
Abstract
This study developed and tested an Internet-based gender-specific drug abuse prevention program for adolescent girls. A sample of seventh, eighth, and ninth grade girls (N = 236) from 42 states and 4 Canadian provinces were randomly assigned to an intervention or control group. All girls completed an online pretest battery. Following pretest, intervention girls interacted with a 12-session, Internet-based gender-specific drug prevention program. Girls in both groups completed the measurement battery at posttest and 6-month follow-up. Analysis of posttest scores revealed no differences between groups for 30-day reports of alcohol, marijuana, poly drug use, or total substance use (alcohol and drugs). At 6-month follow-up, between-group effects were found on measures of 30-day alcohol use, marijuana use, poly drug use, and total substance use. Relative to girls in the control group, girls exposed to the Internet-based intervention reported lower rates of use for these substances. Moreover, girls receiving the intervention achieved gains over girls in the control group on normative beliefs and self-efficacy at posttest and 6-month follow-up, respectively.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Current trends in prevalence data indicate that the gender gap in substance use continues to shrink among adolescents (Johnston et al. 2007). Among eighth graders, past-year illicit drug use was nearly equal for males and females (National Institute on Drug Abuse 2006). In certain instances, girls’ substance use exceeds their male counterparts. Girls’ use of inhalants, amphetamines, methamphetamine, tranquilizers, Rohypnol, and cigarettes exceeds boys’ use (Wallace et al. 2003). Relative to similarly-aged males, eighth grade girls have higher rates of 30-day alcohol use, binge drinking, and drunkenness (Johnston et al. 2006).
Adolescent girls’ use of flavored alcoholic beverages (alcopops or malternatives) also eclipses that of their male counterparts (Johnston et al. 2005). This is not surprising given that girls’ exposure to these particular alcoholic advertisements increased by 216% from 2001 to 2002, while boys’ exposure increased 46% (Jernigan et al. 2004). Males, however, consume more beer, binge drink beer, and experience more alcohol-related problems (Werch et al. 2006). The social normalization of female alcohol and drug use, increased attention girls receive from advertising, and differential drinking patterns exhibited by girls and boys necessitate prevention programming designed expressly for girls.
A dramatic increase in substance use occurs as girls transition from middle to high school. Rates of past-year drug use among girls in 8th and 12th grade are 16%, 29%, and 34.5%, respectively (Johnston et al. 2006). Marijuana use more than doubles during this same period. Whereas 11% of girls report using marijuana in 8th grade, 30% report use by 12th grade (Johnston et al. 2006). Patterns for past-month alcohol use are similar with 20% of girls drinking in 8th grade and 43% of girls drinking by 12th grade (Johnston et al. 2006 ). These trends in substance use initiation indicate that the transition from middle to high school is optimal for delivering prevention programming.
That female rates of substance use match or exceed male rates and more than double from middle school to high school is alarming. Research suggests that, relative to males, females are at greater risk for addiction once drug use begins and that their transition period from initiation to problem use is shorter (Ridenour et al. 2006). Drug and alcohol use also place girls at risk sexually. The relationship between teen substance use and risky sexual behaviors is well established (Graves and Leigh 1995; Valois et al. 1999). As drinking and drug use increase, so too do the odds of engaging in unintended and unprotected sexual intercourse (Naimi et al. 2003; Poulin and Graham 2001).
Few studies on the outcomes of gender-specific substance abuse prevention programs exist. A review of substance abuse prevention programs for adolescent females noted only four such programs in a literature search encompassing the years 1980–2000 (Blake et al. 2001). One program was largely ineffective and possibly counterproductive relative to substance use outcomes. Effects of the remaining three programs were promising, resulting in lower reported rates of alcohol and substance use among girls who received the interventions compared to girls in the control groups. More recently, a program for adolescent girls involved with team sports aimed to prevent drug use and eating disorders (Elliot et al. 2002). Relative to those in the control group, girls who received the program increased their knowledge of substance use, decreased their drug use, and increased their intentions not to use drugs and cigarettes. The present study builds off a pilot test of a gender-specific, CD-ROM intervention to prevent substance use among adolescent females (Schinke and Schwinn 2005).
