
Abstract
This study was designed to test hypotheses about family risk factors and their links to dosage and efficacy of a family-centered preventive intervention. Participants were 172 families with an 11 year-old child randomly assigned to the intervention condition in the Strong African American Families Program (SAAF). Two family risk factors, ratio of adults to children in the household and youth unconventionality, were negatively related to dosage, defined as number of intervention sessions attended. Dosage, in turn, was associated with changes in targeted parenting behavior across the 7 months between pretest and posttest. The effect of family risk factors on the link between program dosage and changes in parenting behavior was stronger for families experiencing more risks. The results highlight the need for engagement strategies for recruiting and retaining high-risk families in preventive interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mental health needs among rural African Americans have received little attention from researchers. Until recently, no empirically based programs had been designed to prevent substance use and early sexual activity among the several million African American youth who live in the rural South (Brody et al., 1997). Data from the National Center on Addiction and Substance Use (2000) indicate that youth substance use and its correlates, such as academic failure, behavioral problems, and emotional difficulties, have been increasing more rapidly in rural than in urban areas. In response to this need, we developed the Strong African American Families Program (SAAF) and are currently evaluating it in a longitudinal prevention trial. To date, analyses of SAAF’s efficacy indicate that families who participated in prevention programming evinced increases in targeted parenting practices and youth protective factors along with a decrease in youths’ likelihood of initiating alcohol use or sexual activity; families in the control condition, who did not participate in the intervention, did not display these changes (Brody et al., 2004b, 2005, 2006; Murry et al., 2005). Our results build on those of other family-centered intervention programs that have been shown to enhance parent and youth competence and inhibit the use of alcohol and other substances, delinquent activity, aggression, and other problem behaviors among young people (Albee & Gullotta, 1997; Dishion & Kavanagh, 2000; Spoth, Redmond, & Shin, 2001; Weissberg & Greenberg, 1998).

Conceptual model
Intervention attendance, or dosage, has been identified as a critical source of variability in intervention outcomes (Spoth & Redmond, 2000). Reported rates of participation in family-centered prevention programs vary from about 30% to 75% (Charlebois et al., 2004; Murry et al., 2004; Spoth & Redmond, 2002). A primary concern voiced by prevention scientists and interventionists is that those families at highest risk for using suboptimal child rearing practices may be more likely to drop out of programs or participate inconsistently, thereby experiencing fewer benefits (Haggerty et al., 2002). Few studies, however, report on dosage variability or the effects of dose on program outcomes. Of those reporting dose effects, linear associations are common, with higher doses leading to better outcomes (Aber et al., 1998; August et al., 2001; Braswell & August, 1997). A number of studies, however, suggest that the relations between dose and outcomes are complex. For example, Spoth et al. (1995) found that intervention attendance was a stronger predictor of parenting outcomes for fathers than for mothers. In recent individual-based interventions, gender (August et al., 2004) and family structure (Charlebois et al., 2004) moderated the associations between interventions and outcomes.
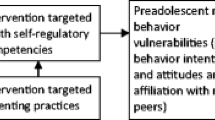
The hypotheses that guided this study are summarized in the conceptual model in Fig. 1. We first tested the hypothesis that SAAF dosage would mediate the influence that family risk factors, which longitudinal studies have shown to compromise African American families’ functioning, exert on changes in intervention-targeted parenting behavior. Families experiencing higher levels of risk were hypothesized to attend fewer prevention sessions. In turn, attendance at fewer sessions was hypothesized to be associated with less change in targeted parenting behavior. The second hypothesis involved the effect of family risk factors on the association between dose and outcome. Families experiencing more risk factors were hypothesized to require more sessions to benefit from the program. In the sections that follow, we briefly review evidence for the risk factors that we expect to influence dose and provide an overview of the SAAF prevention program.
The families who participated in the SAAF research program live in small towns and communities in rural Georgia in which poverty rates are among the highest in the nation and unemployment rates are above the national average (Proctor & Dalaker, 2003). Although 75% of the primary caregivers in the study work an average of 39 hr per week, 50% of the total sample of families live below federal poverty standards and another 25% live within 150% of the poverty threshold. Based on more than a decade of research with rural African American families (Brody et al., 1994, 2002, 2003a,b; Murry & Brody, 1999), we identified six family risk factors that we hypothesized would forecast families’ participation in SAAF: (a) ratio of adults to children in the household, (b) economic stress, (c) maternal depression, (d) poor parent-child relationship quality, (e) youth involvement in unconventional activities, and (f) low religious involvement.
Mother-headed, African American families in rural areas face chronic economic pressures (Brody et al., 1994; Conger et al., 2002) which can induce frustration, anger, depression, feelings of helplessness, and low self-esteem among caregivers (Brody et al., 1994, 2004a). The negative emotions that economic stress engenders compromise healthy family functioning resulting in more disengaged and less supportive parent-child relationships (Brody et al., 1994, 2004a; Conger et al., 1992). Family composition, particularly single parenthood (Dumka et al., 1997; Rohrbach et al., 1994), low family income (Rohrbach et al., 1994; Spoth et al., 1996), poor parental mental health (Rohrbach et al., 1994; Cohen & Linton, 1995) and compromised family relationships (Gorman-Smith et al., 2002) are associated with low rates of participation in family-centered interventions. We predicted that a relatively high ratio of children to adults in the household, economic stress, and caregivers’ depression would be negatively associated with the number of intervention sessions families would attend. Because caregivers in economically and emotionally stressed families experience more difficulty in using effective parenting strategies, we also expected consistent attendance to be particularly important for these families for them to benefit from the intervention.
