
Abstract
The aim of this study was to examine the pathways that link mothers’ early life socio economic status (SES) and mothers’ experience of childhood maltreatment with birth weight among their later born offspring. Data were drawn from a nationally representative longitudinal survey of school-aged respondents, initially enrolled during adolescence in Wave I (1994–1995) and Wave II (1996) of the National Longitudinal Study of Adolescent Health and followed-up in adulthood in Wave III (2001–2002). Data on offspring birth weight were obtained from nulliparous females (N = 1,897) who had given birth between Waves II and III. Analyses used structural equation modeling to examine the extent to which early life maternal risk predicted offspring birth weight, and demonstrated that maternal childhood SES and maternal childhood maltreatment predicted offspring birth weight through several mediated pathways. First, maternal adolescent substance use and prenatal cigarette use partially mediated the association between maternal childhood SES and offspring birth weight. Second, maternal adolescent depressive symptoms and adult SES partially mediated the association between maternal childhood SES and offspring birth weight. Third, adult SES partially mediated the association between maternal childhood SES and offspring birth weight. Fourth, maternal adolescent substance use and prenatal cigarette use partially mediated the association between maternal childhood maltreatment and offspring birth weight. Finally, maternal adolescent depressive symptoms and adult SES partially mediated the association between maternal childhood maltreatment and offspring birth weight. To our knowledge, this is the first study to identify maternal childhood maltreatment as an early life risk factor for offspring birth weight among a nationally representative sample of young women, and to demonstrate the mechanisms that link childhood SES and maltreatment to offspring birth weight. These findings suggest the importance of designing and implementing prevention and intervention strategies to address early life maternal social conditions in an effort to improve inter generational child health at birth.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Low birth weight (LBW, <2,500 g) is a significant public health problem in the United States. LBW infants are at increased risk of neonatal death compared with normal-weight infants (Aarnoudse-Moens et al. 2009). Despite substantial research and advances in obstetric care, the overall rate of LBW increased 6.9% in 1990 to 8.16% in 2009 (Hamilton et al. 2010). The LBW rate among singletons has also risen over the last decade, increasing 8.4% from 1990 through 2008 (Martin et al. 2010). Although some posit the increase in LBW is due to the rise in multiple births, advanced maternal age, availability of medical technologies that increase survival rates of very LBW infants, and increased use of infertility therapies (Engle and Kominiarck 2008; Williams and Sutcliffe 2009), reasons for the decline in birth weight among low-risk singleton infants remain unclear (Donahue et al. 2010).
LBW is linked not only to complications during the neonatal period but also health and chronic disease risk across the life course. Research shows that LBW, as well as in combination with weight gain across the life course, is associated with cardiovascular events in adulthood (Barker et al. 2002; Rich-Edwards et al. 2005). Low birth weight has also been linked to chronic health conditions in adulthood including obesity (Oken and Gillman 2003), type 2 diabetes (Whincup et al. 2008), and hypertension (Gamborg et al. 2007).
One explanation for the lack of progress in reducing the prevalence of LBW is the narrow, conventional approach to pregnancy as a relatively acute condition (Collins et al. 2003), with studies predominantly performed only during the antenatal period among women who seek prenatal care services. Evidence is mounting, however, that this traditional prenatal period is too brief an interval to effectively discern or address the health, social, and psychological needs of women at greatest risk for delivering LBW infants (Lu et al. 2006).
There are numerous interventions that, if delivered prior to the prenatal period could improve pregnancy outcomes; however, preconception care services are not systematically available to all women (Atrash et al. 2006). For example, women most likely to access preconception care services are those with planned pregnancies, which result in the exclusion of a large number of women with unintended pregnancies (Finer and Henshaw 2006). Evidence indicates that individual aspects of preconception care (e.g., smoking cessation) are often effective, but little is known about whether these interventions are successful in improving birth outcomes (Atrash et al. 2006). Given that prenatal and preconception care alone are unlikely to be sufficient to lower the prevalence of LBW, knowledge of early life risk factors could provide valuable information for the design of effective interventions.
Life-course research demonstrates that the mother’s own developmental experiences in infancy, childhood, and adolescence are important determinants of her health in adulthood and the health of her children (Braveman and Barclay 2009). The life-course perspective on health frames an individual’s current biological status as a marker of past social position. In turn, past social position affects future social advantage or disadvantage, which then affects a myriad of economic and health outcomes (Lynch and Smith 2005). For example, a large body of research has documented the long-term effects of exposures to stressful events in childhood on adverse health outcomes and behaviors in adulthood. The Adverse Childhood Experiences (ACE) Study posits that exposure to traumatic events in childhood results in long-term brain dysfunction, which affects health and well-being across the life course. Findings from studies that used ACE Study data, suggest that adults exposed to multiple childhood traumatic events and in some cases specific traumatic events (e.g., childhood abuse, household substance abuse, household mental illness, parental separation or divorce) are at increased risk for substance use (Anda et al. 2006; Dube et al. 2002), mental health problems (Anda et al. 2006; Chapman et al. 2004), and premature death (Brown et al. 2009). These findings, which link early life risk factors to disparities in adult health outcomes, have highlighted the importance of assessing the extent to which maternal early life risk factors may be etiologically significant for adverse birth outcomes.