Toward advancing the science of substance abuse prevention in general, and of gender-specific programming in particular, this study recruited participants and delivered measures and intervention entirely through the Internet. Presently, most evidence-based prevention programming, across such domains as substance use, mental health, and HIV/AIDS is delivered in live group settings (teacher, counselor, coach, etc., leads a group of youths through content; Rotheram-Borus 2000). With the widespread use of the Internet as a communication device, researchers may be missing a unique and teen-friendly modality for imparting skills to youth. In addition to simply appealing to and engaging youths, computer-based interventions are portable, cost effective, easy to use, and allow for interactivity, data storage and retrieval, and fidelity implementation. Compared to live group delivery, Internet-based interventions lend themselves to custom tailoring for population segments and are easily disseminated.
Computer programming allows youths to access content and navigate sessions at their own pace and complete games and skills-building exercises to reinforce content through the use of such media elements as quality graphics, appropriately placed and brief text, movie clips, audio tracks, chat forums, blogs, and animation. Because youths often interact with computers in individual or small group formats, computers are ideal for presenting information on and exploring sensitive topics. Teens frequently use the Internet to access personal health-related content (Borzekowski and Rickert 2001), and they are comfortable disclosing behavioral data to a computer (Rhodes et al. 2003). Finally, computer-based interventions minimize variations in implementation. Empirically-tested and theory-driven programs delivered via the Internet or CD-ROM ensure that all participants receive identical content.
Computer-based interventions have been found effective among youths for substance abuse prevention (Schinke et al. 1994, 2004, 2006), health promotion (Bosworth et al. 1994), smoking cessation (Pallonen et al. 1998), HIV prevention among females (Di Noia et al. 2004), physical activity (Haerens et al. 2007), and depression (DeMaso et al. 2006). Controlled studies of gender-specific interventions to prevent substance use among girls, however, are absent. Based on Social Learning Theory (Bandura 1977) and employing a social competence and skills building strategy (Botvin et al. 1994), we investigated the efficacy of a gender-specific, Internet-based intervention for adolescent girls.
Method
Participants
Study participants were 236 girls from 42 states and 4 Canadian provinces. Girls were recruited through the youth-oriented website, Kiwibox.com™. A solicitation e-mail was sent from Kiwibox.com to 13- and 14-year-old girls who were registered users of the website. Interested girls were asked to submit an electronic form complete with their and their parents’ name and address. An information packet was mailed to the parents of approximately 450 girls who submitted the electronic form within one week of the solicitation e-mail.
The information packet included: (a) letter to parents describing the nature of the study and risks and benefits; (b) two-page fact sheet answering such questions as “Who is responsible for this study?” “Why did my daughter receive this invitation to participate?” “What will be required of my daughter if she participates?” “What kind of questions will my daughter be asked?” and “What kind of information will my daughter receive if she is also randomly selected to interact with the 12 Internet-based sessions?” (c) investigators’ contact information including a toll-free number for parents and girls who desired more information; (d) youth assent form and parental permission form; and (e) self-addressed, stamped envelope to return the forms. To verify parental consent, we contacted parents by telephone to confirm their daughters’ participation. We also visually inspected the daughter’s signature on the assent form and the parent’s signature on the permission form. In one instance, daughter and parent signatures were suspiciously similar and the girl was not enrolled in the study.
Design and Procedures
After study enrollment, girls were randomly assigned to the intervention or control arm. All girls completed online pretest measures via the study’s secure, password protected website. Girls received notification by regular mail alerting them to complete pretest by logging onto our website with a unique ID number. During the initial login, girls were required to establish their own username and password for future access to the measures and, in the case of the intervention group, to the prevention program.
After completing online pretest measures, intervention girls were immediately directed to the first program session. Control girls were thanked for their time and reminded that they would be notified when the next survey was available. Immediately following completion of the last program module, girls in the intervention group completed posttest. Control girls were asked to posttest 6 weeks after pretest (the time estimated for intervention girls to complete the program). Girls from both study groups completed follow-up measures 6 months after posttest. We sent postcards and e-mails and made telephone calls to notify and remind girls about posttest and 6-month follow-up measures. Girls received $20 for completing pretest and posttest and $30 for completing the 6-month follow-up.