Little research has investigated the influence of youth characteristics on prevention dosage (Biglan & Metzler, 1998). Spoth and colleagues (1996) reported that children’s resistance to attending was a salient, but not central, factor impeding attendance in a multicomponent family prevention program. Haggerty and colleagues (2002) found that youth antisocial behavior was associated with higher levels of caregiver participation in a parent training program in which youth did not participate. We have found that unconventional behavior among rural African American youth is both a result of compromised family relationships and a contributor to further relationship disruption (Brody et al., 2004a). Youths’ unconventional or externalizing behavior elicits low involvement, low support, and high negativity from parents (Anderson et al., 1986; Ge 1996; O’Connor et al., 1998). Because both youth and parents were required to participate in the SAAF program, we expected that unconventionality in youth behavior would impede attendance. Furthermore, because unconventional youth behavior presents a challenge to effective parenting, we expected consistent attendance to be especially important for positive outcomes among families with an unconventional youth.
Various forms of religiosity, including organizational, nonorganizational, and attitudinal, have been associated with positive outcomes for African American youth (Brody et al., 1996, 1998; Edwards, 1976; Lee, 1984, 1985). Religious participation provides positive role models for African Americans and serves as a mechanism of racial socialization and political action (Stevenson, 1997; Taylor et al., 1987). Our prior studies revealed a positive association between rural African American mothers’ religiosity and their use of competence-promoting parenting practices (Brody et al., 1996, 1998). In addition, Stevenson (1997) reported that, among African American adolescents, greater religious commitment is related to fewer externalizing problems and more effective anger control. We are not aware of any studies in which religious involvement was examined as a predictor of intervention attendance. Because of religiosity’s link to organized and effective parent-child relationships among African American families, we predicted that families whose religious involvement was low would also demonstrate inconsistent attendance and that these families would require more consistent attendance to actualize parenting changes.
To determine how these contextual sources of risk contributed to dosage levels among families participating in SAAF, we examined each risk factor, both individually and as part of a risk factor index. Examining individual risk factors provides information on their unique characteristics that require modification if attendance is to improve. Studies in developmental psychology and psychopathology, however, suggest that risk factors tend to cluster in families (Masten & Coatsworth, 1998) and that no single risk factor is sufficient to explain family functioning (Sameroff et al., 1993). Risk factors’ effects are cumulative, such that the presence of more risk factors is related to a greater likelihood of negative outcomes (Seifer et al., 1992). The use of a risk factor index in the present study enabled us to determine the stressors’ cumulative effect on participants’ attendance and on the link between dose and parenting outcome.
Method
The data for this study were drawn from the SAAF pretest and posttest assessments.
Family risk factors were measured at the pretest. As described in the introduction, SAAF is based on Brody and Murry’s longitudinal research program, which specifies pathways to competence for rural African American children living in married-parent and single-parent families. SAAF targets parenting skills and family processes that protect youth from using alcohol or other substances and engaging in early sexual activity (Brody et al., 2004b; Murry & Brody, 2004). The seven consecutive weekly meetings that comprise the SAAF prevention program are held at community facilities. Each meeting includes separate, concurrent training sessions for parents and children, followed by a joint parent-child session during which the families practice the skills they learned in their separate sessions. The concurrent and family sessions each last 1 hr; thus, parents and youth receive 14 hr of prevention training.
This study focused on the effect of dosage, defined as program attendance, on intervention-induced changes in regulated, communicative parenting. Brody and Murry’s research indicates that changing the parenting practices that comprise this construct is central to preventing rural African American youth from initiating substance use and sexual activity (Brody et al., 2002, 2003a; Murry & Brody, 1999). Parents in the prevention condition are taught involved-vigilant parenting, which includes the consistent use of nurturant parenting practices along with high levels of monitoring and control; they were also taught strategies for adaptive racial socialization, communication about sexuality; and the establishment of clear rules about alcohol use.
Ten three-person teams, all African American, conducted 19 prevention groups. Potential group leaders were referred to the project by our community liaison network. Group leaders were required to have a minimum of a high school education and prior experience in working with children and families. Group leaders participated in three training sessions during a 4-day period. Before conducting any intervention sessions, the leaders demonstrated their mastery of the curriculum and the prescribed method of presenting it. Group leaders were paid $75.00 per intervention session. After the intervention began, each team was videotaped while conducting sessions to assess fidelity to the program. For each team, two parent sessions were selected randomly and scored for adherence to the prevention curriculum. Coverage of the curriculum components exceeded 80%. An average of 10 families attended each session. Approximately 65% of the pretested families took part in five or more sessions, with 44% attending all seven sessions.
