
Abstract
This study investigates an approach for reducing inhalant initiation among younger adolescents: altering Socio-Personal Expectations (SPEs), a term referring to perceived linkages between behavior and personally relevant social outcomes. The study focuses specifically on SPEs regarding outcomes associated with increased social status and popularity. An anti-inhalant message was embedded within a short anti-bullying education video. Young adolescents (N = 893) were assigned randomly to receive a message focused on the physical or the social harms of inhalant use. The objectives of this study were to test: (1) the malleability of SPEs, (2) SPEs’ predictive validity for future inhalant use, and (3) whether being exposed to a socio-personal threat, rather than a physical threat, led to different variables affecting drug-relevant decision-making processes. Analysis of variance suggested the malleability of SPEs (p < .001). Multiple regression analysis revealed that SPEs were predictive of future inhalant use. SPEs accounted for a significant portion of variance in future intentions over and above demographic variables, prior use, psychosocial variables, and perceived physical harm (R 2 = .26, p < .01). Moreover, being exposed to a social, rather than a physical threat, message resulted in different variables being predictive of future intentions to use inhalants.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Use of volatile chemical substances that produce vapors that are inhaled to achieve mind-altering effects is dangerous and potentially fatal (National Institute on Drug Abuse [NIDA] 2005). Common inhalant substances are solvents, aerosols, gases and nitrites (NIDA 2005). They can be obtained from butane lighters, paint solvents, some glues, gasoline, and other everyday products. A rapid high may be achieved when these vapors are inhaled, often resulting in physical and mental changes (dizziness, increased heart rate, impaired judgment, etc.). These drugs can be dangerous, as even first-time use can cause sudden sniffing death within minutes (NIDA 2005). Long-term users may suffer from muscle weakness, disorientation, depression, and permanent damage to brain, heart, kidneys, and liver, and are more likely to engage in injection drug use (Crano et al. 2008; Dinwiddie 1994; Dinwiddie et al. 1991).
Inhalant use during early adolescence is especially problematic. Inhalants uniquely appeal to young adolescents because they are cheap, easily obtained, and provide a rapid if short-lived high, thereby lessening the likelihood of detection by parents or other authorities (Kurtzman et al. 2001). More than two-thirds of inhalant users report first use at 12–15 years of age (McGarvey et al. 1999). Usage appears to be growing. The Partnership for a Drug-Free America (PDFA 2004) estimated that inhalant use increased from 2002–2004 by 44% (from 18% to 26%) among 6th graders, and by 18% (from 22% to 26%) among 8th graders.
Past media campaigns designed to curtail or prevent inhalant use typically have focused on the physical harms attendant to usage (PDFA 2005). An assumption implicit in this approach is that by drawing attention to physical harms, users will desist and nonusers will not start. This assumption may be true, but inferences regarding physical well-being are not the only factors controlling use of dangerous substances. In related research, Milam et al. (2000) report that smokers consider smoking more harmful than non-smokers. Smokers understood the risks, but still smoked. Somatic consequences often do not predict future use (Chassin et al. 1991). The current research will prove useful in developing a theory based anti-inhalant prevention approach targeting young adolescents, which expands and improves upon prior prevention programs.
Outcome Expectancies
Tolman (1932) defined expectancies as memories or perceptions of the relationship between an action and the anticipated outcome of performing that action, or the expected relationship between a behavior and its consequence (Bolles 1972). Expectancies may be considered if/then statements: If I perform this action, then I should experience this outcome (Christiansen et al. 1989). Arguably, adolescents initiate drug use with specific expectancies in mind. This perspective considers young adolescents active decision makers who engage in inhalant use if they believe its salient benefits outweigh salient costs (Ajzen 1988; Boys et al. 2001). From a theory of planned behavior perspective (Ajzen 1991; Ajzen and Manstead 2007), expectations fall under the heading of attitudes, which are determined by beliefs about consequences of behaviors.
Research concerned with the relationship between adolescent expectations and inhalant use is sparse. However, a consistent pattern emerges in the general drug expectancy literature: Those who use substances perceive greater benefits or fewer costs than those who do not (Budd et al. 1983; Christiansen et al. 1982; Stacy et al. 1991). Expectations regarding the outcomes of substance use are predictive of alcohol use (Brown 1985; Christiansen et al. 1989; Stacy et al. 1991), marijuana use (Stacy et al. 1996) and tobacco consumption (Halpern-Felsher et al. 2004). Alcohol expectations account for significant variation in frequency and quantity of drinking over and above demographic factors, previous drinking levels, and alcohol-related attitudes (Carey 1995). These findings suggest that changing positive outcome expectations associated with inhalant use may curtail initiation.
Choosing the Most Valued Inhalant-Relevant Expectancies
An expectancy-value approach holds that individuals choose behaviors as a function of their outcome expectations and the value placed on these outcomes (Fishbein and Ajzen 1975). The most valued outcome will be most predictive of future drug use (Ajzen 2001). Thus, a belief that inhalant use will lead to feelings of euphoria may or may not result in use, depending upon the value of this outcome to the potential user. Inhalants may seem a useful means to an end for those who place great value on euphoric feelings and believe salient costs are outweighed by this benefit. The first challenge, then, is to specify inhalant-relevant outcomes most desirable to early adolescents. Many outcomes might be associated with use, but to enhance intervention effectiveness, outcomes widely perceived to be linked most positively to inhalant use must be isolated. Research on early adolescent development provides a useful starting point.
Early adolescents are expected to begin to take control of their social environments and behave as individuals with emergent adult identities. Such adaptation is challenging, as children must determine who they are going to be and how they wish to be seen (Erikson 1950). It probably is for this reason that the need for social acceptance and sensitivity to peer opinion peak at this stage (Brown 1990). This sensitivity suggests that young adolescents will be especially attentive to stimuli that might guide their behaviors so as to maximize socio-personal outcomes.
To explore expectations related to the pros and cons of inhalant use, Siegel et al. (2008) conducted a series of focus groups with young adolescents that centered on the question, “Why do people use inhalants?” The most prevalent answers reflected the perception that inhalant use, in and of itself, was a means of gaining social acceptance—popular kids used inhalants. Thus, if one wanted to be popular, one should consider using them too. This finding, combined with the literature pointing to early adolescence as a time when the need for social acceptance is at its peak, led us to concentrate on a term we coin socio-personal expectations (SPEs). In general, we propose the term SPEs as a reference to expectations related to the perceived linkages between a specific behavior and personally desired social outcomes. This study will investigate SPEs; the behavior is inhalant use, and the personally desired social outcome is increased social acceptance or popularity. The SPE concerning inhalant use and social acceptance may be differentiated from many expectations that have been considered under the general social expectancies umbrella: social-celebratory and social-physical pleasure; social assertiveness and social enhancement-impairment; social lubrication and social facilitation—all have been viewed as social expectancies (Aas et al. 1998; Brown 1985, 1993). SPEs specific to social acceptance differ from these earlier constructs as social acceptance SPEs are concerned with people’s expectations of how engaging in a specific behavior will increase popularity and acceptance in and of itself. Prior expectation studies have included a small number of items investigating SPEs of current interest (Zhao et al. 2006). However, SPEs concerning inhalant use and social acceptance or popularity are rarely the sole focus of investigation or intervention.