Measures
At all three measurement occasions, girls were asked to respond to items about demographic characteristics, substance use, and mediators of substance use targeted in the intervention. The mediating variables assessed are regarded in the prevention literature to be strongly associated with substance use (Hansen 1992). The scales for normative beliefs; decision making, goal setting, and drug resistance skills; stress management; social skills; self-esteem (Fearnow-Kenney et al. 2002; Hansen, and McNeal 2001); and body-esteem (Mendelson et al. 1998) have been used in prior studies with youth of the same age and ethnic-racial make-up as our sample. The four-item scale for self-efficacy was created for this study and relates specifically to girls’ perceived ability to resist pressure from a boyfriend (or a boy one likes) to use substances. Unless otherwise noted, internal consistency scores provided are from present study data.
Demographic questions asked girls their age, grade in school, race/ethnicity, average letter grade in school, who they live with most of the time, and what type of school they attend (public, private-religious, private-not religious).
Substance use items, adapted from the CDC’s Youth Risk Behavior Survey (YRBS; Centers for Disease Control and Prevention 2005), asked girls to report how many times in the past month and week they used alcohol, cigarettes, marijuana, cocaine, inhalants, methamphetamines, and ecstasy. Response options ranged from “0 times” to “40 or more times.” Test–retest reliability for YRBS items is 0.82 to 0.95 (Centers for Disease Control and Prevention 2004)
Normative beliefs were assessed with ten items using a 4-point Likert scale and summed to form an index (α = 0.89). Girls were asked to report their perceptions of alcohol and drug use among their closest friends and school peers, and the acceptability of using substances among their friends. Example questions are “How many of your closest friends do you think have been drunk during the past 30 days?” and “What would your best friends think if you smoked cigarettes?”
Decision making skills were measured with a four-item scale, summed to form an index (α = 0.66). Items assessed the degree to which girls considered their options when faced with a difficult decision and the consequences of selecting one option over another. An illustrative item is,”How often do you stop and think about how your decisions may affect others’ feelings?” Response options ranged from “Never” (1) to “All the time” (4).
Goal-setting skills measured the degree to which girls set current and future goals and the extent to which they thought about how to achieve those goals (Never = 1; All the time = 4). Three items were summed to form an index (α = 0.69).
Drug resistance/refusal skills were measured with two items that assessed the ease with which girls felt they could refuse an offer to use drugs from a best friend (α = 0.84). An illustrative item is “Pretend your best friend offered you marijuana and you did not want it. How hard would it be for you to refuse the offer?” Response options ranged from “Very easy” (1) to “Very hard” (4).
Stress-management questions, using a 4-point Likert scale, assessed girls’ perceived ability to manage stress. Sample items are, “I handle stress well” and “Stressful situations are hard for me to deal with.” Three items were summed to derive a total stress-management score (α = 0.67).
Social skills measured the girls’ ability to make friends with female and male peers, assert themselves with friends, and get along with others. Five 4-point Likert-scaled items (e.g., “It is easy for me to make new friends.”) comprised the scale (α = 0.77).
Self-esteem questions were four 5-point Likert-scaled items (α = 0.85) summed to form a self-esteem index; lower scores indicate higher self-esteem. Illustrative questions include, “I like myself for who I am,” “I am proud of myself,” and “I have qualities that make me special.”
Body-esteem questions, derived from the Body-Esteem Scale, were four 5-point Likert-scaled items (α = 0.74) summed to form an index of girls’ self-evaluation of their appearance. Illustrative questions include, “I wish I looked better,” and “I am satisfied with how much I weigh.”
Self-efficacy as it relates to resisting pressure from a boyfriend (or a boy one likes) to use substances was measured with four questions. The 4-point Likert-scaled items were created for this study (α = 0.68). An illustrative item is “If your boyfriend, or a boy you really liked, wanted you to drink a beer, would you?”
Intervention
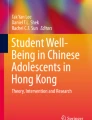
Immediately following completion of the online pretest, girls in the intervention group were routed to the program, RealTeen, via a secured website. The site was comprised of two components: the homepage and 12 intervention sessions. The homepage features, available for access anytime, included news feeds, horoscopes, beauty tips, quotes of the day, fortunes, and access to their blog, pen pal, and the chat forum girls used optionally as a response to intervention session questions. Figure 1 illustrates how girls interacted with the website.