Participants
Participants in the study were African American mothers and their 11-year-old children (M = 11.2 years of age), who resided in eight rural counties in Georgia. These counties were selected based on their rural designation according to the U.S. Bureau of the Census (1993) and their proximity to the University of Georgia. The eight counties were matched based on demographic characteristics, then one county from each matched pair was randomly assigned to either the control or the intervention condition, resulting in the assignment of four counties to each condition. Schools in these counties provided lists of 11-year-old students, from which 521 families were selected randomly. Of these families, 332 completed pretests. Refusal rates were similar across the intervention and control counties. The recruitment rate of 64% exceeds rates commonly reported for prevention trials that address problematic and high-risk behaviors among children and adolescents (Spoth 2000). The participants included 150 families in the control counties and 172 families in the intervention counties. Because the present study addresses family participation in the intervention, the analyses include only those participants randomly assigned to the prevention group. Of the families from intervention counties, 165 (96%) completed both the pretest and posttest; 7 families (4%) who completed the pretest did not complete the posttest. No statistically significant differences emerged at pretest between these 7 families and retained families. To preserve the random nature of the group assignments, the analyses included all families from intervention counties who completed the pretest regardless of the number of sessions that they actually attended (an intent-to-treat analysis). This includes 21 families who did not attend any prevention sessions but who completed the pretest and the 3-month delayed posttest. Excluding these families would have introduced self-selection bias into the findings.
The families who completed the posttest had an average of 2.7 children. In 53.6% of these families, the target child was a girl. Of the mothers in the families, 33.1% were single, 23.0% were married and living with their husbands, 33.9% were married but separated from their husbands, and 7.0% were living with partners to whom they were not married. Of the two-parent families, 93.0% included both of the target child’s biological parents. The mothers’ mean age was 38.1 years, and the fathers were an average of 39.4 years old. A majority of the mothers, 78.7%, had completed high school. The families’ median household income was $1,655.00 per month.
Procedures
The families were contacted initially by Center staff, with follow-up contacts made by community liaisons who reside in the counties in which the participants live and maintain connections between the University research group and the communities. The community liaisons were African American community members selected on the basis of their social contacts and standing in the community. The community liaisons sent a letter to the families and followed up on the letter with phone calls to the primary caregivers. Families were initially recruited into the overall project but were informed that they could be assigned to an intervention condition. Each family was paid $100 at pretest and another $100 at posttest. To enhance rapport and cultural understanding, African American students and community members served as home visitors to collect pretest and posttest data.
During each data collection, one home visit lasting 2 hr was made to each family. Informed consent forms were completed at both data collection points. Mothers consented to their own and their children’s participation in the study, and the children assented to their own participation. At the home visits, self-report questionnaires were administered to mothers and target children in an interview format, which eliminated literacy concerns. Each interview was conducted privately, with no other family members present or able to overhear the conversation. The posttest was conducted in both the prevention and control counties approximately 3 months after the end of prevention programming. The time between pretesting and posttesting averaged 7 months.
Measures
Dosage
Dosage was defined as the total number of SAAF sessions that each family attended. The session facilitators recorded families’ attendance at each of the seven sessions; no make-up sessions were provided. Attendance by both the target child and a caregiver was a requirement of the program. If a secondary caregiver attended instead of the primary caregiver, the session was coded as attended. This occurred in fewer than 8% of the attended sessions.
Family risk factors
The ratio of children to adults in a household was calculated by dividing the number of children living in the home by the number of adults living there. Mothers’ responses to the Money for Necessities subscale from the Family Resource Scale (Dunst & Leet, 1987) were used to determine each family’s perceived economic stress. The subscale consists of six items, rated on a scale ranging from 1 (not at all adequate) to 5 (almost always adequate), concerning clothing, residential heating, indoor plumbing and running water, medical care, dental care, and food. Cronbach’s alpha for this sample was .77.
Maternal depressive symptoms were assessed by mothers’ self-reports on the Center for Epidemiologic Studies Depression Scale (CES–D; Radloff, 1977). The CES–D has been used widely with community samples, some of which included rural African American mothers (Brody et al., 1994, 2002). The items address the frequency with which the respondent experienced various depressive symptoms during the past week, rated on a scale ranging from rarely or none of the time (less than 1 day) to most or all of the time (5 to 7 days). Cronbach’s alpha for this sample was .83. Parent-child relationship quality was measured using mothers’ and youths’ responses to the Interaction Behavior Questionnaire (IBQ; Prinz et al., 1979), which assesses support and involvement in parent-child relationships. Because mothers’ and youths’ reports were correlated at r = .36 (p < .01), their responses were summed to yield a multi-informant assessment of relationship quality. Cronbach’s alpha was .82 for mothers and .78 for youth.
Low involvement in religious activities was assessed using mothers’ responses to three questions concerning families’ church involvement: “Have you attended church on a regular basis in the past 6 months?” “Have you participated in church activities (aside from the Sunday services) during the past 6 months?” and “Has your child been involved in church-based activities during the past 6 months?” The affirmative responses were summed.
Youth unconventionality was assessed by standardizing and summing youths’ responses to three measures: willingness to have sex, ability to resist peer pressure, and resistance efficacy. Willingness to have sex was measured using 1 item from Gibbons and Gerrard’s (1995) research: “Suppose you were alone with your [boyfriend/girlfriend]. He/she wants to have sex, but neither of you has a condom. In this situation, how willing would you be to go ahead and have sex?” The response options ranged from 1 (not at all) to 5 (very). Low resistance to peer pressure was assessed using 3 items (Spoth et al., 1998) that youth rated on a scale ranging from 0 (not true) to 2 (very true). The responses were reverse scored so that high responses indicated an inability to resist peer pressure. Cronbach’s alpha for this scale was .93. On the resistance efficacy scale (Wills et al., 2000), youth responded to the following scenario: “You’re with kids who get some beer. Your friend takes a beer and asks if you want one. What would you probably do in this situation?” Responses included 1 (I would take the beer and drink it), 2 (I would say, “Not now, maybe some other time”), and 3 (I would say “No” and not drink it). The scenario was repeated for cigarette smoking and marijuana use. For the purposes of this study, the responses were reversed scored so that high scores represented low resistance efficacy. This scale had a Cronbach’s alpha of .87.