The recognition that maternal early life risk factors may be linked to future birth outcomes is not new. Maternal birth weight has been positively linked to offspring birth weight (Stein and Lumey 2000). The link between maternal health in childhood and subsequent birth outcomes has been established by studies in the United Kingdom beginning in the 1940s (Baird 1974; Emanuel 1986). A study in Aberdeen, Scotland revealed that women born during the years of the Great Depression (1927–1937) tended to deliver LBW infants (Baird 1974). Similarly, mean infant birth weights were lower among women who moved from lower to higher social classes during life, compared to infants born to women who remained in higher social classes during life (Illsely 1955). More recently, prospective studies have also shown maternal low socioeconomic status (SES) in childhood (Astone et al. 2007; Gisselman et al., 2006) and maternal LBW (Hypponen et al. 2004) positively linked to LBW in offspring. In a recent study, violence/mental health issues in childhood and exposure to multiple childhood hardships were also associated with LBW in offspring (Harville et al. 2010). Despite the body of research that links maternal early life risk factors to offspring LBW, we believe additional research in this area is warranted. Specifically, we need to better understand the mechanisms that link maternal early life conditions and offspring birth weight.
The present study is grounded in a life-course perspective to examine whether maternal early life factors operate in conjunction as well as independently with more proximal, perinatal and economic factors to influence offspring birth weight. In the study reported here, we investigated two pathways that may link a mother’s early life adversity to her infant’s birth weight: maternal childhood SES and childhood maltreatment. The first pathway examines the association between maternal childhood SES and offspring birth weight. Research has shown maternal low childhood SES predicts offspring LBW (Astone et al. 2007; Gisselmann 2006). However, to our knowledge, no study to date has examined potential mechanisms of the effect of childhood SES on offspring LBW. This is a noted limitation because other studies have demonstrated that low childhood SES is associated with depressive symptoms in adolescence and adulthood (Gilman et al. 2002) and prenatal depressive symptoms are associated with LBW (Grote et al. 2010). In addition, low SES in childhood may be an important determinant of LBW in later born offspring, because child and adult SES are associated. Specifically, low childhood SES determines low SES in adulthood, which may be linked to poorer health outcomes in adulthood (Luo and Waite 2005). Studies have shown that low SES women report a higher prevalence of depression (Kahn et al. 2000) and are at increased risk to deliver LBW infants (Grote et al. 2010). Finally, there is evidence that childhood SES may be a risk factor for cigarette, alcohol, and drug use (Humensky 2010). Given the association between adolescent substance use, prenatal substance use, and offspring LBW (Gavin et al. 2011), childhood SES may be an important risk factor for offspring LBW. Specifically, we are interested in examining the role that maternal childhood SES plays in conferring risk on maternal health behaviors and mental health status, which in turn may affect the birth weight of later born offspring.
The second proposed pathway examines the impact of maternal childhood maltreatment on offspring birth weight. Child maltreatment has been found to predict a myriad of adverse outcomes during adolescence and adulthood, including cigarette smoking in adulthood (Topitzes et al. 2009) and adolescent and adult substance use (e.g., tobacco, alcohol, illicit drug use) (Lansford et al. 2009; Wilson and Widom 2009). Childhood maltreatment is also associated with increased risk of mood disorder such as adolescent and adult depression (Chapman et al. 2004) and economic disadvantage in adulthood (Zielinski 2009). Research studies have shown prenatal depressive symptoms (Grote et al. 2010) and prenatal tobacco use (Gyllstrom et al. 2010) to be associated with increased risk of LBW. Recently, Gavin et al. (2011) using longitudinal data from a community-based sample of 136 respondents first assessed in 5th grade and followed through young adulthood, examined pathways linking early life adversity to offspring birth weight. Findings suggest that maternal early childhood maltreatment predicted offspring birth weight through a mediated pathway including adolescent substance use (e.g., binge drinking, tobacco use, illicit drug use) and prenatal substance use (e.g., tobacco and alcohol use). These findings support the assessment of early life risk exposures in the development of interventions designed to reduce the risk of LBW. However, this study included a high-risk, community-based sample of young women. From a prevention framework, it is important to examine the pathways linking early life risk and offspring birth weight in nationally representative samples.
Using data from a nationally representative cohort study of school-age adolescents first interviewed in 7th–12th grades and followed longitudinally through young adulthood, we examined the following research questions: (1) Does childhood SES predict offspring birth weight through a mediated pathway including adolescent substance use, adolescent depressive symptoms, prenatal cigarette use, and adult SES? (2) Does maternal childhood maltreatment predict offspring birth weight through a mediated pathway that includes adolescent substance use, prenatal cigarette use, adolescent depressive symptoms, and adult SES? We hypothesized that childhood SES predicts offspring birth weight through a mediated pathway including adolescent substance use, adolescent depressive symptoms, prenatal cigarette use, and adult SES. Second, we hypothesized that maternal childhood maltreatment predicts offspring birth weight through a mediated pathway including adolescent substance use, adolescent depressive symptoms, prenatal cigarette use, and adult SES.