Schematic of intervention delivery
Content for RealTeen sessions drew on earlier skills-based prevention research (Schinke et al. 2004). The sessions incorporated not only general personal and social skills (self-efficacy, communication, asserting one’s self), but also skills specific to dealing with drug use opportunities (Nation et al. 2003). Girls sequentially completed nine theory-based sessions on: goal setting, decision making, coping (particularly with stress, puberty, and bodily changes), self-esteem, assertion, communication, media influences, peer pressure, and drug facts. The first session served as an introduction; the final two sessions reviewed material and provided additional quizzes.
In session 1, girls personalized their home page, created a personal profile for others to learn about them, reviewed the site’s features and intervention sessions, and were assigned a pen pal who was another study participant. Within each session, steps were taken to increase interactivity and peer-to-peer communication—a component of effective prevention programs (Nation et al. 2003). When girls were required to respond to a question or describe a personal experience their response could be (1) posted to their blog for other participants to see should they access that blog, (2) sent to their pen-pal, (3) posted to the public chat forum and visible to the entire group, or (4) posted to their own diary and kept private.
Across sessions, an older female animated character guided girls through the content and practice exercises. For instance, in the goal-setting session, girls received a brief lesson on the benefits of setting goals, including the difference between short- and long-term goals, how goal-setting can be used, and steps to achieving a personal goal. To provide a context for the information on goal setting, girls were asked to think about how they imagined their life would look when they were a young adult (geographic location, employment, education, relationships, etc). At the end of the session, girls were asked to type onto the screen one short-term goal and one-long term goal, and two steps required for achieving each goal. As with all the exercises necessitating a response, girls’ dictated how and whether their answer was disseminated to the larger group.
Research staff monitored public posts and administrative access allowed for removal of off-topic or inappropriate posts. Additionally, an application screened for profanity and routed questionable responses to research staff for approval before posting to the website. Sessions required approximately 25 min to complete and had to be finished in one sitting. Though instructed to complete two sessions per week, girls were not prohibited from completing more than one session per sitting. Girls received “points” for each session completed. The points could be saved up and used to purchase such items as nail polish, lip gloss, stickers, and similar trinkets online. Girls in the control group completed measures at designated intervals but did not receive the gender-specific drug abuse prevention program.
Data Analysis
Data were analyzed using SPSS 14.0 including procedures for independent t tests, chi-square tests, general linear models (GLM) analysis of covariance (ANCOVA), GLM repeated measures ANOVA, and multiple regressions. After importing and coding the data, individual cases were identified for extreme and/or unreliable patterns of reported substance use across all three measurement occasions. Fifteen cases were removed from subsequent analyses. Independent t-tests and chi-square analyses were performed to confirm baseline comparability on demographic and outcome variables and to detect differential attrition between intervention and control groups.
Intervention effects at posttest and follow-up were determined through a series of GLM ANCOVAs, adjusting for pretest scores, length of time between pretest and posttest, age, and average letter grade in school. These additional covariates were included to increase the precision of estimates. Because drug use scores were small, seven dependent substance use variables for 30-day use were dichotomized and summed to form a 30-day total substance use measure. Alcohol was then removed from that dichotomized variable to produce a 30-day poly drug use measure. Thirty-day alcohol use was unchanged from its continuous variable form.
The effects of study group (factor 1) across time (factor 2) and the interaction between these two factors was assessed using GLM repeated measures ANOVA. Multiple regression analyses assessed the degree of fit between proposed intervention mediators and substance use at pretest. The effect size for 30-day alcohol, marijuana, poly drug, and total substance use was calculated using Cohen’s d (Cohen 1992; Thalheimer and Cook 2002).
Results
Sample
The demographic characteristics of our pretest study sample are presented in Table 1. Participants had an average age of 14 years; 60% were in ninth grade. The ethnic-racial composition of our sample was 60.6% White, 16.5% Black, 7.2% Latina, 6.8% Asian, and 8.9% Other. Girls’ average letter grade in school was between an “A” and “B,” almost 90% of the sample attended public school, and nearly 50% of the sample reported living with their mother and father.
