
Abstract
The objectives of this study were to examine (1) whether the onset of sexually transmitted infections (STI) through age 30 differed for youths who received a social developmental intervention during elementary grades compared to those in the control condition; (2) potential social-developmental mediators of this intervention; and (3) the extent to which these results differed by ethnicity. A nonrandomized controlled trial followed participants to age 30, 18 years after the intervention ended. Three intervention conditions were compared: a full-intervention group, assigned to intervention in grades 1 through 6; a late intervention group, assigned to intervention in grades 5 and 6 only; and a no-treatment control group. Eighteen public elementary schools serving diverse neighborhoods including high-crime neighborhoods of Seattle are the setting of the study. Six hundred eight participants in three intervention conditions were interviewed from age 10 through 30. Interventions include teacher training in classroom instruction and management, child social and emotional skill development, and parent workshops. Outcome is the cumulative onset of participant report of STI diagnosis. Adolescent family environment, bonding to school, antisocial peer affiliation, early sex initiation, alcohol use, cigarette use, and marijuana use were tested as potential intervention mechanisms. Complementary log–log survival analysis found significantly lower odds of STI onset for the full-intervention compared to the control condition. The lowering of STI onset risk was significantly greater for African Americans and Asian Americans compared to European Americans. Family environment, school bonding, and delayed initiation of sexual behavior mediated the relationship between treatment and STI hazard. A universal intervention for urban elementary school children, focused on classroom management and instruction, children’s social competence, and parenting practices may reduce the onset of STI through age 30, especially for African Americans.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the USA, most sexually transmitted infection (STI) and pregnancy prevention efforts have focused on immediate sexual antecedents of risky sex, seeking to provide youth with the knowledge, attitudes, and skills to avoid sexual intercourse or to use protection properly (Kirby 2007). Although influences on young people’s sexual behavior are not limited to explicit messages about sex (Grunseit et al. 1997; Kirby 2007), Kirby has noted that many non-sexual antecedents of youth risky sexual behavior have been generally ignored in STI/HIV and pregnancy prevention programs until recently (Kirby 2007).
Rotheram-Borus (2000) has argued to expand the range of interventions to reduce risky sexual behavior among adolescents by including interventions aimed at improving general social competency and promoting prosocial behaviors. Reviews of interventions targeting risky sexual behavior (Kirby 2007; Nitz 1999) indicate that the most effective prevention programs may include a component to improve adolescent opportunities for prosocial involvement, beliefs, and life skills. Some youth development interventions, even though they did not focus on sexuality, have effectively reduced adolescent pregnancy and birth rates (see Gavin et al. 2010 for a review). In addition, these programs also have had other positive effects on increasing education, improving employment, reducing substance use, and reducing incarceration, which make them more broadly cost-effective in the long run (Aos et al. 2004).
The Seattle Social Development Project Intervention
The Seattle Social Development Project (SSDP) intervention implemented in the present study sought to improve opportunities, involvement, rewards, and life skills for children in elementary school. Guided theoretically by the social development model (Catalano and Hawkins 1996; Hawkins and Weis 1985), we identified and developed methods of management and instruction that could be used by public school teachers and adult caretakers to set children on a positive developmental course by promoting opportunities for children’s active involvement in classroom and family, developing children’s skills for participation, and encouraging reinforcement from parents and teachers for children’s effort and accomplishment. Two intervention conditions were examined, both compared to a no-treatment control group: a “full” intervention condition implemented throughout grades 1 through 6 and a “late” intervention condition implemented only when children were in grades 5 and 6 (Hawkins et al. 2005, 2008).
Studies of the SSDP intervention have found significantly better outcomes in childhood and adolescence in the full-intervention group compared to the control group on family and school factors as well as on child and adolescent outcomes in a developmentally consistent manner. For example, prior work has demonstrated significant intervention differences between full-intervention and control youths, including better family functioning in childhood (Hawkins et al. 1992); less early-onset problem behavior (Hawkins et al. 1992, 1991), better school bonding, higher academic achievement, and improved school conduct (less truancy, cheating, sent from class for misbehavior) in adolescence (Hawkins et al. 1999); less adolescent risk behavior (Hawkins et al. 1999); and better educational, occupational, and mental health outcomes at ages 21, 24, and 27 (Hawkins et al. 2005, 2008).
In addition, although the SSDP intervention included no sex education or any discussion of sex, at age 18, the full-intervention group had significantly lower lifetime prevalences of sexual intercourse, early pregnancy (or causing pregnancy), and multiple sex partners than controls (Hawkins et al. 1999). Lonczak et al. (2002) replicated these findings at age 21 and also found a significantly increased probability of condom use during last intercourse (among single individuals) and decreased incidence of lifetime STI diagnosis in the full-intervention group compared with controls. These latter findings were especially strong among African Americans. The first goal of the present study was to examine an association between intervention condition and cumulative onset of STI diagnosis through age 30.
Mechanisms of Intervention Effects on Risky Sexual Behavior
Since many preventive interventions are guided by theory or by etiological research on risk and protective factors for the intervention outcomes, researchers have encouraged mediational analyses to examine whether observed intervention effects operated through the theoretically specified mechanisms (Kellam and Rebok 1992). Mediation analysis provides information on how the prevention program achieved its effects, which in turn increases understanding of the mechanisms underlying changes in the behavioral outcome. Thus, the second goal of this study was to examine factors that may have mediated the effects of the SSDP intervention on STI onset. Because they were specified as intervention targets by theory and by intervention design, because prior work has shown intervention effects on these factors, and because they have been implicated in the etiology of STIs, we expect that the SSDP intervention may have affected the onset of STIs by improving adolescent family environments and bonding to school and by reducing antisocial peer affiliation.