Methods
Sample and Procedure
We used data from the National Longitudinal Study of Adolescent Health (Add Health), an ongoing nationally representative, school-based study of adolescents in grades 7 through 12 that began in 1994 and follows respondents into young adulthood. Add Health was designed to explore the causes of health-related behaviors, with an emphasis on the influence of social context (Harris et al. 2009). A systematic, random sample of 80 high schools and 52 associated feeder schools from across the United States was then selected, stratified according to region, urbanicity, school type, ethnic composition, and school size. More than 70% of the schools originally selected for the survey participated. During the 1994–1995 school year, the Wave I in-school questionnaire was administered to every student (N = 90,118) from a national sampling frame that included all high schools in the United States that had both an 11th grade and at least 30 students enrolled in the school. From April 1995 to December 1995, Wave I in-home interviews were completed by 20,745 students aged 11 to 19 years (79% response rate). At Wave I, a parent, usually the resident mother also participated in a separate in-home interview. From April 1996 to August 1996, all adolescents in grades 7 through 11 in Wave I were re-interviewed for the Wave II in-home interview, of these, 16,706 students were selected for a second interview in 1996; 13,568 students completed the interview. The response rate for Wave II was 88.2%. In 2001 and 2002, more than 15,000 Add Health respondents, 18 to 28 years old, were re-interviewed in Wave III to investigate the influence that adolescence has on emerging adulthood (response rate of 77.4%) (Bearman et al. 1997; Chantala et al. 2003). The in-home interviews were administered both by Computer-Assisted Self Interview (CASI) and audio Computer-Assisted Self Interview (ACASI). In the former, an interviewer verbally posed questions to respondents and entered the responses directly into a laptop computer. The latter is used to gather information regarding more private topics (e.g., child maltreatment, substance use). For these sections, respondents listened to pre-recorded questions using headphones and entered their own responses (Harris and Cheng 2007).
Data for the present analyses focused on a subsample of nulliparous females who had participated in Waves I–III and reported giving birth to a live singleton between Waves II–III. Add Health study procedures were approved by the Human Subjects Review Committee at the University of North Carolina, Chapel Hill. The present study was approved by the Center for Studies in Demography and Ecology at the University of Washington under contractual agreement from the Carolina Population Center at the University of North Carolina, Chapel Hill.
Measures
Offspring Birth Weight
Offspring birth outcome data were obtained from the Wave III interview. An eligible birth was defined using the following criteria: those who reported no live births prior to Wave II, and who reported a live singleton birth after the Wave II interview and before the Wave III interview. Maternal self-reported data were used to obtain offspring birth weight.
Childhood Maltreatment
In Wave III, respondents were asked three questions regarding the frequency of mistreatment by adults before they began the 6th grade. The maltreatment questions are modified versions of questions from previous surveys (Finkelhor and Dzuiba-Letherman 1994; Straus et al. 2004). The questions were asked retrospectively during the Wave III interview when respondents were on average 22 years old. Due to the sensitive nature of the maltreatment questions, Add Health administered the questions using ACASI. In the present study, we selected three single questions regarding maltreatment in childhood. Respondents were asked “how often had your parents or other adult care-givers not taken care of your basic needs, such as keeping you clean or providing food or clothing?” [physical neglect]; “how often had your parents or other adult care-givers slapped, hit, or kicked you?” [physical abuse]; and “how often had your parents or other adult care-givers touched you in a sexual way, forced you to touch him or her in a sexual way, or forced you to have sexual relations?” [sexual abuse]. Respondents indicated the frequency with which each question applied to her experience (coded from 0 = never happened to 5 = happened more than 10 times).
Childhood SES
Data from the Wave I parental interview, included parental education (coded from 1 = ≤ 8th grade to 9 = post 4-year college, professional degree) and parental household income (coded from 1 = $0–$9,999 to 8 = $50,000 or more).
Adolescent Substance Use
In Wave I, respondents were asked questions about the frequency of their substance use. Based on these data, we created the following adolescent substance use measures: binge drinking (≥5 drinks in a row in the past year [versus never]); 30-day cigarette use (smoked cigarettes ≥1 day in the past month [versus no days]); and 30-day marijuana use (used marijuana ≥1 day in the past month [versus no days]) (Hussey et al. 2006; Jessor et al. 2006; Oesterle et al. 2004). We did not use a gender-specific cutoff (e.g., ≥4 drinks for females), because only one question about 5 drinks or more was asked at Wave I.
Adolescent Depressive Symptoms
In Wave I, the Add Health Study included an 18-item version of the Center for Epidemiologic Studies Depression Scale (CES-D). The CES-D measures the overall level of depressive symptoms (experienced during the past week) (Radloff 1977). In the present study, the internal consistency of the modified scale (α = 0.87) was similar to those reported by previous studies (Cummings et al. 2010). Each item was rated on a scale of 0 (never or rarely) to 3 (most or all the time). CES-D scores ranged from 0 (no symptoms) to 44 (maximum depressive symptoms), and were summed to create a composite score (Mueller 2009).
Prenatal Cigarette Use
In Wave III, respondents were asked to retrospectively report on the frequency of cigarette use during pregnancy. Respondents were asked: “During this pregnancy, how many cigarettes did you smoke?” Response options for cigarette use included 0 = none, 1 = 1 pack a day or less, 2 = more than 1 pack a day, but less than 2 packs a day, and 3 = 2 or more packs a day. In the present study, prenatal cigarette use was coded as 0 = none; 1 = less than 1 pack a day/ 1 or more packs a day.
Adult SES
SES in adulthood was indicated by respondents’ personal income and/or respondent partners’ income (coded from 1 = $0–$9,999 to 8 = $75,000 or more).