Analyses of pretest data revealed that participants in the intervention and control groups were comparable on measured demographics, mediating variables, and substance use. Differential attrition was assessed across the three measurement occasions using the same variables analyzed in baseline equivalency. Pretest to posttest attrition was 6.8%; the attrition rates for girls in intervention and control groups did not differ, X 2 (1) = 1.74, p > 0.05. At final follow-up, attrition was 9%; again, rates did not differ by study group, X 2 (1) =0.84, p > 0.05.
Program Participation
All 12 sessions of the prevention program were completed by 92% (108) of the girls assigned to the intervention group. Three girls completed zero sessions and seven girls completed between 1 and 12 sessions. These 10 girls did not complete posttest or 6-month follow-up. Therefore, the level of participation, defined as completing all 12 sessions, for the effective sample is 100%. On average, girls completed the intervention in approximately 1 month, with 91% of the intervention girls completing the program in less than 2 months. Length of time between pretest and posttest did not correlate with measures of baseline substance use, nor did X 2 tests reveal an association between length of time (categorized as 1 day, 2 weeks, 4 weeks, 6 weeks, more than 6 weeks) and 6-month substance use rates. Still, we adjusted subsequent outcome analyses for time between pretest and posttest to increase precision and as a proxy for the level of involvement with the sessions.
Intervention participants could elect to post their responses to session questions privately or publically. On average, girls posted their responses to their private diary 50% of the time, followed by posting publically to their blog (29%), and posting publically to the chat room (21%). Approximately 30% of chat room postings consisted of non-substantive peer-to-peer feedback on answers to session questions (e.g., statements of affirmation and encouragement). Process data on date and time of session completion indicate that nearly all girls interacted with the program during weekdays between 3:00 p.m. and 1:00 a.m. or on weekends.
Substance Use
At posttest, no effects were found for measures of substance use, adjusting for pretest scores, length of time between pretest and posttest, age, and average letter grade in school. At 6-month follow up, intervention-arm girls reported less substance use, adjusting for the aforementioned covariates (Table 2). Compared to girls in the control group, girls who received intervention had lower 30-day rates of alcohol use, F(1, 190) = 4.00, p < 0.05; marijuana use, F(1, 189) = 5.92, p < 0.05; poly drug use, F(1, 189) = 6.85, p < 0.05; and total substance use, F(1, 189) = 7.70, p < 0.05. Past-month cigarette use did not differ between groups. Repeated measures ANOVA indicated significant group by time interactions for 30-day alcohol use, F(2, 380) = 6.00, p < 0.05; marijuana use, F(2, 380) = 4.20; p < 0.05; poly drug use, F(2, 378) = 7.72, p < 0.05; and total substance use F(2, 378) = 5.21, p < 0.05. Figure 2 shows adjusted mean scores for 30-day total substance use at all three time points by arm. Estimated effect sizes for 30-day alcohol, marijuana use, poly drug, and total substance use were 0.20, 0.20, 0.19, and 0.20, respectively, at 6-month follow-up.

Adjusted 30-day total substance use means, by group and measurement occasion. Means are adjusted controlling for length of time between pretest and posttest, age, and average letter grade in school. 30-day total substance use (R = 0–6) is a composite variable of dichotomized values for alcohol, cigarette, marijuana, cocaine, inhalant, methamphetamine, and ecstasy use
Mediating Variables
Pretest scores for the nine mediator variables were regressed onto baseline substance use scores. Normative beliefs (B = 0.04, p < 0.001) and self-efficacy (B = 0.07, p < 0.01) were significant predictors of total substance use. At posttest, girls in the intervention group reported fewer peers, close friends, and boyfriends who endorsed and used substances, controlling for pretest, length of time between pretest and posttest, age, and average letter grade in school, F(1, 195) = 4.43, p < 0.05. Differences in normative beliefs were not maintained at 6-month follow-up. Posttest scores for self-efficacy did not differ between groups. At 6-month follow-up, however, intervention-arm girls reported higher levels of self-efficacy than control-arm girls, using the aforementioned controls, F(1, 193) = 4.19, p < 0.05.