Evidence also suggests that HIV sexual risk behavior co-occurs with other risk behaviors including alcohol, cigarette, and marijuana use, especially during adolescence (Guo et al. 2002; Lowry 1994; Valois et al. 1999; Cook et al. 2002; Woods et al. 2000; Keyes et al. 2007). Although the SSDP intervention has shown modest results with respect to substance use overall (less alcohol initiation by age 10, less heavy alcohol use at age 18; Hawkins et al. 1999, 1992), it is possible that intervention outcomes may be moderated by ethnicity, as described below. Thus, in addition to the family, peer, and school factors discussed above, we examine whether the SSDP intervention affected the onset of STIs by delaying initiation of sexual behavior and engagement in other health-risking behaviors, including adolescent alcohol, tobacco, and marijuana use.
Intervention by Ethnicity Interactions
National data indicate that there are large ethnic differences in the rates of STI/HIV infection and early pregnancy. For example, in 2006, African Americans experienced the highest rates of AIDS and HIV/AIDS diagnoses and the highest rate for living with AIDS and HIV/AIDS across all age groups (Gavin et al. 2009). In addition, rates of chlamydia, gonorrhea, and syphilis are elevated among minority ethnic groups, especially African Americans (Gavin et al. 2009).
Previous analyses have found that some differences between SSDP intervention groups were moderated by ethnicity. For example, at age 21, the full SSDP intervention was especially effective at increasing condom use at last intercourse and decreasing the likelihood of STI among African Americans. Seventy-nine percent of African Americans in the full-treatment group reported using a condom during last intercourse compared with 36 % in the control group (Lonczak et al. 2002). Among non-African Americans, the prevalence rates were 56 and 47 %, respectively. Similarly, only 7 % of the African Americans in the full-intervention group, compared with 34 % of those in the control group, reported being diagnosed with an STI over their lifetime by age 21. Among non-African Americans, 14 % of those in the full-intervention group reported a STI diagnosis compared with 11 % of those in the control group. These ethnicity × treatment group differences remained after controlling for socioeconomic status (Lonczak et al. 2002).
The third goal of the present paper was to examine whether intervention group differences in STI onset through age 30 were moderated by ethnicity. In particular, we hypothesize that intervention/control group differences will be stronger among African Americans compared with those from other ethnic groups. Finally, this paper investigates whether the family, school, peer, and risk behaviors discussed above mediate links between the intervention and STI onset among African Americans in the sample.
Methods
Sample and Intervention Assignment
Data were drawn from the Seattle Social Development Project (SSDP), a longitudinal study of prosocial and antisocial behavior. The SSDP sample includes about equal numbers of males (n = 412) and females (n = 396) and is ethnically diverse. About 47 % are Caucasian, 26 % are African American, 22 % are Asian American, and 5 % are Native American. Of these groups, 5 % are Hispanic. About 52 % of the panel members are from low-income families as evidenced by participation in the National School Lunch/School Breakfast Program between the ages of 10 and 12. Participants have been surveyed 12 times: assessments were conducted in both the spring and fall of fifth grade (ages 10 and 11), yearly from ages 12 to 16, at age 18, and at ages 21, 24, 27, and 30. Given that the assessments were so closely spaced and that the likelihood of STI infection was extremely low in elementary school, for the present analyses, data from ages 10 and 11 were combined, yielding 11 waves for analysis. Assessments were conducted in person and were administered by trained interviewers. Until age 12, surveys were group-administered in classrooms. Thereafter, face-to-face interviews were conducted in the participant’s home or in another private location. A small number of assessments at each wave (∼5 %) were completed by mail or over the telephone. All phases of the study were approved by the Human Subjects Review Committee at the University of Washington, Seattle. Participants were informed about the nature of the interviews, and parents provided consent; students provided assent prior to age 18. Participants provided consent from age 18 onwards at every wave of data collection.
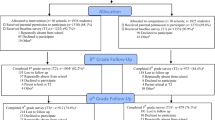
In elementary school, SSDP panel members participated in a test of a social developmental intervention described below. A CONSORT diagram describing the flow of participants through the study is provided in Fig. 1. The quasi-experimental study tested in the present paper examined three conditions (full intervention, late intervention, and control) and was established at grade 5 in the fall of 1985. All fifth grade students in ten intervention elementary schools and all fifth grade students in five control schools were selected to participate. Control schools were selected and matched to the intervention schools based on socioeconomic and ethnic characteristics of students. Initially, a fourth (Parent-Training Only) intervention group administered through three additional schools was created, but it was found not to be comparable at baseline [more European Americans and fewer African Americans (χ 2 = 26.34, p < 0.01) and considerably fewer eligible for free or reduced lunch (χ 2 = 35.77, p = 0.001) compared with the other three conditions] and thus was not included in the current quasi-experimental comparison.