Analytic Strategy
The hypothesized inter generational relations between maternal early life risk factors and offspring birth weight were evaluated using weighted least squares (WLSMV) in Mplus Version 5.0 (Muthén and Muthén 1998–2007). The Add Health study was based on a cluster sample in which clusters were sampled with unequal probability. Therefore, sampling weights were applied in all analyses. Analyses were also conducted using maximum likelihood estimation (MLE) to determine whether findings differed substantially as a function of the estimator. Results were comparable across both estimators (e.g., WLSMV and MLE). Modeling was done in two stages. Given our hypotheses that maternal early life risk exposures influence offspring birth weight, we first evaluated the measurement model by conducting a confirmatory factor analysis (CFA) of maternal childhood SES, childhood maltreatment, adolescent substance use, and adult SES (Kline 2011). Then, we analyzed the hypothesized structural relations among the model constructs. We report three indicators of model fit: the chi-square estimate (χ 2), the comparative fit index (CFI), and the root mean square error of approximation (RMSEA).
Missing Data Strategy
Weighted descriptive statistics presented in Table 1 were estimated in Stata Version 10 (StataCorp 2007) using listwise deletion. Mplus using the WLSMV estimator was also employed to obtain parameter estimates and standard errors for the CFA and the structural relations among the model constructs. The effective sample size for the Mplus analysis was 1,897.
Results
Descriptive Analysis and Confirmatory Factor Analysis
Table 1 shows descriptive statistics of all study variables. In preliminary analyses, prenatal alcohol (r = 0.012) and drug use (r < −0.001) were not significantly correlated with offspring birth weight, and the inclusion of these variables did not alter the other paths in the model. Therefore, these variables were not included in subsequent models. Table 2 presents the factor loadings for the latent variables in the model including maternal childhood maltreatment, childhood SES, adolescent substance use and adult SES. Model fit was acceptable (χ 2 [22] = 48.79, p < .01, CFI = .95, RMSEA = .025). All indicators loaded significantly on their respective latent factors and the CFA of latent constructs suggests support for the hypothesized measurement model. Table 3 presents the results of the bivariate correlation analyses of study variables, showing significant associations among the key variables. Maternal childhood SES was statistically associated with adolescent substance use, adolescent depressive symptoms, and adult SES. Maternal childhood maltreatment was positively and statistically associated with adolescent substance use, adolescent depressive symptoms, and prenatal cigarette use. Additionally, there was a significant and inverse association between prenatal cigarette use and offspring birth weight, while adult SES was positively and statistically associated with offspring birth weight.
Structural Equation Model
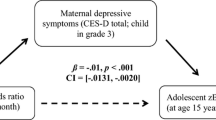
Structural equation modeling (SEM) with WLSMV in Mplus was used to examine the effects of maternal childhood SES and childhood maltreatment on offspring birth weight. Adolescent substance use, adolescent depressive symptoms, prenatal cigarette use, and adult SES were also tested as potential mediators of these early life risks. Figure 1 presents the SEM and the standardized model parameter estimates. The measurement model of the latent variables in the SEM was similar in factor loadings to that described in the CFA. The SEM model fit indicated good representation of the data (CFI = .95, RMSEA = 0.025). Maternal childhood SES significantly predicted more frequent adolescent substance use (β = .24, p = .002), less adolescent depressive symptoms (β = −.15, p = .026), and higher adult SES (β = .22, p = .002). Maternal childhood maltreatment significantly predicted more frequent adolescent substance use (β = .21, p < .001) and higher adolescent CES-D scores (depressive symptoms) (β = .15, p = 0.001). Mediated pathways between maternal childhood SES and offspring birth weight as well as maternal childhood maltreatment and offspring birth weight were similar, such that maternal adolescent substance use significantly predicted more prenatal cigarette use (β = .31, p < .001). In addition, higher maternal adolescent CES-D scores significantly predicted lower adult SES (β = −.10, p = .023). Offspring birth weight was significantly reduced by prenatal cigarette use (β = −.08, p = .015) and higher adult SES significantly predicted higher offspring birth weight (β = .09, p = .035).

The SEM and the standardized model parameter estimates. Coefficients are standardized estimates. Solid lines are significant at p < .05 or better, dotted lines are not significant. Single-headed arrows are regression paths, double headed arrows are correlations. SES = socioeconomic status. *p < .05; **p < .01; ***p < .001; ns = not significant
Discussion
This study examined the mediated pathways between maternal childhood SES and maternal childhood maltreatment and offspring birth weight among a nationally representative sample of young women. Our findings demonstrate mediated pathways of influence from maternal childhood SES and childhood maltreatment to offspring birth weight. To our knowledge, this is the first study to establish a link between maternal childhood maltreatment and offspring birth weight in a nationally representative sample. Further, the influence of maternal childhood maltreatment on offspring birth weight is partially mediated through adolescent substance use and prenatal cigarette use, as well as adolescent depressive symptoms and adult SES. Additionally, this is one of the first studies to examine the mediators that link maternal childhood SES and offspring birth weight among a nationally representative sample of young women. Specifically, we found the pathway between childhood SES and offspring birth weight was partially mediated through adolescent substance use and prenatal cigarette use, adolescent depressive symptoms and adult SES.