A risk score was calculated for each family by summing the measures of the six risk factors (Baldwin et al. 1990; Sameroff et al., 1993). Families’ scores on each risk factor were determined by their positions relative to the measures’ medians for this sample (0 or 1); the index had a possible range of 0 to 6.
Regulated, communicative parenting
Four indicators of this construct were included: involved-vigilant parenting, adaptive racial socialization, communication about sex, and clear communication of expectations about alcohol use. Involved-vigilant parenting was assessed via an instrument that the authors have used in their previous research with rural African American families (Brody et al., 2001, 2003a). The scale is composed of 19 items that assess the frequency, ranging from 1 (never) to 5 (always), of parental behaviors concerning involvement, inductive discipline, consistent discipline, and monitoring. Nine items assessed involvement and inductive discipline, five items concerned child monitoring, and four items assessed consistent discipline. As in our prior research (Brody et al., 2001, 2003a), responses to these subscales were summed to form the involved-vigilant indicator. Cronbach’s alphas for the pretest and posttest assessments exceeded .70. Racial socialization was assessed via the Racial Socialization Scale (Hughes & Johnson, 2001), which includes 15 items regarding parents’ racial socialization practices that are rated on Likert scales ranging from 1 (never) to 3 (three to five times). Cronbach’s alpha at pretest and posttest exceeded .75. The Parental Communication About Sex Scale, adapted from previous scales measuring parental communication about substance use (see Gerrard et al., 2003; Wills et al., 2003), was used to assess communication about sex. The scale consists of 9 items, coded on a scale ranging from 0 (no) to 2 (yes, quite a bit), that concern parent-child discussions. Cronbach’s alphas exceeded .80 at the pre- and posttest assessments. The establishment of clear expectations about alcohol and other drugs was assessed using 2 items written by Spoth et al. (1998): “I have told my child exactly what I feel about alcohol and drugs” and “I remind my child that very few children his or her age get involved with alcohol and drugs.” The response set ranged from 0 (not true) to 2 (very true or often true). The correlation between the 2 items at the pretest and posttest was .51.
Results
Linking family risks, dosage, and changes in regulated, communicative parenting
We tested the hypothesis that higher levels of family risks would be associated with attendance at fewer SAAF prevention sessions; in turn, attendance would be linked to changes from pretest to posttest in regulated, communicative parenting. The data were analyzed using Structural Equation Modeling (SEM) with the maximum likelihood estimation pro-cedures available in AMOS 4.0 (Arbuckle, 1999). Table 1 presents the correlation matrix, means, and standard deviations for the SEM variables. The latent parenting construct was indicated by the involved vigilant parenting, racial socialization, communication about sex, and expectations for alcohol use scales. The posttest parenting construct was regressed on the same construct at pretest. We specified each risk factor as a predictor of dose and further specified dose as a predictor of changes in parenting. This initial model did not fit the data [χ2(86, N = 164) = 192.93, p = .000, χ2/df = 2.24, GFI = .85, CFI = .75]. Examination of nonsignificant paths and modification indices indicated that four of the family risk factors, economic stress, maternal depression, poor relationship quality, and low religious involvement, were not significant predictors of either dosage or parenting. The two remaining predictors, ratio of children to adults and youth unconventionality, did not directly predict parenting. Nonsignificant pathways were subsequently dropped from the model. The revised model is presented in Fig. 2. This model fit the data very well: χ2(40, N = 164) = 33.36, p = .76, χ2/df = .84, GFI = .97, CFI = 1.00. Ratio of adults to children in the household (β = −.24, p < .05) and youth unconventionality (β = −.43, p < .05) were negatively associated with dosage and predicted 24% of the variability in dosage (R 2 = .24). Dosage was associated positively with changes in targeted parenting behaviors (β = .24, p = .05). We conducted a Sobel mediating analysis to test the indirect effects of these risk behaviors on change in parenting through their influence on dose. Both pathways were significant (ratio, t = 1.96, p = .05; unconventionality, t = 2.23, p = .03), indicating that dosage partially mediated the influences of a low ratio of adults to children in the household and youth unconventionality on changes in parenting.

Results of hypothesis testing
In the next analyses, we examined the mediational hypothesis using the aggregated family risk index as a predictor of dose. This model also fit the data well: χ2(31, N = 168) = 30.62, p = .49, χ2/df = .99, GFI = .95, CFI = 97. Although the aggregate family risk index significantly predicted SAAF dosage (β = −.21, p = .05), it predicted considerably less variability in dosage than did the previous model (R 2 = .05). The Sobel test indicated that dose was not a significant mediator of the link between overall family risk and changes in parenting (t = 1.79, p = .073).