CONSORT flowchart of study. The quasi-experimental study (shaded above) tested in the present paper was established in the fifth grade and examines three conditions: full treatment, late treatment, and control. At the fifth grade baseline, the study recruited participants from an earlier trial of eight schools in addition to new participants from 13 new schools. Due to school closures, two early intervention and one early control school were merged into new intervention and control schools, respectively, resulting in 18 schools at baseline (8 + 13 − 3 = 18 schools). This panel was then followed through age 30. *Note that although this diagram presents those lost to follow-up in adulthood, survival analyses employed multiple imputation on the full sample starting at age 10, with 6 % missingness across study variables and effective sample sizes of 137, 235, and 199 for full, late, and control conditions, respectively (approximately 94 % of the samples in allocated conditions). Twenty-five participants were missing data at all three time periods in adulthood
Some of the grade 5 intervention schools included students who had participated in an earlier controlled trial of the SSDP intervention. The earlier randomized controlled trial began with first graders in eight elementary schools. In six of these schools, intervention and control cohorts had been randomized in first grade at the classroom level, consisting of one intervention and one control classroom in each school. In a seventh school, all three first grade classrooms were in the intervention condition. The eighth school was a control school. In the fifth grade, students from the six mixed schools and the intervention school became part of a full-school implementation of the intervention. The prior intervention students thus constituted the full-intervention condition (intervention over grades 1–6) and the prior control students from the mixed schools constituted the late intervention students (grades 5 and 6 only). Children from the control school remained in a control school at fifth grade. Due to school closures, two early intervention and one early control school were merged into new intervention and control schools, respectively, resulting in 18 schools at the fifth grade baseline (8 + 13 − 3 = 18 schools). Twenty students received early treatment only and moved out of project schools before receiving the grades 5–6 intervention, and four students moved between intervention and control schools more than once. These 24 students could not be classified as either full or late intervention. Thus, the present quasi-experimental study examined three groups: full intervention (grades 1–6), late intervention (grades 5 and 6 only), and control (no intervention).
Potential Clustering
It is important to attend to potential clustering concomitant with intervention experience (Dielman 1994; Murray et al. 1994) to minimize type 1 error due to underestimates of parameter standard errors. In consideration of the design of the study, the appropriate cluster is not the initial clustered status (first grade classrooms and schools), nor the final clustered status (5th–6th grade schools), since prior intervention and control students came to these schools with different shared experiences. Rather, the clusters are most accurately represented by the sets of individuals who share the same environmental experience of classrooms and schools through the period of the intervention. As students moved from grade to grade, they sometimes moved to different teachers, but they remained in their respective treatment condition. For example, two students having the same intervention teacher in grade 1 may have had different intervention teachers in grade 2 and still different intervention teachers in grade 3, all while remaining in the intervention condition. Thus, we examined which sets of children shared the same classroom/school (grades 1–4) and school (grades 5 and 6) environments over the course of the intervention and identified 169 different patterns of shared environmental experiences. We then calculated the intraclass correlations (ICC) and design effect for the outcome (lifetime STD) and mediators (family environment, school bonding, early sexual initiation, binge drinking, marijuana use, cigarette use, antisocial peers) examined in this study. The average cluster size was 3.71, with an average ICC of 0.038, resulting in an average design effect of 1.10 (null = 1.00; Hedges and Rhoads 2009; Kish 1965). Since the follow-up analyses described below were also conducted on the African American participants in the study, these analyses were repeated within this group. Within the African American participants, the average cluster size was 2.18, with an average ICC of 0.028, resulting in an average design effect of 1.03. Although these small ICC and cluster size combinations likely introduce only negligible bias (Muthén and Satorra 1995), to be conservative, all standard errors in this study were adjusted (inflated) by the average design effect (Dielman 1994) to account for potential classroom/school clustering effects.
Attrition and Internal Validity
Because the analyses reported below revealed significant differences between the full-intervention and control groups in STI onset and mediators, analyses were conducted to ascertain the initial comparability of intervention groups on factors that might influence outcomes as well as whether the intervention groups remained comparable on these factors by the age 30 follow-up. Since the follow-up analyses described below were also conducted on the African American participants in the study, these baseline and follow-up validity analyses were repeated within this group. At age 30, 91 % of the sample was interviewed (N = 719 of 790 still living); there was no differential attrition across intervention groups (χ 2 = 0.04, p = 0.83). Table 1 presents the results of baseline and age 30 follow-up validity analyses. At baseline and at age 30, the distribution of participants in the full-intervention vs. control conditions did not differ with respect to gender, ethnicity, or childhood low-income status. Given that control students were added to the study at grade 5 and the requirement that full-intervention students attended project schools for more than one semester in grades 1 through 4 and in grades 5 and 6, it is important to rule out differences in residential stability, a potential threat to internal validity. Analyses comparing the full-intervention and control groups found no significant differences in mean number of years living in Seattle by grade 6, proportion of single-parent homes during grade 5, family size, or living in a disorganized neighborhood at age 16 years. The mothers of control group participants were slightly younger (49 years) than full-treatment mothers (50 years) and were more likely to have been teen mothers to the participants. Therefore, all analyses of treatment associations control for child of teen mother status. Each of these analyses was replicated in the African American-only subsample with similar findings. Overall, these validity analyses suggest that a number of factors that might have affected outcomes were comparable across intervention conditions both at baseline and at the age 30 follow-up, for the full sample and for African Americans only, and do not pose major threats to the internal validity of the present study.
The final sample consisted of African, Asian, and European Americans who were in the control, late-treatment, or full-treatment groups. Although the CONSORT diagram presents those not interviewed at ages 24, 27, and 30, survival analyses employed multiple imputation using data from ages 10 through 30. Thus, all participants who had data for at least one time point were retained in the analysis. Across study variables, 6 % of data points were missing. Twenty-five participants were missing data at all three ages: 24, 27, and 30 years. Effective sample sizes (Graham and Hofer 2000) were calculated at 137, 235, and 199 for full, late, and control conditions, respectively (approximately 94 % of the samples in allocated conditions).
Intervention Components
The intervention is more fully described elsewhere (Hawkins et al. 1999, 2005; Lonczak et al. 2002). Each year during grades 1 through 6, teachers in the intervention conditions received 5 days of in-service training in proactive classroom management and interactive instructional methods. Additionally, first grade teachers received instruction in the use of a cognitive and social skills training curriculum. During grade 6, a study consultant provided students with training in refusal skills. When children were in grades 1 through 3, parents were offered a seven-session curriculum in child behavior management skills and a four-session curriculum in skills for supporting their children’s academic development. During grades 5 and 6, intervention parents were also offered a five-session curriculum designed to strengthen skills to reduce their children’s risks for problem behaviors. Forty-three percent of eligible full-intervention parents attended at least one parenting class during grades 1 through 3. During grades 5 or 6, 29 % of parents in intervention conditions attended at least one class, indicating that the parent training component had less reach than the teacher training and child social skills training components. The present study compares the full- and late-intervention groups to the control group.