We found an association between maternal childhood SES and offspring birth weight consistent with previous findings (Astone et al. 2007; Gisselmann 2006). We contribute to this literature by showing that maternal adolescent depressive symptoms and adult SES are two mechanisms by which childhood SES affects offspring birth weight. This study confirmed the association between SES across the early life course and health outcomes, thus lending support to the social causation theory (Warren 2009). Social causation theory posits that the stress associated with low SES may affect the psychological well-being of individuals and increase their vulnerability to health problems (Sareen et al. 2011). In the present study, we showed that maternal childhood SES influenced depressive symptoms in adolescence, that maternal adolescent depressive symptoms influenced SES in adulthood, and that maternal adult SES affected offspring birth weight. Our findings are similar to previous studies that examined a variety of health outcomes (Gilman et al. 2002; Luo and Waite 2005; Melchior et al. 2007) and suggests that childhood SES has long-term effects on offspring birth weight via adolescent mental health and SES in adulthood.
We also found that high adult SES significantly predicted increased offspring birth weight (Nepomnyaschy 2009). Our finding mirrors the findings of numerous studies that have confirmed higher SES in adulthood is associated with better adult health across a range of outcomes (Anderson and Armstead 1995). Interestingly, we also found that adolescent substance use and prenatal cigarette use were mechanisms of influence in the pathway between maternal childhood SES and offspring birth weight. This finding suggests that high SES in childhood may be a risk factor for adolescent substance use, which in turns contributes to cigarette use in later phases of the life course. There is support for this finding. Previous studies have shown that adolescents and college-aged students with more spending money reported higher levels of drinking (Martin et al. 2009). A recent study using Add Health data reported that higher childhood SES (e.g., parental education and household income) was associated with higher rates of binge drinking, marijuana and cocaine use in early adulthood (Humensky 2010).
Our findings indicated that prenatal cigarette use predicted offspring birth weight, consonant with other studies that have shown intrauterine exposure to tobacco smoking to be associated with LBW (Anderson et al. 2009; Gyllstrom et al. 2010). A hypoxic mechanism may explain the biological link between prenatal smoking and LBW. At present, there is evidence that prenatal smoking reduces the production of an enzyme (endothelial nitric oxide synthase [eNOS]), which is responsible for regulating blood vessel dilation (Anderson et al. 2009). Lower production of eNOS may result in the narrowing of blood vessels and less blood flow to the fetus, resulting in physiological changes such as LBW. However, further studies are needed to examine to what extent prenatal smoking reduces eNOS activity by nicotine exposure, carbon monoxide exposure, or exposure to other toxic substances present in cigarette smoke (Anderson et al. 2009).
In the present study, a mechanism of influence of maternal childhood maltreatment on offspring birth weight was through adolescent substance use (Dube et al. 2006; Lansford et al. 2009). Some posit that individuals who experience maltreatment in childhood fail to develop constructive coping strategies necessary to manage with acute and chronic stressors, and will shift to alcohol and drugs use to cope or self-medicate (Widom et al. 2006). Our findings that childhood maltreatment influenced offspring birth weight via adolescent substance use and prenatal smoking, suggest recurrent exposures to childhood maltreatment may adversely affect early development of the central nervous system (Dube et al. 2006). That is, child abuse has been linked with hypothalamic-pituitary-adrenal axis and autonomic nervous system dysregulation in adulthood (Heim et al. 2000). Thus, early physiologic alterations may affect a youth’s ability to cope with negative emotions contributing to problems with self-regulation (van der Kolk et al. 1991) and potential substance abuse.
We also found adolescent depressive symptoms and adult SES mediated the pathway between maternal childhood maltreatment and offspring birth weight. This finding suggests that adolescent depressive symptoms and adult SES are the mechanisms by which childhood maltreatment influenced offspring birth weight. Consistent with our finding, earlier studies have shown that adolescent depressive symptoms were common among individuals who reported childhood maltreatment (Fletcher 2009). Our finding also indicated an association between adolescent depressive symptoms and low SES in adulthood (Goodman et al. 2011). Recent studies have shown significant economic consequences in adulthood among individuals who experienced childhood maltreatment (Currie and Widom 2011). We contribute to this literature by identifying adolescent depressive symptoms as a mediator of the association between childhood maltreatment and adult SES. More importantly, this mediated pathway showed that childhood maltreatment not only affected adult SES, but influenced offspring birth weight via adult SES.
The findings should be interpreted in light of several limitations. First, we relied upon mothers’ reports of birth weight, without verification from clinical records. It has been shown, however, that use of maternal recollection of offspring birth weight is a valid method of obtaining data when clinical verification is unavailable (Tomeo et al. 1990). Second, we used retrospective reports of early life maltreatment, which have been shown to result in high false-negative rates (Hardt and Rutter 2004). Despite this potential limitation, retrospective assessment of childhood maltreatment has been shown to be a valid assessment method (Paivio 2001). Third, birth weight was not adjusted for gestational age and child sex. Nevertheless, findings from the present study are consistent with findings from a previous study that included adjusted birth weight (Gavin et al. 2011), suggesting that maternal childhood SES and childhood maltreatment are important early life risk factors for offspring birth weight despite the method used to assess birth weight.
Our findings suggest that a mother’s economic position in childhood and her experience of maltreatment during childhood has implications for her children born in the next generation. According to Lu and Halfon (2003), the life course perspective, provides a longitudinal assessment of the interplay of biological, psychological, and social factors in producing adverse birth outcomes. The authors suggest that from a life course perspective childhood SES and preconceptional health behaviors are important determinants of offspring birth outcomes as SES and health behaviors during pregnancy (Lu and Halfon 2003). We contribute to this existing literature by showing that childhood maltreatment is also a determinant of offspring birth weight and identifying potential mechanism by which childhood maltreatment and childhood SES affect offspring birth weight (Gavin et al. 2011).