Discussion
Study findings support the efficacy of a female-specific, Internet-based substance abuse prevention program. The results lend credence to the use of the Internet as a means to recruit and maintain a study sample, collect data, and deliver a skills-based interactive intervention. Adolescent girls who participated in the online intervention reported decreased 30-day alcohol, marijuana, poly drug, and total substance use at 6-month follow-up. The absence of posttest effects may be an artifact of timing. Posttest measures were completed immediately after intervention delivery. The trajectory of decreased substance use between posttest and follow-up for intervention-arm girls and increased use among control-arm girls suggests that girls may require time and real-life opportunities to apply acquired skills.
Effect sizes from our intervention compare favorably to results achieved by similar programs. A meta-analysis of school-based prevention programs found that those involving interactive programming and emphasizing comprehensive life skills were most successful (Tobler and Stratton 1997). Among such programs, the average effect sizes for alcohol, marijuana, and illicit drugs was, 0.21, 0.14, and 0.17, respectively. Our study produced effect sizes for 30-day alcohol, marijuana use, and poly-drug use of 0.20, 0.20, and 0.19, respectively. An effect size of 0.20, albeit small (Cohen 1992), is a considerable improvement from that achieved by older, non-interactive, knowledge-based programs that reported effects ranging from 0.04–0.11 (Tobler and Stratton 1997).
Chief among study limitations is the generalizability of the sample. Though residing in 42 states and 4 Canadian provinces, girls were recruited from a single youth-oriented website. The enrollment procedures favored girls who were computer savvy and motivated. Additional evidence of high motivation comes from the sample’s overall high academic grades. During the study period, approximately 30% of North American homes had broadband Internet access (Horrigan 2008), whereas nearly all girls appear to have accessed our intervention program at home. Though homes with children have higher than average rates of Internet access, the Horrigan (2008) data indicate that a substantial number of North American children were still without access during our study period, likely owing to lower economic and rural conditions. Our findings are limited, therefore, to a subset of adolescent girls with intrinsic and extrinsic factors similar to the girls in our sample—particularly, girls who have reliable access to a private computer, regardless of economic or geographic conditions. By measuring self-efficacy in relation to boys one likes or boyfriends, and with intervention content similarly geared toward heterosexual girls, the study findings may be further limited in their generalizaby. Furthermore, although our Internet-based intervention ensured that all girls received identical material, the extent to which girls interacted with different aspects of the intervention program (pen-pal, chat rooms, blogs) and with the larger website itself (news feeds, horoscopes, beauty tips) is unknown. As such, we could not control for variation in levels of participation or conduct principal component analyses.
Despite these limitations, the study used a novel approach to recruit and deliver gender-specific prevention programming. All subjects were recruited via the Internet, and all 12 sessions of the social competence and skills building content were delivered online. The program yielded differences in substance use behavior comparable to labor-intensive and costly live-group, school-based programs. Decreased substance use among girls was achieved without the need for staff training, detractions from valuable classroom learning time, or concerns regarding implementation fidelity. Attrition across both groups was less than 10%.
Perhaps this study will serve as a launching point for prevention science to capitalize on the facility of computer technology to tailor and deliver targeted substance abuse prevention programming. Our program lends itself to home, rather than public, delivery where ease of access and privacy are more assured. The program could, however, be accessed at community-based agencies, schools, and libraries that have private computer terminals. Computer programming allows investigators the freedom to tailor interventions for multiple populations and settings. Future research should also exploit the limitless capacity of the Internet to collect fidelity data. Finally, studies with additional follow-up measures are required to assess the sustainability of Internet-based program effects.
References
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavior change. Psychological Review, 84, 191–215.
Blake, S. M., Amaro, H., Schwartz, P. M., & Flinchbaugh, L. J. (2001). A review of substance abuse prevention programs for young adolescent girls. Journal of Early Adolescence, 21, 294–324.
Borzekowski, D. L. G., & Rickert, V. I. (2001). Adolescents, the internet, and health issues of access and content. Applied Developmental Psychology, 22, 49–59.
Bosworth, K., Gustafson, D. H., & Hawkins, R. P. (1994). The BARN System: Use and impact of adolescent health promotion via computer. Computers in Human Behavior, 10, 467–482.
