki T, Airla N, et al.: Genetic variants in the DRD2 gene moderate the relationship between stressful life events and depressive symptoms in adults: Cardiovascular risk in young Finns study. Psychosomatic Medicine 69(5):391-395, 2007.
Feldman R, Eidelman AI, Rotenberg N: Parenting stress, infant emotion regulation, maternal sensitivity, and the cognitive development of triplets. Child Development 75:1774–1791, 2004.
Haberstick BC, Lessem JM, Hopfer CJ, Smolen A, Ehringer MA, Timberlake D, Hewitt JK: Monoamine oxidase A and antisocial behaviors in the presence of childhood and adolescent maltreatment. American Journal of Medical Genetics 135B:59–64, 2005.
Hanushek EA, Jackson JE: Statistical Methods for Social Scientists. San Diego, Academic Press, 1977.
Hardt J, Rutter, M: Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry 45:260–273, 2004.
Harlaar N, Butcher LM, Meaburn E, Sham P, Craig IW, Plomin R: A behavioural genomic analysis of DNA markers associated with general cognitive ability in 7-year-olds. Journal of Child Psychology and Psychiatry 46:1097–1107, 2005.
Harris KM, Florey F, Tabor J, Bearman PS, Jones J, Udry JR: The National Longitudinal Study of Adolescent Health: Research Design, 2003. http://www.cpc.unc.edu/projects/addhealth/design. Accessed 29 June 2009.
Harris KM, Halpern CT, Smolen A, Haberstick BC: The National Longitudinal Study of Adolescent Health (Add Health) twin data. Twin Research and Human Genetics 9:988–997, 2006.
Huesmann L, Eron L, Lefkowitz M, Walder L: The stability of aggression over time and generations. Developmental Psychology 20:1120–1134, 1984.
Hunter R, Kilstrom N: Breaking the cycle in abusive families. American Journal of Psychiatry 136:1320–1322, 1979.
Jackson AP, Huang CC: Parenting stress and behavior among single mothers of preschoolers. Journal of Social Service Research 26:29–42, 2000.
Jackson AP, Brooks-Gunn J, Huang CC, Glassman M: Single mothers in low-income jobs: Financial strain, parenting, and preschoolers’ outcomes. Child Development 71:1409–1423, 2000.
Kaufman J, Zigler E: Do abused children become abusive parents? American Journal of Orthopsychiatry 57:186–192, 1987.
Kerr DCR, Capaldi DM, Pears KC, Owen LD: A prospective three generational study of fathers’ constructive parenting: Influences from family of origin, adolescent adjustment, and offspring temperament. Developmental Psychology 45:1257–1275, 2009.
Kovan NM, Chung AL, Sroufe LA: The intergenerational continuity of observed early parenting. Developmental Psychology 45:1205–1213, 2009.
Neppl TK, Conger RD, Scaramella LV, Ontai LL: Intergenerational continuity in parenting behavior. Developmental Psychology 45:1241–1256, 2009.
Paternoster R, Brame R, Mazerolle P, Piquero A: Using the correct statistical test for the equality of regression coefficients. Criminology 36:859–866, 1998.
Patterson G: Continuities—A search for causal mechanisms. Developmental Psychology 34:1263–1268, 1998.
Pluess M, Belsky J, Neuman RJ: Prenatal smoking and ADHD: DRD4-7R as a plasticity gene. Biological Psychiatry 66:e5–e6, 2009.
Quinton D, Rutter M: Parents with children in care: II. Intergenerational continuities. Journal of Child Psychology and Psychiatry 25:231–250, 1984.
Quinton D, Rutter M, Liddle C: Institutional rearing, parenting difficulties, and marital support. Psychological Medicine 14:107–124, 1984.
Resnick MD, Bearman PS, Blum RW, Bauman KE, Harris KM, Jones J, Tabor J, Beuhring T, Sieving RE, Shew M, Ireland M, Bearinger LH, Udry JR: Protecting adolescents from harm: Findings from the National Longitudinal Study of Adolescent Health. Journal of the American Medical Association 278:823–832, 1997.
Rutter M: Genes and Behavior: Nature-Nurture Inteprlay Explained. Malden, Blackwell, 2006.
Schaffer A, Burt K, Obradovic J, Herbers JE, Masten AS: Intergenerational continuity in parenting quality. Developmental Psychology 45:1227–1240, 2009.
Serbin L, Karp J: Intergenerational studies of parenting and the transfer of risk from parent to child. Current Directions in Psychological Science 12:138–142, 2003.
Sonuga-Barke EJ, Oades RD, Psychogiou L, Chen W, Franke B, Buitelaar J, et al.: Dopamine and serotonin transporter genotypes moderate sensitivity to maternal expressed emotion: The case of conduct and emotional problems in attention deficit/hyperactivity disorder. Journal of Child Psychology and Psychiatry and Allied Disciplines 50:1052–1063, 2009.
Spinetta J. Rigler D: The child abusing parent: A psychological review. Psychological Bulletin 77:296–304, 1972.
Taylor SE, Way BM, Welch WT, Hilmert CJ, Lehman BJ, Eisenberger NI: Early family environment, current adversity, the serotonin transporter promoter polymorphism, and depressive symptomatology. Biological Psychiatry 60(7):671–676, 2006.
Thornberry T, Feeeman-Gallant A, Lizotte A, Krohn M, Smith C: Linked lives: The intergenerational transmission of antisocial behaviour. Journal of Abnormal Child Psychology 31:171–184, 2003.
Van Ijzendoorn MH: Intergenerational transmission of parenting: A review of studies in nonclinical populations. Developmental Review 12:76–99, 1992.
Whiteside-Mansell L, Pope SK, Bradley RH: Patterns of parenting behavior in young mothers. Family Relations 45:273–281, 1996.
Zuckerman M: Vulnerability to Psychopathology: A Biosocial Model. Washington, American Psychological Association, 1999.
Acknowledgments
This research uses data from Add Health, a program project designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris and funded by Grant PO1-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 17 other agencies. Special acknowledgement is due to Ronald R. Rindfuss and Barbara Entwisle for assistance in original design. Persons interested in obtain data files from Add Health should contact Add Health, Carolina Population Center, 123 W. Franklin Street, Chapel Hill, NC 27516-2524 (addhealth@unc.edu). No direct support was received from Grant PO1-HD31921 for this analysis.
Conflict of interest
The authors have no competing financial interests in relation to the work described.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Beaver, K.M., Belsky, J. Gene-Environment Interaction and the Intergenerational Transmission of Parenting: Testing the Differential-Susceptibility Hypothesis. Psychiatr Q 83, 29–40 (2012). https://doi.org/10.1007/s11126-011-9180-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11126-011-9180-4