The present study findings highlight the need to identify early life risk exposures that may affect a woman’s ability to deliver a normal weight infant. Based on the current findings, we propose four strategies to guide the design of intervention strategies to address the role of early life risks on offspring birth weight. First, research is needed to explore how existing prevention strategies designed to address adolescent substance use may affect perinatal outcomes in early adulthood. Respondents involved in effective interventions that reduced adolescent substance use should be followed up to determine whether perinatal risks in early adulthood were likewise reduced. Second, under American College of Obstetricians and Gynecologists (ACOG) guidelines, providers are encouraged to screen for psychosocial risk factors (e.g., nutrition, substance use, depression) during the perinatal period as a part of comprehensive care (ACOG 2006). Given this screening protocol, women seeking perinatal care services should also be screened for childhood maltreatment. Providers should discuss these childhood experiences with women to identify areas of concern in an effort to determine whether further evaluation and referrals are necessary. Third, also needed are systematic screening for child maltreatment, depression, and substance use among adolescent females in pediatric primary care settings coupled with responsive systems of care to confirm diagnosis and intervene with evidence-based therapies (Williams et al. 2009). Finally, women’s prenatal health care must incorporate a life course perspective, taking into consideration women’s health status during childhood and adolescence. Infant birth weight is related to the mother’s health and well-being; until all women across the life course are provided with high-quality health and mental health care, we will continue to see disparities in child health at birth.
References
Aarnoudse-Moens, C., Weisglas-Kuperus, N., van Goudoever, J., & Oosterlaan, J. (2009). Meta-analysis of neurobehavioral outcomes in very preterm and/or very low birth weight children. Pediatrics, 124, 717–28.
American College of Obstetricians and Gynecologists. (2006). Psychosocial risk factors: Perinatal screening and intervention. ACOG Committee Opinion No. 343. Obstetrics and Gynecology, 108, 469–477.
Anda, R., Felitti, V., Bremner, J., Walker, J., Whitfield, C., Perry, B., et al. (2006). The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience, 256, 174–186.
Anderson, N., & Armstead, C. (1995). Toward understanding the association of socioeconomic status and health: A new challenge for the biopsychosocial approach. Psychosomatic Medicine, 57, 213–225.
Anderson, M., Simonsen, U., Uldbjerg, N., Aalkjaer, C., & Stender, S. (2009). Smoking cessation early in pregnancy and birth weight, length, head circumference, and endothelial nitric oxide synthase activity in umbilical and chorionic vessels. Circulation, 119, 857–864.
Astone, N., Misra, D., & Lynch, C. (2007). The effect of maternal socio-economic status throughout the lifespan on infant birthweight. Paediatric and Perinatal Epidemiology, 21, 310–318.
Atrash, H., Johnson, K., Adams, M., Cordero, J., & Howse, J. (2006). Preconception care for improving perinatal outcomes: The time to act. Journal of Maternal and Child Health, 10, 3–11.
Baird, D. (1974). The epidemiology of low birth weight: Changes in the incidence in Aberdeen, 1948–72. Journal of Biosocial Science, 6, 323–341.
Barker, D., Eriksson, J., Forsen, T., & Osmond, C. (2002). Fetal origins of adult disease: Strength of effects and biological basis. International Journal of Epidemiology, 31, 1235–1239.
Bearman, P., Jones, J., & Udry, J. (1997) The National Longitudinal Study of Adolescent Health: Research Design [WWW document]. URL: http://www.cpc.unc.edu/projects/addhealth/design.html.
Braveman, P., & Barclay, C. (2009). Health disparities beginning in childhood: A life-course perspective. Pediatrics, 124, S163–S175.
Brown, D., Anda, R., Tiemeier, H., Felitti, V., Edwards, V., Croft, J., et al. (2009). Adverse childhood experiences and the risk of premature mortality. American Journal of Preventive Medicine, 37, 389–396.
Chantala, K. M., Kalsbeek, W. D., & Andraca, E. (2003). Non-response in Wave III of the Add Health study. Retrieved from http://www.cpc.unc.edu/projects/addhealth/pubs/guides. Accessed June 10, 2010.
Chapman, D., Whitfield, C., Felitti, V., Dube, S., Edwards, V., & Anda, R. (2004). Adverse childhood experiences and the risk of depressive disorders in adulthood. Journal of Affective Disorders, 82, 217–225.
Collins, J., David, R., Prachand, N., & Pierce, M. (2003). Low birth weight across generations. Journal of Maternal and Child Health, 7, 229–237.
Cummings, J., Ponce, N., & Mays, V. (2010). Comparing racial/ethnic differences in mental health service use among high-need subpopulations across clinical and school-based settings. Journal of Adolescent Health, 46, 603–606.
Currie, J., & Widom, C. S. (2011). Long-term consequences of child abuse and neglect on adult economic well-being. Child Maltreatment, 15, 111–120.
Donahue, S., Kleinman, K., Gillman, M., & Oken, E. (2010). Trends in birth weight and gestational length among singleton term births in the United States 1990–2005. Obstetrics and Gynecology, 115, 357–364.
Dube, S., Anda, R., Felitti, V., Edwards, V., & Croft, B. (2002). Adverse childhood experiences and personal alcohol abuse as an adult. Addictive Behaviors, 27, 713–725.