Moderational effects of family risks on the link between dose and changes in regulated, communicative parenting
We used multigroup comparison procedures (Bollen, 1989) to determine whether the effects of SAAF dosage on changes in regulated, communicative parenting differed by family risk factor level. After performing median splits on each family risk factor and on the family risk index, we first estimated a two-group invariance model by imposing equality constraints on every coefficient estimate. We then relaxed one equality constraint at a time for the specific coefficient under investigation, allowing the coefficient to differ across groups, and re-estimated the model. A change in chi-square between the invariance model and the re-estimated model indicates a significant group difference. Using this procedure for each individual family risk factor, we detected no group differences effects. For the comparison with the risk index, a marginally significant difference emerged: Δχ2(1, N = 101) = 3.59, p < .058. Figure 3 presents the standardized coefficient estimates separately for the high- and low-risk groups. The standardized path coefficient between dosage and change in regulated, communicative parenting was .38 for high-risk families and .05 for low-risk families (see Fig. 3). This indicates that the effect of SAAF dosage on change in the intervention-targeted parenting behaviors was significantly stronger for families experiencing more risks.

Standardized coefficient estimates for the high- and low-risk groups
Discussion
The present study was designed to test hypotheses about family risk processes and their links to dosage and efficacy of a family-centered preventive intervention designed specifically for rural African American families with young adolescents. We hypothesized that the risk factors that our longitudinal research indicated would compromise family functioning would impact changes in parenting outcomes by compromising consistent attendance. The strongest single influence on dosage in this study proved to be youth unconventionality: Families in which the youth was unconventional were unlikely to participate consistently in SAAF. Although our present data do not indicate why this occurs, several possibilities are plausible. Unconventional youth may pressure parents not to attend, or simply refuse to attend. Their parents may have been less effective in organizing their youths’ behavior. This finding may be contrasted with those of Haggerty and colleagues (2002), who found that caregivers of youth who displayed antisocial behavior were more likely to attend parent training. Haggerty and colleagues (2002) speculated that parents of antisocial youth would be more motivated to attend parent training to find ways to learn to manage their adolescents’ behavior. In the context of parent-only intervention, however, youths’ refusal to attend would not affect dosage, and youth may be less motivated to interfere with parents’ attendance. In the SAAF intervention, however, youth were required to participate. It is also important to note that the Haggerty et al. study used a sample of predominantly Caucasian families from a large metropolitan school district. Gorman-Smith and associates (2002) linked two child characteristics to patterns of intervention response: depression and hyperactivity. Families of children with depression were more likely to be minimal responders, a pattern characterized by difficulty in recruitment and subsequent low levels of participation. Families of children with hyperactivity were intervention responders; they were initially difficult to recruit but were highly motivated to attend when recruited. Taken together, these studies highlight the potential for child characteristics to impede intervention attendance or to enhance parents’ motivation to attend. Further research is required to delineate when specific child characteristics will impede or enhance attendance and engagement in family centered interventions.
Ratio of adults to children in the household was a significant predictor of SAAF dosage. This finding is consistent with other studies in which two-parent families were found to be more likely than single-parent families to receive high doses of an intervention (Cohen & Linton, 1995; Toomey et al., 1996). This pattern can be attributed to caregiving burdens and difficulty in finding the time and other resources needed for involvement in preventive interventions. Gross et al. (2001) found that low-income African American parents were most likely to drop out of a parent training program if they experienced time and schedule constraints. In SAAF, several procedures were implemented to resolve families’ logistical problems. Dinner was served to family members attending the prevention sessions, transportation was provided for any families who needed it, and child care at the sessions was available. Even with this level of active assistance, some parents still may have struggled with competing demands arising from social or school activities in which either the targeted youth or their siblings participate. Perhaps preventive interventions should include make-up sessions for parents with several children to accommodate their competing demands.
Four of the six hypothesized predictors of dosage yielded nonsignificant associations. Economic stress was not associated with dosage, a finding similar to those Haggerty et al. (2002) and Spoth and Redmond (2002) obtained. Gorman-Smith et al. (2002) however, found that families with low incomes who experienced economic stress were likely to be either enthusiastic participants or minimal respondents, suggesting that low income may not have a linear association with dose. Maternal depression also was not related to dosage, either in the present study or in the Gorman-Smith and associates (2002) SAFE Children intervention. The support received from family-based interventions may have strongly motivated parents with depression to attend. Alternatively, maternal depression may have a complex association with dose, motivating some parents, and impeding others.
Although an aggregate index of family risk was significantly associated with dose, it was a weaker predictor than a model consisting of ratio of adults to children in the household and youth unconventionality. This suggests that these risk factors may have posed unique obstacles to families’ attendance. The use of pretest measures that screen for high levels of caregiving burden and youth unconventionality could be used to plan expanded engagement procedures for these families.
The second primary hypothesis addressed the moderating influence of risk factors on the link between dose and intervention-targeted parenting behaviors. In contrast to the weaker effect that the aggregate risk index demonstrated in predicting dose, the risk index was useful in explicating the link between dose and changes in parenting behavior. Multigroup analyses indicated that the association of dosage with changes in parenting was stronger for families experiencing relatively higher levels of risk. Among low risk families, inconsistent attendance did not influence change in parenting. For high risk families, however, consistent attendance was crucial for achieving change in parenting. These results underscore the importance of maximizing participation among families who experience multiple risk factors. To date, researchers who develop and disseminate family-centered preventive interventions have not tested the efficacy of strategies for increasing attendance among high-risk families. Santisteban and associates (1996) developed and tested methods for engaging Latino families from different national backgrounds in family therapy and maintaining their involvement. Although the success rates varied among Latino groups, the procedures that the family therapists used could have heuristic value for designers of family-centered prevention programs.