It is important to understand that SPEs and social norms are not one and the same. Norms are socially shared; expectations are specific to the individual (Lapinski and Rimal 2005). Social norms refer to the perceived prevalence of a behavior. A typical social norm message might be “Most students have five or fewer drinks at parties.” Conversely, SPEs are concerned with the perceived relation between engaging in a behavior and a desired social outcome. Social norms can influence social expectations, but SPEs consist of more than just social norms. An individual might believe that only a small percentage of individuals use inhalants, but if the individual desires popularity and believes usage will lead to popularity, then inhalant use will prove an attractive option. For this reason, expectations and social norms are commonly considered different constructs (Tickle et al. 2006; Wood et al. 1992). Moreover, considering the mixed results associated with social norm campaigns (Barnett et al. 1996; Cunningham et al. 2001; Thombs et al. 2004; Werch et al. 2000; Weschler et al. 2003), this current study has the potential to provide a step in a different direction for future efforts—one that has a more explicit focus on the relationship between SPEs and substance use.
SPEs also differ from what Ajzen and Manstead (2007) refer to as normative beliefs: “…the perceived behavioral expectations of important referent individuals or groups such as the person’s family, friends, co-workers, and health professionals” (p. 46). In this current research, we investigate SPEs specific to the expectations held by the individual concerning the social ramifications of using inhalants. Expectations differ from norms, in that they are considered under the general heading of attitudes, whereas normative beliefs fall under the heading of social norms (Ajzen and Manstead 2007). The extent to which important others expect the individual to become a user might affect his or her SPEs, but situations abound in which a behavior such as inhalant use can lead to increased social acceptance or popularity regardless of expectations of important others.
This research is developed to test five features relevant to our conceptualization of SPEs specific to inhalant use and social acceptance or popularity: (1) their malleability, (2) the possible impairment in knowledge of physical dangers resulting from exposure to messages that fail to emphasize physical harms, (3) message features associated with anti-inhalant persuasiveness, (4) the relationship between SPEs and inhalant intentions, and (5) the effect of messages emphasizing socio-personal outcomes on young adolescents’ decision-making processes in general.
Variables and Hypotheses
Malleability of inhalant relevant SPEs
The proposed approach can succeed only if adolescents’ SPEs regarding inhalant use and social acceptance or popularity are malleable. In their discussion of alcohol expectancies, Christiansen et al. (1982) stated, “…expectancy factors are conveyed by family, peer group, and the media as well as by observation of other individuals” (p. 342). If the media can create expectations, they may be capable of changing them as well. Decades of attitude research suggest attitudes are quite changeable, especially when little knowledge is attached to the attitude object (Crano and Prislin 2006). In the case of young adolescents who have had little experience in the agentic role, we expect SPEs concerning inhalant use and social acceptance will prove malleable (H1). Malleability will be tested by creating an ad focused on changing socio-personal expectations.
Fostering anti-inhalant message acceptance
All messages are not created equal. Message exposure does not necessarily result in persuasion. Social psychological research has identified many factors that facilitate the likelihood that a message will be believed and acted upon (Crano and Prislin 2006). This experiment will test whether manipulating message source and message directness, and the social or physical threat contained in the message, affects expectancies. We investigate these variables to gain insight into message- and extra-message features that might help reduce inhalant use, and the ways that such information may be conveyed effectively.
Source
Study of the effects of source variations in persuasion has a long and continuous history. A multitude of source features affect message acceptance (Hovland et al. 1953; Pornpitakpan 2004). If a source is perceived as expert and trustworthy, resistance to its message is reduced and the likelihood of acceptance increases (Tormala and Petty 2004). Generally, a message will not be effective if the source is not seen as credible. The source must be able to convince the message recipient that its information is accurate. Few sources are universally credible; thus, credibility must be judged in context (Siegel and Burgoon 2002). In some contexts, adults will have more influence than adolescents; in others, peers’ influence predominates (Werner-Wilson and Arbel 2000). A doctor is likely to be persuasive when discussing the physical harms of inhalants, but a peer may prove more persuasive when discussing inhalants’ social ramifications. By studying the effects of message source, we may learn to enhance the effectiveness of future interventions.
Message directness
Messages not focused specifically on the receiver have been found more persuasive than messages directly targeting the desired audience (Frey and Eagly 1993; Walster and Festinger 1962). Theoretically, this difference occurs because the target does not feel the need to raise cognitive defenses to defend against such messages. It follows that adolescents viewing an anti-inhalant message that apparently is directed toward parents may be less likely to counter-argue, and thus more persuaded by the message, than if they were exposed to the same message that targeted them directly. By varying the apparent target, we can determine the utility of an inhalant prevention strategy that may inhibit counterargumentation.
Intentions to use inhalants
In addition to being malleable, if our preventive approach is to succeed, the second requirement is that inhalant-related SPEs regarding social acceptance or popularity must be associated with inhalant use. Past studies clearly demonstrate an association between substance use and a range of perceived desirable outcomes (Stacy et al. 1991, 1996). For example, Newcomb et al. (1988) report correlations of desire to use alcohol and marijuana with sought-after outcome expectations, including positive affect, creativity, and social cohesion. Based on the importance of social relationships during early adolescence, we predict SPEs regarding inhalant use and social acceptance will be significant predictors of inhalant intentions. However, SPEs will be of limited value if they do not account for variance over and above variables previously associated with substance use. These variables include age, gender, academic performance, race/ethnicity, prior inhalant use, sensation seeking, peer deviance, parental monitoring, and perceived physical ramifications of use (Ames et al. 2005; Ball 1995; Howard and Jenson 1999; Peterson and Hann 1999; Seydlitz and Jenkins 1998). We predict SPEs will be associated with inhalant intentions even after accounting for all other variables (H2).
Salience and Adolescent Decision Making
Many different expectancies may become associated with a given drug (Brown 1993). However, the more salient a belief, the more likely it will be accessible and thus influence the decision-making process (Ajzen 2001). In addition to changing SPEs associated with inhalant use and social acceptance or popularity, a persuasive message focused on potential social outcomes also might change which expectancies are afforded the greatest weight. Oei and Baldwin (1994) argued that initiation of drug use involves a “mental algebra” in which expectancies about drug use are deliberately weighed. Whereas a young adolescent may have a range of inhalant-relevant beliefs (e.g., inhalants are deadly), not every belief is equally influential. Salience refers to the accessibility of specific information for an individual. A key finding suggests that the more salient the data, the greater the impact that information will have on decision making (Slovic et al. 1982; Taylor and Fiske 1978). Thus, if SPEs regarding inhalant use and social acceptance or popularity are made salient, they should play a large role in the decision making process (Van Schie and Van der Pligt 1995). This leads to the proposition that the decision to use inhalants will be based on information that is most salient (H3). To be clear, we do not expect a social message to directly affect inhalant intentions; rather, we expect the social message to influence the valence and the salience of SPEs, which in turn will affect intentions. Accordingly, we will explore how messages focused on SPEs (vs. physical harms) may lead to differential variables (e.g., parental monitoring, peer deviance, sensation seeking) accounting for more or less variance in inhalant intentions. Simply, a social threat message may not only influence SPEs but the variables that predict inhalant intentions as well.