Dube, S., Miller, J., Brown, D., Giles, W., Felitti, V., Dong, M., et al. (2006). Adverse childhood experiences and the association with ever using alcohol and initiating alcohol use during adolescence. Journal of Adolescent Health, 38, e1–e10.
Emanuel, I. (1986). Maternal health during childhood and later reproductive performance. Annals of the New York Academy of Sciences, 477, 27–38.
Engle, W., & Kominiarek, M. (2008). Late preterm infants, early term infants and timing of elective deliveries. Clinics in Perinatology, 35, 325–341.
Finer, L., & Henshaw, S. (2006). Disparities in rates of unintended pregnancy in the United States, 1994 and 2001. Perspectives on Sexual and Reproductive Health, 38, 90–96.
Finkelhor, D., & Dzuiba-Letherman, J. (1994). Children as victims of violence: A national survey. Pediatrics, 94, 413–420.
Fletcher, J. (2009). Childhood mistreatment and adolescent and young adult depression. Social Science & Medicine, 68, 799–806.
Gamborg, M., Byberg, L., Rasmussen, F., Andersen, P., Baker, J., Bengtsson, C., et al. (2007). Birth weight and systolic blood pressure in adolescence and adulthood: Meta-regression analysis of sex- and age-specific result from 20 Nordic studies. American Journal of Epidemiology, 166, 634–645.
Gavin, A., Hill, K., Hawkins, J., & Maas, C. (2011). The role of maternal early-life and later-life risk factors on offspring low birth weight: Findings from a three-generational study. Journal of Adolescent Health, 49, 166–171.
Gilman, S., Kawachi, I., Fitzmaurice, G., & Buka, S. (2002). Socioeconomic status in childhood and the lifetime risk of major depression. International Journal of Epidemiology, 31, 359–367.
Gisselmann, M. (2006). The influence of maternal childhood and adulthood social class on health of the infant. Social Science & Medicine, 63, 1023–1033.
Goodman, A., Joyce, R., & Smith, J. P. (2011). The long shadow cast by childhood physical and mental problems on adult life. Proceedings of the National Academy of Science, 108, 6032–6037.
Grote, N., Bridge, J., Gavin, A., et al. (2010). A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Archives of General Psychiatry, 67, 1012–1024.
Gyllstrom, M., Hellerstedt, W. L., & McGovern, P. (2010). Independent and interactive associations of prenatal mood and substance use with infant birth outcomes. Journal of Maternal and Child Health, 15, 198–204.
Hamilton B., Martin J., Ventura S., (2010). Births: Preliminary data for 2009. National vital statistics reports; volume 59 no. 3. Hyattsville, MD: National Center for Vital Statistics.
Hardt, J., & Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal Child Psychology and Psychiatry, 45, 260–273.
Harris, K. M., Cheng, M. M. (2007). Dating major life events using an CAPI/CASI event history calendar in Add Health. Retrieved from http://psidonline.isr.umich.edu/Publications/Workshops/ehc-07papers/Add%20Health%20EHC%20Census%20paper%20Dec07.pdf.
Harris, K. M., Perreira, K., & Lee, D. (2009). Obesity in the transition to adulthood: Predictions across race/ethnicity, immigrant generation, and sex. Archives of Pediatric and Adolescent Medicine, 163, 1022–1028.
Harville, E., Boynton-Jarrett, R., Power, C., & Hypponen, E. (2010). Childhood hardship, maternal smoking, and birth outcomes: A prospective cohort study. Archives of Pediatric and Adolescent Medicine, 164, 533–539.
Heim, C., Newport, D., Heit, S., Graham, Y., Wilcox, M., Bonsall, R., et al. (2000). Pituitary-adrenal and autonomic responses to stress in women after sexual and physical abuse in childhood. Journal of the American Medical Association, 284, 592–597.
Humensky, J. (2010). Are adolescents with high socioeconomic status more likely to engage in alcohol and illicit drug use in early adulthood? Substance Abuse Treatment, Prevention, and Public, 5, 19.
Hussey, J., Chang, J., & Kotch, J. (2006). Child maltreatment in the United States: Prevalence, risk factors, and adolescent health consequences. Pediatrics, 118, 933–942.
Hypponen, E., Power, C., & Davey Smith, G. (2004). Parental growth at different life stages and offspring birthweight: An intergenerational cohort study. Paediatric and Perinatal Epidemiology, 18, 168–177.
Illsely, R. (1955). Social class selection and class differences in relation to stillbirths and infant deaths. British Medical Journal, 2, 1520–1524.
Jessor, R., Costa, F., Krueger, P., & Turbin, M. (2006). A developmental study of heavy episodic drinking among college students: The role of psychosocial and behavioral protective and risk factors. Journal of Studies on Alcohol, 67, 86–94.
Kahn, R. S., Wise, P. H., Kennedy, B. P., & Kawachi, I. (2000). State income inequality, household income, and maternal mental and physical health: Cross sectional national survey. British Medical Journal, 321, 1311–1315.
Kline, R. (2011). Principles and practice of structural equation modeling. New York: Guilford.
Lansford, J., Dodge, K., Pettit, G., & Bates, J. (2009). Does physical abuse in early childhood predict substance use in adolescence and early adulthood? Child Maltreatment, 15, 190–194.
Lu, M. C., & Halfon, N. (2003). Racial and ethnic disparities in birth outcomes: A life-course perspective. Maternal and Child Health Journal, 7, 13–30.