Measures
STI Diagnosis
At ages 21 and 24, participants were asked whether they “had ever been told by a nurse or doctor that they had HIV/AIDS” or “a sexually transmitted disease other than HIV/AIDS, such as gonorrhea, genital warts, chlamydia, herpes, or syphilis.” Positive responses were probed to determine the age at first diagnosis. At ages 27 and 30, participants were asked whether they had received an STI diagnosis in the 3 years prior to the interview. Thus, available data on STI diagnosis span the life course up to age 30. Based on responses to these questions, a dichotomous (yes/no) STI diagnosis variable was created for each interview wave. These wave-based variables were used in the construction of a lifetime diagnosis variable, which denoted whether a respondent experienced an STI diagnosis and a duration to first diagnosis variable, which indexed the number of waves until each participant first reported an STI diagnosis and was used as the dependent variable in survival analyses.
Prosocial Family Environment in Adolescence
At ages 10 through 16 and at age 18, measures of positive family environment tapped child involvement in family activities, family conflict (reversed), clear rules and monitoring, and bonding. Items included: “Rules in my family are clear,” “How often do your parents know where you are and who you are with when you’re not at home?,” “How often do you share your thoughts and feelings with your mother?,” “How often do you share your thoughts and feelings with your father?,” “How often do you share your thoughts and feelings with [your siblings]?,” and “People in my family get along well.” Family environment variables were averaged at each age to create age-specific prosocial family environment measures (Cronbach’s α ranged 0.67–0.75 within ages), and then these measures were standardized and averaged across ages 10–18 to produce an average adolescent prosocial family environment measure (α = 0.85).
Bonding to School in Adolescence
Participants reported on their bonding to school at ages 10 through 16 and at age 18. Items tapped attachment and commitment to school and included items such as: “Most mornings, I look forward to going to school,” “I like school,” “I do extra work on my own in class,” “I like my teacher,” and “When I have an assignment to do, I keep working on it until it is finished.” School bonding variables were averaged at each age to create age-specific school bonding measures (Cronbach’s α ranged 0.68–0.80 within ages), and then these measures were standardized and averaged across ages 10–18 to produce an average adolescent school bonding measure (α = 0.80).
Antisocial Peers in Adolescence
At ages 10 through 16, participants were asked a series of questions about the antisocial behavior of their first, second, and third best friends: whether these friends did things that got them in trouble with teachers, used alcohol without parental permission, and tried to do well in school (reversed). Variables were averaged at each age to create age-specific antisocial peer measures (Cronbach’s α ranged 0.63–0.82 across ages), and then these measures were standardized and averaged across ages 10–16 to produce an average adolescent antisocial peers measure (α = 0.78).
Early Sexual Initiation
Participants were asked how old they were the first time they “had sex with another person” at the age 14, 15, 16, 18, 21, and 24 interviews. Available reports were averaged. Some participants did not report having sex by age 24. At ages 27 and 30, we asked participants how many people they had had sex with in the 3 years prior to the interview and were, thus, able to code sexual debut for those people who had not reported having sex at the prior interviews. If a respondent first reported being sexually active at the age 27 interview, their age at that interview was coded as their age at first sex. The same procedure was followed for those who first reported sexual activity at the age 30 interview. A dichotomous “early initiation” variable was created using age 14 as a cutoff. Seventeen people reported that they had not yet been sexually active by age 30. Although their age at sexual debut was, therefore, unknown, we were able to classify them as non-early initiators.
Substance Use
At each wave from age 10 to age 30, participants were asked how often they did each of the following in the month prior to the interview: consumed alcohol, smoked cigarettes, and used marijuana. From ages 10 to 12, response options for each substance ranged from (1) never to (4) more than four times. Beginning at age 13, participants reported the number of days using each substance in the past month. Substance use variables were standardized in order to put them on the same metric at each time point and included in the analysis as time-varying predictors of onset. In addition alcohol, cigarette, and marijuana use measures were standardized and averaged across adolescence for use in the path analyses.
Control Variables
Self-reported gender was included in analyses because it is related to STI prevalence (Gavin et al. 2009). Low-income status (eligibility for the National School Lunch/School breakfast program at age 11, 12, or 13) was included as a control variable because it often is confounded with ethnicity. As discussed above, all analyses of treatment effects controlled for child of teen mother status.
Analysis and Results
Overview
Preliminary analyses examined zero-order relationships between intervention condition and outcomes, intervention condition and potential mediators, and potential mediators and outcomes (A–C, A–B, and B–C relationships in the Baron and Kenny 1986 framework). Complementary log–log survival analyses tested the relationships among intervention condition, mediators, and STI onset (Willett et al. 1998). Significant mediators identified in survival analyses were then included in a path model to examine intervention, mediator, and STI diagnosis simultaneously in a single model.
Section 1: Zero-Order Relationships
Treatment Group and STI Prevalence
About 38 % of participants had been diagnosed with an STI by age 30. Table 2 presents lifetime STI prevalence among all participants and by intervention group. Chi-square tests showed that lifetime STI prevalence by age 30 was significantly lower in the full-treatment group (27 %) compared to the late-treatment and control groups (each 41 %).