Method
This research tests the effects of three manipulated variables on young adolescents’ intentions to use inhalants. Dependent variables are participants’ positive and negative socio-personal expectancies of inhalant use and the perceived harmfulness of inhalant drugs.
Participants
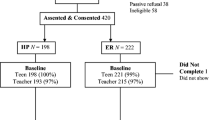
In total, 893 6th (n = 312) and 7th (n = 581) grade students participated. They were drawn from three schools in southern California. The demographic breakdown is reported in Table 1. Consent was obtained from school administration and students’ parents or guardians, and assent was obtained from participants, who were randomly assigned to one of the eight experimental conditions (n > 100 per condition) formed by the factorial combination of three independent variables.
Experimental Manipulations
Social/physical threat
To test the malleability of SPEs as well as the potential detriment of not focusing on physical harms, we created two sets of 60-s messages, both with the same video, but different audio and graphic cards. A class of middle school students assisted us with the writing, filming and directing. The ads focused either on the social or the physical harms of inhalant use. The physical harm message manipulation included information about the number of deaths caused by inhalants, as well as other negative outcomes: brain damage, hearing loss, and seizures. The physical harm ad related the story of two adolescent “sniffers”—one who vomited, the other who ruined his kidneys and required dialysis for the rest of his life.
The social harms script informed viewers that inhalant users were disliked, the type of persons no one wanted to befriend. The ad noted the small percentage of adolescents who used inhalants. Viewers also were told that no one liked or wanted to be around “huffers” and “sniffers.” A story was told about two adolescent “sniffers” who hoped to impress their friends by using inhalants, but ended up being laughed at, rejected, and ignored.
Additional Manipulations
To assess how the persuasive strength of our social/physical threat messages can be maximized, four variations of the social threat message and four variations of the physical threat message were created. Simply, eight variations of a 60 s anti-inhalant ad were created. The four social threat variations and the four physical threat variations were formed by the factorial combination of source and message directness.
Source (peer or doctor)
To manipulate message source, the first 12-s of the experimental anti-inhalant messages contained a medium shot of either a doctor or an adolescent. The source was seen only in these 12-s. The same individual, a young female East Indian medical student, played the high school student and medical doctor roles. The doctor footage was filmed in a doctor’s examination room. Medical equipment was clearly visible. The doctor was dressed in scrubs and a lab coat. In her introduction, she stated, “…I am a medical doctor with teenage patients.” To remind viewers of the message source, the final sentence at the end of the anti-inhalant message was, “As a doctor, I have seen this happen. Ask a doctor you trust.”
The peer condition was filmed in a classroom. The peer source was dressed in jeans and a t-shirt. A chalkboard and a teacher’s desk were in the background. At the start of the message the actress stated, “I just finished my third year of high school.” As with the message involving the doctor, the message ended with a reminder of the source: “…I am a high school junior, I’ve seen this happen. Ask a high schooler you trust.”
Message directness (direct or indirect)
To manipulate message directness, the source explicitly stated that the message was targeted at the adolescent viewer or the parent of the viewer. The direct condition began with: “Are you in the 6th, 7th, or 8th grade?” Then, four times over the course of the ad, statements reinforced the target of the video: “You may think…if you do…” Toward the end of the video, the intended viewer was addressed directly: “Students…” In contrast, the indirect condition began with, “Parents, do you have a young teen at home?” Like the direct condition, statements reinforced the intended ad target: “Your child…they are…” At the end of the message, the apparently intended viewer was addressed directly: “Parents…”
Procedure
Investigators set up 28 laptop computers in quiet areas designated by each school. Students were seated individually at computer stations. Each student was presented with an assent form, which was read aloud by one of the investigators. All provided written declaration of their desire to participate. Once assent was given, participants were instructed to don a pair of headphones and begin the study. On screen, they encountered a series of demographic and psychographic questions, as well as items regarding past substance use. To avoid comprehension problems, a narration of all questions and possible answers was piped through the earphones provided.
After the pretest, participants watched a 5 min anti-bullying video, which was intended to distract participants from the real purpose of the study. The video, written by the investigators, informed viewers how they could avoid being bullied and how they could help the victims of bullying. A short break consisting of two 1-min commercials began approximately two-thirds through the video. The first was a DELL computer commercial. Up to this point, all participants were exposed to the same content. After the computer commercial, participants viewed one of the eight anti-inhalant messages disguised as commercials. Assignment to condition was random. After the 1 min anti-inhalant message was screened, the bullying video continued for approximately 1.5 min. When the video ended, participants completed the posttest. Afterwards, all participants were debriefed. The entire investigation, from assent to debriefing, lasted approximately 30–40 min.
Pretest Measures
Socio-demographics
Age was calculated from adolescents’ self-reported date of birth. Participants also reported their gender, race, and average report card grade.
Inhalant use
A single yes–no item measured past inhalant use. It read, “Have you tried using inhalants (even only once)?”
Sensation seeking (α = .80)
Sensation seeking is posited to be a biologically based personality trait (Zuckerman 1994). High sensation seekers have a need for novel experience, physiological arousal, and a propensity to take various risks to meet this need (Stephenson et al. 2003). Traditionally, sensation seeking has been measured via a 40-item, forced-choice, measure: Form V of the Sensation Seeking Scale (SSS-V; Zuckerman et al. 1979). An eight-item sensation seeking instrument was created due to the length of the SSS-V (Hoyle et al. 2002). This eight-item Brief Sensation Seeking Scale (Hoyle et al. 2002) was used in this current study. Examples from this eight-item, 7-point Likert format, measure include: “I would like to explore strange places,” “I would like to take off on a trip with no pre-planned routes or timetables,” and, “I prefer friends who are excitingly unpredictable.”
Peer deviance (α = .82)
A subscale of the Youth Asset Scale (Oman et al. 2002) is used to assess the perceived extent of one’s peers’ deviant behavior. The Youth Asset Scale was created to measure the developmental assets held by youth. Youth lacking developmental assets are found to be at risk for eight different risk behaviors including tobacco use, truancy, drug and alcohol abuse, and police involvement (Oman et al. 2002). A 7-point Likert response format was used on this four-item measure. Examples of items are: “Do most of your friends stay out of trouble?” and “Do most of your friends follow the rules their parents make for them?”