Lu, M., Kotelchuck, M., Culhane, J., Hobel, C., Klerman, L., & Thorp, J. (2006). Preconception care between pregnancies: The content of internatal care. Journal of Maternal and Child Health, 16, 107–22.
Luo, Y., & Waite, L. (2005). The impact of childhood and adult SES on physical, mental, and cognitive well-being in later life. Journal of Gerontology: Social Sciences, 60B, S93–S101.
Lynch, J., & Smith, G. (2005). A life course approach to chronic disease epidemiology. Annual Review of Public Health, 26, 1–35.
Martin, B., McCoy, T., Champion, H., Parries, M., DuRant, R., Mitra, A., et al. (2009). The role of monthly spending money in college student drinking behaviors and their consequences. Journal of American College Health, 57, 587–596.
Melchior, M., Moffitt, T., Milne, B., Poulton, R., & Caspi, A. (2007). Why do children for socioeconomically disadvantaged families suffer from poor health when they reach adulthood? A life course study. American Journal of Epidemiology, 166, 966–974.
Mueller, C. (2009). Protective factors as barriers to depression in gifted and non-gifted adolescents. Gifted Child Quarterly, 53, 3–14.
Muthén, L., & Muthén, B. (1998–2007). Mplus User’s Guide. Fifth Edition. Los Angeles, CA: Muthén & Muthén.
Nepomnyaschy, L. (2009). Socioeconomic gradients in infant health across race and ethnicity. Maternal and Child Health Journal, 13, 720–731.
Oesterle, S., Hill, K., Hawkins, J., Guo, J., Catalano, R., & Abbott, R. (2004). Adolescent heavy episodic drinking trajectories and health in young adulthood. Journal of Studies on Alcohol, 65, 204–212.
Oken, E., & Gillman, M. (2003). Fetal origins of obesity. Obesity Research, 11, 496–506.
Paivio, S. (2001). Stability of retrospective self-reports of child abuse and neglect before and after therapy for child abuse issues. Child Abuse & Neglect, 25, 1053–68.
Radloff, L. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 384–401.
Rich-Edwards, J., Kleinman, K., Michels, K., Stampfer, M., Manson, J., Rexrode, K., et al. (2005). Longitudinal study of birth weight and adult body mass index in predicting risk of coronary heart disease and stroke in women. British Medical Journal. doi:10.1136/bmj.38434.629630.E0.
Sareen, J., Afifi, T., McMillan, K., & Asmundson, G. (2011). Relationship between household income and mental disorders: Findings from a population-based longitudinal study. Archives of General Psychiatry, 68, 419–427.
StataCorp. (2007). Stata statistical software: Release 10. College Station, TX: StataCorp LP.
Stein, A., & Lumey, L. (2000). The relationship between maternal and offspring birth weights after maternal prenatal famine exposure: The Dutch Famine Cohort Study. Human Biology, 72, 641–654.
Straus M., Kinard E., & Williams L. (2004). The multidimensional neglectful behavior scale, form A: Adolescent and adult-recall version. Durham, NH: University of New Hampshire, Family Research Laboratory. Retrieved from http://pubpages.unh.edu/mas2/NS1G.pdf.
Tomeo, C., Rich-Edwards, J., Michels, K., Berkey, C., Hunter, D., Frazier, A., et al. (1990). Reproductively and validity of maternal recall of pregnancy-related events. Epidemiology, 10, 774–777.
Topitzes, J., Mersky, J., & Reynolds, A. (2009). Child maltreatment and adult cigarette smoking: A long-term developmental model. Journal of Pediatric Psychology, 35, 484–498.
van der Kolk, B., Perry, C., & Herman, J. (1991). Childhood origins of self-destructive behavior. The American Journal of Psychiatry, 148, 1665–1671.
Warren, J. (2009). Socioeconomic status and health across the life course: A test of the social causation and health selection hypotheses. Social Forces, 87, 2125–2153.
Whincup, P., Kaye, S., & Owen, C. (2008). Birth weight and risk of type 2 diabetes: A systematic review. Journal of the American Medical Association, 300, 2886–2897.
Widom, C., Marmorstein, N., & White, H. (2006). Childhood victimization and illicit drug use in middle adulthood. Psychology of Addictive Behaviors, 20, 394–403.
Williams, C., & Sutcliffe, A. (2009). Infant outcomes of assisted reproduction. Early Human Development, 85, 673–677.
Williams, S., O’Connor, E., Eder, M., & Whitlock, E. (2009). Screening for child and adolescent depression in primary care settings: A systematic evidence review for the US Preventive Services Task Force. Pediatrics, 123, 716–735.
Wilson, H., & Widom, C. (2009). A prospective examination of the path from child abuse and neglect to illicit drug use in middle adulthood: The potential mediating role of four risk factors. Journal of Youth and Adolescence, 38, 340–354.
Zielinski, D. (2009). Child maltreatment and adult socioeconomic well-being. Child Abuse & Neglect, 33, 666–678.
Acknowledgements
This publication was made possible by Grant Number 1KL2RR025015-01 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH) and NIH Roadmap for Medical Research. This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis. We would like to thank the anonymous reviewers for their comments on earlier drafts.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gavin, A.R., Thompson, E., Rue, T. et al. Maternal Early Life Risk Factors for Offspring Birth Weight: Findings from the Add Health Study. Prev Sci 13, 162–172 (2012). https://doi.org/10.1007/s11121-011-0253-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-011-0253-2