Treatment Group and Mediators
Table 2 also displays descriptive information on hypothesized mediators averaged across adolescence for the full sample and by treatment group. Participants in the full-treatment group reported significantly higher levels of adolescent positive family environment and adolescent school bonding compared to participants in the control group. Full-treatment group members also were less likely to report early sexual initiation than those in the control group. Differences between participants in the three intervention conditions did not reach statistical significance for adolescent antisocial peers, alcohol use, cigarette use, or marijuana use.
Since we hypothesized that intervention/control group differences would be stronger among African Americans compared to those from other ethnic groups, and subsequent mediational analyses were performed within African Americans only, we also examined intervention differences in mediators among African Americans. Results (not tabled) among African Americans largely reflected the full sample analysis: no statistically significant intervention differences for adolescent antisocial peers, alcohol use, cigarette use or marijuana use; however, African American participants in the full-treatment group did report significantly higher levels of adolescent positive family environment (p < 0.006) and adolescent school bonding (p < 0.019) compared to participants in the control group.
Mediators and STI Prevalence
Table 2 also shows Pearson’s correlations between hypothesized mediators, averaged across adolescence, as well as their point biserial correlations with lifetime STI diagnosis. These correlation analyses show all potential mediators to be significantly correlated with one another and with lifetime STI diagnosis.
Section 2: Discrete-Time Survival Analyses
Analysis
Survival analysis was performed using the logistic procedure with a c-log–log link in SAS, version 9.1 (Allison 1995). We selected survival analysis to examine intervention and mediation effects to maximize power since stacking the interview data for survival analysis results in multiple observations (up to 11) for many participants, resulting in over 5,800 STI observations in total through age 30. The lifetime STI measure served as the “event occurrence” marker, and the number of waves to first diagnosis (range, 1–11) was used as the “duration to event” marker. Right censored individuals—those who did not report an STI diagnosis—were assigned an event status of 0 and a “duration” of 11 (maximum number of observations; Allison 1995). A sequence of models was run to examine the research goals of the study: (a) a baseline model including treatment group membership and demographic controls (childhood low-income status, gender, being the child of a teen mother) examined overall intervention group differences; (b) a treatment-by-ethnicity interaction model examined whether the intervention group differences were the same for Caucasians, African Americans and Asians in the sample; (c) meditational models testing each potential mediator separately; and (d) a model including all of the mediators that were significant in the prior models. Positive family environment, antisocial peers, and school bonding were entered as their average value across adolescence. Alcohol, cigarette, and marijuana use were entered as time-varying predictors at time T-1. Early onset of sexual behavior was entered as a dichotomous (less than age 14 or not) variable. Because the intervals between interview waves were not equivalent at all points (1-year intervals early in the study, 3-year intervals later in the study), intra-wave duration was also controlled in all survival models.
In order to minimize false negatives, lifetime STI diagnosis was coded as missing if an individual did not participate at either age 24, 27, or 30 (n = 110). Because STI questions at ages 27 and 30 only asked about the 3 years prior to the interview, we were uncertain that a person did not have a lifetime diagnosis if they had been missing in the prior wave. To address this, we used multiple imputation (PROC MI and MIANALYZE) procedures to synthesize results from 40 imputed datasets. Leading methodologists recommend multiple imputation as a way to minimize bias in estimates of parameters and standard errors in the presence of missing data (Graham 2009).
Results
The results indicate that the hazard for STI diagnosis in this sample increased sharply beginning around age 15, peaked at age 21, declined slightly by age 24, and then dropped off across the 20s (see Electronic Supplementary Material for a plot of the hazard curves by intervention condition). A series of survival analyses was conducted on the full sample testing (1) the association between intervention group and STI survival, (2) intervention differences controlling for ethnicity main effects, and (3) intervention-by-ethnicity interactions. All models control for gender (male), childhood low-income status, whether an individual was the child of a teen mother, time, time-squared, and inter-wave interval. Table 3 presents the results from the final model only (step 3 above) since these results were substantively similar to models 1 and 2. The results show a significant relationship between full-intervention group membership and the hazard for STI diagnosis, such that participants in the full-treatment condition who had not been previously diagnosed had a lower hazard of STI diagnosis than those in the control group at each time point. This significant association remained after controlling for gender, low-income status, ethnicity, and child of teen mom. The hazard for STI diagnosis did not differ significantly between the late-treatment and control groups. Both the linear and quadratic time terms were significant. Males had a lower hazard of STI diagnosis, and participants who experienced low-income status as children had a higher hazard of STI diagnosis. Table 3 also shows ethnicity (both European American and Asian American vs. African American) to be a significant predictor of hazard of STI onset, such that African Americans had a significantly higher hazard of STI diagnosis than European or Asian Americans. Model 3 also included the ethnicity-by-treatment interactions, and findings show that the relationship between full treatment and STI onset was significantly different for both Caucasians and Asian Americans compared to African Americans (reference group). There were no significant late treatment-by-ethnicity interactions. To understand the nature of the full treatment-by-ethnicity interactions, we examined cumulative incidence (onset) curves by treatment and ethnicity. Those for Caucasians and African Americans are presented in Fig. 2. The results suggest that intervention differences in reduced STIs were particularly large among African Americans in the study. Separate analyses were run within ethnic group (not tabled) and revealed that African Americans in the full-treatment condition were significantly less likely than African American controls to contract STIs. Significant differences between conditions were not found within the Caucasian and Asian American subsamples.