Botvin, G. J., Schinke, S. P., Epstein, J. A., Diaz, T., & Botvin, E. J. (1994). Effectiveness of culturally-focused and generic skills training approaches to alcohol and drug abuse prevention among minority youths. Psychology of Addictive Behaviors, 8, 116–127.
Centers for Disease Control and Prevention. (2004). Methodology of the youth risk behavior surveillance system. Morbidity and Mortality Weekly Report, 53(RR12), 1–13. Retrieved February 20, 2009, from http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5312a1.htm.
Centers for Disease Control and Prevention. (2005). Youth Risk Behavior Survey. Retrieved February 20, 2009, from http://www.cdc.gov/healthyyouth/yrbs/.
Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155–159.
DeMaso, D. R., Marcus, N. E., Kinnamon, C., & Gonzalez-Heydrich, J. (2006). Depression experience journal: A computer-based intervention for families facing childhood depression. Journal of the American Academy of Child & Adolescent Psychiatry, 45, 158–165.
Di Noia, J., Schinke, S. P., Pena, J. B., & Schwinn, T. M. (2004). Evaluation of a brief computer-mediated intervention to reduce HIV risk among early adolescent females. Journal of Adolescent Health, 35, 62–64.
Elliot, D. L., Goldberg, L., Moe, E., Duncan, T., DeFrancesco, C., & Durham, M. (2002). ATHENA: Deterring drug use and disordered eating. Journal of Investigative Medicine, 50, 66A.
Fearnow-Kenney, M., Hansen, W. B., & McNeal Jr., R. B. (2002). Comparison of psychosocial influences on substance use in adolescents: implications for prevention programming. Journal of Child and Adolescent Substance Abuse, 11(4), 1–24.
Graves, K. L., & Leigh, B. L. (1995). The relationship of substance use to sexual activity among young adults in the United States. Family Planning Perspectives, 27, 18–33.
Hansen, W. B. (1992). School-based substance abuse prevention: A review of the state of the art in curriculum, 1908–1990. Health Education Research, 7, 403–430.
Hansen, W. B, & McNeal Jr., R. B (2001). Self-initiated cessation from substance use: A longitudinal study of the relationship between postulated mediators and quitting. Journal of Drug Issues, 31, 957–974.
Haerens, L., Deforche, B., Vandelanotte, C., Maes, L., & De Bourdeaudhuij, I. (2007). Acceptability, feasibility and effectiveness of a computer-tailored physical activity intervention in adolescents. Patient Education and Counseling, 66, 303–310.
Horrigan, J. B. (July 2008). Home broadband adoption 2008. Pew Internet & American Life Project. Retrieved February 17, 2009, from http://www.pewinternet.org/PPF/r/257/report_display.asp.
Jernigan, D. H., Ostroff, J., Ross, C., & O’Hara, J. A. (2004). Sex differences in adolescent exposure to alcohol advertising in magazines. Archives of Pediatrics & Adolescent Medicine, 158, 629–634.
Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2007). Monitoring the Future national results on adolescent drug use: Overview of key findings, 2006 (NIH Publication no. 07-6202). Bethesda, MD: National Institute on Drug Abuse.
Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2005). Monitoring the Future national survey results on drug use, 1975–2004: Volume I, Secondary school students (NIH Publication No. 05–5727). Bethesda, MD: National Institute on Drug Abuse.
Johnston, L. D., O'Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2006). Demographic subgroup trends for various licit and illicit drugs, 1975–2005. (Monitoring the Future Occasional Paper No. 63). Ann Arbor, MI: Institute for Social Research.
Mendelson, B. K., White, D. R., & Mendelson, M. J. (1998). Manual for the body esteem scale for adolescents and adults. Montréal: Concordia University.
Naimi, T. S., Lipscomb, L. E., Brewer, R. D., & Gilbert, B. C. (2003). Binge drinking in the preconception period and the risk of unintended pregnancy: Implications for women and their children. Pediatrics, 111, 1136–1141.
Nation, M., Crusto, C. A., Wandersman, A., Kumpfer, K. L., Seybolt, D., et al. (2003). What works in prevention: Principles of effective prevention programs. American Psychologist, 58, 449–456.