Parental monitoring (α = .82)
Parental monitoring was measured via the Parental Monitoring Scale (Brown et al. 1993). The measure was initially created to challenge the assumption that parents do not influence the behavior of high school adolescents (Brown et al. 1993). The scale’s internal consistency has ranged from .77–.81 (Brown et al. 1993; Krishnakumar et al. 2003). A 7-point Likert format was used for this five-item measure. Examples of items are: “How much does your parent(s) really know … who your friends are?,” “…where you go at night?,” and, “…where you are most afternoons after school?”
Posttest Measures
Consistent with Stacy et al.’s (1996, p. 25) recommendation, both positive and negative socio-personal expectation measures were created. Factor analysis supported the wisdom of this decision, as the two scales loaded on orthogonal factors. Both SPE measures were created specifically for this study.
Positive SPEs (α = .89)
As mentioned, while SPEs can refer to a range of desired social outcomes, for this study we are specifically interested in SPEs regarding inhalant use and social acceptance. Positive SPEs refer to the perceived positive social outcomes (e.g., social acceptance, popularity) associated with inhalant use. The three items used a 7-point Likert format. The items read: “If you used inhalants and everyone found out, how likely is it … more people would want to spend time with you?” “…you would make new friends?” “…people would like you better?”
Negative SPEs (α = .73)
Negative SPEs of inhalant use refer to the perceived relationship between use and social rejection. These items used a 7-point Likert format. The three items read: “If you used inhalants and everyone found out, how likely is it …you would lose some of your friends?” “…people would make fun of you?” “…you would become less popular?”
Physical harms of inhalant use (α = .72)
Items adapted from the National Survey of Parents and Youth (NSPY; NIDA 2006) tapped the belief that inhalant use would lead to physical harm. The NSPY was implemented to assess the effectiveness of the National Youth Anti-Drug Media Campaign in reducing substance use among adolescents. The three items, which made use of a 7-point Likert format, were: “If you used inhalants, how likely is it … you would get sick?” “…you would damage your brain?” “…the inhalants would kill you?”
Inhalant use intentions (α = .82)
This construct assessed respondents’ intentions to use inhalants. The items, also adapted from the NSPY, were: “Do you think you will use inhalants, even once or twice, over the next 12 months?” “Do you think you will ever use inhalants in the future?” “In the future, I will not use inhalants.” “There’s no way that I will use inhalants in the future.” The first two items were scaled on 4-point scales (definitely no to definitely yes) and the last two items on 7-point (strongly agree to strongly disagree) scales. Item values were standardized before computing composite scores.
Data Analytic Plan
To examine the effects of the experimental messages on the SPEs, a factorial MANOVA was conducted. This was followed by independent samples t-tests to decompose significant effects. We then assessed whether SPEs were related to usage intentions via hierarchical multiple regression models—one for all respondents, one for those who received the social threat, and one for those who received the physical threat. The outcome variable was participants’ intentions to use inhalants. Identical predictors were entered into each of the three models, as follows: In the first (“Socio-demographics”) step, age, gender, grades, and race were entered. These variables have been shown to have some association with inhalant use intentions. In the second step, prior inhalant use was entered. This variable is expected to be strongly associated with future usage intentions. The psychosocial measures of sensation seeking, peer deviance, and parental monitoring were entered in the third step. Each of these variables has been shown to be associated with usage (Ramirez et al. 2004). In the fourth step, participants’ expectations regarding the physical outcomes of inhalant use were entered. Positive and negative SPEs of inhalant use—social benefits and social repercussions—were entered in the final step. No problems of multicollinearity were encountered in any of the models, as tolerance levels for each predictor exceeded .55.
Finally, we examined whether the effect of the social/physical threat on inhalant intentions was mediated via expectations. A structural equation model was specified with EQS 6.1 (Bentler 2006), and estimated with Maximum Likelihood. The threat message (1 = social, 0 = physical) was specified to predict the three expectation variables, which in turn were set to predict inhalant intentions. As the three expectancy variables were hypothesized to be interrelated, their error terms were correlated.
Results
Messages on SPEs
The first analysis was designed to determine whether SPEs are malleable. A 2 (source) × 2 (directness) × 2 (threat) multivariate analysis of variance (MANOVA) was conducted to test the effects of the independent variables on positive and negative SPEs and perceived inhalant-related physical harms. Only the multivariate main effect of threat was statistically significant, F(3, 881) = 24.47, p < .001. No other statistically significant multivariate main effects or interactions were found.
Follow-up univariate analyses were conducted on each of the three critical dependent measures to decompose the significant threat effect. As predicted (H1), SPEs were malleable. Participants exposed to the social threat (M = 1.84, SD = 1.21) reported significantly less positive SPEs than those exposed to the physical threat (M = 2.49, SD = 1.59), t(891) = −6.93, p < .001, d = .45, and more negative SPEs (M = 5.40, SD = 1.70) than those exposed to the physical threat (M = 4.76, SD = 1.64), t(891) = 5.72, p < .001, d = .38. However, those exposed to the physical threat message (M = 6.36, SD = 1.10) did not rate the physical dangers of inhalants as greater than those exposed to the social threat (M = 6.22, SD = 1.19), t(891) = −1.85, ns. This particular result suggests that participants who received the social threat were not less wary than those exposed to the physical harms ad of the physical dangers of inhalant use. Although not hypothesized, further analyses tested whether there was a direct effect of the threat manipulation on inhalant intentions. As expected, given that the threat manipulation was brief and would be unlikely to affect cognitions as critical as inhalant intentions, there were no between group differences on this measure as a function of type of threat, t(891) = .74, ns. We did hypothesize that SPEs were associated with whether one intends to use inhalants. This proposed process was tested in the next set of analyses.
SPEs Predicting Inhalant Intentions
At issue now was the predictive validity of these expectations on intentions to use inhalants, after controlling for rival factors. Participants’ positive and negative social expectations were used as predictors of inhalant usage intentions in a series of hierarchical multiple regression analyses.
The multiple regression model involving all participants is presented in Table 2, which displays the added variance contributed by predictors at each step, along with the beta (β) weights associated with the complete model. The analysis disclosed a significant but weak predictive association of the demographic predictors with intentions. Past usage, entered in the second step, was strongly associated with intentions, as expected. Peer deviance and parental monitoring also were significantly associated with intention, in directions consistent with prior research. Physical harms expectations, entered in the fourth step, added unique variance as well. In the final step, as hypothesized (H2), positive and negative SPEs proved significant predictors of intentions, even after accounting for the effects of all the earlier variables. The overall prediction of inhalant intention was statistically significant (R 2 = .26, p < .001). As expected, prior use was the most powerful predictor of usage intentions; the next strongest predictor, as indicated by the final model’s beta weights, was participants’ positive SPEs regarding inhalant use and social acceptance or popularity, followed by parental monitoring, peer deviance, and perception of physical threat.