That 65% of the SAAF families attended five or more of the weekly sessions, with 44% attending all seven, is testimony to their motivation to enhance their children’s development. It should be noted, however, that fathers rarely participated although they were invited to do so. In addition, it is not known whether the results that emerged for rural Georgia families would be replicated with urban families. These cautions notwithstanding, the results reported here document the importance of engaging in family-centered preventive interventions those families and youths who are coping with multiple risks.
References
Aber, J. L., Jones, S. M., Brown, J. L., Chaudry, N., & Samples, F. (1998). Resolving conflict creatively: Evaluating the developmental effects of a school-based violence prevention program in neighborhood and classroom context. Development and Psychopathology, 10, 187–213.
Albee, G. W., & Gullotta, T. P. (1997). Primary prevention’s evolution. In G. W. Albee & T. P. Gullotta (Eds.), Issues in children’s and families’ lives: Vol. 6. Primary prevention works (pp. 3–22). Thousand Oaks, CA: Sage.
Anderson, K. E., Lytton, H., & Romney, D. M. (1986). Mothers’ interactions with normal and conduct-disordered boys: who affects whom? Developmental Psychology, 22, 604–609.
Arbuckle, J. L., & Wothke, W. (1999). Amos 4.0 user’s guide. Chicago: SmallWaters Corporation.
August, G. J., Lee, S. S., Bloomquist, M. L., Realmuto, G. M., & Hektner, J. M. (2004). Maintenance effects of an evidence-based prevention innovation for aggressive children living in culturally diverse urban neighborhoods: the Early Risers effectiveness study. Journal of Emotional and Behavioral Disorders, 12, 194–205.
August, G. J., Realmuto, G. M., Hektner, J. M., & Bloomquist, M. L. (2001). An integrated components preventive intervention for aggressive elementary school children: the Early Risers program. Journal of Consulting and Clinical Psychology, 69, 614–626.
Baldwin, C., Baldwin, A., & Cole, R. (1990). Stress resistant families and stress resistant children. In J. Rolf, A. Masten, D. Cicchetti, K. Nuechterlein, & S. Weintraub (Eds.), Risk and protective factors in the development of psychopathology (pp. 257–280). New York: Cambridge University Press.
Biglan, A., & Metzler, C. W. (1998). A public health perspective for research on family-focused interventions. In R.S. Ashery, E.B. Robertson, & K.L. Kumpfer (Eds.), Drug abuse prevention through family interventions (pp. 430–458). Rockville, MD: National Institute on Drug Abuse.
Bollen, K. A. (1989). Structural equations with latent variables. New York: Wiley.
Braswell, L., & August, G. J. (1997). School-based secondary prevention for children with disruptive behavior: initial outcomes. Journal of Abnormal Child Psychology, 25, 197–208.
Brody, G. H., Flor, D. L., & Neubaum, E. (1998). Coparenting processes and child competence among rural African American families. In M. Lewis & C. Feiring (Eds.), Families, risk, and competence (pp. 227–243). Mahwah, NJ: Erlbaum.
Brody, G. H., Ge, X., Conger, R., Gibbons, F. X., Murry, V. M., Gerrard, M., et al. (2001). The influence of neighborhood disadvantage, collective socialization, and parenting on African American children’s affiliation with deviant peers. Child Development, 72, 1231–1246.
Brody, G. H., Ge, X., Kim, S. Y., Murry, V. M., Simons, R. L., Gibbons, F. X., et al. (2003a). Neighborhood disadvantage moderates associations of parenting and older sibling problem attitudes and behavior with conduct disorders in African American children. Journal of Consulting and Clinical Psychology, 71, 211– 222.
Brody, G. H., Kim, S., Murry, V. M., & Brown, A. C. (2003b). Longitudinal direct and indirect pathways linking older sibling competence to the development of younger sibling competence. Developmental Psychology, 39, 618–628.
Brody, G. H., Kim, S., Murry, V. M., & Brown, A. C. (2004a). Protective longitudinal paths linking child competence to behavioral problems among African American siblings. Child Development, 75, 455–467.
Brody, G. H., Murry, V. M., Gerrard, M., Gibbons, F. X., McNair, L., Brown, A. C., et al. (2006). The Strong African American Families Program: Prevention of youths’ high-risk behavior and a test of a model of change. Journal of Family Psychology, 20, 1–11.
Brody, G. H., Murry, V. M., Gerrard, M., Gibbons, F. X., Molgaard, V., McNair, L., et al. (2004b). The Strong African American Families Program: translating research into prevention programming. Child Development, 75, 900–917.
Brody, G. H., Murry, V. M., Kim, S., & Brown, A. C. (2002). Longitudinal pathways to competence and psychological adjustment among African American children living in rural single-parent households. Child Development, 73, 1505–1516.
Brody, G. H., Murry, V. M., McNair, L., Chen, Y., Gibbons, F. X., Gerrard, M., et al. (2005). Linking changes in parenting to parent-child relationship quality and youth self control: the Strong African American Families Program. Journal of Research on Adolescence, 14, 47–69.