STI onset by ethnicity and intervention condition
Since African Americans in the full-treatment condition were significantly less likely than African American controls to experience STI onset, mediation analyses were tested in the survival models and path model (below) for African Americans only. Table 4 presents the results of tests for the potential mediators of the intervention group differences among the African Americans in the study. Column 1 shows the odds ratios and significance levels for the full- and late-treatment conditions compared with the control condition for African Americans after including demographic controls (childhood low-income status, gender, being the child of a teen mother). STI onset was significantly lower for the African Americans in the full-treatment compared to the control condition, even after the demographic covariates were included. There was no significant association between late treatment and STI onset. In columns 2 through 8, each potential mediator was entered one at a time to determine (1) if it predicted STI onset and (2) if its inclusion created a change in the relationship between full treatment and STI onset. Average adolescent prosocial family environment, bonding to school, having antisocial peers, early sexual initiation, and adolescent smoking all predicted STI onset; however, only prosocial family environment, school bonding, and early sexual initiation reduced the relationship between full treatment and STI onset (increased the odds ratio closer to 1.00). Thus, these were plausible mediators of the intervention effect. The inclusion of antisocial peers and cigarette use during adolescence did not alter the parameter estimates of the intervention and, thus, were less likely mediators of the intervention. Average adolescent alcohol and marijuana use neither predicted STI onset nor altered the link between intervention group and STI onset and were thus also unlikely to be mediators of the intervention. Column 9 presents the prediction of STI onset with all previously significant mediators entered into the regression and indicates partial mediation of the intervention on African American STI onset through positive family environment, school bonding, and delayed initiation of sex.
Section 3: Mediational Path Analysis
A path model using maximum likelihood estimation in Amos 18.0 (Arbuckle 2009) further tested this mediational hypothesis in predicting lifetime STI diagnosis by age 30. As with the survival analyses, intervention status significantly predicted lifetime STI diagnosis among African Americans (β = −0.37, p < 0.001), controlling for gender, childhood low-income status, and child of teen mother. Figure 2 shows the results for the meditational path model, including average adolescent positive family environment, average adolescent school bonding, and early (less than age 14) initiation of sexual behavior as mediators. Gender (female) significantly predicted delayed sexual initiation (β = 0.41, p < 0.001) and greater STI prevalence by age 30 (β = 0.21, p < 0.05). Other demographic variables were unrelated to hypothesized mediators or lifetime STI (not shown). Full-intervention group membership significantly predicted a more positive family environment, higher adolescent school bonding, and later initiation of sexual behavior. In turn, positive family environment predicted lower lifetime STI diagnosis, as did early initiation of sexual behavior. However, unlike in the survival analyses, school bonding did not predict lifetime prevalence of STI diagnosis in this model. With the inclusion of the three adolescent mediators, the coefficient for intervention prediction of lifetime STIs was reduced from β = -0.37 (p < 0.001) to β = -0.27 (p < 0.05), indicating partial mediation of the intervention through better family environment and delayed initiation of sexual behavior.
Discussion
Results from the present study revealed (1) that the universally administered full SSDP preventive intervention in grades 1 through 6 was significantly associated with reduced onset of STIs through age 30; (2) that this association was most pronounced for the African American participants in the study; and (3) that adolescent positive family environment, school bonding, and delayed initiation of sexual behavior mediated, in part, the association between intervention condition and STI onset for African Americans.
The SSDP intervention is not a curriculum-based sex or STI/HIV education program. The intervention sought to reduce risk behavior and promote positive social development by improving teachers’ classroom management and instruction, children’s social competence, and parenting practices during the elementary grades. In conjunction with prior SSDP findings, the results of the current study support Rotheram-Borus’s (2000) suggestion to expand the range of interventions to reduce risky sexual behavior among adolescents by including interventions addressing general social competency and promoting prosocial behaviors. In addition, these findings support the suggestions of Bailey (2009) and O’Connell et al. (2009) that it is important to examine effects of preventive interventions that seek to affect shared risk and protective factors for diverse health-risking behaviors. By addressing shared risk factors for multiple health-risking behaviors and by promoting shared protective factors, it is possible to affect a broad range of mental, emotional, and behavioral outcomes.
The association between the full SSDP intervention and STI onset was strongest for African Americans, a group that bears a disproportionate burden in terms of STI (Gavin et al. 2009, and as indicated by the control group in Fig. 3). This finding of a stronger intervention association for African Americans is consistent with an earlier study by Lonczak et al. (2002) where a greater proportion of single African Americans in the full-intervention group reported use of condoms at last intercourse at age 21. It is possible that that greater use of condoms by African Americans in the full-intervention group contributed to the observed reduction in STI onset among African Americans. A major contribution of this study is the identification of specific meditational mechanisms including improved family functioning, school bonding, and delayed initiation of sexual behavior as additional factors accounting for the reduction in STI onset observed among African Americans in the full-intervention group.

Path model testing meditational mechanisms of association between intervention and lifetime STI by age 30 among African Americans only (n = 175)
Program effects on target outcomes are often reported in research papers, but program effects on mediators, particularly potential mediating mechanisms to explain long-term effects, are less commonly examined (DeGarmo et al. 2009; MacKinnon and Lockwood 2003). The observed associations between intervention group and positive family environment, school bonding, and delayed initiation of sexual behavior are important because the SSDP intervention ended at age 12 with no subsequent booster sessions. Evidence for the mediational role of school bonding was stronger in the survival analyses than in the path model; however, its significant association with lifetime STI may have dropped out of the path model due to its correlation with the other mediators. Overall, it is plausible that gains in family functioning, school bonding, and risk behavior attained through the full SSDP intervention during elementary grades (Hawkins et al. 1992, 1988, 1991) put children on a positive trajectory that continued to affect adolescent and adult risk behaviors through age 30.
There was no association between intervention condition and average adolescent affiliation with deviant peers and alcohol, cigarette, and marijuana use in either the overall sample or within ethnic groups. As shown in Table 2 and in prior research, however, these factors are associated with lifetime STI; therefore, they may still be important intervention targets for preventing STIs, even though they were not found to be mediators of the SSDP intervention in this study.