The aggregated analysis of Table 2 contained participants exposed to either a social or a physical threat. While the social threat ad directly affected socio-personal expectations, there was no overall direct impact of social threat on inhalant intentions. This should not be interpreted as their having no influence on intentions. Separate regression models were estimated for each group (Table 3). Splitting the participants as a function of the message they received revealed that being exposed to a social threat message influenced the factors that affect intentions. As predicted (H3), SPEs were more strongly associated with intentions among those who received the social threat. Among these participants, prior inhalant use and peer deviance emerged in the early steps as significant predictors of inhalant intent. After accounting for these predictors, both positive (β = .23, p < .001) and negative (β = −.16, p < .001) SPEs were found to be significantly associated with intentions. For respondents who viewed the physical threat message, prior inhalant use, low parental monitoring, low physical harm expectations, and positive SPEs predicted inhalant intentions. The patterns of statistically significant beta coefficients overlapped in the two analyses, but there were noteworthy deviations, which will be discussed. Both models produced statistically significant predictions of intentions. Again, while social threat did not directly affect intentions, predictors of inhalant intentions were changed as a result of message type.
Mediational Analysis
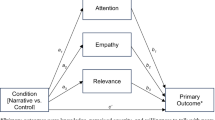
Results from the hypothesized structural equation model (Fig. 1) show that the effect of the message threat manipulation (1 = social, 0 = physical) on inhalant intentions was mediated through both positive and negative SPEs. There was no direct effect of social threat on inhalant intentions, nor was one predicted. Mediation is the feature of interest in this analysis. For diagrammatic clarity, not displayed are the correlated error terms among the expectation measures, which were significant (all p < .001) and as follows: physical harms with positive SPEs (r = −.15), physical harms with negative SPEs (r = .23), and positive and negative SPEs (r = −.37).

Expectations mediating the relationship between social threat and inhalant intentions
The adequacy of the mediational model, χ 2(1) = 9.87, p < .01, was evaluated with the following indices: CFI = .98, IFI = .98, and NFI = .98 These comparative approaches to model fit typically range from approximately 0 to 1.00, with higher values suggesting better fit (Ullman and Bentler 2003). The Root Mean Square Error of Approximation (RMSEA), a residual-based index, was .10. Values above .10 indicate a poor fitting model (Browne and Cudeck 1993).
Discussion
An expectancy-value orientation was adopted to promote a deeper understanding of the role of expectancies in adolescent inhalant use. The approach assumed that expectancies were associated with usage, and that this result would have implications for prevention. Expectancies come in many varieties. This research was built on the assumption that SPEs concerning inhalant use and social acceptance or popularity, largely understudied, would prove crucial for young adolescents who are particularly attuned to social acceptance and rejection. On the basis of past practice, physical threats also were viewed as likely to affect physical expectations. The important question beyond this result is whether the predictive utility of SPEs would be maintained even after accounting for variations in physical expectancies. If so, then the utility of adding a socio-personal factor in inhalant prevention programs is supported.
The first task of the research, therefore, was to determine whether or not SPEs of inhalant use and social acceptance could be modified by communications. Even if SPEs were strongly related to subsequent inhalant use, this information would be largely academic if they were not amenable to change. As hypothesized, analyses demonstrated that SPEs were malleable via mediated ads. Participants exposed to a 60-s message that detailed some of the negative social outcomes of inhalant use were significantly less likely than those whose message focused on the physical dangers of inhalants to associate use with positive socio-personal outcomes, and significantly more likely to associate inhalants with negative socio-personal outcomes. Also important was the relatively negligible impact that the physical harms ad had on participants’ perceptions of inhalant dangers. In combination, these two findings suggest that inhalant prevention efforts focusing on physical harms alone might merely confirm what users and nonusers alike already know, namely that inhalants can be dangerous, even deadly. This is not to suggest that such information is unnecessary, but rather that it might not be sufficient to mitigate use.
The malleability of SPEs concerning inhalant use and social acceptance or popularity would be irrelevant if the construct were not related to intentions. This relation is critical, as considerable research has found intentions to be strongly related to subsequent actions (e.g., Abraham and Sheeran 2003; Ajzen et al. 2004; Sheeran and Abraham 2003). Across all participants, SPEs were significant predictors of inhalant intentions even after accounting for standard demographic factors, school performance, sensation seeking, peer deviance, parental monitoring, perceived physical harms of inhalant use, and even prior use. This result, uncovered in the overall hierarchical multiple regression analysis, suggests that SPEs are strongly associated with inhalant intentions and should be a component of future adolescent-targeted prevention efforts, perhaps in concert with information of the physically debilitating nature of inhalants.
The results suggest that SPEs can be changed via persuasive messages, and these expectations are predictive of inhalant intentions. These two findings alone are important. Many researchers have called for substance abuse campaigns to focus on topics other than physical harms (e.g., Halpern-Felsher et al. 2004), with some advocating what we have termed a SPEs approach (Schoenbachler and Whittler 1996). Current results suggest that these recommendations are well founded, although a SPE approach is not advanced as a cure-all. First, physical harm messages should not be eliminated insofar as physical expectations did prove predictive of inhalant intentions. It also is important to understand that not all adolescents will be equally affected by an SPE approach. An SPE approach will likely be least effective for adolescents who are secure in their social status; conversely, those who have formed a positive use-popularity expectation may find the threat of ostracism relevant and intimidating.
The current results may help explain the variable outcomes of social norms interventions. As noted, earlier social norm campaigns typically focused on correcting misperceptions of substance abuse prevalence (Haines and Spear 1996; Mattern and Neighbors 2004; Neighbors et al. 2004). These campaigns have been met with mixed results (Barnett et al. 1996; Cunningham et al. 2001; Thombs et al. 2004; Werch et al. 2000; Weschler et al. 2003). Capitalizing on, and making explicit the linkage of SPEs concerning substance use and social acceptance or popularity might increase the success of social norm interventions directed toward adolescents (Hansen and Graham 1991).
The hierarchical multiple regression analyses provided information beyond that discussed to this point. To maximize our understanding of the influence of the social threat message, the dataset was split as a function of the threat participants received. SPEs accounted for 8% of the social expectancy-intention variance in those exposed to the social threat; these same expectations accounted for 2% of the variance among those exposed to the physical harm message. Notably, this effect size was over and above other important covariates related to inhalant intentions. From a prevention standpoint, such an impact, in addition to contributing beyond other factors, may have considerable practical implications in terms of sparing some children from contemplating use of these hazardous substances.
Some of the most intriguing findings were revealed by the separate hierarchical regressions on samples differentiated by exposure to social or physical threat messages. These analyses suggested that different forms of threat (social, physical) can affect the pattern of variables that influence inhalant intentions. For example, perceptions of peer deviance were more predictive of inhalant intentions in the social (vs. physical) threat condition, whereas perceptions of parental monitoring were more predictive of intentions in the physical (vs. social) threat condition. Influencing the relevant variables that are active during the decision-making process can have robust influence on adolescent substance use (Stacy and Weir 2006). Notably, these results are similar to those of Routledge, Arndt, and Goldenberg (2004), who found increased interest in sunscreen when mortality was made salient, but increased interest in tanning services when attractiveness of people who tan was emphasized.