Brody, G. H., Neubaum, E., Boyd, G. M., & Dufour, M. (1997). Health consequences of alcohol use in rural America. In E. B. Robertson, Z. Sloboda, G. M. Boyd, L. Beatty, & N. J. Kozel (Eds.), Rural substance abuse: State of knowledge and issues (NIDA Research Monograph 168, pp. 137–174). Rockville, MD: U.S. Department of Health and Human Services.
Brody, G. H., Stoneman, Z., & Flor, D. (1996). Parental religiosity, family processes, and youth competence in rural, two-parent African American families. Developmental Psychology, 32, 696–706.
Brody, G. H., Stoneman, Z., Flor, D., McCrary, C., Hastings, L., & Conyers, O. (1994). Financial resources, parent psychological functioning, parent co-caregiving, and early adolescent competence in rural two-parent African-American families. Child Development, 65, 590–605.
Charlebois, P., Brendgen, M., Vitaro, F., Normandeau, S., & Boudreau, J. -F. (2004). Examining dosage effects on prevention outcomes: Results from a multi-modal longitudinal preventive intervention for young disruptive boys. Journal of School Psychology, 42, 201–220.
Cohen, D. A., & Linton, K. L. (1995). Parent participation in adolescent drug abuse prevention program. Journal of Drug Education, 25, 159–169.
Conger, R. D., Conger, K. J., Elder, G. H., Lorenz, F. O., Simons, R. L., & Whitbeck, L. B. (1992). A family process model of economic hardship and adjustment of early adolescent boys. Child Development, 63, 526–541.
Conger, R. D., Ebert-Wallace, L., Sun, Y., Simons, R. L., McLoyd, V. C., & Brody, G. H. (2002). Economic pressure in African-American families: a replication and extension of the Family Stress Model. Developmental Psychology, 38, 179–193.
Dishion, T. J., & Kavanagh, K. (2000). A multilevel approach to family-centered prevention in schools: process and outcome. Addictive Behaviors, 25, 899–911.
Dumka, L. E., Garza, C. A., Roosa, M. W., & Stoerzinger, H. D. (1997). Recruitment and retention of high-risk families into a preventive parent training intervention. Journal of Primary Prevention, 18, 25–39.
Dunst, C. J., & Leet, H. E. (1987). Measuring the adequacy of resources in households with young children. Child: Care, Health, and Development, 13, 111–125.
Edwards, O. L. (1976). Components of academic success: a profile of achieving Black adolescents. Journal of Negro Education, 45, 408–422.
Ge, X., Conger, R. D., Cadoret, R. J., Neiderhiser, J. M., Yates, W., Troughton, E., et al. (1996). The developmental interface between nature and nurture: a mutual influence model of child antisocial behavior and parent behaviors. Developmental Psychology, 32, 574–589.
Gerrard, M., Gibbons, F. X., & Gano, M. (2003). Adolescents’ risk perceptions and behavioral willingness: implications for intervention. In D. Romer (Ed.), Reducing adolescent risk: Toward an integrated approach (pp. 75–81). Newbury Park, CA: Sage.
Gibbons, F. X., & Gerrard, M. (1995). Predicting young adults’ health risk behavior. Journal of Personality and Social Psychology, 69, 505–517.
Gorman-Smith, D., Tolan, P. H., Henry, D. B., Leventhal, A., Schoeny, M., Lutovsky, K., et al. (2002). Predictors of participation in a family-focused preventive intervention for substance use. Psychology of Addictive Behaviors, 16(4S), S55–S64.
Gross, D., Julion, W., & Fogg, L. (2001). What motivates participation and dropout among low-income urban families of color in a prevention intervention? Family Relations, 50, 246–254.
Haggerty, K. P., Fleming, C. B., Lonczak, H. S., Oxford, M. L., Harachi, T. W., & Catalano, R. F. (2002). Predictors of participation in parenting workshops. Journal of Primary Prevention, 22, 375–378.
Hughes, D., & Johnson, D. (2001). Correlates in children’s experiences of parents’ racial socialization behaviors. Journal of Marriage and Family, 63, 981–995.
Lee, C. C. (1984). An investigation of psychosocial variables related to academic success for rural Black adolescents. Journal of Negro Education, 53, 424–434.
Lee, C. C. (1985). Successful rural Black adolescents: a psychosocial profile. Adolescence, 20, 129–142.
Masten, A. S., & Coatsworth, J. D. (1998). The development of competence in favorable and unfavorable environments: lessons from research on successful children. American Psychologist, 53, 205–220.
Murry, V. M., Brody, G. H., McNair, L., Luo, Z., Gibbons, F. X., Gerrard, M., et al. (2005). Parental involvement promotes rural African American youths’ self-pride and sexual self-concepts. Journal of Marriage and Family, 67, 627–642.
Murry, V. M., Kotchick, B. A., Wallace, S., Ketchen, G., Eddings, K., Heller, L., et al. (2004). Race, culture, and ethnicity: implications for a community intervention. Journal of Child and Family Studies, 13, 81–99.
Murry, V. M., & Brody, G. H. (1999). Self-regulation and self-worth of Black children reared in economically stressed, rural, single mother-headed families: the contributions of risk and protective factors. Journal of Family Issues, 20, 458–484.
Murry, V. M., & Brody, G. H. (2004). Partnering with community stakeholders: engaging rural African American families in basic research and the Strong African American Families preventive intervention program. Journal of Marital and Family Therapy, 30, 271–283.