Limitations should be noted. The study was quasi-experimental and geographically limited. Although SSDP has a number of strong methodological features, including very low attrition, long-term follow-up, and no significant differential attrition by condition, it was a non-randomized controlled trial, and, despite there being no measurable baseline or age 30 characteristic differences between the intervention and control groups on available measures, there may have been unmeasured differences and, thus, residual confounding which could partially account for the observed effect sizes. Second, the study relied heavily on self-reported data from study participants. Estimates of STI prevalence based on self-report may be low because respondents may not know they have an STI. In addition, study questions asked about respondents’ age at first diagnosis, but data on when STIs were actually acquired were unavailable. Hazard rates for first diagnosis in this sample peaked in late adolescence and the early 20s, however, mirroring estimates of the ages of peak risk based on national data (Centers for Disease Control and Prevention 2003). Furthermore, some hypothesized effects were not found: links between the intervention and adolescent positive family environment, school bonding, delayed initiation of sexual behavior, and STI onset and age 30 lifetime prevalence were found for African Americans in the study, but significant links with average adolescent interaction with antisocial peers or alcohol, cigarette, or marijuana use were not observed. Finally, the SSDP study population came from an urban area, with approximately half the children coming from low socioeconomic groups and minority ethnic groups, which might limit the generalizability of these findings to less heterogeneous populations.
Intervention group differences reported in the present study indicate that universal intervention during the elementary grades to improve the classroom management and instructional skills of urban public elementary school teachers strengthen parenting practices in multiethnic urban families, and ensure that children have the skills to participate in the social and academic life of elementary school may reduce the onset of sexually transmitted infections and lifetime prevalence of STIs well into adulthood. Study findings indicate that the association between these childhood intervention components and STI onset was mediated, in part, by better family environments, higher bonding to school, and delayed initiation of sexual behavior during adolescence.
References
Allison, P. D. (1995). Survival analysis using the SAS system: A practical guide (2nd ed.). Cary, NC: SAS Institute.
Aos, S., Lieb, R., Mayfield, J., Miller, M., & Pennucci, A. (2004). Benefits and costs of prevention and early intervention programs for youth. Retrieved 27 September 2004 from http://www.wsipp.wa.gov/pub.asp?docid=04-07-3901.
Arbuckle, J. A. (2009). Amos 18 user’s guide. Crawfordville, FL: Amos Development Corporation.
Bailey, J. A. (2009). Editorial: Addressing common risk and protective factors can prevent a wide range of adolescent risk behaviors. Journal of Adolescent Health, 45, 107–108.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182.
Catalano, R. F., & Hawkins, J. D. (1996). The social development model: A theory of antisocial behavior. In J. D. Hawkins (Ed.), Delinquency and crime: Current theories (pp. 149–197). New York: Cambridge University Press.
Centers for Disease Control and Prevention. (2003). Sexually transmitted disease surveillance, 2002. Atlanta, GA: U.S. Department of Health and Human Services.
DeGarmo, D. S., Eddy, J. M., Reid, J. B., & Fetrow, R. A. (2009). Evaluating mediators of the impact of the Linking the Interests of Families and Teachers (LIFT) multimodal preventive intervention on substance use initiation and growth across adolescence. Prevention Science, 10, 208–220.
Dielman, T. E. (1994). Correction for the design effect in school-based substance use and abuse prevention research: Sample size requirements and analysis considerations. In A. Cázares & L. A. Beatty (Eds.), NIDA Research Monograph: Vol. 139. Scientific methods for prevention intervention research (pp. 115–126). Rockville, MD: National Institute on Drug Abuse.
Gavin, L., MacKay, A. P., Brown, K., Harrier, S., Ventura, S. J., Kann, L., et al. (2009). Sexual and reproductive health of persons aged 10–24 years—United States, 2002–2007. MMWR, 58, 1–58.
Gavin, L., Catalano, R. F., David-Ferdon, C., Gloppen, K. M., & Markham, C. M. (2010). A review of positive youth development programs that promote adolescent sexual and reproductive health. Journal of Adolescent Health, 46, S75–S91.
Cook, R. L., Pollock, N. K., Rao, A. K., & Clark, D. B. (2002). Increased prevalence of herpes simplex virus type 2 among adolescent women with alcohol use disorders. Journal of Adolescent Health, 30(3), 169–174.
Graham, J. W. (2009). Missing data analysis: Making it work in the real world. Annual Review of Psychology, 60, 549–576.
Graham, J. W., & Hofer, S. M. (2000). Multiple imputation in multivariate research. In T. D. Little, K. U. Schnabel, & J. Baumert (Eds.), Modeling longitudinal and multi-group data: Practical issues, applied approaches, and specific examples (pp. 201–218). Hillsdale, NJ: Lawrence Erlbaum.
Grunseit, A., Kippax, S., Aggleton, P., Baldo, M., & Slutkin, G. (1997). Sexuality education and young people’s sexual behavior: A review of studies. Journal of Adolescent Research, 12, 421–453.
Guo, J., Chung, I.-J., Hill, K. G., Hawkins, J. D., Catalano, R. F., & Abbott, R. D. (2002). Developmental relationships between adolescent substance use and risky sexual behavior in young adulthood. Journal of Adolescent Health, 31(4), 354–362.
Hawkins, J. D., & Weis, J. G. (1985). The social development model: An integrated approach to delinquency prevention. Journal of Primary Prevention, 6, 73–97.
Hawkins, J. D., Doueck, H. J., & Lishner, D. M. (1988). Changing teaching practices in mainstream classrooms to improve bonding and behavior of low achievers. American Educational Research Journal, 25, 31–50.