Unexpectedly, the source manipulation had no effect on socio-personal expectations. The source was seen only at the start of the message and even though the viewer was reminded of the source’s identity, it is possible that the manipulation was not sufficiently pronounced to affect acceptance. Conceivably, the actress playing the high school student and the doctor was not convincing, or her ethnicity led to unexpected resistance. These latter possibilities seem unlikely given the other effects that were found. A non-credible source likely would have mitigated the effects of the other treatments as well. As such, the first possibility—an insufficiently strong manipulation—seems the most plausible explanation of the lack of source effects.
Overall, the results of this study highlight three benefits of a more concerted focus on SPEs regarding inhalant use and social acceptance or popularity. SPEs are malleable via persuasive messages. When made salient, they affect inhalant intentions. To the extent that adolescents who engage in inhalant use are aware of the risks, it may be beneficial for prevention efforts to emphasize the negative social ramifications of usage in addition to physical risks for those contemplating inhalant use. Messages that alter young adolescents’ inhalant-based SPEs regarding inhalant use and social acceptance or popularity, as well as other socio-personal outcomes, might play a prominent role in their decision to delay, or refrain from, inhalants. As SPEs concerning inhalant use and social acceptance or popularity are malleable and relevant to young adolescents, making them salient, and ensuring that inhalant use is associated with negative socio-personal outcomes, could help assure the success of future anti-inhalant efforts focused on younger audiences.
Not every belief plays an equal role in every decision. The association of SPEs with inhalant intentions was substantial when participants were exposed to a social threat in an anti-inhalant communication. This suggests that anti-drug media campaigns can change the perceived outcomes associated with use, or they can alter the variables that adolescents consider when deciding whether to use or abstain from a drug. These results also suggest caution when considering predictors of drug use. When SPEs were made salient, peer deviance was a significant predictor of intentions, and parental monitoring was not. When physical harms were made salient, the opposite was true. These variations are not due to a lack of statistical power; rather, the context in which data were gathered affected the prominence of predictors of drug-relevant behavior.
The limitations to this research should be noted. Owing to the use of a one-time experimental design, we can make no assumptions about the longevity of message influence. Also, we do not know if every manipulation of SPEs will succeed. Only one exemplar of this ad type was used. Future longitudinal efforts using several message exemplars stressing social or physical harms should be used. Finally, we did not explore the differential impact of the ad on adolescents of different inhalant user status (e.g., user, nonuser, etc.).
Finally, it is possible that SPEs concerning popularity and social acceptance become less important in later adolescence, when peer acceptance and popularity become less salient. As such, a focus on more personally relevant SPEs might be needed when targeting older groups. Moreover, it should not be assumed that all young adolescents place social acceptance or popularity at the top of the priority list. Popularity and social acceptance are of paramount importance to many adolescents, but the desire to be popular is not universal (Coleman 1961). Future studies need to consider the range of social outcomes desired by adolescents.
Conclusion
Past anti-inhalant media campaigns typically focus on the physical ramifications of drug use (e.g., PDFA 2005). The findings of the current study lend support to calls to broaden intervention efforts to include SPEs regarding inhalant use and social acceptance or popularity along with discussion of physical harms (Chassin et al. 1991; Pechman et al. 2003; Schoenbachler and Whittler 1996). SPEs have proved both changeable and predictive of inhalant intentions. Based on current knowledge, there appears little to be gained by focusing solely on physical harms. A more intensive focus on SPEs could prove effective in persuading adolescents to refrain from use of a class of drugs that represents a serious threat to the well-being of all who use them.
References
Aas, H. N., Leigh, B. C., Anderssen, N., & Jakobsen, R. (1998). Two-year longitudinal study of alcohol expectancies and drinking among Norwegian adolescents. Addiction, 93, 373–384.
Abraham, C., & Sheeran, P. (2003). Acting on intentions: The role of anticipated regret. British Journal of Social Psychology, 42, 495–511.
Ajzen, I. (1988). Attitudes, personality, and behavior. Chicago: Open University Press.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179–211.
Ajzen, I. (2001). Nature and operation of attitudes. Annual Review of Psychology, 52, 27–58.
Ajzen, I., Brown, T. C., & Carvajal, F. (2004). Explaining the discrepancy between intentions and actions: The case of hypothetical bias in contingent valuation. Personality and Social Psychology Bulletin, 30, 1108–1121.
Ajzen, I., & Manstead, A. S. R. (2007). Changing health-related behaviours: An approach based on the theory of planned behaviour. In M. Hewstone, H. A. W. Schut, J. B. F. de Wit, K. van den Bos, & M. S. Stroebe (Eds.), The scope of social psychology: Theory and applications (pp. 43–63). Psychology Press, Philadelphia, PA, USA.
Ames, S. L., Sussman, S., Dent, C. W., & Stacy, A. W. (2005). Implicit cognition and dissociative experiences as predictors of adolescent substance use. American Journal of Drug and Alcohol Abuse, 3, 129–162.
Ball, S. A. (1995). The validity of a five-factor measure of personality in cocaine abusers. Psychological Assessment, 2, 148–154.
Barnett, L. A., Far, J. M., Mauss, A. L., & Miller, J. A. (1996). Changing perceptions of peer norms as a drinking reduction program for college students. Journal of Alcohol and Drug Education, 41, 39–62.
Bentler, P. M. (2006). EQS 6 structural equations program manual. Encino, CA: Multivariate Software.
Bolles, R. C. (1972). Reinforcement, expectancy, and learning. Psychological Review, 79, 394–409.
Boys, A., Marsden, J., & Strang, J. (2001). Understanding reasons for drug use amongst young people: a functional perspective. Health Education Research, 16, 457–469.
Brown, S. A. (1985). Expectancies versus background in the prediction of college drinking patterns. Journal of Consulting and Clinical Psychology, 53, 123–130.
Brown, S. A. (1990). Adolescent alcohol expectancies and risk for alcohol abuse. Addiction and Recovery, 10, 16–19.
Brown, S. A. (1993). Drug effect expectancies and addictive behavior change. Experimental and Clinical Psychopharmacology, 1, 55–67.
Brown, B. B., Mounts, N., Lamborn, S. D., & Steinberg, L. (1993). Parenting practices and peer group affiliation. Child Development, 64, 467–482.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural models (pp. 136–162). Newbury Park, CA: Sage.
Budd, R., Bleiker, S., & Spencer, C. (1983). Exploring the use and non-use of marijuana as reasoned actions: An application of Fishbein and Ajzen’s methodology. Drug and Alcohol Dependence, 11, 217–224.