National Center on Addiction and Substance Abuse. (2000). No place to hide: Substance abuse in mid-size cities and rural America. New York: Author.
O’Connor, T. G., Deater-Deckard, K., Fulker, D., Rutter, M., & Plomin, R. (1998). Genotype-environment correlations in late childhood and early adolescence: antisocial behavioral problems and coercive parenting. Developmental Psychology, 34, 970– 981.
Prinz, R. J., Foster, S. L., Kent, R. N., & O’Leary, K. D. (1979). Multivariate assessment of conflict in distressed and nondistressed mother-adolescent dyads. Journal of Applied Behavior Analysis, 12, 691–700.
Proctor, B. D., & Dalaker, J. (2003, September). Poverty in the United States: 2002 (U.S. Census Bureau Current Population Reports Series P60-222, Consumer Income). Washington, DC: U.S. Government Printing Office.
Radloff, L. S. (1977). The CES-D Scale: a self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401.
Rohrbach, L. A., Hodgson, C. S., Broder, B. I., Montgomery, S. B., Flay, B. R., Hansen, W. B., et al. (1994). Parental participation in drug abuse prevention: results from the Midwestern Prevention Project. Journal of Research on Adolescence, 4, 295– 317.
Sameroff, A. J., Seifer, R., Baldwin, A., & Baldwin, C. (1993). Stability of intelligence from preschool to adolescence: the influence of social and family risk factors. Child Development, 64, 80–97.
Santisteban, D. A., Szapocznik, J., Perez-Vidal, A., Kurtines, W. M., Murray, E. J., & LaPerriere, A. (1996). Efficacy of intervention for engaging youth and families into treatment and some variables that may contribute to differential effectiveness. Journal of Family Psychology, 10, 35–44.
Seifer, R., Sameroff, A. J., Baldwin, C. P., & Baldwin, A. (1992). Child and family factors that ameliorate risk between 4 and 13 years of age. Journal of the American Academy of Child and Adolescent Psychiatry, 31, 893–903.
Spoth, R., & Redmond, C. (2000). Research on family engagement in preventive interventions: toward improved use of scientific findings in primary prevention practice. Journal of Primary Prevention, 21, 267–284.
Spoth, R. L., & Redmond, C. (2002). Project Family prevention trials based in community-university partnerships: toward scaled-up preventive interventions. Prevention Science, 3, 203–221.
Spoth, R., Redmond, C., Haggerty, K., & Ward, T. (1995). A controlled parenting skills outcomes study examining individual differences and attendance effects. Journal of Marriage and the Family, 57, 449–464.
Spoth, R., Redmond, C., Hockaday, C., & Shin, C. Y. (1996). Barriers to participation in family skills preventive interventions and their evaluations: a replication and extension. Family Relations, 45, 247–254.
Spoth, R., Redmond, C., & Shin, C. (1998). Direct and indirect latent-variable parenting outcomes of two universal family-focused preventive interventions: extending a public health-oriented research base. Journal of Consulting and Clinical Psychology, 66, 385–399.
Spoth, R., Redmond, C., & Shin, C. (2000). Modeling factors influencing enrollment in family-focused preventive intervention research. Prevention Science, 1, 213–225.
Spoth, R. L., Redmond, C., & Shin, C. (2001). Randomized trial of brief family interventions for general populations: adolescent substance use outcomes 4 years following baseline. Journal of Consulting and Clinical Psychology, 69, 627–642.
Stevenson, H. C. (1997). Validation of the Scale of Racial Socialization for African American Adolescents: steps toward multidimensionality. Journal of Black Psychology, 20, 445–468.
Taylor, R. J., Thornton, M. C., & Chatters, L. M. (1987). Black Americans’ perception of the socio-historical role of the church. Journal of Black Studies, 18, 123–138.
Toomey, T. L., Williams, C. L., & Perry, C. L. (1996). An alcohol primary prevention program for parents of 7th graders: the Amazing Alternatives! Home program. Journal of Child Adolescent Substance Abuse, 5, 35–53.
U.S. Bureau of the Census. (1993). Poverty in the United States, 1992 (Current Population Reports, Series P60–185, No. 185). Washington, DC: U.S. Government Printing Office.
Weissberg, R., & Greenberg, M. T. (1998). Community and school prevention. In I. Sigel & A. Renninger (Eds.), Handbook of child psychology: Vol. 4. Child psychology in practice (5th ed., pp. 877–954). New York: Wiley.
Wills, T. A., Gibbons, F. X., Gerrard, M., & Brody, G. H. (2000). Protection and vulnerability processes relevant for early onset of substance use: a test among African American children. Health Psychology, 19, 253–263.
Wills, T. A., Gibbons, F. X., Gerrard, M., Murry, V. M., & Brody, G. H. (2003). Family communication and religiosity related to substance use and sexual behavior in early adolescence: a test for pathways through self-control and prototype perceptions. Psychology of Addictive Behaviors, 17, 312–323.
Acknowledgements
This research was supported by grants from the National Institute on Alcohol Abuse and Alcoholism and the National Institute of Mental Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brody, G.H., Murry, V.M., Chen, Yf. et al. Effects of Family Risk Factors on Dosage and Efficacy of a Family-centered Preventive Intervention for Rural African Americans. Prev Sci 7, 281–291 (2006). https://doi.org/10.1007/s11121-006-0032-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-006-0032-7