Hawkins, J. D., Von Cleve, E., & Catalano, R. F., Jr. (1991). Reducing early childhood aggression: Results of a primary prevention program. Journal of the American Academy of Child and Adolescent Psychiatry, 30, 208–217.
Hawkins, J. D., Catalano, R. F., Morrison, D. M., O’Donnell, J., Abbott, R. D., & Day, L. E. (1992). The Seattle Social Development Project: Effects of the first four years on protective factors and problem behaviors. In J. McCord & R. E. Tremblay (Eds.), Preventing antisocial behavior: Interventions from birth through adolescence (pp. 139–161). New York: Guilford.
Hawkins, J. D., Catalano, R. F., Kosterman, R., Abbott, R., & Hill, K. G. (1999). Preventing adolescent health-risk behaviors by strengthening protection during childhood. Archives of Pediatrics & Adolescent Medicine, 153, 226–234.
Hawkins, J. D., Kosterman, R., Catalano, R. F., Hill, K. G., & Abbott, R. D. (2005). Promoting positive adult functioning through social development intervention in childhood: Long-term effects from the Seattle Social Development Project. Archives of Pediatrics & Adolescent Medicine, 159, 25–31.
Hawkins, J. D., Kosterman, R., Catalano, R. F., Hill, K. G., & Abbott, R. D. (2008). Effects of social development intervention in childhood fifteen years later. Archives of Pediatrics & Adolescent Medicine, 162, 1133–1141.
Hedges, L. & Rhoads, C. (2009). Statistical Power Analysis in Education Research (NCSER 2010-3006). Washington, DC: National Center for Special Education Research, Institute of Education Sciences, U.S. Department of Education. This report is available on the IES website at http://ies.ed.gov/ncser/.
Kellam, S. G., & Rebok, G. W. (1992). Building developmental and etiological theory through epidemiologically based preventive intervention trials. In J. McCord & R. E. Tremblay (Eds.), Preventing antisocial behavior: Interventions from birth through adolescence (pp. 162–195). New York: Guilford.
Keyes, M. A., Iacono, W. G., & McGue, M. (2007). Early onset problem behavior, young adult psychopathology, and contextual risk. Twin Research and Human Genetics, 10(1), 45–53.
Kirby, D. (2007). Emerging answers: Research findings on programs to reduce teen pregnancy. Retrieved September 2008 from http://www.thenationalcampaign.org/resources/pdf/pubs/EA2007_FINAL.pdf.
Kish, L. (1965). Survey sampling. New York: Wiley.
Lonczak, H. S., Abbott, R. D., Hawkins, J. D., Kosterman, R., & Catalano, R. F. (2002). Effects of the Seattle Social Development Project on sexual behavior, pregnancy, birth, and sexually transmitted disease outcomes by age 21 years. Archives of Pediatrics & Adolescent Medicine, 156, 438–447.
Lowry, R., Holtzman, D., Truman, B. I., Kann, L., Collins, J. L., & Kolbe, L. J. (1994). Substance use and HIV-related sexual behaviors among US high school students: Are they related? American Journal of Public Health, 84(7), 1116–1120.
MacKinnon, D. P., & Lockwood, C. M. (2003). Advances in statistical methods for substance abuse prevention research. Prevention Science, 4, 155–171.
Murray, D. M., Rooney, B. L., Hannan, P. J., Peterson, A. V., Ary, D. V., Biglan, A., et al. (1994). Intraclass correlation among common measures of adolescent smoking: Estimates, correlates, and applications in smoking prevention studies. American Journal of Epidemiology, 140, 1038–1050.
Muthén, B. O., & Satorra, A. (1995). Complex sample data in structural equation modeling. Sociological Methodology, 25, 267–316.
Nitz, K. (1999). Adolescent pregnancy prevention: A review of interventions and programs. Clinical Psychology Review, 19, 457–471.
O’Connell, M. E., Boat, T., & Warner, K. E. (2009). Preventing mental, emotional, and behavioral disorders among young people: Progress and possibilities. Washington, DC: National Academies Press.
Rotheram-Borus, M. J. (2000). Expanding the range of interventions to reduce HIV among adolescents. AIDS, 14, s33–s40.
Valois, R. F., Oeltmann, J. E., Waller, J., & Hussey, J. R. (1999). Relationship between number of sexual intercourse partners and selected health risk behaviors among public high school adolescents. Journal of Adolescent Health, 25(5), 328–335.
Willett, J. B., Singer, J. D., & Martin, N. C. (1998). The design and analysis of longitudinal studies of development and psychopathology in context: Statistical models and methodological recommendations. Development and Psychopathology, 10, 395–426.
Woods, W. J., Lindan, C. P., Hudes, E. S., Boscarino, J. A., Clark, W. W., & Avins, A. L. (2000). HIV infection and risk behaviors in two cross-sectional surveys of heterosexuals in alcoholism treatment. Journal of Studies on Alcohol, 61(2), 262–266.
Acknowledgments
Funding for this study was provided by the National Institute on Drug Abuse (NIDA; R01DA003721, R01DA009679, R01DA024411) and 21548 from the Robert Wood Johnson Foundation. These organizations had no further role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Financial Disclosure
Dr. Catalano receives reimbursement for being a member of the board of Channing Bete Co., distributor of Supporting School Success and Guiding Good Choices.
Additional Information
Supporting School Success and Guiding Good Choices were tested in the study that produced the dataset used in this article.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 50 kb)
Rights and permissions
About this article
Cite this article
Hill, K.G., Bailey, J.A., Hawkins, J.D. et al. The Onset of STI Diagnosis Through Age 30: Results from the Seattle Social Development Project Intervention. Prev Sci 15 (Suppl 1), 19–32 (2014). https://doi.org/10.1007/s11121-013-0382-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-013-0382-x