Carey, K. B. (1995). Alcohol-related expectancies predict quantity and frequency of heavy drinking among college students. Psychology of Addictive Behaviors, 9, 236–241.
Chassin, L., Presson, C. C., Sherman, S. J., & Edwards, D. A. (1991). Four pathways to young-adult smoking status: Adolescent social-psychological antecedents in a Midwestern community sample. Health Psychology, 10, 409–418.
Christiansen, B. A., Goldman, M. S., & Inn, A. (1982). The development of alcohol-related expectancies in adolescents: Separating pharmacological from social learning influences. Journal of Consulting and Clinical Psychology, 50, 336–344.
Christiansen, B. A., Smith, G. T., Roehling, P. V., & Goldman, M. S. (1989). Using alcohol expectancies to predict adolescent drinking behavior one year after. Journal of Consulting and Clinical Psychology, 57, 93–99.
Coleman, J. S. (1961). The adolescent society: the social life of the teenager and its impact on education. New York: Free Press.
Crano, W. D., & Prislin, R. (2006). Attitudes and attitude change. Annual Review of Psychology, 57, 345–374.
Crano, W. D., Ting, S. A., & Hemovich, V. (in press). Inhalants. In L. Cohen, F.L. Collins, A. M. Young, D. E. McChargue, & T. Leffingwell (Eds.), The pharmacology and treatment of substance abuse: An evidence based approach. Mahwah, NJ: Erlbaum.
Cunningham, J. A., Wild, T. C., Bondy, S. J., & Lin, E. (2001). Impact of normative feedback on problem drinkers: A small-area population study. Journal of Studies on Alcohol, 62, 228–233.
Dinwiddie, S. H. (1994). Abuse of inhalants: A review. Addiction, 89, 925–939.
Dinwiddie, S. H., Reich, T., & Cloninger, C. R. (1991). Solvent use as a precursor to intravenous drug use. Comparative Psychiatry, 32, 133–140.
Erikson, E. H. (1950). Childhood and society. New York: Norton.
Fishbein, M., & Ajzen, I. (1975). Belief, attitude, intention, and behavior: An introduction to theory and research. Reading: Addison-Wesley.
Frey, K. P., & Eagly, A. H. (1993). Vividness can undermine the persuasiveness of messages. Journal of Personality and Social Psychology, 65, 32–44.
Haines, M., & Spear, S. F. (1996). Changing the perception of the norm: A strategy to decrease binge drinking among college students. Journal of American College Health, 45, 134–140.
Halpern-Felsher, B. L., Biehl, M. A., Kropp, R. Y., & Rubinstein, M. L. (2004). Perceived risks and benefits of smoking: Differences among adolescents with different expectancies and intentions. Preventive Medicine, 39, 559–567.
Hansen, W. B., & Graham, J. W. (1991). Preventing alcohol, marijuana, and cigarette use among adolescents: Peer pressure resistance training versus establishing conservative norms. Preventive Medicine, 20, 414–430.
Howard, M. O., & Jenson, J. M. (1999). Inhalant use among antisocial youth: Prevalence and correlates. Addictive Behaviors, 24, 59–74.
Hovland, C. I., Janis, I. L., & Kelley, H. H. (1953). Communications and persuasion: psychological studies in opinion change. New Haven, CT: Yale University Press.
Hoyle, R. H., Stephenson, M. T., Palmgreen, P., Lorch, E. P., & Donohew, R. L. (2002). Reliability and validity of a brief measure of sensation seeking. Personality and Individual Differences, 32, 401–414.
Krishnakumar, A., Buehler, C., & Barber, B. K. (2003). Youth perceptions of interparental conflict, ineffective parenting, and youth problem behaviors in European-American and African-American families. Journal of Social and Personal Relationships, 20, 239–260.
Kurtzman, T. L., Otsuka, K. N., & Wahl, R. A. (2001). Inhalant abuse by adolescents. Journal of Adolescent Health, 28, 170–180.
Lapinski, M. K., & Rimal, R. N. (2005). An explication of social norms. Communication Theory, 15, 127–147.
Mattern, J. L., & Neighbors, C. (2004). Social norms campaigns: Examining the relationship between changes in perceived norms and changes in drinking levels. Journal of Studies on Alcohol, 65, 489–493.
McGarvey, E. L., Clavet, G. J., Mason, W., & Waite, D. (1999). Adolescent inhalant abuse: Environments of use. American Journal of Drug Alcohol Abuse, 25, 731–41.
Milam, J. E., Sussman, S., Ritt-Olson, A., & Dent, C. W. (2000). Perceived invulnerability and cigarette smoking among adolescents. Addictive Behaviors, 25, 71–80.
National Institute of Drug Abuse. (2005). NIDA Research report series: Inhalant Abuse. NIH Publication Number 05-3818.
Neighbors, C., Larimer, M. E., & Lewis, M. A. (2004). Targeting misperceptions of descriptive drinking norms: Efficacy of a computer delivered personalized normative feedback intervention. Journal of Consulting and Clinical Psychology, 72, 434–447.
Newcomb, M. D., Chou, C. P., Bentler, P. M., & Huba, G. J. (1988). Cognitive motivations for drug use among adolescents: Longitudinal tests of gender differences and predictors of change in drug use. Journal of Counseling Psychology, 35, 426–438.
National Institute of Drug Abuse [NIDA] (2006). User’s guide for the evaluation of the national youth anti-drug media campaign: Restricted use files for the National Survey of Parents and Youth (NSPY), Rounds 1, 2, 3, and 4. Rockville, MD: Westat.
Oei, T. P. S., & Baldwin, A. R. (1994). Expectancy theory: A two-process model of alcohol use and abuse. Journal of Studies on Alcohol, 55, 525–534.
Oman, R. F., Vesely, S. K., McLeroy, K. R., Harris-Wyatt, V., Aspy, C., Rodine, S., et al. (2002). Reliability and validity of the Youth Asset Survey (YAS). Journal of Adolescent Health, 31, 247–255.
Partnership for a Drug Free America. (2004). More pre-teens abusing inhalants. http://www.drugfree.org/Portal/About/NewsReleases/More_Pre_Teens_Abusing_Inhalants. Accessed March 5, 2005.
Partnership for a Drug Free America. (2005). Case studies about the effectiveness of the Partnership’s media-based educational campaigns. http://www.drugfree.org/Portal/DrugIssue/News/New_Findings_on_Inhalants_Parent_&_Youth. Accessed October, 10, 2006.
Pechman, C., Zhao, G., Goldberg, M. E., & Reibling, E. L. (2003). What to convey in antismoking advertisements for adolescents: The use of protection motivation theory to identify effective message themes. Journal of Marketing, 67, 1–18.
Peterson, G. W., & Hann, D. (1999). Socializing children and parents in families. In M. B. Sussman, S. K. Steinmetz, & G. W. Peterson (Eds.), Handbook of marriage and the family, (2nd ed). New York: Plenum.