National Institute on Drug Abuse. (March 2006). NIDA INFO Facts. US Department of Health and Human Services. Retrieved February 20, 2009, from http://www.drugabuse.gov/pdf/infofacts/HSYouthTrends06.pdf.
Pallonen, U. E., Velicer, W. F., Prochaska, J. O., Rossi, J. S., Bellis, J. M., Tsoh, J. Y., et al. (1998). Computer-based smoking cessation interventions in adolescents: Description, feasibility and six month follow-up findings. Substance Abuse and Misuse, 33, 935–965.
Poulin, C., & Graham, L. (2001). The association between substance use, unplanned sexual intercourse and other sexual behaviours among adolescent students. Addiction, 96, 607–621.
Ridenour, T. A., Lanza, S. T., Donny, E. C., & Clark, D. B. (2006). Different lengths of times for progressions in adolescent substance involvement. Addictive Behaviors, 31, 962–983.
Rhodes, S. D., Bowie, D. A., & Hergenrather, K. C. (2003). Collecting behavioural data using the World Wide Web: Considerations for researchers. Journal of Epidemiology and Community Health, 57, 68–73.
Rotheram-Borus, M. J. (2000). Expanding the range of interventions to reduce HIV among adolescents. AIDS, 14, S33–S40.
Schinke, S. P., Di Noia, J., & Glassman, J. R. (2004). Computer-mediated intervention to prevent drug abuse and violence among high-risk youth. Addictive Behaviors, 29, 225–229.
Schinke, S. P., Moncher, M. S., & Singer, B. R. (1994). Native American youths and cancer risk reduction: Effects of software intervention. Journal of Adolescent Health, 15, 105–110.
Schinke, S. P., & Schwinn, T. M. (2005). Gender-specific computer-based intervention for preventing drug abuse among girls. American Journal of Drug and Alcohol Abuse, 31, 609–616.
Schinke, S. P., Schwinn, T. M., & Cole, K. (2006). Preventing alcohol abuse among early adolescents through family and computer-based interventions: Four-year outcomes and mediating variables. Journal of Developmental and Physical Disabilities, 18, 149–161.
Schinke, S. P., Schwinn, T. M., Di Noia, J., & Cole, K. C. (2004). Reducing the risks of alcohol use among urban youth: 3-year effects of a computer-based intervention with and without parent involvement. Journal of Studies on Alcohol, 65, 443–450.
Thalheimer, W., & Cook, S. (2002, August). How to calculate effect sizes from published research articles: A simplified methodology. Retrieved February 20, 2009, from http://work-learning.com/effect_sizes.htm.
Tobler, N. S., & Stratton, H. H. (1997). Effectiveness of school-based drug prevention programs: A meta-analysis of research. The Journal of Primary Prevention, 18, 71–128.
Valois, R. F., Oeltmann, J. E., Waller, J., & Hussey, J. R. (1999). Relationship between number of sexual intercourse partners and selected health risk behaviors among public high school adolescents. Journal of Adolescent Health, 25, 328–335.
Wallace, J. M., Bachman, J. G., O’Malley, P. M., Schutenberg, J. E., Cooper, S. M., & Johnston, L. D. (2003). Gender and ethnic differences in smoking, drinking and illicit drug use among American 8th, 10th, and 12th grade students, 1976–2000. Addiction, 8, 225–234.
Werch, C., Jobli, E. C., Moore, M. J., DiClemente, C. C., Dore, H. S., & Hendricks Brown, C. (2006). Do alcohol consumption patterns of adolescents differ by beverage type? Journal of Child and Adolescent Substance Abuse, 15, 45–62.
Acknowledgments
This research was supported by National Institute on Drug Abuse Grant DA13305. We also thank Berlin Productions, Inc. for their technical support of the RealTeen program.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by funding from Grant DA13305 from the National Institute on Drug Abuse.
Rights and permissions
About this article
Cite this article
Schwinn, T.M., Schinke, S.P. & Di Noia, J. Preventing Drug Abuse Among Adolescent Girls: Outcome Data from an Internet-Based Intervention. Prev Sci 11, 24–32 (2010). https://doi.org/10.1007/s11121-009-0146-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-009-0146-9