Pornpitakpan, C. (2004). The persuasiveness of source credibility: A critical review of five decades’ evidence. Journal of Applied Social Psychology, 34, 243–281.
Ramirez, J. R., Crano, W. D., Quist, R., Burgoon, M., Alvaro, E. M., & Grandpre, J. (2004). Acculturation, familism, parental monitoring, and knowledge as predictors of marijuana and inhalant use in adolescents. Journal of Addictive Behaviors, 18, 3–11.
Routledge, C., Arndt, J., & Goldenberg, J. L. (2004). A time to tan: Proximal and distal effects of mortality salience on sun exposure intentions. Personality and Social Psychology Bulletin, 30, 1347–1358.
Schoenbachler, D., & Whittler, T. (1996). Adolescent processing of social and physical threat communications. Journal of Advertising, 25, 37–54.
Seydlitz, R., & Jenkins, P. (1998). The influence of families, friends, schools, and community on delinquent behavior. In T. Gullotta, G. Adams, & R. Montemayor (Eds.), Delinquent violent youth: Theory and interventions (pp. 53–97). Thousand Oaks, CA: Sage.
Sheeran, P., & Abraham, C. (2003). Mediator of moderators: Temporal stability of intention and the intention–behavior relation. Personality and Social Psychology Bulletin, 29, 205–215.
Siegel, J.T., Alvaro, E.M., Patel, N., & Crano, W.D. (in press) “…you would probably want to do it. Cause that’s what made them popular”: Exploring perceptions of inhalant utility among young adolescent non-users and occasional users. Substance Use and Misuse.
Siegel, J. T., & Burgoon, J. K. (2002). Expectancy theory approaches to prevention: Violating adolescent expectations to increase the effectiveness of public service announcements. In W.D. Crano & M. Burgoon (Eds.), Mass media and drug prevention: Classic and contemporary theories and research (pp. 163–186). Mahwah, NJ: Erlbaum.
Slovic, P., Fischhoff, B., & Lichtenstein, S. (1982). Facts versus fears: Understanding perceived risk. In D. Kahneman, P. Slovic, & A. Tversky (Eds.), Judgment under uncertainty: Heuristics and biases (pp. 463–492). Cambridge: Cambridge University Press.
Stacy, A. W., Galaif, E. R., Sussman, S., & Dent, C. W. (1996). Self-generated drug outcomes in high-risk adolescents. Psychology of Addictive Behaviors, 10, 18–27.
Stacy, A. W., Newcomb, M. D., & Bentler, P. M. (1991). Cognitive motivation and drug use: A 9-year longitudinal study. Journal of Abnormal Psychology, 100, 502–515.
Stacy, A. W., & Wiers, R. W. (2006). Common themes and new directions in implicit cognition and addiction. In R. W. Wiers & A. W. Stacy (Eds.), Handbook of implicit cognition and addiction (pp. 497–506). Thousand Oaks, CA: Sage.
Stephenson, M. T., Hoyle, R. H., Palmgreen, P., & Slater, M. D. (2003). Brief measures of sensation seeking for screening and large-scale surveys. Drug and Alcohol Dependence, 72, 279–286.
Taylor, S. E., & Fiske, S. T. (1978). Salience, attention, and attribution: Top of the head phenomena. In L. Berkowitz (Ed.), Advances in experimental social psychology (Vol. 11, pp. 249–288). New York: Academic.
Thombs, D. L., Dotterer, S., Olds, R. S., Sharp, K. E., & Giovannone, R. (2004). A close look at why one social norms campaign did not reduce student drinking. Journal of American College Health, 53, 61–68.
Tickle, J. J., Hull, J. G., Sargent, J. D., Dalton, M. A., & Heatherton, T. F. (2006). A structural equation model of social influences and exposure to media smoking on adolescent smoking. Basic and Applied Social Psychology, 28, 117–129.
Tolman, E. C. (1932). Purposive behavior in animals and men. Berkeley, CA: University of California Press.
Tormala, Z. L., & Petty, R. E. (2004). Source credibility and attitude certainty: A metacognitive analysis of resistance to persuasion. Journal of Consumer Psychology, 14, 427–442.
Ullman, J. B., & Bentler, P. M. (2003). Structural equation modeling. In J. A. Schinka & W. F. Velicer (Eds.), Handbook of psychology (pp. 607–634). Hoboken, NJ: Wiley.
Van Schie, E. C. M., & Van der Pligt, J. (1995). Influencing risk preference in decision making: The effects of framing and salience. Organizational Behavior and Human Decision Processes, 63, 264–275.
Walster, E., & Festinger, L. (1962). The effectiveness of “overheard” persuasive communications. Journal of Abnormal and Social Psychology, 65, 395–402.
Werch, C. E., Pappas, D. M., Carlson, J. M., DiClemente, C. C., Chally, P. S., & Sinder, J. A. (2000). Results of a social norm intervention to prevent binge drinking among first-year residential college students. Journal of American College Health, 49, 85–92.
Werner-Wilson, R. J., & Arbel, O. (2000). Assessment of interpersonal influences on adolescents: The parent and peer influence scale. The American Journal of Family Therapy, 28, 265–274.
Weschler, H., Nelson, T. F., Lee, J. E., & Seibring, M. (2003). Perception and reality: A national evaluation of social norms marketing interventions to reduce college students’ heavy alcohol use. Journal of Studies on Alcohol, 64, 484–494.
Wood, M. D., Nagoshi, C. T., & Dennis, D. A. (1992). Alcohol norms and expectations as predictors of alcohol use and problems in a college student sample. American Journal of Drug and Alcohol Abuse, 18, 461–476.
Zhao, X., Sayeed, S., Cappella, J., Hornik, R., Fishbein, M., & Ahern, R. K. (2006). Targeting norm-related beliefs about marijuana use in an adolescent population. Health Communication, 19, 187–196.
Zuckerman, M. (1994). Behavioral expression and biosocial bases of sensation seeking. New York: Cambridge University Press.
Zuckerman, M., Eysenck, S., & Eysenck, H. J. (1979). Sensation seeking in England and America: Cross-cultural age and sex comparisons. Journal of Consulting and Clinical Psychology, 46, 139–149.
Author information
Authors and Affiliations
Corresponding author
Additional information
The contents of this article are solely the responsibility of the authors and do not necessarily reflect the views of the National Institute on Drug Abuse. This research was supported by National Institute on Drug Abuse Grant 5R01 DA015957-03, which we gratefully acknowledge. We thank Justin Hackett, Vanessa Hemovich, and Sarah Ting for their assistance at various phases of this research.
Rights and permissions
About this article
Cite this article
Siegel, J.T., Alvaro, E.M., Crano, W.D. et al. Influencing Inhalant Intentions by Changing Socio-Personal Expectations. Prev Sci 9, 153–165 (2008). https://doi.org/10.1007/s11121-008-0091-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-008-0091-z